Dyslipidaemia - getting to lower LDL targets safely - deNovo ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Leader in digital CPD
Earn 3
for Southern African
free CEUs Cardiovascular diseases
healthcare professionals
Dyslipidaemia – getting to
lower LDL targets safely
Learning objectives
You will learn:
• New South African guidelines on lipid-lowering are recommending lower LDL-cholesterol
levels:
Dyslipidaemia – getting to lower LDL targets safely
Evidence of LDL-cholesterol’s pivotal role in
atherosclerosis
Professor Derick Raal
The Cholesterol Treatment Trials collabora- relationship between reduction in LDL-
tion (CTT) evaluated the results of 26 statin cholesterol levels and the annual incidence
trials involving more than 170 000 patients of major coronary artery disease (CAD) and
over more than a decade and showed the vascular events (Table 1).1,2
Table 1. Every 1mmol/l reduction in LDL-cholesterol leads to:
• An annual 21-24% reduction in major CAD or vascular events
• 12% annual reduction in overall mortality.
Latest cholesterol-lowering guidelines
The South African Dyslipidaemia Guideline cardiovascular risk (Table 2).3 These have
Consensus Statement of 2018 set LDL- now been updated in accordance with the lat-
cholesterol targets for patients at very high est evidence.4
“In the future, Table 2. South African guidelines: Patients at very high cardiovascular risk require
I believe the immediate intensive lipid management4
LDL-cholesterol
• Established atherosclerotic disease:
target for – CAD
very high-risk – Cerebrovascular disease
patients will be – Peripheral vascular disease
further reduced • Type 2 diabetes mellitus plus one or more cardiovascular disease risk factors or age >40 years
• Type 1 diabetes mellitus with microalbuminuria/proteinuria
to ≤1mmol/l” • Chronic kidney disease:
Professor Raal – eGFR
Dyslipidaemia – getting to lower LDL targets safely
Table 4. Definition of high- and very high-risk patients4
High-risk: • Framingham 10-year risk of >15% is high-risk and >30% very high-risk
• Markedly elevated single risk factors – TC >8mmol/l or LDL-C >4.9mmol/l or BP
≥180/110mmHg
• FH without other major risk factors
• Moderate CKD (eGFR 30-59ml/min/1.73m2)
• DM with target organ damage.
Very high-risk • ASCVD (clinical/imaging)
• FH with ASCVD or another major risk factors
• Severe CKD (eGFR 20 years.
Clinical strategy: How to get to these lower LDL-cholesterol targets?
The principle in daily clinical practice of Using ezetimibe plus statin to reach a lower
...less than 10% getting to this lower target is: firstly, to use LDL-cholesterol target achieves better results
only high-intensity statins; secondly, con- as was shown by the lower LDL-cholesterol
of FH patients
sider combination therapy using agents that levels achieved in the IMPROVE-IT study,
were shown have different mechanisms of action, such as which showed an additional 16.4% reduction
in the South ezetimibe; and thirdly, use the newly available in cardiovascular events and death when this
African cohort of (in South Africa) PCSK9 inhibitors. combination was used.5
the SAFEHEART
“In my clinical practice, I only use high- The clinical expectation when using a com-
study to reach
intensity statins such as atorvastatin and bination of a high-intensity statin and
these new rosuvastatin at maximal doses. Simvastatin ezetimibe is a 55-65% reduction in LDL-
recommended very rarely forms part of my therapeutic cholesterol levels. This is sufficient for many
lower LDL- approach,” said Professor Raal. patients with established ASCVD. However, it
cholesterol is important in the South African context to
It is important to note that doubling of remember that less than 10% of FH patients
target levels the statin dose only results in a further 6% were shown in the South African cohort of
prior to the reduction in LDL-cholesterol and that the the SAFEHEART study to reach these new
introduction residual risk associated with statin-only use recommended lower LDL-cholesterol target
of the PCSK9 can be reduced by further lowering of LDL- levels prior to the introduction of the PCSK9
inhibitors cholesterol using either ezetimibe or a PCSK9 inhibitors.
inhibitor or both.
The essential role of PCSK9 inhibitors in achieving
‘optimal’ LDL-cholesterol levels
EARN FREE While PCSK9 inhibitors have been available study7 in 2012 showed that alirocumab mono-
CPD POINTS globally for four years or longer, South Africa
is one of the last countries in the world to get
therapy can achieve a 60% reduction in LDL-
cholesterol and that the effect lasts for 2-3
Join our CPD community at these agents (alirocumab and evolocumab) for weeks following a single dose; levels return to
www.denovomedica.com cholesterol lowering. PCSK9 inhibitors are baseline within 2-4 weeks.
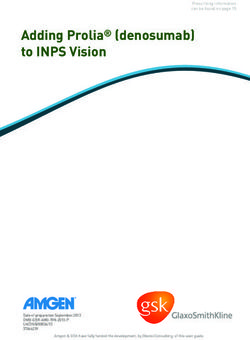
monoclonal antibodies and, in essence, the
and start to earn today! inhibition of PCSK9 rescues LDL-receptors “In a study of homozygotes and heterozygous
from degradation and increases the presence FH patients whom I was involved with some
and role of these receptors in removing LDL- five years ago,8 treatment with PCSK9 inhibi-
cholesterol from the circulation (Figure 1).6 tors on top of statin and ezetimibe therapy
achieved LDL-cholesterol target levels in
Lipidologists in South Africa have been these patients that I had never seen before
involved in the clinical trials of PCSK9 – truly remarkable drugs,” Professor Raal
inhibitors since the initial proof of concept explained (Table 5).
JANUARY 2021 I 3
Dyslipidaemia – getting to lower LDL targets safely
Table 5. Clinical guide to medications and their lipid-lowering intensity
Treatment Average LDL-cholesterol reduction
Moderate-intensity statin ≈ 30%
High-intensity statin ≈ 50%
High-intensity statin and ezetimibe ≈ 65%
PCSK9 inhibitor ≈ 60%
PCSK9 inhibitor and high-intensity statin ≈ 75%
PCSK9 inhibitor and high-intensity statin and ezetimibe ≈ 85%
Without PCSK-inhibition With PCSK-inhibition
Figure 1. Effects on LDL-cholesterol with and without PCSK9 inhibition6
“The most PCSK9 inhibitors – for which patients are they indicated?
deserving “The most deserving patients for the use of of statin and ezetimibe.4
patients for the PCSK9 inhibitors are those furthest from
their recommended LDL-cholesterol target,” Also, PCSK9 inhibitors should be consid-
use of PCSK9 Professor Raal noted. ered in primary prevention for individuals
inhibitors are with heterozygous FH at very high-risk, who
those furthest In order to address some concern that all require a ≥50% reduction from baseline and
from their patients in the high-risk category not at their have an LDL-cholesterol goal ofDyslipidaemia – getting to lower LDL targets safely
What is the long-term safety of and experience
with PCSK9 inhibitors?
Professor Dirk Blom, University of Cape Town
A reassurance as to safety with regard to lipid levels in pregnant Zimbabwean women
the concept of PCSK9 inhibition is seen in which identified a woman with extremely
natural-occurring human genetic mutations low levels of LDL-cholesterol:Dyslipidaemia – getting to lower LDL targets safely
Table 6. Adverse events by LDL-cholesterol level11
0.5 to 1.3 to 1.8 toDyslipidaemia – getting to lower LDL targets safely
Efficacy and dosing of PCSK9 inhibitors
The dose of alirocumab used in the clinical tri- mutations in both LDL-receptor alleles. In
als was 75mg once every two weeks; if the LDL- patients with homozygous FH the response
cholesterol target was not reached, this was to treatment is determined by the residual
up-titrated to 150mg once every two weeks.12 LDL receptor function.13 Some patients with
no residual receptor function do not respond
“I will, however, predict that we are going to at all. Patients with homozygous FH should
see wider use of the 150mg dose of alirocumab ideally be referred to a specialist lipid clinic
in clinical practice, which would also be my for review and evaluation as they may benefit
preference, to get maximal LDL-cholesterol from the addition of novel therapies that do
lowering quickly,” Professor Blom noted. not require LDL receptors to act.
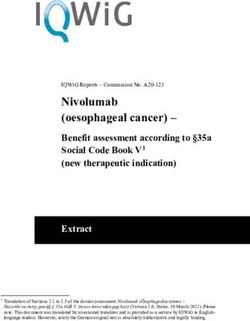
In the ODYSSEY trial of heterozygous FH The results of an open-label extension study
patients, the approach of starting at 75mg of patients in South Africa treated with
“It is clear that and up-titrating at week 8 resulted in a alirocumab in the ODYSSEY clinical trial
drop of 51%-58% (on higher dose) in LDL- programme and whose therapy continued
all cells are able
cholesterol. (Figure 2). showed that over a further three years, these
to synthesise low levels of LDL-cholesterol were main-
the cholesterol Patients with homozygous FH respond tained; South African patients responded just
they need rather less well to PCSK9 inhibitors as they have as well as those in the rest of the world.10,14
than relying
exclusively
on importing 4.5 174
cholesterol;
4 155
very low LDL-
LDL-C, LS mean (±SE), mmol/l
cholesterol 3.5 135
is thus not
associated 3 116
mg/dl
with increased
2.5 97
neurocognitive
events, 2 77
haemorrhagic
stroke or non- 1.5 58
cardiovascular 1 39
causes of 0 4 8 12 16 24 36 52 64 78
mortality”
Week
Professor Blom
No. patients analysed
FH I
ALI 322 304 290 277 279
EARN FREE PBO 163 152 149 146 145
CPD POINTS FH II
ALI 166 152 157 158 154
Join our CPD community at
PBO 81 76 78 78 71
www.denovomedica.com
Placebo + statin therapy Alirocumab + statin therapy
at maximum tolerated at maximum tolerated dose
and start to earn today!
dose ± other LLT ± other LLT
FH I FH I
FH II FH II
ALI: alirocumab; PBO: placebo
Figure 2. ODYSSEY extension trial results10
JANUARY 2021 I 7Dyslipidaemia – getting to lower LDL targets safely
Long-term extension studies over five years studies, despite including different patient
with evolocumab treatment in the Fourier populations, achieved an absolute risk reduc-
study of post-ACS patients also showed that tion of 1% in cardiovascular and non-fatal
the initial change in LDL-cholesterol levels myocardial infarction events. Patient accept-
from baseline was maintained with ongoing ance of PCSK9 inhibitor therapy is high; this
therapy. class of medication is highly effective and
very safe,” Professor Blom concluded.
“Both the alirocumab14 and evolocumab10
Key learnings
• It is important to realise that the maximum benefit occurs in patients at the highest risk and that
accurately stratifying risk is essential in determining the benefit of PCSK9 inhibitor therapy
• It is important in clinical practice to understand that many patients will benefit from PCSK9 inhibitor
therapy, but that it is important initially to select those who will receive the highest benefit from this
particular lipid-lowering therapy.
EARN FREE
CPD POINTS NOW EARN FREE CPD POINTS
Are you a member of
Southern Africa’s leading
digital Continuing
Professional Development
website earning FREE
CPD points with access to
Click here to access and submit deNovo Medica’s CPD modules
best practice content?
Only a few clicks and
References
you can register to start
earning today
Click on reference to access the scientific article
1. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety variability and antidrug-antibody formation with bococizumab.
of cholesterol lowering treatment: prospective meta-analysis N Engl J Med 2017; 376: 1517-1526.
Visit of data from 90,056 participants in 14 randomised trials of 9. Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and
statins. Lancet 2005; 366: 1267-1278. clinical outcomes in patients with cardiovascular disease. N Engl
2. The Cholesterol Treatment Trialists (CTT) collaboration. Efficacy J Med 2017; 376: 1713-1722.
www.denovomedica.com and safety of more intensive lowering of LDL cholesterol: 10. Kastelein JJP, Ginsberg HN, Langslet G, et al. ODYSSEY FH I
a meta-analysis of data from 170 000 participants in 26 and FH II: 78 week results with alirocumab treatment in 735
randomised trials. Lancet 2010; 376(9753): 1670-1681. patients with heterozygous familial hypercholesterolaemia. Eur
For all Southern African 3. Klug EQ, Raal FJ, Marais AD, et al. South African Dyslipidaemia Heart J 2015; 36(43): 2996-3003.
healthcare professionals Guidelines Consensus Statement: 2018 update. A joint 11. Giugliano RP, Pedersen TR, Park J-G, et al. Clinical efficacy and
statement from the South African Heart Association (SA Heart) safety of achieving very low LDL-cholesterol concentrations
and the Lipid and Atherosclerosis Society of Southern Africa with the PCSK9 inhibitor evolocumab: a prespecified secondary
(LASSA). S Afr Med J 2018; 108(11b): 973-1000. analysis of the FOURIER trial. Lancet 2017; 390(10106): 1962-
4. Klug EQ, Raal FJ. New cholesterol targets for patients at high 1971.
or very high cardiovascular risk and the indications for PCSK9 12. Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and
inhibitors (Letter to the editor). S Afr Med J 2020; 110(11): cardiovascular outcomes after acute coronary syndrome. N Engl
1059. J Med 2018; 379: 2097-2107. DOI: 10.1056/NEJMoa1801174
5. Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe added 13. Hooper AJ, Marais AD, Tanyanyiwa DM, et al. The C679X
to statin therapy after acute coronary syndromes. N Engl J Med mutation in PCSK9 is present and lowers blood cholesterol
Find us at 2015; 372(25): 2387-2397. in a Southern African population. Atherosclerosis 2007; 193:
6. Hovingh G K, Davidson MH, Kastelein JJP, et al. Diagnosis and 445-448.
treatment of familial hypercholesterolaemia. Eur Heart J 2013; 14. Blom DJ, Breedt J, Burgess LJ, et al. Long-term safety
34(13): 962-971. and efficacy of alirocumab in South African patients with
DeNovo Medica
7. Stein EA, Mellis S, Yancopoulos GD, et al. Effect of a heterozygous familial hypercholesterolaemia: the ODYSSEY
monoclonal antibody to PCSK9 on LDL cholesterol. N Engl J Open-Label Extension study. Cardiovasc J Afr 2019; 30(5):
Med 2012; 366: 1108-1118. 279-284.
8. Ridker PM, Tardif J-C, Amarenco P, et al. Lipid-reduction
@deNovoMedica
deNovo Medica
This summary report was compiled Disclaimer Published by
for deNovo Medica by © 2021 deNovo Medica
The views and opinions expressed in the article are those of the presenters and do not necessarily reflect Reg: 2012/216456/07
Julia Aalbers those of the publisher or its sponsor. In all clinical instances, medical practitioners are referred to the 70 Arlington Street, Everglen, Cape Town, 7550
BSc Hons product insert documentation as approved by relevant control authorities. Tel: (021) 976 0485 I info@denovomedica.com
8 I JANUARY 2021You can also read