Rising unemployment and increasing spatial health inequalities in England: further extension of the North-South divide
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Journal of Public Health Advance Access published January 4, 2013
Journal of Public Health | pp. 1–9 | doi:10.1093/pubmed/fds085
Rising unemployment and increasing spatial health
inequalities in England: further extension of the North – South
divide
Holger Möller1,2, Fiona Haigh3, Chris Harwood2, Tony Kinsella2, Daniel Pope4
1
University of Liverpool, School of Management, Liverpool L69 3BX, UK
2
NHS Wirral, Performance and Public Health Intelligence Team, Old Market House, Hamilton Street, Birkenhead CH41 5LF, UK
3
Centre for Health Equity Training Research & Evaluation, University of New South Wales, LMB 7103, Liverpool BC NSW 1871, Australia
4
Department of Public Health and Policy, University of Liverpool, Whelan Building, Quadrangle, Liverpool L69 3GB, UK
Address correspondence to Holger Möller, E-mail: hmoller@uws.edu.au
A B S T R AC T
Background Unemployment negatively affects health. In this study, we quantify the impact of current and rising levels of unemployment on
limiting long-term illness (LLTI), mental health problems and mortality in North and South England.
Methods Excess cases of LLTI and mental health problems in the unemployed were calculated as the difference in the prevalence between
the employed and unemployed using data from large population surveys for England. Mortality due to unemployment was calculated using
the formula for the population-attributable fraction.
Results Current levels of unemployment were estimated to be causing 1145 deaths per year and a total of 221 020 cases of mental health
problems and 275 409 cases of LLTI in England. Rates of mortality, mental health problems and LLTI due to unemployment were distinctively
higher in the North compared with the South. Considering hidden unemployment in the calculations considerably increased the proportion
of women suffering from ill health due to unemployment.
Conclusions Our study quantifies the detrimental effect of unemployment on health in England. There is a clear difference between
North and South England highlighting the contribution of unemployment to spatial health inequalities. A public health priority should be to
(i) prevent unemployment in the first place and (ii) provide support for the unemployed.
Keywords economics, education, employment and skills, finance and industry, morbidity and mortality
Introduction could be missed by being classified as economically in-
active.2 It was estimated that hidden unemployment was
Unemployment has risen steeply in England since the start
around 1 million in England in 2007.2
of the financial crisis. Approximately 2.2 million people were
Despite small improvements in the first quarter of 2011,
unemployed at the end of 2011, an increase of almost 62%
unemployment rates are predicted to further increase due to
compared with the last quarter in 2007.1 The true level of
slowing economy and large numbers of public sector jobs
unemployment is likely to be even higher due to hidden un-
employment.2 Measures of unemployment include job
seekers allowance (JSA) claimant count and the International
Labour Organization (ILO) defined unemployment: ‘per- Holger Möller, Research Fellow
centage of unemployed available for work, who have been Fiona Haigh, Research Fellow
actively looking for work in the last 4 weeks per economical- Chris Harwood, Intelligence Manager
ly active population’.3 Whilst the ILO expands on the JSA Tony Kinsella, Head of Performance and Intelligence
claimant count a large proportion of hidden unemployment Daniel Pope, Lecturer in Epidemiology
# The Author 2013, Published by Oxford University Press on behalf of Faculty of Public Health. All rights reserved 12 J O U R NA L O F P U B L I C H E A LT H
being cut through government austerity measures.4 There is Morbidity
a great variation in unemployment by geographical region Unemployment has been linked with LLTI5,6 and mental
and by socioeconomic status. Unemployment rates in the health problems29 – 32 and a number of studies have sug-
North East (10.4%) are almost double than those of the gested a positive relationship between unemployment and
South East (5.9%) and rates in the most deprived (16.7%) heart disease.33 – 36 Whilst there is good evidence for the as-
are 4.4 times those in the least deprived (3.9%).1 sociation of unemployment with mental health problems
The negative health effects of unemployment have been and LLTI, evidence for the association with heart disease is
studied extensively and unemployment has been linked with inconclusive.37 The analysis was therefore restricted to these
increased morbidity5 – 7 and mortality.8 Unemployment has outcomes.
also been shown to negatively affect the family and wider Calculations for LLTI and mental health problems were
community9 – 11 and tends to disproportionately impact on based on two studies of British Household Panel Survey
certain vulnerable population groups such as women, young data (Table 1).5,32 The findings of these studies are in line
people, the least educated and lower socio-economic with those of other studies.6,29 and were chosen for calcula-
groups.12,13 Differences in regional employment rates have tions of impact as they are reflecting British data and differ-
been shown to account for health inequalities between entiating by sex. The upper and lower limits of the estimates
regions in England.14,15 of effect were explored in a sensitivity analysis (Table 1).
In contrast, studies on the effect of economic recession at
a population level have reported overall mortality to decrease Mortality
or remain unchanged during recession.16 – 22 While this may Longitudinal studies from the 1980 and 1990s have pro-
seem paradoxical, such decreases have been explained by a vided strong evidence for a causal relationship between un-
corresponding reduction in work- and traffic-related acci- employment and increased mortality.34,38 – 42 A recent
dents16,17,22 – 24 and people adopting healthier life styles out meta-analysis of 42 studies reported significant pooled esti-
of necessity due to financial constraints.22,25,26 Rather than mates of effect of 1.78 and 1.37 for all-cause mortality in
study the population as a whole the current research focuses unemployed men and women, respectively.8
on the health effects on the unemployed. While some of the associations observed in earlier studies
This study estimates the impact on mental health pro- may have been influenced by confounding of individual risk
blems and limiting long-terms illness (LLTI) and mortality factors, a Swedish study, which controlled for pre-existing
in England of current unemployment and a rise in rates of health conditions and a large number of confounders,
unemployment. To investigate the regional differences reported statistically significant positive associations between
England is divided into North and South using the geo- unemployment and mortality outcomes.43 Alternative
graphical boundaries adopted in a recently published study methods of adjusting for confounding has been to study the
summarizing differential mortality between North and health effects of unemployment in times of generally high
South England.27 unemployment, therefore reducing possible bias of health
selection44, and to exclude deaths occurring in the first few
years after unemployment from the analysis, as these are
more likely to be due to pre-existing health problems.45,46
Methods
Most studies on mortality compared the unemployed with
Excess cases of mental health problems, LLTI and mortality the employed, hence not being directly transferable at the
in the unemployed were calculated based on the best avail- population level as they are missing out the economically in-
able evidence from large population studies and routine data active group. Based on an analysis of a large population
for North and South England. For unemployment the def- sample from census data for Finland, Martikainnen and
inition of the ILO3 was used. Unemployed not meeting Valkonen reported 3.1- and 2.4-fold increased risk of mor-
these criteria were classified as economically inactive. Of the tality in inactive men and women, respectively.47
inactive, those who would like a job and are able to start The effect of unemployment on all-cause mortality was
within the next 2 weeks were included in the analysis to con- estimated using the age stratified results of the meta-analysis
sider hidden unemployment. Excess morbidity was calcu- by Roelfs et al.8 for statistical modelling (Table 1). In a sensi-
lated as the difference in the prevalence between tivity analysis, the impact of applying the findings of a sub-
unemployed and employed and mortality by using the analysis by Roelf et al.8 and those of the studies by Lundin
formula for the population-attributable fraction (PAF).28 et al.43 and Martikainnen et al.44 were explored (Table 1).U N E M P LOYM EN T A N D H E A LT H I N EQUA L I TI ES 3
Table 1 Estimates of effect taken from the literature for LLTI, mental health problems and mortality used in the main model and sensitivity analysis
Outcome Age Men Women Based on the study
Main model
Mental Health problems All age groups 2.05 1.72 Thomas et al.32
LLTI All age groups 2.41 2.06 Bartley et al.6
Mortality 16– 39 1.73 1.73 Roelfs et al.8
40– 49 1.77 1.77 Roelfs et al. 8
50– 64 1.25 1.25 Roelfs et al. 8
Sensitivity analysis
Mental health problems All ages 1.71 1.39 Lower 95% CI, Thomas et al. 32
All ages 2.47 2.12 Upper 95% CI, Thomas et al. 32
LLTI All ages 1.92 1.68 Lower 95% CI, Bartley et al. 6
All ages 3.01 3.12 Upper 95% CI, Bartley et al. 6
Mortality All ages 1.56 1.17 Lower 95% CI, Roelfs et al. 8
All ages 2.02 1.60 Upper 95% CI, Roelfs et al. 8
All ages 1.30 1.30 Lundin et al. 43
All ages 1.25 1.25 Martikainnen et al. 44
a
16– 39 1.95 1.73 Roelfs et al., sub-model8,
8,a
40– 49 1.86 1.34 Roelfs et al., sub-model
a
50– 64 1.17 0.94 Roelfs et al., sub-model8,
a
Based on 93 hazard ratios which were adjusted for age, had an age range smaller or equal to 35 years, did not use the general population as the
control group and did not include persons not in the labour force in the case group and were from studies with less than a 1 year gap between the
end of baseline and the beginning of follow-up.
Table 2 Overview of surveys and measures used in the analysis
Survey Sample Measures used in the study
Labour Force Survey48 n ¼ 57 747 (48.5% men, 51.5% Number of unemployed and inactive wanting a job and able to start work
women) within 2 weeks
Health Survey for n ¼ 3594 (45.7% men, 54.3% women) Prevalence of LLTI in employed. LLTI was measured in questionnaire as: ‘presence
England 200949 of these 2787 were employed of longstanding illness that is limiting activity’.
Adult Psychiatric n ¼ 5425 (43.6% men, 56.4 women) Prevalence of mental disorders in employed. In the survey mental health
Morbidity Survey 200750 of these 3964 were employed problems were measured using the revised Clinical Interview Schedule (CIS-R). A
score of .12 indicates the presence of significant neurotic symptoms and
people with a score of 18 or above are likely to require clinical treatment
Data sources as weighted proportions using individual weights supplied in
Mortality data for England for 2009 were obtained from the the respective data sets.
Office for National Statistics. Unemployment data were
extracted from the quarter four 2010 Labour Force Survey
(LFS).48 The prevalence of LLTI and mental health pro- Statistical analysis
blems in the employed was calculated from the Health The effects of current levels and a 1% increase in un-
Survey for England (HSE) 2009 49 and the Adult employment on morbidity and mortality were calculated for
Psychiatric Morbidity Survey (APMS) 200750, respectively the age groups 16 –39, 40 – 49 and 50– 64. Calculations
(Table 2). The prevalence rates for LLTI and mental health were carried out using Stata version 1051 and Microsoft
problems by employment status and region were calculated Excel. England was split into North and South for the4 J O U R NA L O F P U B L I C H E A LT H
analysis by government office regions using the same divid- the North and 356 100 (54%) in the South (Supplementary
ing line between the Wash and Severn Estuary as a recent data, Table S2).52
publication by Hacking et al.27
Excess cases of LLTI and mental health problems among Prevalence of LLTI and mental health problems
the unemployed (Nex) were calculated as Based on the findings of the HSE 2009 for assessment of
Nex ¼ ðPe RRu Nu Þ ðPe Nu Þ ð1Þ LLTI and the AMPS for mental health problems, 12.2% of
16– 64 year olds employed were suffering from LLTI and
where Pe is the percentage of people with LLTI or mental 12.9% from mental health problems in England. Rates of
health problems in the reference population (employed), mental health problems in women were significantly higher
RRu the increased risk in the unemployed and Nu the in the North compared with the South (Supplementary data,
number of unemployed. Table S3). The three leading causes of LLTI in 16 –64 year
Mortality in the 16– 64 olds economically active was cal- olds were problems of the musculoskeletal system (27.9%),
culated by subtracting mortality in the economically inactive mental disorders (11.9%) and problems of the heart and cir-
from the total mortality in that age group using the findings culatory system (11.5%).
by Martikainnen et al.41 Mortality in the inactive and
unemployed was calculated using the formula for the PAF:25 Morbidity attributable to unemployment
PðRR 1Þ Current levels of unemployment were estimated to contrib-
PAF ¼ ð2Þ ute to 221 020 cases of mental health problems and 275 409
PðRR 1Þ þ 1
cases of LLTI in England (Table 3). Men represent 51.2%
where P is the prevalence of economic inactivity or un- of those individuals with mental health problems and 62.8%
employment and RR the relative risk of mortality. of LLTI. A 1% increase in unemployment was estimated to
The expected excess mortality due to increased un- result in an additional 35 624 cases of mental health pro-
employment was calculated using the formula: blems and 52 571 cases of LLTI (Table 4). Rates were sig-
Ðm Ðm nificantly higher in men and women in the North compared
RRðxÞPðxÞdx x¼0 RRðxÞP 0 ðxÞdx with the South (Tables 3 and 4). The 16– 39 year olds con-
PAF x¼0 Ðm ð3Þ
x¼0 RRðxÞPðxÞdx tributed the largest amount of mental health problems
(52.3%) and LLTI (69.6%) (Fig. 1) and the 40 –49 and
where P(x) is the proportion of population at each exposure 50– 64 year olds had the highest rates measured per un-
level, RR(x) the relative risk of mortality for each exposure employed population (Supplementary data, Fig. SA1).
category level, P 0 (x) the counterfactual proportion of popula- Including hidden unemployment in the analysis was esti-
tion at each exposure level and m the maximum exposure mated to result in a 74% increase in mental health problems
level. Increased levels of unemployment were defined as a and a 66% increase in LLTI. The percentage contribution of
counterfactual scenario.28 women also increased, reflecting the high prevalence of in-
active women who would like to work (Table 3). Sensitivity
analysis calculated the estimates for England for current
Results levels of unemployment of between 134 929 and 326 220
Unemployment in England for mental health problems and between 178 577 and 451
According to the 2010 LFS,48 1 036 456 people (59% men, 391 for LLTI (Supplementary data, Tables S4 and S5).
41% women) were unemployed in the North and 985 463
(57% men, 43% women) in the South of England. Mortality attributable to unemployment
Unemployment rates were highest in the 16 –39 year olds, Around 1145 deaths (628 in the North and 517 in the
higher in men compared with women and higher in the South) in the 16– 64 year olds were estimated to be attribut-
North compared with the South for the 16 – 39 and 40 –49 able to current levels of unemployment in England per year.
year olds. Of those who are economically inactive and able Rates were higher in the North compared with the South
to start work, 675 162 (57% women, 43% men) wanted a (Table 3). About 72% of deaths related to men with the
job; the majority of whom were aged 16 – 39 (52%) largest proportion of deaths occurring in the 16– 39 and
(Supplementary data, Table S1). From 2007/08 to 2011/12 40– 49 year olds (36%) (Fig. 1). The older age groups had
the number of unemployed had risen by 419 100 (60.2%) in the highest attributable mortality rates (Supplementary data,U N E M P LOYM EN T A N D H E A LT H I N EQUA L I TI ES 5
Fig. SA1). A 1% increase in unemployment was estimated
105.7, 107.7
228.7, 231.6
108.8, 110.8
222.4, 225.3
Table 3 Mortality, mental health problems and LLTI due to current levels of unemployment (rates per 1000 for LLTI and mental health problems and per 100 000 for mortality and 95% confidence
to result in an extra 221 deaths per year (114 in the North
29.5, 40.7
48.4, 62.5
95%CI
and 107 in the South) (Table 4). Adjusting for hidden un-
employment resulted in an increase of 37% in mortality
(Table 3). Sensitivity analysis showed a spread in results
106.7
230.1
109.8
223.9
from 606 to 1773 in the unemployed and from 785 to 2487
35.1
55.4
Rate
when adjusting for hidden unemployment (Supplementary
data, Tables S4 and S5).
Number
Women
45 789
98 740
47 127
96 048
150
238
Discussion
140.6, 142.5
133.7, 135.6
212.6, 215.0
93.0, 94.6
59.1, 72.6
81.3, 97.0
Main findings
95% CI
Current levels of unemployment were estimated to be
causing around 1145 excess deaths per year, and a total of
141.5
134.6
213.8
221 020 cases of mental health problems and 275 409 cases
93.8
65.9
89.2
Rate
of LLTI in England. A 1% increase in the unemployment
rate was calculated to result in an extra 221 death per year,
118 945
Number
52 198
78 759
74 912
35 624 cases of mental health problems and 52 571 cases of
South
Men
367
496
LLTI. Morbidity and mortality rates were distinctively higher
in the North compared with the South, indicating that dif-
145.2, 147.5
281.4, 284.6
128.9, 131.1
241.3, 244.3
ferential unemployment rates exacerbate geographical health
33.8, 45.8
52.6, 67.4
95% CI
inequalities. Considering hidden unemployment suggests
that women might be suffering to a much greater extent
from unemployment, than reflected in routine statistics. This
146.4
283.0
130.0
242.8
supports the argument by Bambra that the current econom-
39.8
60.0
Rate
ic crisis is likely to have a much greater effect of women
than any of the past recessions.13
120 209
103 119
Number
Women
62 163
55 205
Sensitivity analysis indicated the possible range of out-
169
255
comes and, even for the most conservative assumptions, the
numbers of cases of mental health problems, LLTI and
142.5, 144.4
159.5, 161.5
228.2, 230.6
98.7, 100.3
86.9, 102.3
mortality due to unemployment were still of significant
68.1, 81.8
95% CI
magnitude.
What is already known on the topic
143.5
160.5
229.4
99.5
75.0
94.6
Rate
Unemployment has been linked with increased morbidity5 – 7
and mortality.8 Studies on economic cycle and health
140 347
Number
60 870
87 762
98 165
reported increases in suicide and decreases in mortality from
North
Men
459
579
traffic accidents during times of recession.16,17,22 While
some studies reported a decrease in overall mortality during
Unemployed þ inactive wanting job
Unemployed þ inactive wanting job
Unemployed þ inactive wanting job
economic downturn17,20 – 22,53 others have found no change
in all-cause mortality.16,23 A recent study reported an in-
crease in suicides during the 2008 – 10 economic recession
in England and showed a strong correlation with local un-
employment rates.53
The differences in mortality found between North and
Unemployed
Unemployed
Unemployed
Mental illness
South England are in line with the findings reported by
Hacking et al. 27 suggesting that the differential unemploy-
Mortality
intervals)
ment could be a contributory factor to these higher mortal-
LLTI
ity rates.6 J O U R NA L O F P U B L I C H E A LT H
Table 4 Mortality, mental health problems and LLTI per 1% increase in unemployment (rates per 1000 for LLTI and mental health problems and per
100 000 for mortality and 95% confidence intervals)
North South
Men Women Men Women
Number Rate 95% CI Number Rate 95% CI Number Rate 95% CI Number Rate 95%CI
Mental illness 9436 15.4 15.1, 15.7 9018 21.2 20.8, 21.7 8958 16.1 15.8, 16.4 8212 19.1 18.7, 19.6
LLTI 18 338 30.0 29.5, 30.4 9186 21.6 21.2, 22.1 15 898 28.6 28.1, 29.0 9150 21.3 20.9, 25.7
Mortality 72 11.7 9.0, 14.4 42 9.9 6.9, 12.9 68 12.2 9.3, 15.1 39 9.0 6.2, 12.9
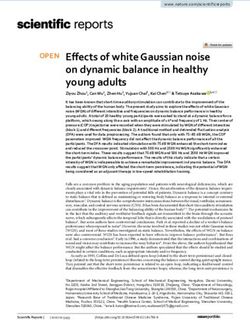
Mental health problems risk of LLTI in the economically inactive. We limited the
80 LLTI analysis to the 675 162 inactive, wanting a job, who are able
70 Mortality
to start work. These are likely to be conservative estimates,
60
considering that 1.7 million of the economically inactive
50
wanted a job1 and Beatty et al.2 estimated around 1 million
Percent
40
people to be suffering from hidden unemployment in
30
England in 2007.
20
10
Health selection is a known problem in the study of un-
0
employment and it has been postulated that the strength of
16–39 40–49 50–64 16–39 40–49 50–64 the relationship between unemployment and poor health
Male Male Male Female Female Female decreases during periods of recession as more people are
Fig. 1 Percentage distribution of mental health problems, LLTI and drawn into the unemployed category.14 This is supported by
mortality due to unemployment by age groups and sex in England. the studies of Martikainnen et al. and Lundin et al., which
reported lower increased risk of mortality in times of eco-
What this study adds nomic recession and after adjusting for pre-existing health
This study is the first to estimate the impact of unemploy- conditions, respectively.43,44 Both these studies were
ment on morbidity and mortality in the unemployed popula- included in the sensitivity analysis of our study. Another ap-
tion in England. Estimates of population-level health proach to adjust for health selection has been to exclude
impacts provide valuable evidence to support policy-makers deaths occurring in the first few years after unemployment
and commissioners of health services for decision-making from the analysis.45,46 A recent UK study found no differ-
and planning processes. Identifying regional differences ence in mortality with or without using a wear-off period in
highlights potential impacts of the recession on geographical the analysis and concluded that there was little evidence of a
health inequalities. This study focused on the unemployed selection effect operating on the unemployed in their
and also considered hidden unemployment; these groups study.46 Similarly Akinwale et al.54 reported the pattern of
have not been specifically considered in previous population mortality by labour market position to be unchanged after
level studies on unemployment and health. In addition our applying a wear off period of 5 years.
study also estimates morbidity outcomes and uses current Mortality in the unemployed was calculated by subtracting
exposure data to provide up to date estimates of the current mortality in the inactive from the total mortality. To calculate
recession. mortality in the inactive we used risk estimates from a large
Finnish population study.47 These estimates are higher com-
Limitations pared with those of a recent UK study,54 indicating that esti-
The analysis was extended to include the inactive wanting a mates for the unemployed may be conservative. However,
job and able to start work in the next 2 weeks to adjust for Aikinwale et al.54, only looked at the older age groups and it
hidden unemployment. Only limited studies have looked at is not clear if the difference would remain for all age
the inactive separately. The economically inactive have been groups.
shown to experience higher mortality compared with the The prevalence of mental health problems among the
economically active8,47,54 and Bartley et al. 6 reported higher employed differed between North and South regions ofU N E M P LOYM EN T A N D H E A LT H I N EQUA L I TI ES 7
England and to estimate the relationship in the unemployed Acknowledgements
we applied national values. The true increase in mental
This work contains data from the Health Survey for
health problems and LLTI in the unemployed might also
England and Adult Psychiatric Morbidity survey from the
differ by region, which could not be adjusted for in this
National Centre for Social Research. These studies were
study. Other health problems might be related to unemploy-
commissioned by the Information Centre for Health and
ment that were not included in this study, indicating that the
Social Care and the data are available through the UK data
true impact might be even greater.
archive. Data for the Labour for Survey is from Office for
Due to small sample size at a regional level of the HSE
National Statistics, Social Survey Division, also available
and APMS surveys, analysis was limited to North and South
through the UK data archive. The data are Crown copyright
of England. There are potentially large inter regional inequal-
material is reproduced with the permission of the Controller
ities15 which could not be considered in the analysis. Further
of HMSO and the Queen’s Printer for Scotland. The origin-
regional breakdown should be included in future analysis.
al data creators, depositors or copyright holders, the funders
The calculation of mortality attributable to unemployment
of the Data Collections (if different) and the UK Data
was based on the methodology of the PAF.28 By necessity this
Archive bear no responsibility for their further analysis or
method uses relative risks from the best available evidence
interpretation of the data. We thank Sacha Wyke from
base from literature reviews. This method may yield biased
North West Public Health Observatory for providing the
estimates when used with relative risk estimates adjusted for
mortality data extract and Liz Harris and Scott Walter from
confounding.55 This potential bias has been explored and
University of New South Wales and Louisa Jorm from
Darrow and Steenland56 reported that when the crude relative
University of Western Sydney for commenting on the paper.
risk is greater than the adjusted, as would be the case in our
study, the attributable fraction may be underestimated.
Funding
Conclusion
Our study clearly demonstrates the detrimental effect of un- This project was funded by Wirral Primary Care Trust.
employment on health in England. Women might be suffer-
ing to a much greater extent from unemployment, than References
reflected in routine statistics. There is a clear difference
between North and South England highlighting the contribu- 1 Office for National Statistics (ONS). Nomis official labour market
statistics, annual population survey, 2011. http://www.nomisweb.co.
tion of unemployment to health inequalities. This is sup- uk/articles/554.aspx (11 January 2012, date last accessed).
ported by the fact that the gap in unemployment between the
2 Beatty C, Fothergill S, Gore T et al The real level of unemployment
most and least deprived groups of the population has 2007. Sheffield: Centre for Regional Economic and Social Research
increased since the start of the financial crisis. While the (CRESR), 2007. http://www.shu.ac.uk/_assets/pdf/cresr-RealLevel
overall impact of the economic crisis might not change the Unemployment07.pdf (12 April 2012, date last accessed).
heath status at a population level or even have beneficial 3 Hussmanns R. Measurement of employment, unemployment and
effects as highlighted earlier,17,20 – 22 the detrimental health underemployment—current international standards and issues in
consequences of unemployment cannot be overlooked. The their application. Geneva: International Labour Organisation, 2007.
http://www.ilo.org/wcmsp5/groups/public/– -dgreports/– -stat/
results of our study show that everything possible should be
documents/publication/wcms_088394.pdf (12 April 2012, date last
done to avoid unemployment in the first place and support accessed).
the unemployed as much as possible. Social protection has 4 The Chartered Institute of Personnel and Development (CIPD).
been shown to mitigate the negative health effects of un- UK jobs market takes a turn for the worse: looks like the only way
employment16 and Bambra highlighted the different levels of is up for unemployment.http://www.cipd.co.uk/pressoffice/press-
intervention at the macro, meso and the individual level.57 releases/uk-jobs-market-takes-turn-for.aspx (11 January 2012, date
Special focus should be paid to the most vulnerable groups last accessed).
such as lower qualified workers and young people which have 5 Bartley M, Plewis I. Accumulated labour market disadvantage and
been shown to be more strongly affected by unemployment.5 limiting long-term illness: data from the 1971 – 1991 Office
for National Statistics’ Longitudinal Study. Int J Epidemiol
2002;31(2):336– 41.
Supplementary data 6 Bartley M, Sacker A, Clarke P. Employment status, employment
conditions, and limiting illness: prospective evidence from the
Supplementary data are available at the Journal of Public British Household Panel Survey 1991 – 2001. J Epidemiol Community
Health online. Health 2004;58(6):501 – 06.8 J O U R NA L O F P U B L I C H E A LT H
7 Arber S, Lahelma E. Inequalities in women’s and men’s ill-health: 26 Kruger NA, Svensson M. Good times are drinking times: empirical
Britain and Finland compared. Soc Sci Med 1993;37(8):1055 – 68. evidence on business cycles and alcohol sales in Sweden 1861 –
8 Roelfs DJ, Shor E, Davidson KW et al Losing life and livelihood: a 2000. Appl Econ Lett 2010;17(4 – 6):543 – 6.
systematic review and meta-analysis of unemployment and all-cause 27 Hacking JM, Muller S, Buchan IE. Trends in mortality from 1965
mortality. Soc Sci Med 2011;72(6):840 –54. to 2008 across the English north– south divide: comparative obser-
9 Moser KA, Fox AJ, Jones DR et al Unemployment and mortality: vational study. BMJ 2011;342:d508.
further evidence from the OPCS Longitudinal Study 1971 – 81. 28 Murray CJL, Ezzati M, Lopez AD et al Comparative quantification
Lancet 1986;327(8477):365 – 67. of health risks: conceptual framework and methodological issues.
10 Novo M, Hammarstrom A, Janlert U. Do high levels of unemploy- Popul Health Metr 2003;1:1 – 20.
ment influence the health of those who are not unemployed? A 29 Paul KI, Moser K. Unemployment impairs mental health:
gendered comparison of young men and women during boom and meta-analyses. J Vocat Behav 2009;74(3):264– 82.
recession. Soc Sci Med 2001;53(3):293 – 303. 30 McKee-Ryan F, Song Z, Wanberg CR et al Psychological and physic-
11 Solantaus T, Leinonen J, Punamäki R-L. Children’s mental health in al well-being during unemployment: a meta-analytic study. J Appl
times of economic recession: replication and extension of the family Psychol 2005;90(1):53– 76.
economic stress model in Finland. Dev Sci 2004;40(3):412– 29. 31 Murphy GC, Athanasou JA. The effect of unemployment on
12 Employment Conditions Knowledge Network (EMCONET). mental health. J Occup Organ Psychol 1999;72:83– 99.
Employment conditions and health inequalities. Final report to the 32 Thomas C, Benzeval M, Stansfeld SA. Employment transitions and
WHO commission on the social determinants of health. Benach J, mental health: an analysis from the British Household Panel Survey.
Muntaner C, Santana V, chairs; report writing group, Marcelo J Epidemiol Community Health 2005;59(3):243 – 9.
Amable [et al.]; general editor, Jacqueline Murray 2007. Barcelona,
33 Mattiasson I, Lindgärde F, Nilsson JA et al Threat of unemployment
Spain: Health Inequalities Research Group. http://www.who.int/
and cardiovascular risk factors: longitudinal study of quality of sleep
social_determinants/resources/articles/emconet_who_report.pdf
and serum cholesterol concentrations in men threatened with re-
(12 April 2012, date last accessed).
dundancy. BMJ 1990;301(6750):461 – 6.
13 Bambra C. Yesterday once more? Unemployment and health in the
34 Iversen L, Sabroe S, Damsgaard MT. Hospital admissions before
21st century. J Epidemiol Community Health 2010;64(3):213– 5.
and after shipyard closure. BMJ 1989;299(6707):1073 – 6.
14 Bambra C. Work, Worklessness and the Political Economy of Health.
35 Janlert U. Unemployment and blood pressure in Swedish building
Oxford, UK: Oxford University Press, 2011.
labourers. J Intern Med 1992;231(3):241 – 6.
15 Bambra C, Popham F. Worklessness and regional differences in the
36 Hammarström A. Health consequences of youth unemployment.
social gradient in general health: evidence from the 2001 English
Public Health 1994;108(6):403– 12.
census. Health Place 2010;16:1014– 21.
37 Weber A, Lehnert G. Unemployment and cardiovascular diseases: a
16 Stuckler D, Basu S, Suhrcke M et al The public health effect of eco-
causal relationship? Int Arch Occup Environ Health
nomic crises and alternative policy responses in Europe: an empiric-
1997;70(3):153– 60.
al analysis. Lancet 2009;374(9686):315– 23.
38 Moser KA, Fox AJ, Jones DR. Unemployment and mortality in the
17 Lin SJ. Economic Fluctuations and health outcome: a panel analysis
OPCS Longitudinal Study. Lancet 1984;2(8415):1324 – 9.
of Asia-Pacific countries. Appl Econ 2009;41(4 – 6):519– 30.
39 Iversen L, Andersen O, Andersen PK et al Unemployment and
18 Granados J. Recessions and mortality in Spain, 1980 – 1997. Eur J
mortality in Denmark, 1970 – 80. BMJ 1987;295:879– 84.
Popul 2005;21(4):393 –422.
40 Martikainen PT. Unemployment and mortality among Finnish men,
19 Granados JAT. Increasing mortality during the expansions of the
1981 – 5. BMJ 1990;301(6749):407– 11.
US economy, 1900 – 1996. Int J Epidemiol 2005;34(6):1194– 202.
41 Stefansson CG. Long-term unemployment and mortality in
20 Tapia Granados JA. Macroeconomic fluctuations and mortality in
Sweden, 1980 – 1986. Soc Sci Med 1991;32(4):419– 23.
postwar Japan. Demography 2008;45(2):323– 43.
42 Morris JK, Cook DG, Shaper AG. Loss of employment and mor-
21 Granados JAT, Roux AVD. Life and death during the great depres-
tality. BMJ 1994;308(6937):1135 – 9.
sion. Proc Natl Acad Sci USA 2009;106(41) pp. 17290 – 95.
43 Lundin A, Lundberg I, Hallsten L et al Unemployment and mortal-
22 Ruhm CJ. Are recessions good for your health? Q J Econ
ity—a longitudinal prospective study on selection and causation in
2000;115(2):617 – 50.
49 321 Swedish middle-aged men. J Epidemiol Community Health
23 Svensson M. Economic upturns are good for your heart but watch 2010;64(1):22– 8.
out for accidents: a study on Swedish regional data 1976 – 2005.
44 Martikainen P, Maki N, Jantti M. The effects of unemployment on
Appl Econ 2010;42(5):615 – 25.
mortality following workplace downsizing and workplace closure: a
24 Granados JAT, Ionides EL. Mortality and macroeconomic fluctua- register-based follow-up study of Finnish men and women during
tions in contemporary Sweden. Eur J Popul 2011;27(2):157 – 84. economic boom and recession. Am J Epidemiol 2007;165(9):1070 – 5.
25 Ruhm CJ. Economic conditions and health behaviors: are recessions 45 Fox AJ, Goldblatt PO, Adelstein AM. Selection and mortality differ-
good for your health? N C Med J 2009;70(4):328 – 9. entials. J Epidemiol Community Health 1982;36(2):69 – 79.U N E M P LOYM EN T A N D H E A LT H I N EQUA L I TI ES 9
46 Clemens T, Boyle P, Popham F. Unemployment, mortality and the 51 StataCorp. Stata Statistical Software: Release 10. College Station, TX:
problem of health-related selection: evidence from the Scottish and StataCorp LP, 2007.
England & Wales (ONS) longitudinal studies. Health Stat Q 52 Office for National Statistics (ONS). NOMIS official labour market
2009;43:7 – 13. statistics, 2012. http://www.nomisweb.co.uk/ (11 January 2012,
47 Martikainen P, Valkonen T. Bias related to the exclusion of the eco- date last accessed).
nomically inactive in studies on social class differences in mortality. 53 Barr B, Taylor-Robinson D, Scott-Samuel A et al Suicides associated
Int J Epidemiol 1999;28:899 – 904. with the 2008 – 2010 economic recession in England: time trend
48 Office for National Statistics. Social and vital statistics division and analysis. BMJ 2012;345:e5142.
Northern Ireland Statistics and Research Agency, Central Survey Unit. 54 Akinwale B, Lynch K, Wiggins R et al Work, permanent sick-
Quarterly Labour Force Survey, January –March, 2007, 4th edn. ness and mortality risk: a prospective cohort study of England
Colchester, Essex: UK Data Archive, 2010. SN: 5657 [computer file]. and Wales, 1971 – 2006. J Epidemiol Community Health
49 National Centre for Social Research and University College London. 2011;65(9):786 – 92.
Health survey for England, 2009. Department of Epidemiology 55 Flegal KM, Graubard BI, Williamson DF. Methods of calculating
and Public Health. Colchester, Essex: UK Data Archive, 2011. SN: deaths attributable to obesity. Am J Epidemiol 2004;160(4):331– 8.
6732 [computer file].
56 Darrow LA, Steenland NK. Confounding and bias in the attribut-
50 National Centre for Social Research and University of Leicester. able fraction. Epidemiology 2011;22(1):53 –8.
Adult psychiatric morbidity survey, 2007, 3rd edn. Colchester,
57 Bambra C. Work, worklessness and the political economy of
Essex: UK Data Archive, 2011. SN: 6379 [computer file].
health inequalities. J Epidemiol Community Health 2011;65(9):746 – 50.You can also read