RESEARCH DURING A PANDEMIC: FINDINGS FROM THE COVID-19 GLOBAL RHEUMATOLOGY ALLIANCE REGISTRY - MILENA GIANFRANCESCO, PHD, MPH ASSISTANT PROFESSOR ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Research During a Pandemic:
Findings from the COVID-19 Global
Rheumatology Alliance Registry
Milena Gianfrancesco, PhD, MPH
Assistant Professor
Division of Rheumatology
University of California, San Francisco
August 21, 2021
Disclosures • Research program support: • NIH/NIAMS (K01 AR07585) • Rheumatology Research Foundation K Supplement • NIH/NIAMS K Supplement • Several slides courtesy of Dr. Jinoos Yazdany (UCSF)
COVID-19 in immunosuppressed patients ! Little to no information available at onset of the pandemic ! Previous studies established that immunosuppression and comorbidities are associated with increased risk of serious infection in rheumatic disease ! Some medications used to treat rheumatic disease used for COVID-19 and complications (HCQ, anti-IL-1, anti-IL-6, JAK inhibitors, steroids) ! Need for immediate data to guide patient care

What are the risk factors for poor outcomes? Comorbidities associated with severe illness and mortality ! Cardiovascular disease ! Diabetes mellitus ! Hypertension ! Chronic lung disease ! Cancer ! Chronic kidney disease ! Obesity ! Immunocompromising conditions?

Are people receiving immunosuppressive drugs significantly more susceptible to initial infection with SARS-Cov-2?

Low prevalence of infection
among immunosuppressed
patients
! Survey of 995 rheumatology patients
in Lombardy between February and
April
! 98% response
! The incidence of confirmed COVID-
19 similar to the general population
(0.62% vs 0.66%; p=0.92)
! No severe complications or deaths
Favalli et al. Arthritis & Rheum, June. 2020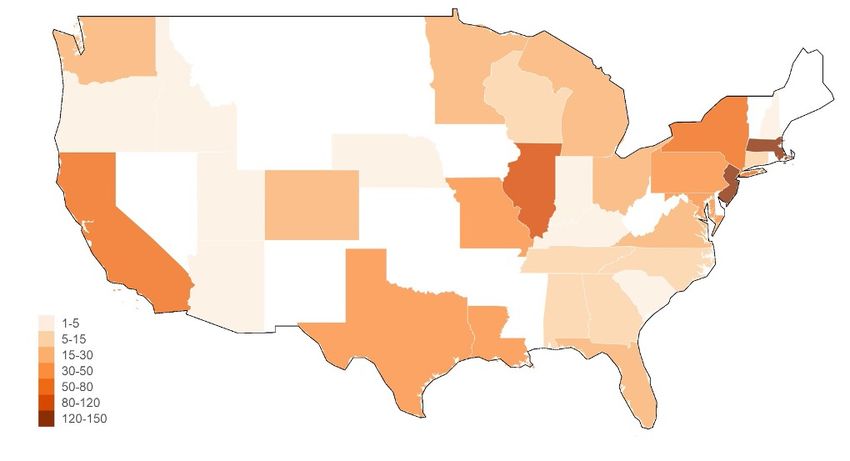
Population-based study in Hong Kong
• 1067 cases of COVID-19
diagnosed in Hong Kong which
has a population of 7.5 million
• Only 5 patients with rheumatic
disease developed COVID-19
• The incidence of COVID-19 was
1.26 cases per 100,000 patients
with rheumatologic diseases,
compared to 1.42 per 100,000 in
the general population
Fhkam et al. Seminars in Arthritis and Rheum, July 24, 2020.
Immunosuppressive drugs not associated with higher
COVID-19 incidence in IBD
• National VA data between Jan and
April 2020
• 37,821 Veterans with inflammatory
bowel disease:
• 36 cases of COVID-19
• No increase among TNF users or
thiopurine users
Khan et al. Gastroenterology, May 29, 2020.
• In almost all studies, incidence of
COVID-19 in immunosuppressed
individuals with autoimmune disease +SARS-COV-2
N
similar to the general population N (%)
tested
• Caveat: People who are Diamond Princess Cruise Ship 3,711 712 (19.2)
immunosuppressed may be more likely Charles de Gaulle aircraft 1,760 1,046 (59.4)
to follow COVID-19 precautions carrier crew
Boston homeless shelter 408
147 (36.0)
occupants
• High attack rates in vulnerable
populations (prison inmates, homeless Los Angeles homeless shelter 178
43 (24.2)
occupants
individuals, nursing home residents)
illustrate that initial infection is most NYU OB patients 214 33 (15.4)
strongly associated with high-risk King County, Washington 76
48 (63.2)
exposures nursing home residents
https://www.scripps.edu/science-and-medicine/translational-institute/about/news/sarc-cov-2-
infection/index.html
People with autoimmune diseases do not
appear to have higher rates of initial
infection with SARS-Cov-2 compared to the
general population
ACR Guidance:
Immunosuppressed
individuals should be
counseled on general
preventive measures
for COVID-19
https://www.rheumatology.org/Portals/0/Files/ACR-COVID-19-Clinical-Guidance-Summary-Patients-with-Rheumatic-Diseases.pdfWhat are the outcomes of COVID-19 in immunosuppressed individuals?
Do rheumatic disease
patients have higher Age
mortality from COVID-19?
• Study Design: Observational cohort
from UK electronic health record data on
17 million individuals
• Outcome: Hospital deaths
• Findings:
• Confirmed many risk factors like age,
obesity, comorbidities
• Highlighted risk of poverty/social
determinants RA, SLE,
Psoriasis
• 885,000 with ”RA/SLE/Psoriasis” had
slightly higher risk (HR1.23, 1.12-1.35)
Williamson, et al. Nature (2020)NYC and Boston studies
• NYC study (Haberman, N Engl J Med. 2020 Jul
2;383(1):85-88)
• 86 COVID-19 positive patients with autoimmune
disease
• Incidence of hospitalization (16%) was consistent
with that of the corresponding general
population (26%); only one patient died
• Boston study (D’Silva, Ann Rheum Dis. 2020 May
26) rheumatic disease patients with COVID-19 matched
to 104 controls
• A similar proportion of patients with and
without rheumatic disease were hospitalized (23
(44%) vs 42 (40%)), p=0.50) but those with
rheumatic disease required intensive care
admission and mechanical ventilation more often
[11 (48%) vs 7 (18%)]
• Mortality was similar between the two groups (3
(6%) vs 4 (4%), p=0.69).The risk of severe outcomes in patients with
rheumatic diseases is closely tied to age and
comorbidities, like the general population
ACR and EULAR
Outcomes in Guidance:
immunosuppressed Immunosuppressive
patients with medications should be
continued in non-
autoimmune have
infected individuals to
been reassuring reduce the risk of disease
flare
ACR COVID Guidance: https://www.rheumatology.org/Portals/0/Files/ACR-COVID-19-Clinical-Guidance-Summary-Patients-with-Rheumatic-
Diseases.pdf
EULAR COVID Guidance: https://ard.bmj.com/content/79/7/851European Population-Based Studies
• Increased risk of poor COVID-19 outcomes in RD patients
• Sweden: ↑ risk hospitalization, ICU admission, and death due to COVID-19 vs.
population referents
• Denmark: ↑ risk of more severe COVID-19 outcome (death, ARDS, or
transfer to ICU)
• England: ↑ risk death
• France: ↑ odds of death in hospitalized patients vs. population referents
1. Bower et al. Annals of the rheumatic diseases. 2021.
2. Cordtz et al. Rheumatology. 2020.
3. Peach et al. Rheumatology. 2021.
4. AI2R /SFR/SNFMI/SOFREMIP/CRI/IMIDIATE consortium
Annals of the rheumatic diseases. 2020.Are COVID-19 outcomes more severe with specific immunosuppressive drugs?
C OV I D - 1 9 C O L L A B O R AT I O N
2 8 8 O R G A N I Z AT I O N S
> 3 0 0 I N V E S T I G ATO R S
WO R L DW I D E What we are trying to accomplish?
E N G AG E D PAT I E N T A DV I S O RY
B OA R D
Two main questions:
• What are the outcomes of
patients with rheumatic disease
with COVID19?
• Can we make any inferences
about immunosuppressive/anti-
malarial drugs?It started with a Tweet…
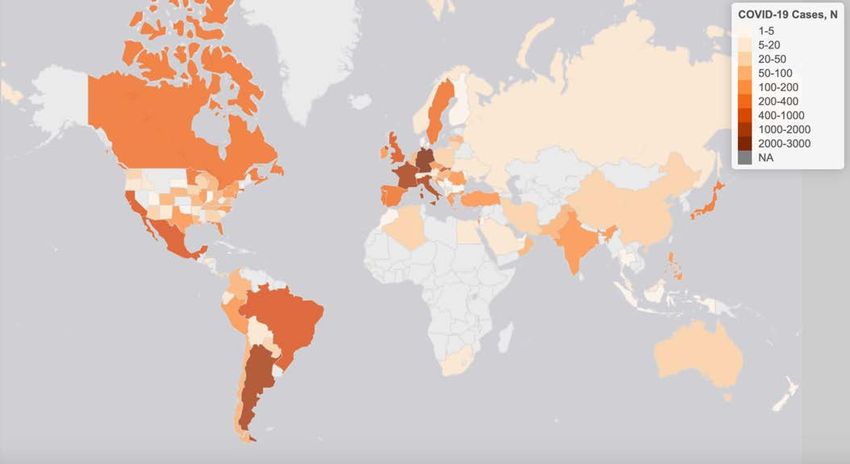
Aug 2021
COVID 19-GRA Provider Registry Jan 2021
~20,000
~9,000
July 1
March 11 March 24 ~4,000
2020
April 20
April 1 ~600
>100
March 17:
Bay Area SIPrheum-covid.org/map As of July 1, 2021
Additional Major Projects • Global scholarships: We will be providing small grants to underrepresented countries to participate in the physician registry • Patient survey regarding impact of the COVID-19 on people with rheumatic disease • Literature reviews are being conducted in collaboration with the Cochrane group • Rheum drugs and treatment of COVID-19 • Rheum COVID-19 outcomes
Physician registry, initial research
question:
What are risk factors for hospitalization?Characteristic N (%)
Female 423 (71)
Age, Median (IQR) 56 (45 - 67)
Common rheumatic diagnoses:
RESU LTS: RA
SLE
230 (38)
85 (14)
C H ARAC TERISTIC S O F SpA - PsA 74 (12)
SpA – AS or other 48 (8)
600 PATIEN TS Vasculitis 44 (7)
Common comorbidities
HTN 199 (33)
Lung Disease 127 (21)
Diabetes 69 (12)
! Patients have inflammatory CVD 63 (11)
CKD/ESRD 40 (7)
rheumatic disease Smoking
! Cases submitted March 24- Ever
Never
129 (22)
389 (65)
April 20, 2020 Unknown 82 (14)
Medications
! Which cases are entered? No DMARD
csDMARD only, including anti-malarial
97 (16)
272 (45)
! Sick enough to receive csDMARD only, excluding anti-malarial
Anti-malarial, with or without other DMARD
122 (20)
130 (22)
COVID-19 Anti-malarial only 52 (9)
diagnosis/testing b/tsDMARD only
csDMARD + b/tsDMARD combination
107 (18)
124 (21)
! Only some practices have NSAIDs 111 (21)
Prednisone-Equivalent Glucocorticoids (N=592)
systems for capturing all None 403 (68)
COVID-19 cases 1-9 mg/day
more than 10 mg/day
125 (21)
64 (11)
Hospitalized 277 (46)
Gianfrancesco et al. Ann Rheum Dis. 2020 Jul;79(7):859-866. Deceased 55 (9)RESU LT S:
H O SPITALIZATIO N
STATUS
• Risk factors for hospitalization
• Older age &
comorbidities
• Prednisone ≥10 mg/day
• Steroid effect remained
after adjusting for
disease activity
• Fewer hospitalizations among
those on b/ts DMARD only
*Models adjusting for smoking and disease activity yielded similar results
Gianfrancesco et al. Ann Rheum Dis. 2020 Jul;79(7):859-866.RESULTS: More on HCQ
and biologic DMARDs
• TNFi users have fewer hospitalizations in
adjusted models (OR 0.40, 95% CI 0.19, 0.81)
• No significant association between antimalarials
and hospitalization in adjusted models (OR
0.94, 95% CI 0.57, 1.57)
Gianfrancesco et al. Ann Rheum Dis. 2020 Jul;79(7):859-866.What are risk factors for mortality?
PH YSIC IA N G RA
DATA , N =3705
• Risk factors for mortality
• Older age
• Male sex
• Smoking
• AND
• HIGH disease activity
*Models also adjusted for other comorbidities, smoking, additional diseases, and several
Strangfeld et al., 2021, Ann Rheum Dis other classes of DMARDs and biologics and disease activity yielded similar resultsComorbidities increase risk of mortality among rheumatic disease patients Strangfeld et al., 2021, Ann Rheum Dis
Higher risk with SSZ, Rituximab vs. MTX mono Strangfeld et al., 2021, Ann Rheum Dis
Health Disparities among Patients with Rheumatic Disease Diagnosed with COVID-19
Racial/Ethnic
Disparities in
Rheumatic Disease
• Higher risk of rheumatic disease
in non-white populations
• Racial/ethnic minority patients
experience a higher burden of
disease activity and severity
compared to white patients1-3
• One study found that disparities
remained after adjusting for
demographic and socioeconomic
1. Greenberg et al, 2013, Am J Med
factors, including health
2.
3.
Bruce et al, 2007, J Rheumatol
Barton et al, 2011, Arthritis Care Res
insurance status1COVID-19 Outcomes by Race/Ethnicity in
Rheumatic Disease
• Disproportionate adverse outcomes of COVID-19 could have a
substantial long-term impact on patients’ health and quality of life
• Non-white patients with SLE hospitalized at higher rates than white
patients in NY1
• 83% non-white, 42% Hispanic SLE versus
• 59% non-white, 29% Hispanic ambulatory
• No information on other rheumatic diseases, in other areas at the
time
1. Fernandez—Ruiz et al, 2020, Arthritis RheumatolAssociation of Race/Ethnicity With COVID-19
Outcomes in Rheumatic Disease
• Cases Mar 24 – Aug 26, 2020, USA only
• Multivariable logistic regression analyses
• Race: white (ref), Black, Latinx, Asian (East or South), other/mixed
• Main outcomes:
• Hospitalization status (Y/N)
• Ventilatory status among hospitalized (No supp O2 vs. supp O2 /non- invasive
ventilation vs. mechanical ventilation/ECMO)
• Death (Y/N)
• Covariates: Age, sex, smoking status, rheumatic disease, disease activity,
comorbidities, and rheumatic disease medications pre-COVID
Gianfranceso et al 2020 Arth & Rheum1324 cases
White patients were less likely to be hospitalized (29%) compared to:
Black (51%), Latinx (37%), Asian (43%), and other/mixed race (35%) patients
Gianfranceso et al 2020 Arth & RheumAssociation of Race/Ethnicity With COVID-19
Outcomes in Rheumatic Disease
• Race/Ethnicities associated with HIGHER ODDS of hospitalization
• Black 2.74 (1.90, 3.95)*
• Asian 2.69 (1.16, 6.24)*
• Latinx 1.71 (1.18, 2.49)*
• Race/Ethnicities associated with HIGHER ODDS of ventilatory support
• Latinx 3.25 (1.75, 6.05)*
• Mortality – no significant differences
Gianfranceso et al 2020 Arth & RheumPooled Analyses Across Registries
• Rheumatic Disease (GRA)
Data from pooled • Inflammatory Bowel Disease
registries (SECURE-IBD)
• Psoriasis (PsoProtect) Registries
• 6,077 cases
• Objective: To compare the association between TNFi monotherapy
and COVID-19-related hospitalization or death among individuals with
immune-mediated inflammatory diseases, with other commonly
prescribed immunomodulatory regimens
• Analyses controlled for age, sex, smoking status, diagnosis, disease
activity, various comorbidities, and glucocorticoid dose
Izadi Z. et al. (2021) AcceptedRegistry OR (95% CI)
TNFi + AZA/6MP vs. TNFi monotherapy
SECURE-IBD 1.51 (0.98, 2.31)
--Pooled estimate 1.74 (1.17, 2.58)
--Pooled estimate (sensitivity analysis) 1.57 (1.06, 2.35)
.
TNFi + MTX vs. TNFi monotherapy
GRA 1.20 (0.80, 1.79)
SECURE-IBD 1.59 (0.76, 3.34)
--Pooled estimate 1.18 (0.85, 1.63)
--Pooled estimate (sensitivity analysis) 1.14 (0.81, 1.60)
.
AZA/6MP monotherapy vs. TNFi monotherapy
GRA 5.28 (1.51, 18.43)
SECURE-IBD 1.50 (1.00, 2.24)
--Pooled estimate 1.84 (1.30, 2.61)
--Pooled estimate (sensitivity analysis) 1.69 (1.19, 2.39)
.
MTX monotherapy vs. TNFi monotherapy
GRA 2.21 (1.59, 3.08)
SECURE-IBD 2.66 (0.95, 7.43)
PsoProtect 8.76 (2.94, 26.06)
--Pooled estimate 2.00 (1.57, 2.56)
--Pooled estimate (sensitivity analysis) 2.10 (1.62, 2.72)
.
JAKi monotherapy vs. TNFi monotherapy
GRA 2.41 (1.46, 3.99)
SECURE-IBD 0.60 (0.22, 1.64)
--Pooled estimate 1.82 (1.21, 2.73)
--Pooled estimate (sensitivity analysis) 1.77 (1.16, 2.69)
.
Favors other regimen Favors TNFi monotherapy
.2 1 5 30
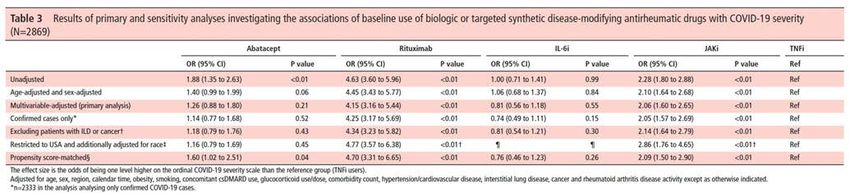
Izadi Z. et al. (2021) AcceptedDisease-Specific Analyses
Associations of baseline use of biologic or targeted
synthetic DMARDs with COVID-19 severity in RA
• RA cases from March 24, 2020 – April 12, 2021 (n=6132)
• Subset of patients on: abatacept (n=237), rituximab (n=364), IL-6i
(n=317), JAKi (n=563), or TNFi (n=1388) monotherapy at time of
COVID-19 onset [total n=2869]
• Exposure = medications
• Outcome = ordinal COVID-19 severity outcome
1. No hospitalization
2. Hospitalization with no oxygenation
3. Hospitalization with any oxygenation or mechanical ventilation
4. Death
Sparks et al, 2021, Ann Rheum DisOther Condition-Specific Projects In Progress - SLE - Vasculitis - Scleroderma (in collaboration with EUSTAR) - Pregnancy - ARDS prediction Future Projects - Outcomes in patients with breakthrough infections - Regional differences in outcomes over time
Summary • Risk in patients with rheumatic disease is largely driven by age and comorbidities • Consistent signal of worse outcomes with moderate or high doses of steroids (may be driven by disease activity) • Within the U.S., race/ethnicity associated with worse outcomes • Other drugs with a high-risk signal (rituximab, immunosuppressants) need to be further confirmed in other studies and/or across different registries
C19-GRA Steering Committee ! Philip Robinson, Chair ! Jinoos Yazdany,Vice-Chair Twitter: @rheum_covid ! Paul Sufka ! Rebecca Grainger Website: rheum-covid.org ! Zach Wallace ! Suleman Bhana ! Emily Sirotich ! Jean Liew ! Jonathan Hausmann ! Pedro Machado ! Wendy Costello
You can also read