SLU and GWEP Develop a Telehealth Platform for Geriatric Services
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Spring 2021
Vol. XXX, No. 1
SLU and GWEP Develop a Telehealth
Platform for Geriatric Services
I
By John Morley, MB, BCh
n the summer of 2019, the Gateway Geriatric Workforce
Enhancement Program (GWEP) began work on developing a
telehealth platform, Aging Successfully, that would enable
users to gather assessment data and deliver services virtually.
Collaborating with a technology
development company to create
a HIPAA-compliant telehealth
platform, we aim to deliver services
to older adults electronically.
In those pre-pandemic days,
we envisioned a suite of programs
to include the Rapid Geriatric
Assessment and Cognitive
Stimulation Therapy. With the
advent of COVID-19, awareness is
heightened regarding continuing
increases in the number of older
adults, the small numbers of
healthcare professionals specializing
in geriatric care (particularly
geriatricians), and a need to
(continued on page 4)
Questions? FAX: 314-977-3370 email: aging@slu.edu Aging Successfully, Vol. XXX, No. 1 1
we
want to
hear
from
YOU and YOU and YOU!
1 Telehealth
Platform
2 Needs
Assessment
2021 GERIATRIC EDUCATION
3 Editorial: The
COVID-19
Pandemic
5 Sojourns
Leadership
NEEDS ASSESSMENT
Scholar
The Gateway Geriatric Education Center is requesting
7 Hindsight is 20/20
input regarding your needs and preferences related to
10 News at SLU
13 Live Discharge
geriatric education. Please complete the 2021 Geriatric
from Hospice
Care
Education Needs Assessment by following the link or
15 Interprofessional scan the QR code above. Your feedback is invaluable
Teamwork
for our planning. Thank you!
17 Keeping the Faith
19 GWEP Pivots to https://slu.az1.qualtrics.com/jfe/form/SV_eVcFCtQiAqRpDYF
Virtual Delivery
SLU
23 Circle of Friends©
25 CST Facilitator
Certification
27 Academic
GEMS
Approaches to
Enhance Health
Education
The ever-popular SLU GEMS booklet has been updated and
expanded to include the latest screening tools and mnemonics.
Order your copy now! Email us at aging@slu.edu.
2 Aging Successfully, Vol. XXX, No. 1 email: aging@slu.edu Questions? FAX: 314-977-3370
EDITORIAL
The COVID-19 Pandemic
During the last year, the COVID-19 with such syndromes as cognitive important that all persons over 60
pandemic totally changed the lives dysfunction (“brain fog”), loss of taste years are vaccinated as well as most
of older people. Obviously, COVID-19 and smell, dyspnea, a chronic cough, young persons. However, at present
selectively killed older headaches, recurrent getting the vaccine does not take away
persons, resulting in fever, joint and muscle the need to social distance and wear a
the USA in a one-year pain, depression, mask. As more strains of the corona
decrease in lifespan. and anxiety. These virus develop, it may be necessary to
In addition to the symptoms can still be regularly develop new versions of the
high mortality, both present for a year with vaccine, similar to the situation with
lockdown and fear about 20% being present influenza vaccinations.
of becoming infected at ten weeks and 2 to 5% The COVID-19 pandemic should be
has led to physical one year after having seen as a wake-up call for politicians
and social isolation of contracted the virus. and public health officials. Some
many older persons, Similar syndromes countries, such as Taiwan, Bhutan,
especially those in have been seen after and New Zealand, have demonstrated
residential facilities other viral syndromes, that early recognition of the pandemic
and nursing homes. such as infectious and rapid introduction of public health
John E. Morley, MB, BCh
Isolation for older mononucleosis. It is measures show that the devastating
persons results in essential that exercise outcomes of the pandemic could have
severe stress and loneliness. Loneliness programs and psychological been mitigated. The need for political
leads to depression and an increase in support are made available to leaders to use scientifically supported
cardiovascular disease. These result in persons following COVID-19 for the public health measures, such as mask
an increase in mortality. In retrospect, duration of their symptoms. It is wearing, and the expectation for the
the lockdown in the nursing homes also important to recognize that a public to do the same, is essential. It
which prohibited family visitors was subset of persons with COVID-19 can is also important that social media
clearly one of the great failures of have severe lung, kidney or cardiac education programs are developed.
social care. The lack of availability damage. This group is in need of These initiatives need to include
of personal protective equipment for specialized care. It is important that specific programs aimed to reduce
visitors was a major reason for this. health care professionals recognize the impact of “anti-vaxers” and “anti-
Secondly, hospitals sending infected the long COVID syndrome and are maskers.” Finally, design of nursing
persons to nursing homes before they not dismissive of patients with these homes and senior centers should be
had cleared the virus was a major complaints. There is a need for developed to allow avoidance of social
reason for the spread of COVID-19 in interprofessional “long COVID clinics” isolation.
the nursing home. that provide the necessary support for
Another major problem is the long these patients to fully recover.
COVID syndrome. It is characterized by A set of excellent COVID-19
a severe lack of energy (fatigue) along vaccines has been developed. It is
Questions? FAX: 314-977-3370 email: aging@slu.edu Aging Successfully, Vol. XXX, No. 1 3
Telehealth
(continued from page 1)
enhance the telehealth options for
and competencies of professionals
providing primary care. As a result,
we are working to expedite and
expand our original vision for the
platform. We hope to strengthen the
capacity of the geriatric workforce
to deliver services via telehealth. To
that end, we are nearing completion
of the first of the suite of programs
to be developed, including the
Rapid Geriatric Assessment (RGA),
Medicare Annual Wellness Visit,
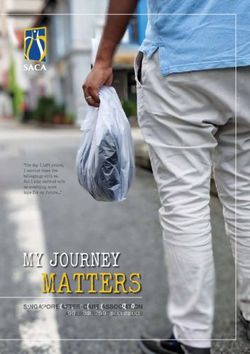
Figure 1.
and Cognitive Stimulation Therapy. year, CMS now allows the AWV to be question on FRAIL, they receive
Future plans include expanding delivered via telehealth. Our GWEP further questionnaires looking for
programs to address areas of care team previously incorporated the sleep apnea and depression and
that are specifically needed for older Rapid Geriatric Assessment (RGA) suggesting the measurement of a
persons, including the assessment into the Annual Wellness Visit and TSH and vitamin B12.
of and intervention in sleep apnea, has shown that this tool can be used Our second major undertaking
home care, and loneliness and as the basis for the AWV in the is the creation of virtual Cognitive
social isolation, all of which can be nursing home setting1. With support Stimulation Therapy (CST). As
identified through the RGA and/or from the CARES Act, we received regular readers of this newsletter
the Medicare Annual Wellness Visit. supplemental funding from the know, CST is a non-pharmacologic
This new Aging Successfully Health Resources and Services i n t e r ve n t i o n fo r p e r s o n s
platform provides a HIPAA- Administration (HRSA) to develop experiencing early and moderate
compliant environment with secure a computer-assisted version of the dementia2. In addition to enhancing
teleconferencing solution and Medicare Annual Wellness Visit. cognition, CST decreases depression
sophisticated data analysis. The Through our work with a technology and improves quality-of-life.
tools to quickly develop a HIPAA- development firm, we are creating Currently in the beta-testing phase,
compliant application with the a version that can be completed the Aging Successfully platform
teleconferencing component will by the patient and family on the includes a telehealth version of
enable providers and researchers computer at home, with or without CST that is delivered by Zoom.
to input, track, and analyze assistance. The program includes a Participants and facilitators will
data as well as track patients, variety of screening scales to assess connect via Zoom and have access
and medical and social service frailty (FRAIL and FRAIL-NH), to audio and video-based activities.
personnel’s involvement in group sarcopenia (SARC-F), anorexia The platform will also enable
activities. We are working with the (SNAQ), cognition (initial Rapid collection of demographic, pre-
technology development company Cognitive Screen (RCS) and annual and post-assessment data, session
to create content, field testing, and (RGY)), loneliness (ALONE), documentation, and evaluation data.
training for users to implement the quality of life (LIFEAD), depression
programs in practice settings. The References
(AMSAD), endocrine function 1. Little MO, Sanford AM, Malmstrom TK,
applications are designed to provide (ADAM), activities of daily living Traber C, Morley JE. Incorporation of
immediate benefit and, in the long- (ADLs), and what matters (Figure Medicare Annual Wellness visits into
the routine clinical care of nursing home
term, allow the company to use the 1). Depending on the response to residents. J Am Geriatr Soc 2020;Dec 18
collected data to create AI (artificial each item, further questions are doi: 10.111/jgs.16984 [Epub ahead of print].
intelligence) predictive models. posed which provide data to make 2. Berg-Weger M, Tebb S, Henderson-Kalb J,
With fewer than 25% of older a definitive diagnosis of the reason Zubatsky M, Lundy J, Hayden D. Cognitive
stimulation therapy: A tool for your practice
persons receiving the Medicare for the problem. For example, if the with persons with dementia? J Am Med Dir
Annual Wellness visit (AWV) each person responds “yes” to the fatigue Assoc 2015;16:795-796.
4 Aging Successfully , Vol. XXX, No. 1 email: aging@slu.edu Questions? FAX: 314-977-3370
Cara Wallace Named 2020 Sojourns Leadership Scholar by Cambia Health Foundation In January, Cambia Health cost of services through resource at North Carolina State University. Foundation announced their latest utilization.14-16 Though not formal mentors on the cohort of the Sojourns Scholar Well-suited to address long- Leadership Program. The goal of standing needs in the St. Louis the program includes “identifying, community, heightened due to cultivating and advancing the circumstances amid the COVID-19 next generation of palliative care pandemic, this project will address leaders” and provides scholars hospice misperceptions through a with funding for professional culturally relevant intervention. development and to carry out an Utilizing community engagement, award, Drs. John Morley and Marla innovative and impactful project project aims are to: create Berg-Weger, Co-Directors of The in the field of palliative care. educational/promotional materials Gateway Geriatric Education Cara L. Wallace, SLU Assistant about hospice using art and Center, express excitement about Professor in the School of Social narratives; distribute materials the possibilities of her project as “it Work and Geriatric Workforce with a targeted approach; and enhances our current community Enhancement Program-affiliated evaluate impact and community partnerships serving our local, faculty, was one of 12 scholars perception changes to hospice aging community.” selected across the U.S. Her care. Partnerships will include Dr. Wallace describes her project, building from her prior local organizations serving low- vision of leadership as defined work and guided by theory, is income, primarily by her roles “as to complete a social norms and African American a researcher, health education campaign to older adults, educator, and social reframe hospice among vulnerable community artists advocate,” but adds residents in St. Louis. creating mural that it is a “deep For the general public, hospice displays depicting passion to impact is associated with one word – hospice, and a the experience death.1,2 Even clinicians report videographer of palliative and confusion discerning hospice creating narrative end-of-life care in from palliative care, fear that stories of current meaningful ways.” discussing hospice will take away hospice patients She states, “As a hope, and discomfort and lack of and families. young hospice social training in effective end-of-life Dr. Wallace has worker, my patients conversations.3,4 Though hospice established a strong and families became use is growing, the median length team of local and my teachers and I of stay is only 24 days, and nearly national mentors quickly recognized one of three patients dies in a to enhance her the immense week.5 In addition to overarching project and ongoing value in barriers,1-4 cultural barriers development as a leader including hospice support at the end remain apparent6,7,8 and structural Dr. Patrick White, Division of life. I developed deep racism creates unequal access Chief of Palliative Medicine emotions surrounding the to resources causing ongoing at Washington University; Dr. type of death I want for health disparities.9 Obtaining Ricardo Wray, SLU Professor myself and for my loved timely access to EOL care is and Chair of the Department of ones. Years later when my important in improving quality of Behavioral Science and Health professional experiences death,10,11 symptom management,12 Education; and Dr. Karen Bullock, with death turned into bereavement for family,11,13 and Head of the School of Social Work (continued on page 6) Questions? FAX: 314-977-3370 email: aging@slu.edu Aging Successfully, Vol. XXX, No. 1 5

Wallace Named Sojourns Leadership Scholar
(continued from page 5)
personal ones,
I encountered Years later, when my professional experiences
first-hand some
of the challenges with death turned into personal ones, I
I witnessed as a
clinician. When I encountered first-hand some of the challenges
teach, my students
refer often to I witnessed as a clinician.
my ‘enthusiasm
and passion for
the material’ me to focus on the next stage of my Work End Life Palliative Care 7(1), 83-98.
doi:10.1080/15524256.2011.548048
and my ability to make ‘difficult career…and how I might contribute 8. Wallace CL (2017) Examining hospice
topics…interesting, applicable, to lasting change as a national leader enrollment through a novel lens: Decision
and relevant.’ This passion, along in the field of palliative care.” time. Palliat Supportive Care 15(2), 168-
Since the program’s inception in 175.
with my personal and professional 9. Yearby R (2018). Racial disparities in
experiences, channels my drive for 2014, Cambria Health Foundation health status and access to healthcare: the
my professional work.” has awarded 74 grants to emerging continuation of inequality in the United
The Sojourns Scholar Leadership leaders nationwide. Each grantee States due to structural racism. Am J Econ
Sociol 77(3-4), 1113-1152.
Program will allow Dr. Wallace is a member of an interdisciplinary 10. Teno JM, Clarridge BR, Casey V, Welch
to seek additional development palliative care team or is otherwise LC, Wetle T, Shield R, Mor V. (2007).
surrounding the application working to advance the field. Family perspectives on end-of-life care at
the last place of care. JAMA 291(1), 88-93.
of narrative intervention and Congratulations to Dr. Wallace! 11. Higgins PC, Prigerson HG. (2013).
implementation science within Caregiver evaluation of the quality of
palliative care, further preparing References: end-of-life care (CEQUEL) Scale: The
1. Andruccioli J, Montesi A, Raffaeli W, caregiver’s perception of patient care
her for national leadership. “As a near death. PLoS ONE, 8(6). doi: 10.1371/
Monterubbianesi MC, Turci P, Pittureri
social worker, my work is patient- C, Rossi AP. (2007). Illness awareness journal.pone.0066066
and family-centered and guided by of patients in hospice: psychological 12. Zhang B, Wright AA, Huskamp HA, et
the core values and ethics of the evaluation and perception of family al (2009). Health care costs in the last
members and medical staff. J Palliative week of life: associations with end-of-life
profession. My training enables 10(3), 741-748. doi:10.1089/jpm.2006.0200 conversations. Arch Int Med 169(5), 480-
me to approach situations through 2. Feeg VD, Elebiary H. (2005). Exploratory 488.
a systemic lens that considers study on end-of-life issues: barriers to 13. Wright AA, Zhang B, Ray A, et al.
(2008). Associations between end-of-
problems through the interaction palliative care and advance directives. Am
life discussions, patient mental health,
J Hosp Palliat Med 22(2), 119-124. doi:10.
of various forces – psychological, 1177/104990910502200207 medical care near death, and caregiver
social, economic, and political – and 3. De Vleminck A, Houttekier D, Pardon K, bereavement adjustment. JAMA 300(14),
1665-1673.
transactions between individuals et al. Barriers and facilitators for general
practitioners to engage in advance care 14. Taylor DH, Ostermann J, Van Houtven,
and their environment. Leaders CH, Tulsky JA, Steinhauser K. (2007).
planning: a systematic review. Scand J
must be able to both envision the Prim Health Care 2013, 31(4):215-226. What length of hospice use maximizes
larger context for the future of 4. Song MK, Dabbs ADV, Studer SM, & reduction in medical expenditures near
Arnold RM. (2009). Palliative care death in the US Medicare program? Soc
palliative care and consider Sci Med 65, 1466-1478.
referrals after lung transplantation in
individual roadblocks in the major transplant centers in the United 15. Kelley AS, Deb P, Du Q, Carlson MDA,
realization of that vision. As States. Crit Care Med 37(4), 1288-1292. Morrison RS (2013). Hospice enrollment
5. NHPCO. (2019). Hospice Facts and Figures. saves money for Medicare and improves
a clinician first, my research care quality across a number of different
Retrieved from https://www.nhpco.
is informed by clinical org/wp-content/uploads/2019/07/2018_ lengths-of-stay. Health Aff 32(3), 552-561.
practice and I am committed NHPCO_Facts_Figures.pdf doi: 10.1377/hlthaff.2012.0851
16. Gozalo PL, Miller SC, Intrator O, Barber
to providing translational 6. Chung K, Essex E, & Samson LF. (2008).
JP, Mor V. (2008). Hospice effect on
Ethnic variation in timing of hospice
research that directly impacts referral: Does having no informal government expenditures among nursing
care and services for patients caregiver matter? J Pall Med 11(3), 484- home residents. Health Serv Res 43(1),
134-153.
and families. Participation 491. doi: 10.1089/jpm.2007.0149
in this program will allow 7. Bullock K (2011). The influence of culture
on end-of-life decision making. J Soc
6 Aging Successfully, Vol. XXX, No. 1 email: aging@slu.edu Questions? FAX: 314-977-3370
H I N DSIGH T I S 20/20
Lessons Learned from Managing COVID-19 in the Nursing Home
By Angela M. Sanford, MD, CMD
I am the medical director of a 200-bed dually
certified skilled and long- term care nursing facility
in a large suburb. This nursing home has superb
leadership and a central core of faithful employees
that work well as a team to provide care to a
diverse patient population.
In March 2020, as we developed polices and put approach that does not enable success of minimizing viral
protocols in place to mitigate the effects of COVID-19, a spread. The next eight weeks went by in a blur with most
quiet hopefulness resided in several team members that of us working more hours than ever before. We struggled
maybe COVID wouldn’t “hit” our nursing facility. The with lack of resources, numerous employees walking off
rest of the team seemed to be bracing themselves for the of the job and not returning, and most of all, the loss of
inevitable and engaged in “watchful waiting.” our beloved patients who were members of our nursing
On the evening of May 1, my 10-year wedding home community. The virus was uncontainable without
anniversary, I received a call from the Director of Nursing the ability to test and isolate patients and staff in a timely,
(DON) about a patient residing in the locked dementia effective manner. Though we eventually gained free access
unit who had been sent to the emergency room earlier in to all of the testing supplies needed, the majority of cases
the day and incidentally tested positive for COVID. The and deaths occurred while we had limited resources. After
overwhelming sense of dread immediately set in, signaling the initial, massive COVID-19 outbreak, we had periods
that our fortitude, teamwork, and resilience were about to of “quiet,” followed by smaller outbreaks. The end result
be tested in ways unlike ever before. Our nursing home had was that COVID touched 150 of our 200 residents. After
been in full lock-down mode for nearly two months and introspecting and asking myself what could have been done
none of the patients from the dementia unit had been off the different and what I have learned, I have come up with the
unit or out of the building during that timeframe. We made following ten lessons:
a separate unit for dialysis and skilled rehabilitation patients 1. The lack of testing supplies and resources was the
to prevent those coming and going from the building from paramount reason for our failure of containment of the
bringing COVID back into the building. However, getting COVID-19 virus in the nursing home. In the weeks after
the news that one of the patients in the locked dementia our first case, the DON and administrator spent hours on
unit, where social isolation and masking is an impossibility the phone trying to locate more nasopharyngeal testing
and cohabitation is the norm, seemed incredulous. I called kits. They called the county health department and were
the emergency room physician and asked that he admit told that there was an outbreak in a local prison and that
the patient to the hospital until I could figure out a plan for they could only send us two nasopharyngeal testing kits
mass testing and isolation of those in the dementia unit who for the foreseeable future. When the DON called the state
were silently positive. Initially, I was told that the patient Department of Health and Senior Services, they sent
did not meet “inpatient criteria.” I must have sounded our nursing home 100 testing kits with a $50,000
desperate enough that he agreed to admit the patient to the bill because the state lab had no capabilities to bill
hospital while I worked with nursing home administration patient insurances. With no means to pay $50,000,
to implement a plan to stop the spread of COVID in our we reluctantly returned these testing kits. I felt like
dementia unit. I was being told subtly that the lives of my nursing home
The next day—a Saturday—we had an emergency residents did not matter. How was I to contain a virus (if
meeting of the nursing home leadership, infection control that is indeed possible?) if I could not test residents and
nurse, and several employees to lay out a plan. Unfortunately, test frequently—much less test the staff? In my nursing
we only had ten nasal pharyngeal testing kits in the facility. home community, staff undoubtedly unintentionally
The dementia unit had nearly 30 residents. Lack of testing brought the virus to our patients. In addition to lack of
supplies forced testing only symptomatic individuals, an (continued on page 8)
Questions? FAX: 314-977-3370 email: aging@slu.edu Aging Successfully , Vol. XXX, No. 1 7
HINDSIGHT (continued from page 7)
testing supplies, many other essential resources such as quality of life. I often referred to it as the “slow COVID
hand sanitizer, masks, latex gloves, etc., were all being death” and laid awake in bed many nights wondering
diverted to the hospital. We could not get any refills for what the best solution was. We were trying to “protect”
our wall hand sanitizers for several months because the our nursing home residents, but serious implications and
supplier diverted all units to hospitals. Again, a subtle negative consequences may have led to our “protection
reminder that the lives behind the walls of my building protocols” being more harmful. Especially in my facility
were less important than the lives elsewhere. Most where despite our best efforts, the majority of residents
assuredly, the lack of resources and testing supplies contracted COVID. I often ask myself, “Did the isolation
contributed to massive spread and uncontrollable save any lives? Was anything positive achieved? What
outbreaks in nursing homes across the country and this would my personal values be if my life expectancy was
was largely out of nursing homes’ control. very limited and I was a nursing home resident? What
2. The infection control guidelines from governing bodies are the rights of each nursing home resident and did
were unclear, difficult to decipher, and there was no we infringe on basic human rights?” For me, I believe
centralized leadership to guide struggling nursing homes. I would want to see my family and I would want to do
The wording in these documents was often very nebulous activities that contributed to my sense of purpose despite
and started with “You may want to consider…” When the potential risks of contracting COVID. I watched
one would call the governing body for clarification, the as several patients who were ambulatory to the dining
answers would vary depending on who was on the other room and around the facility before COVID became
end of the phone and answers were routinely divergent non-ambulatory and had a marked decline in functional
for the same question. Additionally, reporting measures status because of being confined to their small rooms for
were non-centralized, over-burdensome and incredibly so long. In the months and years to come, I foresee many
tedious. The DON at my nursing home cites this as the literature articles addressing the short-term and long-
number one cause of his frustration and burnout during term effects of social and physical isolation in nursing
the COVID epidemic. In addition to managing extremely home residents. It is my hope we can learn from this
high patient acuity, he was expected to report to as many research and are perhaps able to come up with innovative
as eight agencies each day, all of whom wanted slightly alternatives to complete “lock-downs.”
different information. Most nursing homes do not have 4. Families are essential in the care of nursing home residents
a dedicated information technology and were unable to see their loved ones at
department to assist with developing a time when their advocacy would have
centralized databases that would feed helped understaffed facilities the most.
these 8 different spreadsheets the With the absence of family from our
requested data, and thus the data was nursing home facility for more than one
manually inputted each day, requiring year now, I have learned just how much
hours of precious time away from we previously relied on their advocacy
patient care. to provide high-quality, whole person-
3. The social isolation from lockdown centered care. The information we
did as much damage as contracting routinely glean from families regarding
COVID-19 on the physical health the intricacies of their loved one’s life
and mental well-being of the nursing such as what that person’s favorite food
home residents. The deleterious is, what hobbies they had, or TV shows
effects of social isolation became they like, is invaluable and assists the
apparent nearly immediately in nursing facility in providing the degree
many of the nursing home residents. of personalized care that improves
The rates of depression, weight loss, quality of life. While transmission
and functional status decline soared of information can be done over the
as residents remained isolated to telephone, it seems to occur much
their rooms for months. I had and more frequently with in-person visits.
still have an ethical struggle with Important discussions regarding
the idea of confining people to their advanced care planning and functional/
rooms and severely impairing their (continued on page 9)
8 Aging Successfully, Vol. XXX, No. 1 email: aging@slu.edu Questions? FAX: 314-977-3370
HINDSIGHT (continued from page 8) cognitive decline are also more effective in-person at the When one team member was quarantined or on sick leave bedside. Not only do families improve the care delivered, during the pandemic, the effects across the community many nursing home residents were greatly felt. I remember find their sense of purpose in working in our COVID unit their families. Without family one day and noting that every visits, many patients lost their patient’s floor was sticky and sense of purpose, impairing the rooms were unkempt. After their will to live and ultimately, inquiring about what happened, passed away. as our facility is typically very 5. The COVID pandemic will have clean, I was told the dayshift long lasting effects on nursing house keeper had COVID home staff and has resulted in and was quite sick. I reflected the loss of many employees who that day on how essential each have left the field completely. person’s role was and how we all The nursing home I work at has work together in concert to keep a lower staff turnover rate than the facility functional. Nursing most facilities in our area, but homes present the idealistic several of our employees left model of cohesive teamwork their positions during the pandemic. Some had health when compared to other medical settings and are among co-morbidities and were fearful of working in a high-risk the most successful at providing true interdisciplinary environment while others needed to take care of children care. Each interdisciplinary team member sees the patient who were out of school. Many simply became burned through their own lens and plays a pivotal role in providing out from the long hours of working in an understaffed comprehensive, whole-person care. I saw a model of “all environment with very sick patients and decided to hands-on deck” during COVID where roles were less explore other options. One day, one of the residents living well defined and everyone chipped in to help other team in the dementia unit passed away from complications of members who were struggling to keep up and worked to COVID-19 and the routine dayshift nurse became very fill positions where staff were absent. Teamwork in the emotional after the resident died. When I saw her in the nursing home provided the quintessential backbone of hallway, she was crying and asked me how many more managing COVID in the nursing home. of her residents she must watch die. She then commented 7. The importance of self-care and caring for others on the about how she did not know how I could work in the team became paramount to mitigate the physical and hospital with sick patients dying of COVID. In the emotional effects of COVID on nursing home staff. We hospital, it is in some ways easier because we typically had many “huddles” to talk about our feelings regarding do not develop longitudinal relationships with patients what was happening around us and our responses and their families in the way that is commonplace in the to these events. To support staff, the nursing home nursing home. I have really begun to regard the nursing administration bought lunch on many days and provided home community as part of my extended family and feel us with snacks and bottles of water. We were also given a strong sense of personal responsibility for the good and matching t-shirts highlighting how healthcare workers bad outcomes. I imagine that many medical directors were “heroes.” Most days, though, I do not think staff must feel this way. The emotional toll from months of felt like heroes. I personally found it difficult to stress and watching nursing home residents become very compartmentalize my work and come home ill and die still pierces quite deeply for most nursing home and care for my small children without bringing employees. It has led to high rates of burnout, lack of staff my work home with me. With typical outlets for to resident engagement, and even higher rates of staff stress relief closed, (i.e., the gym, restaurants, coffee turnover. This leads to the question of how does a nursing shops, church) stress levels seemed to be sustained at an facility successfully provide high quality care with these all-time high. Fortunately, there was a true sense of “we staff shortages and what can be done to recruit more staff are in this together” and I could commiserate with our to the industry? DON, nurses, care partners, and even patients, and we 6. Teamwork in the nursing home has always been essential all understood the high emotional toll this was taking on and was noted to be even more crucial during COVID. (continued on page 12) Questions? FAX: 314-977-3370 email: aging@slu.edu Aging Successfully, Vol. XXX, No. 1 9

in the
NEWS at SLU
To address COVID-19 issues, Geriatric Workforce Julie Gammack, MD, is a recipient of
Enhancement Program Team members received the Pastoral Care Department of SSM
funding to address the impact of COVID-19 on older Health Saint Louis University Hospital’s
adults. These grants include: 2021 Caring Physician Award. Also
Marla Berg-Weger, PhD, LCSW, nominated is Lina Toledo-Franco. MD.
Executive Director, Gateway Geriatric Dr. Julie A.
Gammack
Education Center and John Morley, MB,
BCh, Professor Emeritus, Division of
Geriatric Medicine, received: Lina Toledo-Franco, MD, joined the
• A one-year supplement to the GWEP Division of Geriatric Medicine in August,
Dr. Marla
Berg-Weger grant to provide telehealth and dementia 2020 as an Assistant Professor. Dr.
care services. The funding, from the Toledo-Franco graduated from Pontificia
Health Services Resource Administration, provided Universidad Javeriana in Bogotá,
an additional $95,625 & $5,000, respectively. Dr. Toledo- Colombia in June 2003. She completed her
• Grant funds totaling $10,000 from The Saint Louis Franco residency and Geriatric Fellowship at Yale
University COVID-19 Rapid Response Seed Grant University School of Medicine (St. Raphael
to support a project entitled, Technology-Assisted Hospital) in June 2010. She returned home to Bogota
Intervention to Address Loneliness and Social Columbia before deciding she wanted to specialize
Isolation Among Older Adults. in Hospice and Palliative Medicine. Toledo-Franco
recently completed a one-year Fellowship in Hospice
GWEP Team member and Coordinator of the and Palliative Medicine at Saint Louis University.
university-wide Interprofessional Graduate Certificate
in Gerontology, Cara Wallace, PhD, LMSW, Max Zubatsky, PhD, LMFT, Department
APHSW-C, and MSW alumna and gerontology of Family & Community Medicine, Medical
certificate awardee, Liz Ricks-Ahearn, published Therapy Program Chair, and Marla Berg-
“Practice Considerations for Trauma-Informed Care Weger, PhD, LCSW, Executive Director,
at End of Life” in The Journal of Social Work in End- Gateway Geriatric Education Center were Dr. Max
of-Life and Palliative Care. They were also featured awarded two grants to help older adults Zubatsky
in The Playbook, a website launched by the Institute during the pandemic:
for Healthcare Improvement (IHI) and supported • St. Louis Community Foundation provided
by The Commonwealth Fund, The John A Hartford $13,989 for a project entitled, Behavioral Health
Foundation, and Robert Wood Johnson Foundation, Outreach for Underserved and Homebound Older
among others. Goals for the Playbook are “to improve Adults through COVID-19 to provide information
the health outcomes and daily lives of people in the and referrals to older adults during the pandemic’s
U.S. with the most complex care needs. early months.
• In partnership with the St. Louis Housing Authority
and the Association for Aging with Developmental
Marla Berg-Weger, PhD, LCSW, Professor,
Disabilities, the Saint Louis University Aging &
School of Social Work, and Executive Director,
Memory Clinic received $49,998 from the Regional
Gateway Geriatric Education Center has assumed
Health Commission to offer the evidence-based
the role of President of the National Association
intervention, Circle of Friends©, through virtual
of Geriatric Education. Berg-Weger was also
delivery.
named one of the Memory Care Home Solutions
Champion Awardees for 2020.
10 Aging Successfully, Vol. XXX, No. 1 email: aging@slu.edu Questions? FAX: 314-977-3370Angela Sanford, MD, CMD, Associate Division of Geriatric Medicine Welcomes New
Professor, Division of Geriatric Medicine, Fellowsysicians are completing fellowships in
is providing geriatric consultation to the the Division of Geriatric Medicine for specialized
Ahmed Eltarras, MD, completed
University of Missouri ECHO project fellowship training:
medical school at the Alexandria
specifically aimed at supporting longterm
University School of Medicine in Egypt,
Dr. Angela care facilities during the pandemic. This
Sanford ECHO program is a “learning hub” of over
where he grew up. He served as a
field physician in the Egyptian navy.
100 nursing homes who come together 3
Dr. Ahmed He completed his internal medicine
days a week (35 nursing home cohorts each day) for Elterras residency training at the American
16 weeks to discuss best COVID-19 management
strategies for nursing homes. Funded by the Health University of Beirut Medical Center. While in Lebanon,
Resource and Services Administration, the information Ahmed volunteered in medical campaigns helping
is valuable for all who work in care facilities and creates refugees. He was drawn to SLU’s geriatric program
a safe space for the different homes to discuss the by the educational opportunities, diverse patient
challenges they are facing. population, and the emphasis on wellness and
holistic patient care. After his geriatric fellowship, Dr.
Eltarras plans to complete a fellowship in cardiology
SLU Research Team Receives NIH Grant and subspecialize in geriatric cardiology.
to Study Live Discharge from Hospice
Care. Led by Cara Wallace, PhD, School Parneeta Bhatia, MD, graduated from the Grant
of Social Work, the interprofessional, inter- Government Medical College in Mumbai, India.
institutional team will be studying needs of She completed a residency in Anesthesiology at
Dr. Cara SLU and a fellowship in Critical Care Medicine and
Wallace patients’ post-hospice discharge and how
patients and their caregivers attempt to Anesthesiology at Barnes Jewish Hospital. Dr. Bhatia
meet those needs. For more information, visit Maggie also served as a physician at the John Cochran
Rotermund’s story on the project on page 13. Veterans Administration Medical Center in St. Louis.
SLU Geriatricians Recognized
BEST DOCTORS 2020
Congratulations to these Saint Louis University geriatric physicians who were recognized as Best Doctors of
2020. The Best Doctors list includes more than 1,000 physicians, chosen by their peers.
Dr. Gerald Mahon Dr. Christine K. Dr. Julie A. Dr. Angela Sanford
Jacobs Gammack
Questions? FAX: 314-977-3370 email: aging@slu.edu Aging Successfully, Vol. XXX, No. 1 11HINDSIGHT (continued from page 9)
each other. It was important to vaccines against COVID-19,
try and incorporate aspects of an end to COVID is finally
self-care in our daily routines in sight. As we look back in
because only when we were the rearview mirror, I am
nourishing ourselves, could hopeful that nursing home
we provide wholehearted communities will be able to
care to others. find some positive outcomes
8. The media portrayal of the from the pandemic.
management of COVID 10. The nursing home
in the nursing home was environment, despite all
often not accurate and did which was missing and in
not foster trust in the care the face of adversity, was at
being provided. Many news all times one of resilience
programs and newspaper and strength. When COVID
articles were quick to focus entered our buildings, we
on the deaths occurring from were working in the trenches
COVID in nursing home and still focused on providing
residents but did not dig the best care possible for
deeper into why there were the members of our nursing
so many deaths. Despite home communities. Most
nursing homes appearing on of us felt the residents were
the local and national news extensions of our families and
nightly as the deaths soared, we continued to come to work
the lack of testing supplies, day after day and care for
protective equipment and those who were sick and those
overall frailty of the nursing who were well. I saw so many
home population was rarely examples of commitment,
discussed in detail. Instead faithfulness, and selflessness.
of focusing on what critical roles the nursing homes There were countless instances of staff going above and
were playing in providing care to the most vulnerable beyond to provide personalized care for residents. They
population, nursing homes were portrayed in a very truly made a difference in these residents’ lives and
negative light and blamed for the widespread mortality. together, provided comfort, minimized suffering, and
The culture that was created from this biased reporting improved quality of life. Without the presence of families
did not boost nursing home staff morale or improve in the nursing home, staff have stepped up to become the
nursing homes’ reputations. residents’ surrogate families and be their voices. Never
9. There is hope in the vaccine. Given the natural course have I been prouder and more grateful to be a medical
of most viral pandemics and now that there are effective director of a nursing home.
SLU Geriatrics is always on the move. Keep up with us!
facebook.com/GatewayGEC
@GatewayGEC
@meddocslu
http://www.youtube.com/c/GatewayGeriatricEducationCenterstl
12 Aging Successfully, Vol. XXX, No. 1 email: aging@slu.edu Questions? FAX: 314-977-3370SLU Research Team Receives NIH Grant to Study Live Discharge from Hospice Care What happens to hospice patients who are discharged from care after their condition stabilizes? by Maggie Rotermund, Senior Media Relations Specialist, Saint Louis University A new study from Saint Louis University seeks to evaluate the health and quality of life outcomes for patients and caregivers following live discharge from hospice care. Cara Wallace, Ph.D., Assistant Professor in the School of Social Work, received a $427,276 grant from the National Institute of Nursing Research of the National Institutes of Health (NIH) to study the needs of patients post-hospice discharge and how patients and their caregivers attempt to meet those needs. Hospice care has been shown to improve end-of-life outcomes Hospice services may include survey will assess the quality of for adults with chronic illness, yet nurse and physician care; life, service utilization and health with eligibility limited, the system physical, occupational or speech status for adult patients and their is not set up to accommodate therapy; social services; nursing adult caregiver. The study will longer term needs. Eligibility aides, medical equipment and evaluate healthcare utilization for hospice requires a patient supplies; counseling; and short- and health status at time of live to forgo curative treatments for term inpatient services. Care discharge and following a live his or her terminal condition is available around the clock, in discharge; determine service and a physician to certify life the patient’s home and is focused patterns and the continuity of care expectancy of six months or less. on symptom management. transitions; and analyze patient Those adult patients who The six-month longitudinal and caregiver perspectives on stabilize, or have a change service coordination and in terminal prognosis, may potential impacts to quality be given a live discharge of life. from hospice care. “Without understanding In 2017, 6.7%, or nearly the impact of a live 90,000 hospice patients, were discharge, improving care discharged after they no longer and providing appropriate met eligibility requirements. support is impossible,” “Our study aims to find out Wallace said. “This is the what happens to the patient first step in developing a and the caregiver when the protocol to create effective patient outlives this prognosis The research team, from top left, includes Stephanie Wladkowski, live discharge standards.” and hospice services are Cara Wallace, Leslie Hinyard and Verna Hendricks-Ferguson, (continued on page 14) removed,” Wallace said. works via Zoom. Submitted photo. Questions? FAX: 314-977-3370 email: aging@slu.edu Aging Successfully, Vol. XXX, No. 1 13
presents the 2nd Annual
Dementia Friendly Healthcare and Community Virtual Symposium
Wednesday, June 16, 2021, 8:15 a.m. - 5:15 p.m. CT
FREE learning opportunities for providers, healthcare professionals, and community workers
Hear Keynote on Pros and Cons of Medications for Dementia
Connect with national experts on dementia care to learn about:
f Early Detection of Dementia f Training Providers for Caregiver Education f
f Cognitive Stimulation Therapy f
f Whole Person Dementia Assessment f Loneliness and Social Isolation f
Continuing Education Credits and Social Workers’ Education Credits applied for.
To pre-register
scan this QR code Questions?Email gunjan.manocha@und.edu
Live Discharge from Hospice
(continued from page 13)
The study participants will be supported by the deans
referred from hospice agencies of the College for Public
affiliated with the Greater St. Health and Social Justice,
Louis Hospice Organization, School of Medicine, SLU
a coalition of independent Center for Outcomes
agencies who meet regularly Research, Trudy Busch
to foster communication and Valentine School of
collaboration. Nursing, Doisy College
Co-investigators include Verna of Health Sciences, Parks
Hendricks-Ferguson, Ph.D., College of Engineering,
Irene Riddle Endowed Professor Aviation and Technology,
in the Trudy Busch Valentine the College of Arts and
School of Nursing; Leslie Hinyard, Ph.D., director Sciences and the Office of the Vice President for
of the Advanced HEAlth Data (AHEAD) Institute Research.
and chair of the Department of Health and Clinical For more information on referrals and registration,
Outcomes Research; and Stephanie Wladkowski, please visit: https://gatewayeol.com/refer-your-
Ph.D., associate professor of Social Work at Eastern patients-for-a-research-opportunity-the-impact-of-
Michigan University. live-discharge-from-hospice-on-patients-caregivers/
The partnership between Wallace and This study is supported by the National Institute of Nursing
Hendricks-Ferguson was initiated as part of SLU’s Research of the National Institutes of Health (NIH), 1R21
Interdisciplinary Health Sciences Research Grant NR017978-01A1. This article was reprinted with permission
Program. This SLU-sponsored program was of the author.
14 Aging Successfully, Vol. XXX, No. 1 email: aging@slu.edu Questions? FAX: 314-977-3370Interprofessional Teamwork: Improving Care for Older Adults By Devita T. Stallings, PhD, RN The Saint Louis University teams from Saint Louis University and advance the health of Division of Geriatric Medicine and and the University of Minnesota populations; Gateway Workforce Enhancement competed in the final inter- 3) Communicate with patients, Program (GWEP) held its 6th GWEP competition on Monday, families, communities and Annual Interprofessional Geriatric November 9, 2020. professionals in health and Case Competition. For this case Interprofessional practice other fields in a responsive competition, interprofessional is the hallmark of geriatric and responsible manner that student teams are tasked with care and allows students the supports a team approach to developing a plan of care for a opportunity to participate in a promotion and maintenance of complex geriatric patient that is collaborative experiential learning health and the prevention and presented to a panel of faculty opportunity that is essential for treatment of disease; judges from multiple universities their future practice. The geriatric 4) Apply relationship-building values and professions. Given the current case competition is based on and the principles of team COVID-19 pandemic, the annual the Interprofessional Education dynamics to perform effectively competition was transitioned to Collaborative core competencies for in different team roles a virtual event. An addition to interprofessional teamwork: to plan, deliver, and the 2020 case competition was a 1) Work with individuals of other evaluate patient/ collaboration with the Minnesota professions to maintain a population-centered Northstar Geriatric Workforce climate of mutual respect and care and population health Enhancement Program (GWEP) at shared values; programs and policies that are the University of Minnesota. The 2) Use the knowledge of one’s own safe, timely, efficient, effective, competition consisted of three role and that of other professions and equitable. parts: first, semi-final, and the to appropriately assess and For the case competition, final Inter-GWEP competition. address the healthcare needs students and faculty are The semi-final round winning of patients and to promote (continued on page 16) Questions? FAX: 314-977-3370 email: aging@slu.edu Aging Successfully, Vol. XXX, No. 1 15
Interprofessional Teamwork
(continued from page 15)
recruited to participate in a
month-long interprofessional
case competition. In teams of
3-4 students, a total of 26 teams
were comprised of undergraduate
and graduate students from
occupational therapy, physical
therapy, nursing, medicine,
social work, pharmacy, dentistry,
medical family therapy, speech
language and hearing sciences,
and communication sciences
and disorders. A faculty mentor/
coach is assigned to each team
for collaboration on the geriatric
case study that focused on the
development of a care plan for
an older patient with multiple,
chronic health conditions, including
COVID-19. The students created an
innovative 20-minute pre-recorded
electronic case presentation. The
case presentations were judged by
a team of interprofessional faculty.
The top-rated team from the semi-
final round at SLU and UMN The winning team from Saint Louis University’s semi-final round. Students included: Alake Brown
competed via a live zoom during School of Social Work, MSW student; Erin Dewberry, School of Social Work, MSW student; John
the Inter-GWEP. Hartman School of Medicine, 2nd year medical student; Sydney Rosenthal, School of Medicine,
Photos: For the inter-GWEP 2nd year medical student; Andrea Weile, School of Social Work, MSW student; Team Coach:
Susan Elliot, ANP, Division of Geriatric Medicine
competition, the University of
Minnesota’s student team received
the highest scores. The top team
was awarded a cash prize and each
of the members of the top two
teams received medallions for their
participation.
We would love to engage more
students from health professional
programs at SLU and
surrounding universities in
future case competitions.
For more information, contact
aging@slu.edu
References
1. Interprofessional Education Collaborative. The winning team from the University of Minnesota’s semi-final round and the winners of the
Core competencies for interprofessional final Inter-GWEP competition: Students included: Emily Feye, School of Nursing, adult health/
collaborative practice: 2016 update. Retrieved gerontological clinical nurse specialist student; Katherine Tyeryar, College of Liberal Arts, SLP
from https://ipecollaborative.org/Resources. student; Kelsi Johnson, Center for Allied Health Programs, OT student; Kendra Bollig, Center
html for Allied Health Programs, OT student; Team Coach: Lizzie Choma, PT, DPT, GCS.
16 Aging Successfully, Vol. XXX, No. 1 email: aging@slu.edu Questions? FAX: 314-977-3370Keeping the Faith
The Role of Spirituality in Older Adults with Memory Loss
By Max Zubatsky, PhD, LMFT
Eleanor (pseudonym of one saw each group members’ pictures. spirituality are often taboo to discuss
participant) was a spirited 77-year- When Eleanor showed her canvas, with their own family members
old member of our first she commented, “I and friends. When we went back
Cognitive Stimulation don’t know if this is and reviewed the literature on
Therapy (CST) group what you wanted, reminiscence interventions and
at SLU. She took so but it’s the most spirituality, we found very little that
much appreciation in important thing incorporated personal beliefs and
the little things in life, that’s gotten me faith into group
Photos taken from
even when her recall through rough days.” activities.3,4,5 Our the Lutheran
of recent events was Eleanor’s picture was research team Foundation Event
often compromised. of an angled, wooden quickly realized for Spiritual
During her time in an cross with a rosary that there was a CST at Saint
assisted living facility, draped over the significant gap Louis University
she was challenged side. The aesthetic that was missing in February of
2020. Samples of
not only with ongoing detail of the piece in group-based spiritual toolboxes
memory issues, but absolutely floored all i n t e r v e n t i o n s are seen on the
chronic pain in her of us. She recalled for adults with pedestals.
back due to past this image in her dementia.
surgeries. Eleanor’s sciatica caused mind from her mother’s old living In 2019, SLU received a grant from
her to have sharp pains while sitting room, where they would drape the Lutheran Foundation to study
for long periods. Yet, she had a different rosary beads from their the impact that spirituality played
wonderful attitude in the group and travels over a cross on the wall. She in cognition and memory for older
always provided a ray of sunshine regretted not having saved this after adults. Our research team partnered
for group members. Throughout the their move, but always remembers with Dolan Memory Homes and
entire protocol of CST sessions and the memories of their family and The SARAH Community to test
themes,1,2 the group bonded very the importance faith played through how Cognitive Stimulation Therapy
well and became a vital source of tough times. with a spiritual component could
support on Monday mornings. help improve areas of dementia
At our last in-person session, and health with this population.
we had a creative arts activity. The study showed that not only
Each person would get a small, was memory of participants
blank canvas and several improved from spirituality
pictures on the table to serve as incorporated in the groups, but
visual prompts. We also used overall mood and well-being
our large screen to show pictures as well. All group participants
of the past actors, trips, movies, across five CST groups also
songs, and other things that were completed a “spiritual
covered during the entire group toolkit,” which was a small
process of CST. Part of me was The takeaway from this CST box that members would
excited to see how they would use group session was profound. The continually add meaningful
different mediums of paint, pastel facilitators not only noticed how faith-based items to across the
and colored pencil on their canvases. powerful Eleanor’s piece was, study. Qualitative narratives were
Another part was terrified that but how the group engaged in a also collected from group members
our conference room walls could conversation about the meaning about their experiences in sharing
quickly turn into a representation of of faith in their lives. It sparked faith-based information and themes
Jackson Pollack. At the end of the further conversation amongst group during the sessions.
30-minute activity, the facilitators members about why religion and (continued on page 18)
Questions? FAX: 314-977-3370 email: aging@slu.edu Aging Successfully, Vol. XXX, No. 1 17Keeping the Faith
(continued from page 17)
The project was capped off by a malas, and
community event that was hosted statues.
by Saint Louis University. The As we
event highlighted several spiritual continue
toolboxes used by individuals in CST groups
the CST groups at all three sites. on virtual
Community partners and other platfor ms,
SLU students attended the event members
and could observe the creations have been
that CST participants made across able to report
the project. Narrative quotes and new areas of
summaries of sessions were also fa i t h a n d
posted for attendees to view at the belief during
event. Although the start of the C OV I D -19. their “virtual” community. Eleanor’s
COVID-19 pandemic interrupted Among th e m a n y themes and experience was a great example of
further in person sessions, conversations covered over the how powerful one’s belief system
individuals continued to share past y e a r, f a i t h continues to be can be in getting through life’s
their meaningful experiences with a popular a r e a f o r members most challenges circumstances.
facilitators through phone and to process. Participants are excited For more information, contact Dr.
ongoing virtual groups. to share small items and trinkets Max Zubatsky at the Saint Louis
The following are items and on Zoom to other members. Others University Aging & Memory Clinic:
belongings that participants in the may recall their week and highlight 314-977-9759 or memoryclinic@
spirituality group used in their the importance of staying connected health.slu.edu.
Spiritual Toolbox: virtually with their church,
References
• Poems- Writings that have been synagogue, mosque, or other faith 1. Spector, A., Thorgrimsen, L., Woods, B. O.
meaningful to them over the years organizations. Virtual adaptations B., Royan, L., Davies, S., Butterworth, M.,
• Hymns and scripture- Religious of CST are starting to occur across & Orrell, M. (2003). Efficacy of an evidence-
based cognitive stimulation therapy
songs or versus that inspire the world,6 where facilitators programme for people with dementia:
individuals in their coping around are continuing to recognize the randomised controlled trial. Br J Psychiatry,
memory loss and give them importance of reaching vulnerable 183(3), 248-254.
2. Spector, A., Orrell, M., & Woods, B. (2010).
perspectives in life adults with memory loss through
Cognitive Stimulation Therapy (CST):
• Old pictures: Helps to reminisce technological means. effects on different areas of cognitive
about events in peoples’ lives and Providers who work with older function for people with dementia. Int J
can help bring back stories in their adults with dementia and other Geriatr Psychiatry, 25(12), 1253-1258.
3. Elias, S. M. S. (2018). A review of spiritual
childhood and early adulthood. memory challenges should consider reminiscence therapy for older people with
• Candles-Used by participants how faith and spirituality play an mental health problems. In Proceedings of
during times of prayer or important role in patients’ lives. Global Public Health Conference (Vol. 1,
No. 1, pp. 27-36).
meditation in their home We often lose site of the spiritual 4. MacKinlay, E., & Trevitt, C. (2020). Spiritual
• Greeting Cards- Could be dimension of health when factoring factors in the experience of Alzheimer’s
general cards or holiday just biopsychosocial areas of disease and other Dementias. In Religion
cards that helped remind patients’ and caregivers’’ lives. and Theology: Breakthroughs in Research
and Practice (pp. 334-357). IGI Global.
individuals about their During COVID-19, we have seen 5. Smeaton, E., & Maher, C. (2016). Supporting
loved ones. many socially isolated individuals Spiritual Engagement for People Living
• Quotes-These often came from with memory loss issues who must with Dementia. Health and Social Care
Chaplaincy 4(2), 130-141.
books, readings, or notes that use any form of resiliency they can 6. Cheung, G., & Peri, K. (2020). Challenges
were collected by individuals to endure disconnection from the to dementia care during COVID-19:
over the years. outside world. Our group has seen innovations in remote delivery of group
cognitive stimulation therapy. Aging Ment
• Spiritual Items-Rosary beads, how powerful faith can be for many Health. 2020 Jul 7; 103. doi:10.1080/1360786
meditation bells, Hebrew dreidels, and what can be shared with others in 3.2020.1789945.
18 Aging Successfully, Vol. XXX, No. 1 email: aging@slu.edu Questions? FAX: 314-977-3370You can also read