BULLETIN Serving East Bay physicians since 1860 - March/April 2021 - Alameda-Contra Costa Medical Association
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

BULLETIN ALAMEDA-CONTRA COSTA MEDICAL ASSOCIATION Serving East Bay physicians since 1860 March/April 2021
YEARS
Health care you can count on.
Service you can trust.
www.alamedaalliance.org
BULLETIN
A
COS1T8 6 0MEDIC
A
AL
TR
DA–CON
ASSOCIATION
AME INC
ALAMEDA-CONTRA COSTA MEDICAL ASSOCIATION
71
R
18
AL O
PO .
R AT E D JA N
ACCMA EXECUTIVE COMMITTEE
Suparna Dutta, MD, President
Robert Edelman, MD, President-Elect
Edmon Soliman, MD, Secretary-
Treasurer
Katrina Peters, MD, MPH, Serving East Bay physicians since 1860 March/April 2021 | Vol. LXXVII, No. 2
Immediate Past President
COUNCILORS & CMA DELEGATES
Eric Chen, MD
5 YOUR IN YOUR
MEMBERSHIP COMMUNITIES
Rollington Ferguson, MD
Harshkumar Gohil, MD PRESIDENT'S PAGE
COVID Vaccines in Private
AT WORK
Russ Granich, MD
19
James Hanson, MD
Shakir Hyder, MD Practice are Long Overdue
Alexander Kao, MD
Irina Kolomey, MD
By Suparna Dutta, MD,
ACCMA President 8 #ThisIsOurShot for a
COVID-Free World
Arden Kwan, MD Become a Physician
Terence Lin, MD
Advocate
Lilia Lizano, MD
Abbas Mahdavi, MD IN YOUR 20
Ross Pirkle, MD
Jeffrey Poage, MD PRACTICE 9 Community Assessment
and Transport Team –
Stephen Post, MD Recent ACCMA Advocacy
Thomas Powers, MD
Richard Rabens, MD 7 Priorities Alameda County’s New
Comprehensive Crisis
Free PPE Direct Shipment
11 Response
Steven Rosenthal, MD
Katrina Saba, MD for California Physicians
Suresh Sachdeva, MD
Ahmed Sadiq, MD
and Medical Groups Commitment to Our
Jonathan Savell, MD
Edmon Soliman, MD
25
Communities Through
Climate Change Action 17
Judith Stanton, MD NEW MEMBERS
COVID-19 Vaccination
15
Clifford Wong, MD
CMA & AMA REPRESENTATIVES
Update for Employers
By Jamie M. Bossuat, Esq. Letter from CMA President 27
Patricia L. Austin, MD, AMA
By Peter Bretan, MD, Supporting Our Members
27
Delegate
Mark Kogan, MD, CMA Trustee, President, California Medical Through the COVID-19
AMA Alternate-Delegate Association Pandemic
Suparna Dutta, MD, AMA Alternate Superlative Customer By Scott Coffin, CEO,
Service – Key to Successful
23
Delegate (at Large)
Alameda Alliance for Health
Ronald Wyatt, Jr., MD, CMA Trustee Practice
MEMBERSHIP &
COMMUNICATIONS COMMITTEE
By Debra Phairas Supporting Physician
Health with On-Demand 30
Mark Kogan, MD, Chair Webinars COUNCIL REPORTS
Patricia Austin, MD
Sharon Drager, MD
Robert Edelman, MD 28 34
James Hanson, MD
The ACCMA Physician CLASSIFIEDS
Jeffrey Klingman, MD
Leadership Program
34
Stephen Larmore, MD
Terence Lin, MD By Hilary Worthen, MD,
Irene Lo, MD Course Director IN MEMORIAM
Lamont Paxton, MD
Katrina Peters, MD
Frank Staggers, Jr., MD
Ronald Wyatt, MD
ACCMA STAFF
Joseph Greaves, Executive Director
Mae Lum, Deputy Director
Griffin Rogers, Director, Napa &
Solano County Medical Societies
David Lopez, Assoc. Dir. of Advocacy
and Strategic Initiatives A
COS1T8 6 0MEDIC
A
Essence Hickman, Operations
ALAMEDA-CONTRA COSTA MEDICAL ASSOCIATION
AL
TR
DA–CON
ASSOCIATION
Associate
6230 Claremont Avenue, Oakland, CA 94618
Jennifer Mullins, Education and
AME
Tel: 510/654-5383 Fax: 510/654-8959 www.accma.org
INC
71
R
Events Associate
18
AL O
PO .
R AT E D JA N
Angelina Perez, Executive Assistant
Hannah Robbins, Policy Associate
REDUCE – REUSE – RECYCLE
Printed in the U.S.A. with soy inks on paper stock certified by the Forest Stewardship Council.
ACCMA BULLETIN | MARCH/APRIL 2021 3
The Pediatric Colorectal Center
NEWS & UPDATES
at Shriners Hospitals for Children — Northern California
Advanced Pediatric
Colorectal and Motility Care
Shriners Hospitals for Children — Northern California is a California Children’s Services designated Special Care Center
for colorectal and urology care. Our Pediatric Colorectal Center brings together specialists to evaluate, diagnose and
solve colorectal health issues, including:
» Anorectal malformations » Encopresis » Pseudo-obstruction
(imperforate anus)
» Fecal incontinence » Rectal prolapse
» Bladder extrophy
» Hirschsprung disease » Rectal trauma
» Caudal regression syndrome/
sacral agenesis » Idiopathic constipation » Spina bifida
» Chronic constipation » Megacolon » VATER/VACTERL association
» Cloaca/cloacal anomaly » Neurogenic bladder
» Cloacal extrophy » Neurogenic bowel
To learn more visit, https://bit.ly/3hclCX5.
To refer a patient: Call: 916-453-2191 Fax: 916-453-2394 Email: referrals.ncal@shrinenet.org
PRESIDENT'S PAGE
President’s Page: COVID
Vaccines in Private Practice are
Long Overdue
By Suparna Dutta, ACCMA President
A lthough the ACCMA Council does not typically meet in
April, we held a special meeting this month to hear from
Dustin Corcoran, CEO of the California Medical Association
vaccination strategy. CMA’s priorities include advocating for
a more streamlined, less bureaucratic enrollment process for
independent practices; reducing the quantity for minimum orders;
(CMA), about the state’s vaccination efforts. CMA has been increasing reimbursement rates for vaccination administration;
working with the State of California and the designated third- and many other technical, practical issues. Mr. Corcoran noted
party administrator (TPA) for vaccine distribution, Blue Shield of that CMA and county medical associations (including ACCMA)
California, to expand the distribution of vaccines to independent are even willing to commit staff time and resources to help
physician practices and other providers who have thus far been onboard more practices. Stay tuned for more info.
left out of the state’s distribution efforts. Dr. Peter Bretan, CMA The inclusion of independent practices in the State’s
President, recently sent a letter to members outlining CMA’s vaccination efforts is critical for achieving health equity. Patients
advocacy efforts around vaccine distribution in California – you who are hesitant about getting vaccinated may be more receptive
can read the full letter on page 15. after consulting with a physician they know and trust. Ideally, if
Some ACCMA members have gone through painstaking possible, they should get a shot right then and there. Referring
efforts to enroll with the state to administer vaccinations. In some patients to another location creates an unnecessary barrier.
cases, they have done so on different occasions and in different To be clear, the efforts to vaccinate our community to date
iterations as the state’s enrollment system has “evolved.” They – by the counties, health systems, community clinics, federal and
have invested in purchasing capital equipment to safely store and state partners, community-based organizations, and others – have
administer vaccines. But, as of press time, these members are been truly impressive and inspiring. But these mass vaccination
continuing to wait without a clear timeline. clinics do not work for everyone. Some require the use of a
Getting into the queue is not easy. According to the state computer with internet to register for an appointment and/or a
website (https://eziz.org/covid/enrollment), a practice must vehicle to access the clinic, making it challenging for patients who
first enroll in a local vaccine registry and myCAvax, sign a TPA do not have or are unable to utilize these tools. Giving patients the
contract with Blue Shield, prepare the site/clinic in accordance opportunity to get vaccinated from their trusted physician at their
with requirements, and train staff. Once they get through all of doctor’s office will help ensure more shots get into the arms of
these steps, they then need to enroll and train their staff in using patients who need them.
the MyTurn/MyClinic system, which they are required to use We are hopeful that these issues will be resolved soon. With
to manage COVID vaccination appointments and reporting eligibility now expanded to everyone over the age of 16, the
requirements. Of course, integrating a separate scheduling and inclusion of independent practices is a vital step in ensuring all
reporting system will come with its own challenges. communities within our counties have easy, timely access to the
To simplify this process, CMA is meeting frequently with vaccine. This will allow physicians to provide the high-quality
the state, Blue Shield, and others in an effort to lower barriers medical care their patients expect.
and ensure that independent practices are part of the State’s
Explore ACCMA Volunteer Opportunities! Visit ACCMA.org/Volunteer,
or call ACCMA at (510) 654-5383 to find out more.
ACCMA BULLETIN | MARCH/APRIL 2021 5
HEALTHY CHECKOUT
PPE Relief
The California Medical Association partnered with local county medical
societies and the Office of Emergency Services to deliver over 100 million
pieces of personal protective equipment (PPE) to California physicians from
August through December 2020.
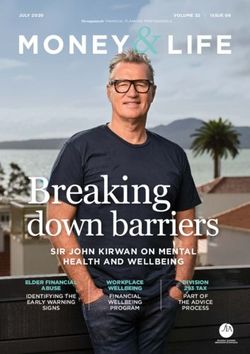
PPE Distributed to Date: 100+ Million Pieces
21 Million 2.5 Million 400,000 35 Million
N95 Face Hooded Examination
Respirators Shields Coveralls Gloves
2.3 Million 35 Million 3 Million 700,000
Isolation Surgical Sanitizing Sanitizer
Gowns Masks Wipes Bottles
Total Value to Practices: $200+ Million
To learn more about CMA’s PPE Relief efforts, visit cmadocs.org.
Distribution is ongoing and these numbers are accurate as of January 1, 2021.PPE FOR PHYSICIANS
Free PPE Direct Shipment for California
Physicians and Medical Groups
A CCMA and the California Medical Association (CMA)
are extending its distribution of free personal protective
equipment (PPE) with direct shipment of supplies to California
coveralls, 21 million N95 respirators, 3 million sanitizing wipes
and 700,000 sanitizer bottles.
“Receiving PPE by way of the ACCMA was indispensable to
physicians. my practice during the early days of the pandemic,” said Oakland
The new online portal (ppereliefdirect.org) offers California cardiologist Rollington Ferguson, MD. “We tried to order PPE
physicians the ability to register for specific types of PPE including through our usual vendors, who basically stated that we could
coveralls, face shields, goggles, hand sanitizer, sanitizing wipes, not get PPE because of the small volume purchasing power of
isolation gowns, N95 masks, surgical masks, and vinyl gloves. our practice. I then contacted the hospital where I am on staff in
The PPE is free, and the medical practice pays a nominal cost for the city of Oakland, hoping that they might be able to help with
shipping and handling. PPE. I was told that there was nothing they could do because of
CMA distributed over 100 million pieces of PPE to a conflict of interest. As you may recall, during those early days
physicians and medical groups from August 1 to December of the pandemic in 2020, PPE was difficult to come by even for
31, 2020. (See infographic on opposite page.) The donations hospitals.”
supported approximately 100,000 California physicians and their Doctor Ferguson continued, “In fact, we were reusing
staff, which represented a total value of more than $200 million. N95 masks, even in the hospital setting. Then, like manna from
“Lack of PPE throughout the COVID-19 pandemic heaven, ACCMA and CMA were able to provide private practice
has compounded hardships for medical practices and hindered physicians like me with PPE—thus helping to keep my staff and
physicians’ ability to serve patients,” said CMA President Peter patients protected during one of the most trying periods for the
N. Bretan, Jr., MD. “We knew we had to act – and fast – to medical profession. Thank you, ACCMA and CMA!”
help physicians keep their practices open. What resulted was “It was a welcome relief to be able to receive, through the
an unprecedented effort in the organization’s 165-year history. efforts of the ACCMA, a large and valuable supply of PPE in
CMA is grateful to our partners for their collaboration and the early days of the COVID-19 pandemic,” said Castro Valley
support, which ultimately helped so many Californians continue ophthalmologist Robert Edelman, MD. “Supply shortages due to
to receive health care.” high demand made it difficult to acquire PPE by any means. There
Last summer, CMA partnered with local county medical was a valid concern that I and other physicians would not be able
societies to develop an entirely new statewide distribution system to safely care for patients. The supply of PPE that the ACCMA
for essential medical equipment, which included PPE donations provided without charge provided an important lifeline for the
from the Office of Emergency Services (OES). Within weeks, survival of our medical practices during those days of crisis.”
PPE was being moved from state warehouses, repackaged into The lessons learned during the PPE distribution effort will
individual boxes, and loaded on trucks to be handed out at drive- be applied to helping the state build its vaccination network. “The
through events across the state. In Alameda and Contra Costa administration of COVID-19 vaccines brings hope into focus, but
counties, the ACCMA distributed a two-month supply of PPE the global pandemic remains challenging,” said CMA President
to East Bay physicians in late July and early August 2020, totaling Doctor Bretan. “Equity and speed remain vital components of
over $3.4M and reaching 522 private medical practices, at no any successful vaccination strategy, and we cannot compromise
charge to them. one for the other. The lessons learned distributing PPE will guide
After these drive-through events, physicians and medical CMA as we help the state build out their robust vaccination
practices continued to access free PPE through CMA’s online network connected to community physicians that millions of
request portal, paying only a nominal fee. Californians already rely on for flu shots and routine vaccinations.”
As of December 31, 2020, the effort has distributed a For more information about our PPE Relief program, contact
combination of 35 million masks, 35 million sets of gloves, 2.3 the ACCMA at accma@accma.org or (510) 654-5383.
million isolation gowns, 2.5 million face shields, 400,000 hooded
ACCMA BULLETIN | MARCH/APRIL 2021 7BECOME A PHYSICIAN ADVOCATE
Become a Physician Advocate
ACCMA LEADERSHIP AND LEGISLATIVE OPPORTUNITIES
B ecome a physician advocate in your community by working
with the Alameda-Contra Costa Medical Association
(ACCMA) and the California Medical Association (CMA) to
and Quality of Care Committee, and more. To read more
about the ACCMA committees and the nomination process,
visit accma.org/Leadership/ACCMA-Committees.
improve health care and aid the medical profession. Advocacy • Join your colleagues at our annual Legislative
gives physicians the opportunity to lobby for policy issues and Day. The 47th CMA Legislative Advocacy Conference took
laws to make the health care system better for all patients. The place from Monday, April 5 to Friday, April 9. CMA’s
ACCMA makes it easy for members to get involved with health Legislative Advocacy Day usually hosts more than 400
care policy and community projects. Here’s how you can become California physicians, medical students, and CMA Alliance
an advocate: members from all over the state as they lobby legislative
• Attend meetings with elected officials (https://bit. leaders in Sacramento on priority health care issues, but this
ly/3fwjqeq). These meetings, which are open to all ACCMA year it was all virtual. CMA Legislative Advocacy Day takes
members, provide ACCMA members an opportunity to place yearly, so if you are interested in joining next year’s
attend in-district meetings with local, state, and federal event, please contact Mr. David Lopez, Associate Director of
legislators to discuss pertinent issues affecting the health care Advocacy and Strategic Initiatives, at dlopez@accma.org or
community (see page 9 to read more about recent meetings (510) 654-5383.
with legislators).
• Join the ACCMA Legislative Committee – the Whether you have years of training in health care policy or
Legislative Committee conducts political action on behalf no experience at all, ACCMA invites all members to get involved!
of the ACCMA, meets with elected officials (https://bit. Visit www.accma.org/GetInvolved to find out more about
ly/3fwjqeq) to advocate for legislation and policy changes, ACCMA Committees, CMA Legislative Advocacy Day, meeting
evaluates candidates for local, state and federal offices with local legislators, and other ways to become a physician
representing this community, and makes recommendations advocate. If you are interested in getting involved or have any
to the ACCMA’s and CMA’s political action committees. questions, you can also contact Mr. David Lopez, Associate
Already in 2021, the ACCMA Legislative Committee has Director of Advocacy and Strategic Initiatives, at dlopez@accma.
coordinate meetings with multiple Assemblymembers org or (510) 654-5383.
and Senators (see the sidebar below for a complete list of
meetings this year). While these meetings are coordinated by
the ACCMA Legislative Committee, most of the meetings
with legislators are open to all members of the ACCMA. Visit 2021 MEETINGS WITH
https://bit.ly/2PdV7XX for more information. LEGISLATORS
• ACCMA committees are the workshops of the association
Senator Steve Glazer (D – 7th District)
and are responsible for developing many of the ACCMA’s
Senator Nancy Skinner (D – 9th District)
policies and programs that assist physicians and improve
Senator Bob Wieckowski (D – 10th District)
the quality of medical care in our community. Over 300 Assemblymember Rebecca Bauer-Kahan
ACCMA members currently serve on ACCMA committees. (D – 16th District)
In addition to the Legislative Committee, members can Assemblymember Rob Bonta (D – 18th District)
be nominated for the Advisory Committee on Physician Assemblymember Alex Lee (D – 25th District)
Wellbeing, the Community Health Committee, the Assemblymember Bill Quirk (D – 20th District)
Continuing Medical Education (CME) Committee, the Assemblymember Buffy Wicks (D – 15th District)
Emergency Committee, the Medical Services, Technology,
8 ALAMEDA-CONTRA COSTA MEDICAL ASSOCIATION BULLETINADVOCACY PRIORITIES
Recent ACCMA Advocacy Priorities
I n 2021, the ACCMA has already met with several legislators
during ongoing meetings throughout the year as well as on
Legislative Advocacy. The issues of focus so far this year have
establishment of a patient telehealth bill of rights would ensure
that patients can continue to receive appropriate and adequate f
ollow-up care after their DTC telehealth appointment and would
included AB 454, AB 457, SB 242, SB 250, and AB 1400. These prevent unnecessary emergency room visits, as DTC telehealth
issues and recommended positions are summarized below. services often refer patients to the ER for follow-up services.
SUPPORT: AB 454 (RODRIGUEZ) SUPPORT: SB 242 (NEWMAN)
This bill that would require medical plans and insurers to SB 242 by Senator Newman will support patients and providers
support their provider network, and improve access to care by requiring Health plans, insurers and the Department of Health
for their members, during a public health emergency. AB Care Services (DHCS) provide reasonable reimbursement for
454 would require supplemental payments to physicians, mandated PPE and supplies. SB 242 will ensure plans fulfill their
as well as implement a requirement to reimburse obligation to protect patients by working with providers who have
for unexpected additional costs to practices from the been struggling during this pandemic to identify an appropriate
pandemic, such as increased PPE and infection control share of costs in PPE and testing. This bill aides community
costs. This bill will ensure that patients continue to have access providers who are struggling to remain open and provide services
to care by using premiums to stabilize and protect provider to patients who desperately need the care.
networks. During the COVID pandemic, physicians in all CMA supports this bill because SB 242 requirements are
modes of practices and specialties have struggled financially. In specific to complying with public health orders during a public
a recent survey conducted by the California Medical Association health emergency for the duration of the emergency, and calls for
(CMA), 87% of physician practice are still worried about their a reasonable reimbursement negotiated between the plans and
financial health. Even with more than 8 out of 10 practices providers for the costs of PPE and testing. Health plans also have
now utilizing telehealth, the average volume of patient visits and an obligation to their members to maintain adequate networks
practice revenue is still down by one third, with 25% of practices and network adequacy suffers when providers are unable to
still experiencing a revenue decline of 50% or greater. On top provide services. Finally, health plans have a shared responsibility
of revenue decreases, practice costs have increased by 14% due in ensuring physician practices remain open and not forced
to COVID-19 pandemic expenditures (e.g., PPE, disinfecting to choose between cutting hours of operation and services or
procedures, implementation of telehealth, pre-visit screening, acquiring necessary PPE.
etc.), adding to the financial distress practices are experiencing. AB
454 would help protect physicians from shouldering the full SUPPORT: SB 250 (PAN)
financial burden that has come with the COVID-19 pandemic. Senate Bill 250 works within the current construct of plans’
and insurers’ utilization management process and streamlines
SUPPORT: AB 457 (SANTIAGO) the system by using data they already maintain. The bill would
This bill would create a patients’ telehealth bill of rights which relieve physicians who have a proven track record of appropriate
would protect the physician-patient relationship, provider for utilization from having to file prior authorizations for a period
better integration of care, and ensure that patients continue to of two years. At the end of that two-year period, a health plan or
enjoy existing protections. AB 457 will enhance the continuity of insurer may audit the physician’s utilization record for the previous
care for patients who have been seen by a third-party provider or two years to determine if they still qualify for this status. If they
a direct-to-consumer provider (DTC) via telehealth. This would do quality, the physician continues with no prior authorization
allow for the patient’s primary care provider (PCP) to receive requirements; if they do not qualify, the physician must return to
medical records from the DTC provider telehealth visit. The practicing with traditional prior authorization requirements. This
goal of the bill is not to remove access to direct-to-consumer approach is balanced and works within the existing structure of
telehealth, but rather to ensure that they are good players in the utilization management so as not to cause undue disruption.
market and to preserve continuity of care after the visit. The continued on page 11
ACCMA BULLETIN | MARCH/APRIL 2021 9ADVOCACY PRIORITIES (continued from page 9)
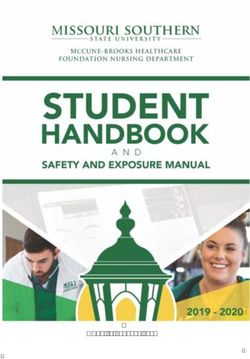
COVID-19 VACCINE CONVERSATIONS
TOP 5 MESSAGES
SAFETY
The vaccine will help protect you from getting sick from COVID.
Millions of Americans have been safely vaccinated and are now
protected against COVID.
SIDE EFFECTS
Side effects are common. They are a sign your body is activating
to protect you. For a few days after vaccination, many people feel:
1. Sore arm (near site of shot)
2. Tired or fatigue
3. Headache
4. Muscle pain
5. Joint pain
EFFECTIVENESS AND CHOICE
The best vaccine of them all? The one you can get first! Each
vaccine is 100% effective in saving your life from COVID! It will
allow us to get back to the things we love and miss. (Avoid
mentioning “normal”).
SPEED
Health experts took all the necessary steps to produce a safe
vaccine. It was built on 20 years of research and science.
? QUESTIONS?
It’s good to be careful when new things come along. We are glad
you want to know more. Ultimately, the choice is yours to get it
now, later, or not at all. Talk with your doctor or healthcare provider
to discuss if it is right for you. Visit getvaccineanswers.org and
greaterthancovid.org/theconversation for more information.
Help spread the truth about COVID vaccines.
#ThisIsOurShot ThisIsOurShot2021 ThisIsOurShot www.thisisourshot.infoCLEAN AIR STANDARDS
ACCMA Sends Letter in Support of
Clean Air Standards
T he ACCMA has recently taken a number of actions related
to climate change and the health of our communities. At
their meeting on February 3, 2021, the Community Health
send a letter urging BAAQMD to fulfill its mission to protect
health by continuing to adopt policies that focus on patient health
by reducing PM2.5 emissions. The letter on page 12 was sent to Mr.
Committee received presentations about climate change and its David Joe, Assistant Manager of the Rule Development Section at
impact on health. One of the presentations included information the Bay Area Air Quality Management District (BAAQMD.)
about a rulemaking process that is underway by the Bay Area Air In addition to the letter sent to BAAQMD, the ACCMA/
Quality Management District (BAAQMD), which is developing District IX Delegation recently considered multiple climate
draft amendments to Regulation 6: Particulate Matter, Rule change-related resolutions as part of the California Medical
5: Particulate Emissions from Petroleum Refinery Fluidized Association (CMA) Quarter 2 resolution process. The
Catalytic Cracking Units. The purpose of these amendments is to Delegation developed feedback for CMA regarding the climate
address emissions of particulate matter from petroleum refinery change resolutions, specifically noting that, while ACCMA
fluidized catalytic cracking units, which are some of the largest recognizes the threat of climate change, ACCMA leadership and
individual sources of particulate matter emissions in the San the District IX Delegation encourage CMA to focus any new
Francisco Bay Area (visit https://bit.ly/2PM80s8 for rulemaking policy specifically on the health impacts of climate change. While
documents). the Delegation generally supported CMA utilizing advocacy
Following the presentation, a motion was made to send a letter resources to prioritize climate change as a health issue, the
supporting a requirement for East Bay refineries to expeditiously Delegation also recognized the need to give these complex issues
implement the Best Available Retrofit Control Technology more consideration and thus encouraged the development of a
(BARCT) and any and all other measures to reduce the particulate Technical Advisory Committee that could focus on actionable
matter (and especially PM2.5) burden in our communities strategies related to climate change. A copy of the full ACCMA/
The Committee agreed to recommend that the ACCMA District IX Delegation testimony can be found on page 13.
ADVOCACY PRIORITIES (continued from page 9)
SB 250 would also alleviate the burden of collecting patient This issue has become an increasing problem as high deductible
cost-sharing amounts by hospital-based physicians. The bill products become more common. By shifting the responsibility of
would streamline the billing process by requiring payors to collections to the parties in contract, the bill streamlines the billing
collect patient cost-sharing amounts directly. Many hospital- process and alleviates the collection burden for physicians, while
based physicians spend significant staff and economic resources maintaining patient protections regarding medical billing that
to collect the copays and deductibles from the patient directly, currently exist in statute.
while not receiving a full payment for their services from the
health plan. Practices should be worried about the provision For questions about ACCMA advocacy, contact David
of care, not collecting on the cost-sharing agreement between Lopez, ACCMA Associate Director of Advocacy and
the payor and the purchaser. Thus, this issue is a burden in two Strategic Initiatives, by emailing dlopez@accma.org or calling
places, tying up practice resources in collection, and preventing 510-654-5383.
physicians from receiving full payment for services rendered.
Join the ACCMA at www.accma.org/membership/join-now
ACCMA BULLETIN | MARCH/APRIL 2021 11ACCMA LETTERS (continued from page 11)
David Joe
Assistant Manager of the Rule Development Section
Bay Area Air Quality Management District
375 Beale Street, Suite 600
San Francisco, CA 94105
Dear Mr. Joe,
The Alameda-Contra Costa Medical Association (ACCMA), representing over 5,000 East Bay physicians, is concerned
about the negative health impacts that particulate matter (PM), especially PM2.5, has on our patients and community.PM2.5 is
hazardous to health; it is linked to lung damage, asthma, heart disease, cancer, adverse birth outcomes, cognitive impairment,
and premature death along with increases in hospitalization, emergency department visits, and lost days of work and school.1
Evidence shows that even with small increases in chronic PM2.5 exposure, which is known to be emitted in substantial quantities
from refineries, there is an associated 8% increase in county-level COVID-19 mortality rates after accounting for many area-
level confounders.2
The California Environmental Protection Agency, World Health Organization, and other institutions have specified that
there is no clear lower limit of safe levels of exposure to PM2.5 particles, suggesting that current federal regulatory standards
for PM2.5 may not be adequate to protect public health. An estimated 2,000-3,000 lives are lost in the Bay Area each year from
PM2.5.3 In addition, the health impacts of PM2.5 exacerbate existing racial- and socioeconomic-associated health disparities and
disproportionately impact residents living in close proximity to refineries4, who already experience some of the worst health
outcomes in our community.
As medical professionals who care for vulnerable and at-risk populations, including babies, children, young adults, and
the elderly throughout the East Bay, we urge BAAQMD to protect the health of our patients and our community by requiring
refineries to take steps to meaningfully and substantially reduce PM2.5 emissions.
If you have any questions or wish to discuss these concerns, please contact Joseph Greaves, ACCMA Executive Director, at
510-654-5383 or jgreaves@accma.org.
Sincerely,
Suparna Dutta, MD
ACCMA President
1. https://ww2.arb.ca.gov/resources/inhalable-particulate-matter-and-health
2. Wu, X., et al., 2020. Air pollution and COVID-19 mortality in the United States: Strengths and limitations of an ecologicalregression analysis. Science
advances, 6(45), p.eabd4049.
3. https://www.baaqmd.gov/~/media/files/planning-and-research/research-and-modeling/cost-analysis-of-fine-particulate-matterin-the-bay-area.pdf.
4. https://www.baaqmd.gov/~/media/files/board-of-directors/2020/ssc_presentations_12172020v2-pdf.pdf?la=en.
Put Your ACCMA Membership to Work! Go to www.accma.org
> Membership, or call ACCMA at (510) 654-5383 for help.
12 ALAMEDA-CONTRA COSTA MEDICAL ASSOCIATION BULLETINACCMA LETTERS (continued)
Dear Doctor Jacobson and Members of the CMA Council on Science and Public Health,
The District IX/Alameda-Contra Costa Medical Association (ACCMA) Delegation met on Tuesday, March 9, to discuss the
California Medical Association (CMA) Quarter 2 Resolutions addressing climate change and would like to offer the following
testimony:
The ACCMA represents over 5,000 members and, accordingly, we have a broad range of opinions on issues related to
climate change, which is reflected within our Delegation. Our Delegation was, however, unanimously supportive of Resolution
108-20 and supports CMA utilizing its advocacy resources to highlight the substantial public health impacts of climate change,
prioritizing general advocacy on climate change, and including climate change as a focus within medical education. Importantly,
the Delegation appreciates that Resolution 108-20 is focused principally on health and healthcare, and we believe that CMA
advocacy on climate change should principally be focused on issues that are germane to CMA’s mission as a professional
medical association.
The Delegation is also unanimously supportive of Resolution 109-21. Climate change is a wide-ranging issue with many
facets, many of which are extremely technically complex and may not be germane to CMA’s focus on medical and professional
issues. We believe a Technical Advisory Committee would be beneficial in giving ample consideration to these complexities and
helping to identify specific and actionable strategies that are appropriate for CMA advocacy.
In regards to Resolutions 106-20 and 110-20, the Delegation recommends that these two resolutions be combined to
create a unified policy supporting the phasing out of desflurane and limiting nitrous oxide use in healthcare settings. Out of
the two resolutions, the Delegation favors the more focused approach of 106-20 but recommends it be adapted to include
provisions for other health practitioners and not be restricted to physicians. The Delegation also agreed that any CMA policy
regarding desflurane and nitrous oxide should be focused on healthcare and other settings that are germane to medical practice
and should not comment on their usage in culinary and other non-healthcare settings.
When considering Resolution 101-20, the Delegation acknowledged that carbon taxes are considered by many to be an
effective strategy for reducing greenhouse gas emissions, but the Delegation was uncertain about the extent to which CMA
should weigh in given physicians’ lack of expertise on the subject. Members who spoke in favor of this resolution likened it to a
tobacco tax, wherein if something is harmful to public health, the total item cost should include the social cost of that product,
which also serves to reduce consumption. The Delegation believes that CMA policy related to carbon emission taxes would be
an appropriate issue to refer to a TAC for further consideration.
The District IX/ACCMA Delegation recommends against adopting Resolution 111-20 in its present form since
many of the resolveds are outdated and/or address topics that are not germane to CMA’s mission. There may be specific
recommendations that would be appropriate for further review and consideration by a Technical Advisory Committee.
For example, the Delegation noted that the first and second resolveds seem appropriate and could be incorporated into
CMA climate change policy. However, as noted previously, we believe a TAC would be helpful in evaluating these and other
recommendations to develop a more comprehensive policy on climate change.
Thank you for the opportunity to provide feedback on these resolutions. We appreciate the opportunity to contribute
to CMA policymaking related to climate change, specifically as it relates to public health, medical care, and the health of our
patients.
If you have any questions or wish to discuss this matter further, please feel free to contact me or Joe Greaves, ACCMA
Executive Director, at 510-654-5383 or jgreaves@accma.org.
Sincerely,
Katrina Peters, M.D. ACCMA/District IX Delegation Chair
ACCMA BULLETIN | MARCH/APRIL 2021 13ACCMA LETTERS (continued from page 13)
Get your free copy of From Exam Room
to Courtroom: Lessons Learned from Real
Medical Malpractice Cases
Avoid Lawsuits in
Your Practice
In the most recent compilation of CAP’s
“Case of the Month” column, you will find
10 case studies of physicians involved in
medical malpractice legal disputes. These
cases offer important insights to help you Get Your FREE Copy at
reduce medical risk and increase patient CAPphysicians.com/EXAMROOM5
safety in your practice.
Learn more about common areas of
liability such as:
Physician misjudgment
Gaps in communication and
documentation
Oversights during specialist referrals
As a leading provider of superior medical
malpractice coverage in California for more
than 40 years, the Cooperative of American
Physicians, Inc. (CAP) is pleased to offer this
free resource to help you and your staff run
a safe and successful practice.
Medical professional liability coverage is provided to CAP members by the Mutual Protection Trust (MPT), an
unincorporated interindemnity arrangement organized under Section 1280.7 of the California Insurance Code.LETTER FROM CMA PRESIDENT
Letter from CMA President
By Peter Bretan, MD, President, California Medical Association
T he approval of two COVID vaccines in December 2020
has brought some much-needed positive news in the fight
against COVID-19. But we know that many physicians are still
We must ensure, when supply allows, they can get their COVID
vaccination the same way.
Community physician practices have the capability to
struggling to find useful and reliable information to share with administer 4.5 million doses of COVID vaccines requiring
their patients about how and when vaccines are coming to their refrigeration per month statewide, according to projections
community. based on recent CMA survey results. These practices can reach
While supply continues to be an issue, CMA is engaged patients who may not have the technological savvy to schedule an
with the Newsom Administration to ensure the needs and voices appointment through a new smartphone app or the ability to wait
of California physicians, and their patients, are heard. We have in line all day at a mass vaccination clinic.
successfully pushed the Newsom Administration to relax the strict While smartphone apps and mass vaccination sites are an
tier system for vaccine prioritization that was causing confusion important part of the solution, they cannot be the entire solution.
and slowing down the vaccine distribution process and are now CMA is fighting to get the vaccine in the hands of community-
working to ensure our vast network of community physicians are based physicians who can most easily and effectively reach
deployed as a key part of the vaccination solution. We also argued Californians where they live – particularly those that are in low-
that we needed a statewide, rather than a decentralized local income communities and/or communities of color.
strategy, to simplify navigating the system for both physicians and CMA leaders have made this case in hours of discussions
the general public. with senior Newsom administration officials and collected some
CMA has demonstrated its ability to reach community of these ideas in a recent letter to the governor’s office (a copy
physicians and shown the state how it is possible to equip those of which can be found on page 16). Simplifying the eligibility
who most directly serve the communities across the state. When framework and standardizing vaccine information and data on
California struggled to get personal protective equipment (PPE) a statewide basis are necessary to connect our communities to
in the hands of community practices, they turned to CMA. So vaccination in a timely way. These changes will accelerate the rate
far CMA, with help from our component medical societies, has of vaccinations across California and improve the experience of
distributed more than 100 million pieces of PPE to physician both vaccine administrators and vaccine recipients.
practices across California. Meanwhile, we are also working to make it easier for the
CMA can help connect state administrators with community thousands of physicians who have reached out looking to help
physicians to build a robust vaccination network and help the staff vaccine clinics in their communities and around the state.
state meet its goal of getting California vaccinated. Last month, the governor signed an Executive Order that extends
Equity and speed are both vital components of any successful liability protections to physicians and other vaccine administrators
vaccination strategy. We must make sure we do not compromise – something that CMA had requested for months (visit https://
one in the name of the other, and that we have a fast, effective and bit.ly/3dli4Ah to read more about the Executive Order.)
fair distribution of vaccines statewide. We know that your patients want to know when they will be
That means getting the vaccine into the communities that able to get the vaccine. The short answer is – we don’t know yet.
need it most. We do not have to reinvent the wheel. We can But we are fighting to make sure the concerns of all of you, and
simply stick with what has worked for other types of vaccinations. your patients, are heard. Despite the frustrations, we are making
That means fully engaging community-based physicians so that progress, and will continue to advocate on your behalf, and keep
people can be vaccinated in a place they are familiar with, under you informed of our efforts. I encourage you to regularly visit
the care of a provider they trust. Millions of Californians receive CMA’s COVID-19 vaccine page at https://www.cmadocs.org/
care from an independent physician practice. This is the place covid-19/vaccine for the latest information.
where they get their routine vaccinations and annual flu shots.
ACCMA BULLETIN | MARCH/APRIL 2021 15LETTER FROM CMA PRESIDENT
The Honorable Gavin Newsom
Governor of California
State Capitol
Sacramento, CA 95814
RE: Vaccine Distribution Efforts – Operationalizing Equity
Governor Newsom:
The physicians of California have been encouraged by recent changes to the vaccine distribution and administration plans.
Simplifying the eligibility framework and standardizing vaccine information and data on a statewide basis are necessary to
connect our communities to vaccination in a timely way. These changes will accelerate the rate of vaccinations across California
and improve the experience of both vaccine administrators and vaccine recipients. The changes should not reflect, however, a
retreat from equity as a guiding principle of vaccine distribution.
California physicians request, as important components for addressing equity, that the state ensure vaccine allocations
factor in community morbidity and transmission rates to determine vaccine need, and that community physician practices are
incorporated into the distribution model.
Transmission Focused Place-Based Allocations
A strategy that focuses exclusively on age will reinforce the disparities that are being laid bare by COVID-19. An analysis out
of UCSF of the COVID-19 deaths overlaid with the over 65 vaccination criteria finds that nearly 75% of those deaths among
people under 65 were Latinx people. To avoid exclusion based on omission, CMA advocates that vaccine allocations consider
morbidity and transmission rates of communities. In some cases, younger Latinx communities are at greater risk of serious or
fatal COVID disease than older White or Asian patients. The state should require that allocation determinations be weighted
toward those communities with the greatest rates of transmission. Especially within these communities, the flexibility that has
been created by recent changes to the prioritization framework can be leveraged by vaccine administrators to protect those at
highest risk.
In conjunction with the request that vaccine allocations be made with consideration of the greatest risk of morbidity and
transmission, it is important to couple that with concerted efforts to outreach to those populations within the community who
are at greatest risk to ensure they are able to make appointments for vaccination at locations in their own communities.
Community Physician Practices as Vaccine Providers
The California health care system, including community physician practices, needs to be fully engaged to vaccinate their
patients. Millions of Californians receive care from an independent physician practice. Though the Pfizer vaccine requires
extraordinary storage and handling, many practices have the refrigeration capacity to meet the storage requirements for the
Moderna vaccine and others that may soon by granted Emergency Use Authorization by the Food and Drug Administration. In
a recent survey of more than 4,000 community physician practices, CMA asked practices with the interest and the refrigeration
capacity for the Moderna vaccine to estimate their potential monthly vaccination volume. The survey, conducted from Jan. 6-11
with a margin of error of 1.42%, showed that respondents could deliver more than 736,000 doses per month. Based on this
16 ALAMEDA-CONTRA COSTA MEDICAL ASSOCIATION BULLETINLETTER FROM CMA PRESIDENT (continued)
information, we extrapolated to the larger community and estimate that community physician practices across California have
the capacity to administer approximately 4.5 million vaccine doses per month statewide. Importantly, these practices already
have relationships with patients and would be an important avenue for building trust and sharing accurate information about
the safety and efficacy vaccine. These practices can also help ensure a more equitable distribution of the vaccine, meeting many
low-income patients and communities of color where they are instead of asking them to rely on technology or distant sites to
receive their vaccination.
Physicians have reported that the current COVID-19 vaccine enrollment process is onerous and currently can take up to 30
days to complete. CMA recommends streamlining the application process for these practices. CMA is able to provide practice
information that can be uploaded into the registration system rather than requiring practices to upload that information, which
would eliminate one administrative step.
Additionally, we would like to request collaboration in helping to provide education, targeted specifically for these
community physician practices, on enrolling in the California Immunization Registry (CAIR) as an intermediate step to
prepare for the time when CalVax enrollment is open to a wider audience of providers.
Finally, it is important to ensure that the state’s provider help desk infrastructure is reinforced to enable support of an influx
of additional providers.
We join you in believing that California communities that have borne the worst of the pandemic should not be left
behind. We believe the steps outline above are critical to California building a vaccine program administrative structure that
operationalizes this shared value.
Sincerely,
Peter N. Bretan, M.D.
President
California Medical Association
Cc: The Honorable Mark Ghaly, M.D., M.P.H., Secretary, Health and Human Services
The Honorable Yolanda Richardson, Secretary, Government Operations Agency
Mr. Richard Figueroa, Deputy Cabinet Secretary, Office of Governor Newsom
NEW MEMBERS
Kishor Avasarala, MD Bogdan Silviu Eftimie, MD Karen M Goodwin, DO
Pediatrics Internal Medicine General Surgery
UCSF Children’s Hospital Oakland UCSF Washington Cancer Center UCSF Cancer Center Berkeley
(Fremont)
Kathryn Lauren Burge, MD Amit Gupta, MD
Pediatrics Inessa Gofman, MD Anesthesiology
Primary Pediatrics Alameda Pediatrics UCSF Children’s Hospital Oakland
UCSF Bay Area Children’s Physicians
Premjit Singh Chahal, MD Erica Marie Hadley, MD
Gastroenterology Janet Moore Goldman, MD Pediatrics
Diablo Digestive Care, Inc Maternal and Fetal Medicine UBCP PPMG Alameda
UCSF Benioff Children’s Physicians
continued on page 29
ACCMA BULLETIN | MARCH/APRIL 2021 17BYLAWS AMENDMENTS
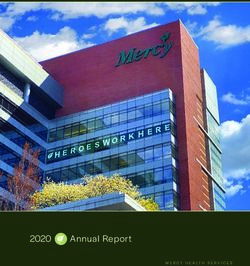
LANGUAGE DO'S & DON'TS
Do Say Don't Say
Vaccination Injection or shot
A safe and effective vaccine A vaccine developed quickly
Authorized by FDA based on clinical testing Approved by FDA, Operation Warp Speed; Emergency
Use Authorization¹
Get the latest information There are things we still don't know
Keep your family safe; keep those most Keep your country safe
vulnerable safe
Public Health Government
Health / medical experts and doctors Scientists
People who have questions People who are hesitant, skeptical, resistant, or "anti-vaxxers"
1. The perceived speed of vaccine development is a current barrier among many audiences
These recommendations are based partly on research conducted by the de Beaumont Foundation.
Messaging Elements That Resonate Messaging Elements That DON’T Resonate
Validate Concerns & Answer Questions Negativity & Fear
Acknowledge people's hesitancy rather than challenge it. People push back when reminded of how difficult a year it's been—it
Provide scientifically-base plain language answers. tends to put them in a pessimistic, hopeless or frustrated frame of mind.
Fear tactics are likely to backfire because this does little to generate
Moments Missed trust or answer people's questions about vaccines.
Reference things the people miss most. With many feeling
COVID-19 fatigue, missed moments (especially human Guilt
connections that we took for granted like visiting family and References to "many people already stepping up" can come off as pushy
friends) serve as a powerful reminder of the ultimate end goal: or accusatory. Those who are hesitant do not see themselves as "free
vaccination as a pathway to the possibility of regaining these riders" letting others take risks first; rather, they are worried about being
moments. "guinea pigs" for new COVID-19 vaccines.
Protection Overpromising
Emphasize "protecting myself, loved ones, and those in my Avoid claims that are unproven. Being overly rosy may cause concern.
community" (rather than "coming together as a nation"). Be clear about the facts without any sugarcoating. Most people
understand that mass vaccination is a long-term process. Avoid
Positive Tone messages that inadvertently imply that vaccine availability will "flip the
Be inviting and respectful as opposed to demanding. switch."
Acknowledge that the "choice is yours to make," which
connects with the deeply rooted American value of liberty. "Back to Normal"
Some just want things to "get back to normal," but for others,
post-pandemic life will never be "the way it was." It's more about getting
back to life rather than back to normal. Messages that focus on
economic recovery—rather than public health—do not perform well.
Research, insights, & content provided by Kaiser Family Foundation, AdCouncil, & COVID Collaborative
#ThisIsOurShot ThisIsOurShot2021 ThisIsOurShot www.thisisourshot.infoTHIS IS OUR SHOT
#ThisIsOurShot for a COVID-Free World
T his Is Our Shot (TIOS) is a national grassroots coalition of
healthcare heroes and allies that aim to build COVID-19
vaccine trust by elevating the voices of healthcare workers through
• Share your vaccine-selfies and personal stories on your social
media platforms, using #ThisIsOurShot and tagging @
ThisIsOurShot. You can also share your stories directly with
stories, photos, and videos using evidence-based messaging. The TIOS by visiting https://bit.ly/3wgboft.
campaign, which is led and supported by the California Medical • Share your vaccination story with the ACCMA! If you would
Association, grew organically as front-line workers turned to social like to participate in TIOS, you can share your vaccination
media to document their own experiences receiving COVID story about why you got questions, or common questions
vaccines. that your patients have about the vaccine, and the ACCMA
Throughout the COVID-19 pandemic, targeted disinforma- will share your responses on Twitter, @EastBayDocs, tagging
tion paired with decades of structural inequality and mistrust ThisIsOurShot. You can share your story with the ACCMA
in traditional institutions have contributed to the rise of vaccine by emailing dlopez@accma.org or calling (510) 654-5383.
hesitancy, particularly among communities of color. While sci-
entific innovation has led to the discovery of vaccines that are If you have any questions, please contact David Lopez,
highly effective at preventing illness and spread of COVID-19, ACCMA Associate Director of Advocacy and Strategic Initiatives,
the increase in disinformation and vaccine hesitancy is threaten- at dlopez@accma.org or at (510) 654-5383, ext. 6320.
ing our future and creating a barrier to reaching heard immunity
in our country.
This Is Our Shot aims to tackle the disinformation move-
ment by sharing stories, photos, videos, and facts from healthcare
Tracy Zweig Associates
workers across the country. Personal doctors and healthcare pro- A REGISTRY & PLACEMENT FIRM
viders are the most trusted source of information on the COVID-
19 vaccine across all races, ethnicities, and political affiliations.
#ThisIsOurShot allows those with questions about the vaccines Physicians
to network with health experts to provide facts and help allay fears. Nurse Practitioners
If you are a healthcare provider who is interested in helping build Physician Assistants
vaccine-trust for a COVID-free world, consider getting involved
with TIOS:
• TIOS hosts weekly calls to discuss public messaging, social
media, and this mission. These calls are held via Zoom every
Tuesday from 5:30 to 7:00 PM. To join the Zoom meeting,
visit https://bit.ly/31BDWSI (note that this link will take
you directly to the Zoom meeting, which will not be open
until 5:30 PM on Tuesday evenings).
• Get involved on social media. TIOS is very active on most
social media platforms and has created a website, https:// Locum Tenens
thisisourshot.info/, that links to social media toolkits. Access Permanent Placement
the social media toolkits directly by visiting the links below:
• Facebook: www.facebook.com/groups/thisisourshot Voice: 800- 919- 9141 or 805-6 41-91 41
FAX : 805- 641 -914 3
• Instagram: www.instagram.com/thisisourshot/
• Twitter: twitter.com/ThisIsOurShot jnguyen@ t r acyzw eig.com
• Sign up for email updates by visiting https://thisisourshot. w w w.t r acyzw eig.c om
info/join-us/.
ACCMA BULLETIN | MARCH/APRIL 2021 19CATT PROGRAM
Community Assessment and Transport
Team (CATT)
ALAMEDA COUNTY'S NEW COMPREHENSIVE CRISIS RESPONSE
O n February 25, 2021, the ACCMA’s Emergency Committee
received a presentation from Dr. Karl Sporer, Medical
Director of the Alameda County Emergency Medical Services
time the officer may leave the scene.
The CATT licensed behavioral health clinician can make
referrals and assist with transport to a shelter, sobering center,
Agency, and Yolanda Takahashi, Alameda County Emergency wellness center, mental health facility, or other designated
Medical Services Coordinator and CATT Project Manager, about destinations that fit the individual’s needs at that moment. If a
the County’s new Community Assessment and Transport Team CATT unit arrives and suspects the patient requires medical
(CATT) program. Alameda County Health Care Services Agency attention, the EMT completes a medical evaluation to determine
launched the new community-based behavioral health service in whether advance care and transport to an emergency department
July 2020; the program is the first of its kind in Alameda County is necessary.
and one of very few like programs in California. The CATT “CATT is a cross-community partnership delivering crisis
program aims to revolutionize the way mental health crises are care as a holistic intervention,” said Karyn Tribble, PsyD, LCSW,
addressed in the Emergency Medical Services (EMS) system. Director, Alameda County Behavioral Health Care Services. “We
“We finally have a program that ensures behavioral health care are meeting individuals at a critical point in their lives and shifting
services are provided as the first response to people in crisis,” said the conversation to a more health-oriented episode of care. These
Dr. Karl Sporer, Medical Director, Alameda County Emergency real time interactions provide further insight and drive feedback to
Medical Services Agency. “To get here, we had to invent the our system allowing us to further innovate and improve services
mental health first responder and that’s a game-changer.” for our community.”
This first-of-its-kind pilot program is a collaborative effort
WHAT IS CATT? between Alameda County Behavioral Health (ACBH), Alameda
CATT is a mobile crisis team staffed by an Emergency Medical Care Connect (Whole Person Care), Alameda County EMS
Technician (EMT) and a Licensed Behavioral Health Clinician. Agency, Bonita House, Inc., and Falck Alameda County. Operating
These teams operate in Oakland, San Leandro, Hayward, and out of modified SUVs, the goal of CATT is to reduce stigma
Fremont. While the program is still relatively new, the goal is to and increase access to behavioral health services for individuals
have 12 teams operating staggered hours between 7 AM and 11 who may otherwise be needlessly transported to an emergency
PM. There are a few similar programs in other parts of California, department, detained under a 5150 or placed into custody.. The
but no one has yet to develop a program this expansive. CATT program not only reduces the burden on already-impacted
emergency departments, but it provides much-needed behavioral
HOW DOES CATT WORK? health care to priority populations.
CATT teams provide medical and mental health assessments, CATT units have access to the Community Health Record
management, transportation, and referrals to patients who are (CHR), so they are able to look up any known history about
presenting with mental health emergencies in the prehospital the patient, including existing providers and care plans. The
setting. The CATT program is integrated into the 9-1-1 dispatch CHR pulls information from the Social Health Information
system to reduce the rate of involuntary detentions and increase the Exchange (SHIE), which was developed by Alameda County’s
efficiency and effectiveness of linking clients to needed services. Care Connect whole person care initiative. The CHR and SHIE,
Law enforcement is always first on scene and they conduct both launched in 2019, are data-sharing infrastructure projects,
an evaluation to determine if an individual meets the guidelines focused on high utilizers of medical, behavioral, housing, and
to activate CATT. When law determines the scene is safe and emergency services, that integrate social data into the EHRs of
the individual will benefit from CATT services, they request medical providers. Read more about CHR and SHIE at https://
the team through the Alameda County Regional Emergency bit.ly/3cBZK6M.
Communications Center and conduct a brief turnover at which By using the Community Health Record, CATT teams can
20 ALAMEDA-CONTRA COSTA MEDICAL ASSOCIATION BULLETINYou can also read