REPORT TO THE SLEEP HEALTH FOUNDATION 2016 SLEEP HEALTH SURVEY OF AUSTRALIAN ADULTS ROBERT ADAMS, SARAH APPLETON, ANNE TAYLOR, DOUG MCEVOY, AND ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Report to the Sleep Health Foundation 2016 Sleep Health Survey of Australian Adults Robert Adams, Sarah Appleton, Anne Taylor, Doug McEvoy, and Nick Antic. The University of Adelaide The Adelaide Institute for Sleep Health
2016 Sleep Health Survey of Australian Adults Executive Summary
Sleep problems are common
It is apparent that inadequate sleep, of either duration or quality, and its daytime consequences
are very common in Australian adults, affecting 33-45% of adults.
These problems occur across all age groups.
Medical sleep conditions are also very common, with diagnosed sleep apnea affecting 8%,
significant insomnia 20% and restless legs 18% of adults.
Average reported sleep time is 7 hours, although 12% sleep less than 5 ½ hours and 8% over 9
hours. Three-quarters (76%) who sleep less than 5 ½ hours report frequent daytime impairment
or sleep-related symptoms.
Frequent, loud snoring is reported by 24% of men and 17% of women. Frequent, loud snoring
and breathing pauses in sleep are more often seen in middle age. Among those with frequent,
loud snoring, 70% report daytime impairment or other sleep-related symptoms.
Among the 19% of people with frequent loud snoring and/or witnessed breathing pauses but no
prior diagnosis of OSA on a sleep study, 63% report awakening unrefreshed, and 65% report
one or more daytime sleep-related symptoms, suggesting undiagnosed sleep apnea is relatively
common in the community.
The effect of the ‘24/7 society” is profound.
A quarter of all adults (26%), both use the internet most or every night of the week just before
bed and have frequent sleep difficulties or daytime impairments. Similarly, 16% of all working
adults do work just before bed and also have frequent sleep difficulties or daytime sleep-related
symptoms.
Nearly a quarter (23%) report their typical weekday routine of work or home duties does not
allow them to get enough sleep.
Younger adults (18-34y) sleep around 1 hour longer before non-work days that working days,
compared to 18 minutes in older age groups.
Sleep problems have a major effect on work performance.
In the past month 17% have missed work because they were sleepy and 17% have also fallen
asleep on the job. In the past 3 months 29% of adults report making errors at work due to
sleepiness or sleep problems.
People with sleep problems are significantly more likely to report decreased work productivity
(as assessed on the Stanford Presenteeism Scale).
Sleepiness and sleep problems are a major source of risk on our roads.
Driving while drowsy at least every month is reported by 29% of people, 20% have nodded off
while driving and 5% have had an accident in the past year because they dozed off.
Sleep problems may be increasing in the community
The prevalence of sleep difficulties and daytime consequences appears to have increased since
2010, with various sleep problems reported by more adults than in 2010.
2Contents Page
Executive Summary 2
Introduction 4
Methods 5
Results 7
Sleep difficulties and clinical sleep conditions 7
Daytime symptomatology 7
Sleep duration 7
Insomnia 8
Chronic illness and sleep 8
Burden of sleep problems in relation to sleep disorders 8
Activities done in the hour before bed 8
Sleep habits and environmental influences 9
Causes of sleep disturbance 9
Effect of sleep problems on work and social activities 9
Effect of sleep habits and routine on sleep quality and daytime functioning 10
Changes in sleep problems since 2010 11
Discussion 12
References 14
Tables
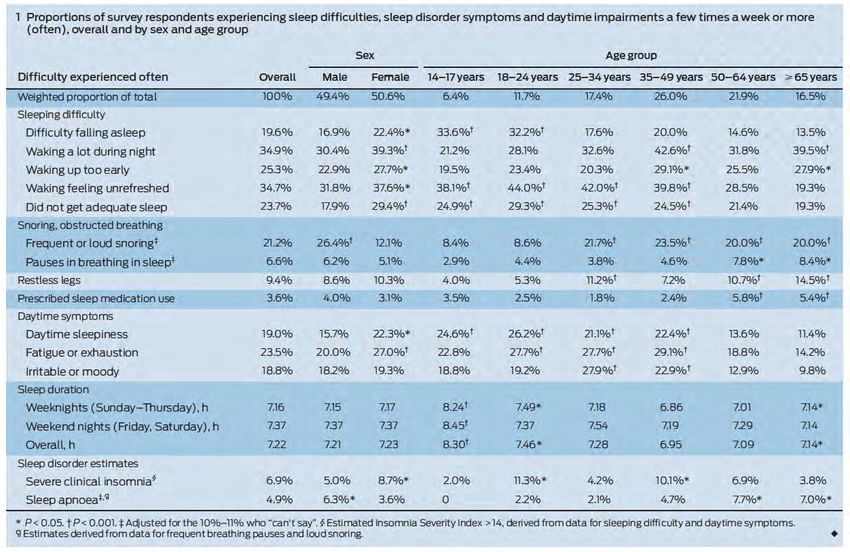
Table 1. Prevalence (%) of sleep difficulties, sleep disorder symptoms and daytime 17
impairments a few times a week or more.
Table 2. Prevalence (%) of sleep problems in relation to sleep apnoea, symptoms and 18
comorbidities.
Table 3. Sleep problems and daytime problems experienced ≥3 times/week among people 20
1) without OSA or OSA symptoms or restless legs symptoms, 2) likely undiagnosed OSA
3) diagnosed OSA, and 4) only restless legs symptoms.
Table 4. Prevalence of activities conducted in the hour before going to bed in the last month 21
in relation to sex and age.
Table 5. Approach to sleep problems and sleep aid use in relation to sex and age. 23
Table 6. Reported causes of sleep disturbance and effect on relationships. 25
Table 7. Sleep problems and effect on driving, work and social life. 26
Table 8. Mean (SD) Stanford Presenteeism Scale scores in relation to sleep factors. 28
Table 9. Prevalence (%) of sleep problems in relation to activities conducted in the hour 29
before bed and sleep hours.
Appendix A
Table 1. Sociodemographic characteristics of survey participants. 31
Figure 1. Results from the 2010 Sleep Health Foundation Survey 32
Appendix B
Sleep survey questionnaire 33
Cover photo: Lautrec in bed, 1893. Henri de Toulouse-Lautrec. Wikipedia Commons.
3Introduction Sleep is a fundamental biological requirement for human health. Over the past 20 years there has been increasing interest in the bidirectional association between sleep and adverse health effects. Sleep disorders can affect the quality of sleep and insufficient time allowed or available for sleep can also lead to inadequate sleep or sleep quality. Specific sleep disorders, such as obstructive sleep apnea (OSA), have been strongly linked to a variety of health problems and chronic diseases, such coronary heart disease, stroke, atrial fibrillation, diabetes, hypertension, depression, erectile dysfunction, nocturia, cognitive impairment and mortality risk.1-6 Symptoms of sleep problems, such as snoring and breathing pauses during sleep have also been associated with increased risk of heart disease.7 Insomnia, defined as difficulty getting off to sleep or maintaining sleep with daytime symptoms such as fatigue, is also associated with increased risk of mortality.8-10 Shortened sleep time also carries health risks and may adversely affects metabolic health through changes in the activity of neuroendocrine systems.11 Studies show sleeping less than six or seven hours on average per night may increase the risk for obesity,12, 13 type 2 diabetes,14, 15 and heart disease.16 Sleep deprivation affects the body’s metabolism, including glucose metabolism. Laboratory studies have consistently found short-term sleep loss decreases glucose tolerance and insulin sensitivity.17 Research has also found that when sleep-deprived, people increase intake of comfort foods high in fat and sugar.18 These changes to body metabolism and eating behavior with sleep-deprivation will tend to increase the risk of obesity and diabetes. Population level studies have also shown that people who sleep less than 8 hours on average have a higher body mass index and show changes in the hormones that control appetite, such as ghrelin, contributing to the risk of obesity.19 Short sleep also reduces natural immune function,20 increasing the risk of infections and possibly cancer. Reduced sleep is also liked to hypertension and heart disease, possibly by triggering over- activity in the body’s stress responses such as sympathetic hyperactivity or inflammation. 21, 22 Sleep disorders, other sleep problems and insufficient sleep are linked to cognitive function and mental well-being. Disturbance in mood, thinking, concentration, memory, learning, vigilance and reaction times have been reported.23, 24 Problems with sleep have a substantial economic and social cost. Increase risk of motor vehicle and workplace accidents, as well as decreased workplace performance and productivity have been associated with sleep problems. Deloitte Access Economics estimated that in 2010 the healthcare costs of the three most common sleep disorders, OSA, primary insomnia and restless legs, was $818 million. Indirect financial and non-financial costs of these sleep disorders were estimated at a further $4.3 billion. The scope of sleep problems in Australia has been examined in only a few studies. In 2010 the Sleep Health Foundation commissioned a telephone survey of 1512 Australians aged 14 to
Methodology
The survey was conducted in March 2016 on behalf of the Sleep Health Foundation among 1,011
adults aged over 18 years across Australia, with representativeness for age, sex, location and an
indicator of socio-economic status. Researchers from The University of Adelaide were responsible
for the survey design and analysis.
The study objective was to assess the scale of the health and social consequences of insufficient
sleep and sleep disorders in Australia. The survey aimed to measure the prevalence and economic
impacts of sleep problems in Australia, including sleep loss, insufficient sleep, and sleep disorders,
including sleep apnea, insomnia and restless legs syndrome. The economic impact includes
absenteeism, reduced productivity and performance.
The survey questions are taken largely from the 2002 US National Sleep Foundation Sleep in
Adults survey with some additional questions from the Australian 2005 Sleep in Adults survey plus
further items that examined the impact of sleep on work, including absenteeism and work
performance. The Stanford Presenteeism Scale (SPS) 25 was also used to examine work
performance. The SPS measures workers’ perceptions of their ability to overcome the distraction of
physical and/or psychological problems in order to handle job stress, complete tasks, achieve goals
and maintain sufficient focus and energy levels. The scale measures two factors that the authors
labeled as completing work and avoiding distraction.
The questionnaire is included as Appendix B.
The survey was conducted online by the Survey Sampling International (SSI) research organization.
SSI have developed a panel of over 220,000 Australians who are invited to complete surveys for a
small remuneration. Participants are selected from SSI’s online sample blend, a consistently-
managed, diverse and large frame. To minimize the risk of bias, SSI uses a three-stage
randomization process in matching a participant with a survey they are likely to be able to complete
To minimize the risk of bias, SSI uses a three-stage randomization process in matching a participant
with a survey they are likely to be able to complete. First, participants are randomly selected from
SSI’s panels to be invited to take a survey, and these participants are combined with others entering
SSI’s DynamixTM sampling platform after responding to online messaging. A set of profiling
questions is randomly selected for them to answer (these are methodologically correct questions,
never affirmation questions) and upon completion, participants are matched with a survey they are
likely to be able to take (ie the sleep survey), using a further element of randomization. Invitations
to participate include e-mail invitations, telephone alerts, banners and messaging on SSI panel
community sites. The messages themselves are also varied, including invitations to give your
opinion, or let your voice be heard. A diversity of motivation contributes to high-quality sample. To
avoid self-selection bias, specific project details are not generally included in the invitation. Rather,
participants are invited to “take a survey.” The details are disclosed later, when a survey has been
selected within the system.
The survey methodology was approved by The University of Adelaide Office of Research Ethics,
Compliance and Integrity’s Human Research Ethics Secretariat (H-2016-029).
Statistical analysis and power
Data were analyzed using IBM SPSS version 20.0 (IBM Corporation, Armonk, NY, USA). T-tests
and ANOVA determined mean levels of continuous variables (e.g. sleep duration, Stanford
Presenteeism Scale) in relation to sex, age, and sleep factors. Differences in the distribution of other
5sleep variables were determined with the Pearson Chi-square or Linear-by-linear association statistic (Mantel-Haenszel) for testing the presence of a linear trend. A sample size of 1000 provides estimates of proportions to within +/- 2.5%, and of means of +/- 1%. For estimating differences between groups this sample size will provide 99% power of detecting a small effect size (Cohen’s d
Results
The sample was generally representative of the Australian population with regards to age, gender,
income and geographic location across states and metropolitan and rural locations (see Appendix A,
Table 1). The sample had a higher proportion with post-school qualifications, particularly
Bachelor degrees or higher, than population estimates. The survey completion time was 15-20
minutes.
Sleep difficulties and clinical sleep conditions (Table 1)
The percentage of adults who report difficulties sleeping at least a few times a week or more, is
high. Females (40%) are more likely than males (26%) to experience difficulty in falling asleep
with little difference across age groups. Nearly half (47%) of women wake often overnight, which
is a problem that also increases significantly with age. Problems with waking early and not being
able to easily get back to sleep also increase with age. However, older age groups are significantly
more likely to report getting adequate sleep and less likely to report awakening unrefreshed than
younger adults. Frequent, loud snoring is reported by 24% of men and 17% of women, and is less
common among younger adults. Frequent, loud snoring and breathing pauses in sleep are more
often seen in middle age, but symptoms of restless legs are constant across age groups.
Diagnosed sleep disorders are common. A doctor-diagnosis of sleep apnea was over 3 times more
common in men than women, although the gender difference in the cardinal symptoms of sleep
apnea, i.e. snoring, breathing pauses and daytime symptoms, was much less pronounced. For
example, 9% of women and 14% of men report breathing pauses, a defining feature of sleep apnea.
Very high percentages (70-80%) of people with symptoms of clinical sleep disorders (i.e. frequent
snoring, observed breathing pauses, restless legs) also reported having two or more of problems
with daytime symptoms such as sleepiness, or sleep difficulties, such as problems getting off to
sleep, compared with around 40% of people without symptoms of clinical sleep disorders (see
Table 2).
Daytime symptomatology
Daytime symptoms related to insufficient or unrefreshing sleep, such as sleepiness, fatigue or
feeling irritable are common, being seen in 30-39% of adults. These symptoms are significantly
more common among younger age groups than older adults, with these problems occurring in
around half of 18-24y, twice the level of those >65y. Pathological daytime sleepiness where people
describe a strong tendency to doze off, as assessed by the Epworth Sleepiness Scale (ESS), is also
significantly more common in younger adults. Over one-quarter of people aged 18-35 years (27%)
have an abnormal ESS score, double the prevalence of older adults (65+ years – 13%).
Sleep Duration
Duration of reported sleep was around 7 hours on average on week-days (or before working days)
but 35 minutes longer on week-ends (or non-working days), which varied little by gender. Although
there was little difference across age groups in sleep time during the working week, younger adults
slept an hour or more longer before non-working days, significantly more than older adults. The
distribution of sleep time is large, with a standard deviation in 18-24y of over 2 hours, indicating
many people, especially younger adults, sleep for much less than the average time. Overall, 12% of
adults sleep less than 5 ½ hours, with 8% sleeping over 9 hours on average. Although difficulties
with sleep onset and maintenance and daytime sleep-related symptoms are more common in women
than men, the amount of time spent sleeping and the use of prescribed sleep medications does not
differ between the sexes.
7Insomnia
The criteria for clinically significant insomnia by The International Classification for Sleep
Disorders-3 classification26 includes a report of sleep initiation or maintenance problems and
daytime consequences (daytime sleepiness /fatigue or exhaustion/ irritable or moody) at least three
times per week with adequate opportunity and circumstances to sleep. This constellation of
symptoms of insomnia was present in 20% of adults. Although significantly more common in
women (23%), insomnia was also estimated to be present in 17% of men. Insomnia was also seen
more often among young and late middle-aged adults than the elderly. Prescribed sleep medication
is used at least a few times a week by 9%, more often by the middle-aged (35-54y) than other age
groups.
Chronic illness and sleep (Table 2)
The effect of chronic illness on sleep is also significant. Multimorbidity, or a higher number of
comorbid chronic diseases in an individual, was associated with higher frequency of 2 or more
sleep difficulties or daytime symptoms. Among those 4 or more chronic conditions, 68% reported
having 2 or more sleep difficulties, compared to 36% of those with no chronic conditions. Some
specific, individual conditions (heartburn/reflux; depression; anxiety; lung disease) are associated
with higher frequency of sleep difficulties than people without those individual conditions.
Burden of sleep problems in relation to sleep disorders (Table 3)
To examine the relative effect of clinical sleep conditions on the population burden of sleep
problems, the prevalence of sleep symptoms and daytime sleep-related symptoms reported ≥3
times/week were compared among people: 1) without diagnosed OSA or OSA symptoms or restless
legs symptoms; 2) with diagnosed OSA (with or without restless legs symptoms) ; 3) with likely
undiagnosed OSA, defined as loud snoring and/or witnessed breathing pauses at least 3 times/week
but no prior diagnosis of OSA on a sleep study (with or without restless legs symptoms), and 4)
with restless legs symptoms only. Although the percentage of frequent sleep problems or daytime
symptoms was lower in the group without OSA or restless legs, the absolute total number in this
group was similar to those with specific clinical conditions
Activities done in the hour before bed (Table 4)
It is common for people to do activities in the hour before bed that may affect their sleep. Overall,
44% of adults (47% women, 40% men) are on the internet just before bed almost every night. This
is more frequent in younger people (18-24y – 75%; 25-34y – 55%) but even in over 65y 22% use
devices before sleeping. Work intrudes late into the evening for many. At least a few nights per
week, 17% do job-related work before sleeping. This is common in younger adults, with 36% of 18-
24y and 28% of 25-34y working before bed. Over half of adults watch TV (52%) before bed
although the age distribution is reversed from internet use, with 35% of 18-24 year olds, TV
watching compared to 66% of those 65 years and over. Age differences are seen for other
behaviours as well. Young adults also more likely to have a hot bath or shower before bed a few
nights per week, with 48% of 18-24 year olds reporting this behaviour compared with 32% of over
65 year olds. The young are also more likely to have sex before sleeping a few nights per week,
reported by 30% of 24-35y compared with 8% of 55-64yo. However, they are less likely to drink
alcohol (18-24y – 14%; 45-64y – 26%).
8Sleep habits and environmental influences (Table 5)
Nearly a quarter of adults report their typical routine does not allow them to get enough sleep, with
this figure rising to around 30% in the prime working ages of 18-44y. Many people take naps, with
40% napping at least twice weekly. This was common across age groups, with 35% of 35-44y
napping twice weekly or more. Napping was more common among men, with 44% of men taking 2
or more naps per week, compared with 36% of women. Among women who nap, 26% sleep for
over 1 hour, compared to 16% of men.
Nearly a quarter (24%) of adults think that they have a sleep problem, and although more common
in older adults, reported by 31% of 55-64 year olds, 21 % of 18-24yo consider they have a sleep
problem. There was little difference by gender. What individuals would do if they thought they had
a sleep problem also varied by age. Younger adults were more likely to assume a sleep problem
would go away and were less likely to talk to a doctor than older adults.
Only a minority of adults report using sleep aids, such as medications. Over-the counter
preparations are used by 7% of people a few nights per month and by 5% most nights. Prescribed
sleep medications from a doctor are used by 5% on a few nights per month and by 8% most nights.
There was little difference by gender in the reported use of sleep aids, and no significant difference
across age groups.
Many adults consume caffeinated drinks, with over one-third (34%) of adults taking in 4 or more
caffeinated drinks per day. Caffeine intake is more common among older age groups, with 40% or
more of over 45y taking in 4 or more drinks per day, compared with 9% of 18-24yo.
Causes of sleep disturbance (Table 6)
Half of women (50%) and 38% of men find it somewhat or very difficult to get back to sleep if they
are awoken during the night. Nominated causes of awakening from sleep include environmental
stimuli such as noise, reported by 50%, and light, by 27%. Cognitive or emotional issues such as
stress (28%), thinking about work (24%), or nightmares (24%) and physical or health reasons,
including pain (25%) and going to the bathroom (60%) are other common reasons for disturbance
from sleep. All of these reasons are more common in women than men. Cognitive or emotional
reasons such as stress are more common among younger adults whilst physical reasons for sleep
disturbance such as pain occur more frequently with age. For 1 in 7 adults (14.3%) a partner’s sleep
problem has a moderate or significant effect on the couple’s relationship.
Effect of sleep problems on work and social activities (Table 7)
Seventeen percent of people report missing at least one day of work in the past four weeks because
they were too sleepy or had a sleep problem. This was especially common in younger adults, with
27% of 18-24y and 30% of 24-35y reporting days off from sleepiness. Errors at work from
sleepiness or sleep problems are also common, with 20% reporting errors on 1-2 days in the past 3
months, and 9% on 3 or more days. Again this was more common in younger adults, with around
half of 18-34y reporting errors at work from sleep problems at least 1-2 days in the past 3 months.
Sleep problems are a common reason people are late for work, with 14% of men and 21% of
women reporting being late because they were too sleepy when they woke up or have a sleep
problem. Further, 21% of men and 13% of women have fallen asleep at work in the past month,
which is a common finding up to the age of 55y. Sleep related decreases in productivity, where
workers are present at work but have a reduced ability to finish tasks, focus on work and cope with
distractions (also known as presenteeism), were also common. Specifically, people who report sleep
9problems, have observed breathing pauses during sleep, or restless legs, report significantly more
work impairments, as assessed by the Stanford Presenteeism Scale (SPS, Table 8). The difference
in SPS scores between those with two or more sleep problems and those with zero or one, was
around half of a standard deviation, indicating at least a moderate effect size on work performance
from sleep problems. Sleep-related work impairment was more likely among younger adults aged
18-34y compared to older adults aged over 55y.
Being too sleepy or a having sleep problem is also a common reason for missing social activities,
with 22% of men and 27% of women reporting missing social events on at least 1 day in past 3
months. Again this was more common in younger age groups, affecting 45% of 18-24y and 37% of
24-34y.
Drowsiness while driving is also common. Being drowsy when driving occurring at least every
week is reported by 17% of men and 15% of women, and 29% report doing so at least monthly.
This figure varies by age, with 30% of 25-34yo, compared with less than 1% of over 65yo. A
further 13% of adults report driving while feeling drowsy once or twice a month. One-fifth of adults
(22% men, 17% women) have nodded off while driving, with 5% have had a motor vehicle accident
in the past year because they dozed off or were too tired. Reported accidents from sleepiness were
more common among younger adults, reported by 10% of 25-34y.
Effect of sleep habits and routine on sleep quality and daytime functioning (Table 9)
Nearly half of adults (48%) report having 2 or more sleep-related problems or difficulties (i.e.
difficulty falling asleep, waking up a lot overnight, daytime sleepiness, daytime fatigue or
exhaustion, feeling irritable or moody or pathological daytime sleepiness [ESS>10]).
Of the 22% of people who report doing work related to their job in the hour before bed a few nights
of the week or more, 69% have 2 or more sleep problems, significantly more than adults who do not
work before bed. Similarly, of the 44% of people who use the internet most or every night of the
week, that figure is 59%, i.e. 26% of adults both use the internet most or every night of the week
and also have 2 or more sleep difficulties or daytime symptoms. Among the 12% of adults who
sleep less than 5 ½ hours before workdays, three quarters (76%), report 2 or more sleeping
difficulties or daytime symptoms, compared to 43% of those who sleep more than 5 ½ hours.
Higher caffeine use is associated with higher likelihood of sleep problems. Among those who do
not consume caffeinated drinks, 40% report ≥2 sleep problems, compared with 61% who consume
≥6 caffeinated drinks per day.
10Comparison with 2010 survey
In 2010, a national landline telephone survey of adolescents and adults between 14 to > 70 years of
age) was conducted across successive weekend evenings by Roy Morgan Research on behalf of the
Sleep Health Foundation. There were 1512 respondents from all states and territories, both urban
and rural, with sampling proportionate to the populations of those areas, sex and age. Results of this
survey were published by Hillman and Lack in 2013.27 Although differences in survey methodology
exist between this survey and the current one, including use of landline telephones and sample size
(1415 adults aged over 18y), it is instructive to compare results from the two surveys as 14 identical
items were asked in the two surveys.
Overall, comparison of the results from the previous survey shows reported increases in the
prevalence of sleep problems in Australia since 2010 (see Appendix A, Figure 1). The number of
adults who report sleep difficulties more than a few times per week, such as difficulty falling asleep,
awakening unrefreshed and who report they did not get adequate sleep has increased. These
changes were seen across all age groups, including older adults aged >65 years. The use of
prescribed sleep medication has increased to match, particularly in younger adults aged 18-34 years.
The percentage of adults who have daytime symptoms related to insufficient or unrefreshing sleep,
such as daytime sleepiness, fatigue or irritability, has also shown an increase. These changes were
more pronounced in younger adults, especially 18-24 year olds, where over half now report
sleepiness or fatigue most days. The length of self-reported time asleep has remained fairly
constant at around 7 hours on workdays, with a consistent finding of increased sleep on non-
working days.
Diagnosed, clinical sleep disorders have also increased, although not universally. Doctor-diagnosed
sleep apnea prevalence has doubled in men to 12.9%, although the prevalence of frequent, loud
snoring has not altered much. However diagnosed sleep apnea prevalence has remained unchanged
in women.
Despite increasing awareness in the general media and medical literature of the potential adverse
consequences of poor sleep, the prevalence of sleep problems appears to have not improved since
2010.
11Discussion
The results from this national survey of Australian adults shows that sleep problems, related to
clinical sleep disorders and/or lifestyle and behavioural choices, produce a considerable burden on
public health, social life and workplace functioning. Nearly half of adults report having two or more
sleep-related problems, such as difficulty initiating or maintaining sleep, or daytime sleepiness or
fatigue. Much of this is due to competing demands on people’s time, with a quarter of all adults
reporting their usual routine does not allow them to get enough sleep. Lifestyle choices affecting
sleep habits, such as working or using the internet just before bed, are also having adverse effects
on sleep and daytime performance. The data shows insufficient or inadequate sleep adversely
effects social events and workplace performance, with absenteeism and falling asleep at work
common. Alarming numbers report driving when drowsy, and the frequency that young, relatively
inexperienced drivers report accidents after dozing off is also a major concern. Although
comparisons with the previous 2010 survey should be made with caution due to differences in
methodology, it certainly appears sleep problems and their consequences are increasing in scope
and frequency. Whilst specific issues vary with age, sleep-related problems occur frequently across
all age groups. Overall, the picture emerges of a nation whose health, social life and productivity is
suffering from lack of quality sleep.
Specific diagnosed sleep conditions, such as sleep apnea, are common. However, many continue to
report significant sleep-related symptoms following a clinical diagnosis. For instance, a quarter of
people with diagnosed sleep apnea report pathological daytime sleepiness on the Epworth
Sleepiness Scale (ESS)28 and over half report one or more daytime sleep-related symptom such as
fatigue or irritability. It is also likely that under-diagnosis of sleep apnea is also common. Around
10% of the population report frequent loud snoring with observed breathing pauses during sleep,
cardinal symptoms of sleep apnea. Less than half of these people feel they get adequate sleep and
22% also have abnormal ESS scores. Snoring and breathing pauses during sleep have also been
associated with increased risk of heart disease.7 It seems that there is potential to substantially
improve both the diagnosis and treatment of sleep apnea to reduce the population health burden of
this condition. Recognition by clinicians and in the community that snoring may not be a benign
symptom and that daytime impairment may have a pathological cause is an important first step.
Although it is often assumed sleep problems are a feature of ageing our results in general did not
bear this out. In this our results were consistent with recent reports from the HypnoLaus population
study in Switzerland, in that older people complained less about sleepiness, and pathological
sleepiness was significantly lower than in younger subjects.29 Self-reported sleep quality and
daytime functioning also improved with aging. Whilst sleep apnea and awakening overnight
increased with age, our findings were consistent with those of the HypnoLaus study authors29 who
concluded that “sleep complaints should not be viewed as part of normal aging but should prompt
the identification of underlying causes”.
Our data shows many people, particularly younger adults, require “catch-up” sleep on days off from
work after limited weekday or workday sleep. Social jet lag refers to the phenomenon where
individuals have different sleep schedules for workdays than days off. Commonly this occurs when
people with delayed sleep times on workdays force themselves onto daytime society’s schedule
with extra sleep on days off.30 This misalignment of sleep timing is associated with metabolic risk
factors that predispose to diabetes and atherosclerotic cardiovascular disease, including raised
cholesterol, triglycerides and insulin resistance.31 Delayed sleep problems are reportedly common in
adolescents but we found the need for catch-up sleep is common up to at least age 35y. This is
associated with pre-sleep habits that will work against quality sleep, such spending time on the
Internet and working up until bedtime. We also found these lifestyle behaviours, whether forced by
circumstance or by choice, that limit sleep are strongly associated with daytime symptoms and
12reduced workplace performance. There is some evidence that catch-up sleep may ameliorate some
of the adverse effects of reduced sleep. In one study, three nights of 'catch-up' sleep improved
insulin sensitivity and testosterone in men with chronic, repetitive sleep restriction.32 However, the
weekend sleep-in can contribute to circadian rhythm disruption and difficulties in establishing a
sleep routine. The frequency of impaired daytime functioning suggests that currently the adequacy
of a catch-up sleep strategy is insufficient for many people in the community.
Chronic sleep restriction has been linked to cardio-metabolic disorders.11, 24, 33 Lifestyle behaviours
and choices influence sleep. A quarter of adults report use of the internet most or every night of the
week just before bed and also have 2 or more sleep difficulties or daytime symptoms. The intrusion
of work into non-work lives is also associated with adverse effects on sleep and daytime
functioning, including workplace productivity. The data indicates that the population burden of
sleep problems in the community likely related to lifestyle choices of sleep habits and duration
rivals that of clinical disorders. There is potential to improve sleep and consequences of inadequate
sleep with relatively simple lifestyle changes.
Sleepiness or sleep problems were a common reason for work absenteeism, errors at work, reduced
punctuality and dozing off at work. Presenteeism, where workers are physical present but less than
fully functional, was significantly more common among those with sleep problems. A number of
authors have found that performance-based work loss or presenteeism represented a far greater
proportion of lost productivity compared with absenteeism.34-37 US estimates are that presenteeism
accounted for approximately three-quarters of the loss in national productivity.38, 39 The implication
from this is that interventions that focus on absenteeism and ignore presenteeism not only
underestimate the true magnitude of the impact of health on productivity, but also may not
accurately characterize the financial return on health interventions.40 The difference in work
impairment among those with observed breathing pauses in sleep compared to those with a
diagnosis of sleep apnea, suggests there remains a significant burden of under-diagnosed sleep
apnea in the community on workplace productivity. The SPS measures an individual’s perception
of their ability to avoid distraction and complete tasks and it can be asked whether self-perception
regarding work performance may not always be accurate. However, much research has found that
self-reporting measures are reliable and accurate.41, 42
The limitations of a self-report survey may have affected our results. Many people with insomnia
misperceive their sleep, with the tendency to overestimate sleep latency and underestimate total
time asleep.43 However, self-reported sleep restriction and perceived poor sleep quality is associated
with increased all-cause mortality risk among younger and older people in some studies,44 as well as
hypertension,45 heart disease,16 and diabetes.14 The survey sample was closely matched to the
general population for age, gender, income and geographic distribution, but respondents were on
average better educated than the general population, which may have influenced the study results.
In conclusion, sleep problems, inadequate sleep and poor sleep quality are common and have
adverse health, social and economic costs. There is significant potential to improve this situation
but this will require concerted action from a number of key players. These include health care
providers and peak bodies increasing their advocacy for healthy sleep to become a higher priority to
the community. Despite to relationship to general health and to key national priorities such as
obesity, cardiovascular disease and diabetes, healthy sleep is not a national health priority or given a
high priority in healthcare policy. The data in this report indicates this situation deserves to be
rectified.
13References
1. Kendzerska T, Gershon AS, Hawker G, Leung RS, Tomlinson G. Obstructive sleep apnea
and risk of cardiovascular events and all-cause mortality: a decade-long historical cohort study.
PLoS Med 2014;11:e1001599.
2. Kendzerska T, Gershon AS, Hawker G, Tomlinson G, Leung RS. Obstructive sleep apnea
and incident diabetes. A historical cohort study. Am J Respir Crit Care Med 2014;190:218-25.
3. Kendzerska T, Mollayeva T, Gershon AS, Leung RS, Hawker G, Tomlinson G. Untreated
obstructive sleep apnea and the risk for serious long-term adverse outcomes: A systematic review.
Sleep Med Rev 2014;18:49-59.
4. Loke YK, Brown JW, Kwok CS, Niruban A, Myint PK. Association of obstructive sleep
apnea with risk of serious cardiovascular events: a systematic review and meta-analysis. Circulation.
Cardiovascular quality and outcomes 2012;5:720-8.
5. Bucks RS, Olaithe M, Eastwood P. Neurocognitive function in obstructive sleep apnoea: a
meta-review. Respirology 2013;18:61-70.
6. Wang XIA, Bi Y, Zhang Q, Pan F. Obstructive sleep apnoea and the risk of type 2 diabetes:
A meta-analysis of prospective cohort studies. Respirology 2013;18:140-6.
7. Niiranen TJ, Kronholm E, Rissanen H, Partinen M, Jula AM. Self-reported obstructive sleep
apnea, simple snoring, and various markers of sleep-disordered breathing as predictors of
cardiovascular risk. Sleep Breath 2016;20:589-96.
8. Li Y, Zhang X, Winkelman JW, et al. Association Between Insomnia Symptoms and
Mortality: A Prospective Study of US Men. Circulation 2014;129:737-46.
9. Vgontzas AN, Liao D, Pejovic S, et al. Insomnia with short sleep duration and mortality: the
Penn State cohort. Sleep 2010;33:1159-64.
10. Kripke D, Garfinkel L, Wingard D, Klauber M, Marler M. Mortality associated with sleep
duration and insomnia. Arch Gen Psychiatry 2002;59:131 - 6.
11. Schmid SM, Hallschmid M, Schultes B. The metabolic burden of sleep loss. Lancet
Diabetes Endocrinol 2015;3:52-62.
12. Wu Y, Zhai L, Zhang D. Sleep duration and obesity among adults: a meta-analysis of
prospective studies. Sleep Med 2014;15:1456-62.
13. Gangwisch J, Malaspina D, Boden-Albala B, Heymsfield S. Inadequate sleep as a risk factor
for obesity: analyses of the NHANES I. Sleep 2005;28:1289 - 96.
14. Cappuccio FP, D'Elia L, Strazzullo P, Miller MA. Quantity and quality of sleep and
incidence of type 2 diabetes: a systematic review and meta-analysis. Diabetes Care 2010;33:414-20.
15. Ayas NT, White DP, Al-Delaimy WK, et al. A prospective study of self-reported sleep
duration and incident diabetes in women. Diabetes Care 2003;26:380-4.
16. Cappuccio FP, Cooper D, D'Elia L, Strazzullo P, Miller MA. Sleep duration predicts
cardiovascular outcomes: systematic review and meta-analysis of prospective studies. Eur Heart J
2011;32:1484-92.
17. Reynolds AC, Dorrian J, Liu PY, et al. Impact of five nights of sleep restriction on glucose
metabolism, leptin and testosterone in young adult men. PLoS One 2012;7:e41218.
18. Spiegel K, Tasali E, Penev P, Van Cauter E. Brief communication: Sleep curtailment in
healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased
hunger and appetite. Ann Intern Med 2004;141:846-50.
19. Taheri S, Lin L, Austin D, Young T, Mignot E. Short sleep duration is associated with
reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med 2004;1:e62.
20. Irwin M, McClintick J, Costlow C, Fortner M, White J, Gillin JC. Partial night sleep
deprivation reduces natural killer and cellular immune responses in humans. FASEB J 1996;10:643-
53.
1421. Konecny T, Kara T, Somers VK. Obstructive sleep apnea and hypertension: an update.
Hypertension 2014;63:203-9.
22. Torres G, Sanchez-de-la-Torre M, Barbe F. Relationship Between OSA and Hypertension.
Chest 2015;148:824-32.
23. Zhai L, Zhang H, Zhang D. Sleep duration and depression among adults: a meta-analysis of
prospective studies. Depression and Anxiety 2015;32:664-70.
24. Van Someren EJ, Cirelli C, Dijk DJ, Van Cauter E, Schwartz S, Chee MW. Disrupted Sleep:
From Molecules to Cognition. The Journal of neuroscience : the official journal of the Society for
Neuroscience 2015;35:13889-95.
25. Koopman C, Pelletier KR, Murray JF, et al. Stanford presenteeism scale: health status and
employee productivity. J Occup Environ Med 2002;44:14-20.
26. Sateia MJ. International classification of sleep disorders-third edition: Highlights and
modifications. Chest 2014;146:1387-94.
27. Hillman DR, Lack LC. Public health implications of sleep loss: the community burden. Med
J Aust 2013;199:S7-10.
28. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale.
Sleep 1991;14:540-5.
29. Luca G, Haba Rubio J, Andries D, et al. Age and gender variations of sleep in subjects
without sleep disorders. Ann Med 2015;47:482-91.
30. Okawa M, Uchiyama M. Circadian rhythm sleep disorders: characteristics and entrainment
pathology in delayed sleep phase and non-24-h sleep-wake syndrome. Sleep Med Rev 2007;11:485-
96.
31. Wong PM, Hasler BP, Kamarck TW, Muldoon MF, Manuck SB. Social Jetlag, Chronotype,
and Cardiometabolic Risk. J Clin Endocrinol Metab 2015;100:4612-20.
32. Killick R, Hoyos CM, Melehan KL, Dungan GC, 2nd, Poh J, Liu PY. Metabolic and
hormonal effects of 'catch-up' sleep in men with chronic, repetitive, lifestyle-driven sleep restriction.
Clinical endocrinology 2015;83:498-507.
33. Van Cauter E, Spiegel K, Tasali E, Leproult R. Metabolic consequences of sleep and sleep
loss. Sleep Med 2008;9 Suppl 1:S23-8.
34. Burton WN, Conti DJ, Chen CY, Schultz AB, Edington DW. The role of health risk factors
and disease on worker productivity. J Occup Environ Med 1999;41:863-77.
35. Goetzel RZ, Long SR, Ozminkowski RJ, Hawkins K, Wang S, Lynch W. Health, absence,
disability, and presenteeism cost estimates of certain physical and mental health conditions
affecting U.S. employers. J Occup Environ Med 2004;46:398-412.
36. Hemp P. Presenteeism: at work--but out of it. Harv Bus Rev 2004;82:49-58, 155.
37. Kessler RC, Akiskal HS, Ames M, et al. Prevalence and effects of mood disorders on work
performance in a nationally representative sample of U.S. workers. The American journal of
psychiatry 2006;163:1561-8.
38. Goetzel RZ, Ozminkowski RJ, Sederer LI, Mark TL. The business case for quality mental
health services: why employers should care about the mental health and well-being of their
employees. J Occup Environ Med 2002;44:320-30.
39. Stewart WF, Ricci JA, Leotta C, Chee E. Validation of the work and health interview.
Pharmacoeconomics 2004;22:1127-40.
40. Collins JJ, Baase CM, Sharda CE, et al. The assessment of chronic health conditions on
work performance, absence, and total economic impact for employers. J Occup Environ Med
2005;47:547-57.
41. Druss BG, Schlesinger M, Allen HM, Jr. Depressive symptoms, satisfaction with health care,
and 2-year work outcomes in an employed population. The American Journal of Psychiatry
2001;158:731-4.
1542. Lerner DJ, Amick BC, 3rd, Malspeis S, Rogers WH. A national survey of health-related
work limitations among employed persons in the United States. Disability and rehabilitation
2000;22:225-32.
43. Harvey AG, Tang NK. (Mis)perception of sleep in insomnia: a puzzle and a resolution.
Psychol Bull 2012;138:77-101.
44. Kurina L, McClintock M, Chen J, Waite L, Thisted R, Lauderdale D. Sleep duration and all-
cause mortality: a critical review of measurement and associations. Annals of epidemiology 2013;
23: 361 - 70.
45. Gangwisch JE, Heymsfield SB, Boden-Albala B, et al. Short sleep duration as a risk factor
for hypertension: analyses of the First National Health and Nutrition Examination Survey.
Hypertension 2006;47:833–9
16Table 1. Prevalence (%) of sleep difficulties, sleep disorder symptoms and daytime impairments a few times a week or more.
Overall Sex Age category p across
age
Male Female 18-24 25-34 35-44 45-54 55-64 ≥65
n 1011 503 508 121 184 195 182 154 175
% 49.8 50.2 12.0 18.2 19.3 18.0 15.2 17.3
Sleeping difficulty
Difficulty falling asleep 33.2 26.4 40.0† 41.3 31.5 29.7 34.6 33.1 32.0 0.40
Waking a lot during night 41.9 36.8 47.0† 25.6 31.0 42.6 47.3 49.4 52.0Table 2. Prevalence (%) of sleep problems* in relation to sleep apnoea, symptoms and
comorbidities.
Sleep symptoms and comorbidities % of ≥1 sleep ≥2 sleep
population problem problem
65.9% 48.4%
Frequent loud snoring ≥3 nights/week PTable 2 (cont’d). Prevalence (%) of sleep problems* in relation to sleep apnoea, symptoms
and comorbidities.
Sleep symptoms and comorbidities % of ≥1 sleep ≥2 sleep
population
problem problem
Diabetes P=0.64 P=0.29
No 89.8 66.7 49.2
Yes 10.2 64.4 43.6
Heartburn/GORD pTable 3. Sleep problems and daytime problems experienced ≥3 times/week among ~people 1)
without OSA or OSA symptoms or restless legs symptoms, 2) likely undiagnosed OSA 3)
diagnosed OSA, and 4) only restless legs symptoms.
Sleep symptoms and No OSA or Likely OSA Only p
comorbidities restless legs undiagnosed diagnosed restless
OSA* on a sleep legs
†
study
n=505 n=193 n=84 n=229
Difficulty falling asleep 21.2 48.2 31.0 48.0Table 4. Prevalence of activities conducted in the hour before going to bed in the last month in relation to sex and age.
Overall Male Female 18-24y 25-34y 35-44y 45-54y 55-64y ≥65y p across
age
n 1011 503 508 121 184 195 182 154 175
% 49.8 50.2 12.0 18.2 19.3 18.0 15.2 17.3
Activity
Work related to jobTable 4 (cont’d). Prevalence of activities conducted in the hour before going to bed in the last month in relation to sex and age.
Overall male female 18-24 25-34 35-44 45-54 55-64 ≥65 p across
age
ExercisedTable 5. Approach to sleep problems and sleep aid use in relation to sex and age.
Overall male female 18-24 25-34 35-44 45-54 55-64 ≥65 p across age
n 1011 503 508 121 184 195 182 154 175
% 49.8 50.2 12.0 18.2 19.3 18.0 15.2 17.3
Typical weekday routine (work/home duties) allows you to get enough sleep 60 min 20.4 15.6 25.7 35.9 13.7 25.8 20.2 18.2 12.3
Do you think you have a sleep problem? 0.02
Yes 23.6 23.1 24.2 20.7 17.4 19.0 29.1 31.2 25.1
No 51.2 53.3 49.2 52.1 55.4 55.9 48.9 46.1 48.0
Maybe 21.5 19.3 23.6 23.1 21.7 20.5 19.2 20.8 24.0
Don’t know/not sure 3.6 4.2 3.0 4.1 5.4 4.6 2.7 1.3 2.9
Approach to sleep problems if thought had a problem
Assume it will go away in time 27.1 28.0 26.2 48.8 36.4 25.1 24.2 21.4 12.6Table 5 (cont’d). Approach to sleep problems and sleep aid use in relation to sex and age.
Overall male female 18-24 25-34 35-44 45-54 55-64 ≥65 p across age
Frequency of sleep aid use
OTC sleep aids 0.70
Never/rarely 88.1 89.6 88.1 89.1 85.6 87.2 86.0 92.2 89.7
Few nights/month 6.9 5.7 6.9 6.7 10.0 8.5 8.4 3.2 4.0
Few nights/every or almost 4.9 4.7 4.9 4.2 4.4 4.3 5.6 4.5 6.3
every night/week
Doctor prescribed sleep medications 0.67
Never/rarely 87.1 87.0 87.3 88.2 85.1 87.8 84.9 91.6 86.3
Few nights/month 4.7 4.3 5.2 6.7 7.7 3.7 5.0 1.9 3.4
Few nights/every night/week 8.1 8.7 7.6 5.0 7.2 8.5 10.1 6.5 10.3
†
Alcohol/beer/wineTable 6. Reported causes of sleep disturbance and effect on relationships.
Overall male female 18-24 25-34 35-44 45-54 55-64 ≥65 p across
age
n 1011 503 508 121 184 195 182 154 175
% 49.8 50.2 12.0 18.2 19.3 18.0 15.2 17.3
Difficulty getting back to sleep if awoken during night † 0.31
Very difficult 10.8 9.8 11.9 8.3 7.7 12.4 11.0 11.7 13.1
Somewhat difficult 33.8 28.9 38.5 33.1 36.8 37.1 33.7 20.9 30.9
Not very/not at all difficult 52.7 57.7 47.8 56.2 51.6 46.4 52.5 56.5 55.4
Don’t know 2.7 3.6 1.8 2.5 3.8 4.1 2.8 1.9 0.6
What if anything awakens you during the night
Noise† 49.8 44.9 54.5 52.1 48.9 51.3 52.7 51.9 42.3 0.23
Light 27.2 26.6 27.8 32.2 31.5 24.6 31.3 22.1 22.3 0.019
†
Stress 27.9 21.3 34.4 33.1 32.1 31.3 31.3 24.0 16.0Table 7. Sleep problems and effect on driving, work and social life.
Overall male female 18-24 25-34 35-44 45-54 55-64 ≥65 p across
age
n 1011 503 508 121 184 195 182 154 175
% 49.8 50.2 12.0 18.2 19.3 18.0 15.2 17.3
Driving while feeling drowsy in past yearTable 7 (cont’d). Sleep problems and effect on driving, work and social life.
Overall male female 18-24 25-34 35-44 45-54 55-64 ≥65 p across
age
Reasons why late to work
Went to bed too late 10.1 10.1 10.2 10.4 16.3 8.9 7.8 9.0 0.0 0.02
Slept too late 13.0 11.8 14.3 27.1 21.5 11.0 8.6 4.5 0.0Table 8. Mean (SD) Stanford Presenteeism Scale scores in relation to sleep factors* Sleep symptoms and comorbidities Mean (SD) p ≥1 sleep problem
Table 9. Prevalence (%) of sleep problems in relation to activities conducted in the hour
before bed and sleep hours.*
Activity % of population ≥1 sleep problem ≥2 sleep problem
65.9% 48.4%
Sex pTable 9 (cont’d). Prevalence (%) of sleep problems in relation to activities conducted in the hour before bed and sleep hours.* Activity % of population ≥1 sleep problem ≥2 sleep problem Exercised p=0.61 p=0.09 Never/rarely 77.7 67.2 48.1 Few nights/month 9.2 51.6 36.3 Few nights/week 9.5 71.0 61.3 Every/almost every night/week 3.6 77.1 57.1 Number caffeinated drinks/day p
APPENDIX A
Appendix Table 1. Sociodemographic characteristics of survey participants [%, (n)]
Survey ABS
sample population
estimates
Sex Male 49.8 (503) 49.8
Female 50.2 (508) 50.2
Age 18-24 12.0 (121) 12.2
25-34 18.2 (184) 18.0
35-44 19.3 (195) 18.5
45-54 18.0 (182) 17.9
55-64 15.2 (154) 15.2
65 and over 17.3 (175) 18.3
State of residence ACT/NT 2.8 (28) 2.7
NSW 33.3 (337) 32.1
QLD 19.9 (201) 20.1
SA 7.4 (75) 7.4
TAS 2.1 (24) 2.3
VIC 24.9 (252) 24.9
WA 9.6 (97) 10.4
Area of residence Metropolitan 65.7 (664) 64
Rural 31.6 (319) 33.3
ACT/NT 2.8 (28) 2.7
Country of birth Australia 74.7 (755) 72
UK/Ireland 7.0 (71) 6
Rest of world 16.9 (171) 22
Refused 1.4 (14) -
Highest education level Still studying 4.4 (44) 6
High school 21.5 (217) 40
Trade/apprenticeship/
Certificate/Diploma 38.2 (387) 30
Bachelor degree or higher 34.5 (349) 24
Refused 1.4 (14) -
Household income $150,000 8.3 (84) 10.0
Refused/don’t know 15.1 (153) 10.9
31Figure 1. Results from the 2010 Sleep Health Foundation Survey, n=1512 (From Hillman DR, Lack LC. Med J Aust 2013;199:S7-S10).
32SLEEP SURVEY 2016
APPENDIX B.
Sleep Survey Questionnaire
33SLEEP SURVEY 2016
Sleep Survey
Questionnaire
2016
WELCOME PAGE
Thank you for agreeing to take part in this important survey regarding sleep and
health for The University of Adelaide.
I can assure you that all information given will remain confidential. The answers from
all people interviewed will be gathered together and presented in a report. No
individual answers will be passed on.
Whilst your input to the survey is very important to us, participation is voluntary and
you can choose not to answer any particular question or any section. You are free to
withdraw from the survey at any time.
The study has been approved by the Human Research Ethics Committee at the University of
Adelaide (approval number H-2015-xxx). If you have questions or problems associated with
the practical aspects of your participation in the project, or wish to raise a concern or
complaint about the project, then you should consult the Principal Investigator, Professor
Robert Adams on 08 82227413 or by email (Robert.adams@adelaide.edu.au). Contact the
Human Research Ethics Committee’s Secretariat on phone 08 8313 6028 or by email to
hrec@adelaide.edu.au if you wish to speak with an independent person regarding concerns
or a complaint, the University’s policy on research involving human participants, or your
rights as a participant. Any complaint or concern will be treated in confidence and fully
investigated. You will be informed of the outcome.
The questionnaire will take approximately 15-20 minutes to complete, but may take
longer depending on the number of questions that are relevant to you. Please click
‘start survey’ to begin.
34SLEEP SURVEY 2016
A. DEMOGRAPHICS
As some of the next questions relate to certain groups of people only, could you
please tell me…
A.1 How old you are?
(Single Response)
1. Enter age
2. Not stated
3. Don’t know
Sequence Guide: If A.1SLEEP SURVEY 2016
9. 6:30 AM – 6:44 AM
10. 6:45 AM – 6:59 AM
11. 7:00 AM – 7:14 AM
12. 7:15 AM – 7:29 AM
13. 7:30 AM – 7:44 AM
14. 7:45 AM – 7:59 AM
15. 8:00 AM – 8:14 AM
16. 8:15 AM – 8:29 AM
17. 8:30 AM – 8:44 AM
18. 8:45 AM – 8:59 AM
19. 9:00 AM – 9:14 AM
20. 9:15 AM – 9:29 AM
21. 9:30 AM – 9:44 AM
22. 9:45 AM – 9:59 AM
23. 10:00 AM – 10:59 AM
24. 11:00 AM – 11:59 AM
25. 12:00 PM (Noon) – 5:59 PM
26. 6:00 PM – 11:59 PM
27. Refused
28. Don’t know
B.2 At what time do you usually go to bed on nights before workdays or weekdays?
(Single response)
1. 12:00 AM (Midnight)
2. 12:01 AM – 12:59 AM
3. 1:00 AM – 1:59 AM
4. 2:00 AM – 5:00 AM
5. 5:01 AM – 8:59 AM
6. 9:00 AM – 11:59 AM
7. 12:00 PM (Noon) – 6:59 PM
8. 7:00 PM – 7:59 PM
9. 8:00 PM – 8:59 PM
10. 9:00 PM – 9:14 PM
11. 9:15 PM – 9:29 PM
12. 9:30 PM – 9:44 PM
13. 9:45 PM – 9:59 PM
14. 10:00 PM – 10:14 PM
15. 10:15 PM – 10:29 PM
16. 10:30 PM – 10:44 PM
17. 10:45 PM – 10:59 PM
18. 11:00 PM – 11:14 PM
19. 11:15 PM – 11:29 PM
20. 11:30 PM – 11:44 PM
21. 11:45 PM – 11:59 PM
22. Refused
23. Don’t know
36SLEEP SURVEY 2016
B.3 On workdays or weekdays, how many hours, not including naps, do you usually sleep
during one night?
(Do not accept ranges)
1. Enter Hours and/or
2. Enter Minutes
3. Refused
4. Don’t know
B.4 Thinking about your usual non-workday or weekend, please answer the following
questions. At what time do you usually get up on days you do not work or weekends?
(Single response)
1. 12:00 AM (Midnight)
2. 12:01 AM – 4:59 AM
3. 5:00 AM – 5:14 AM
4. 5:15 AM – 5:29 AM
5. 5:30 AM – 5:44 AM
6. 5:45 AM – 5:59 AM
7. 6:00 AM – 6:14 AM
8. 6:15 AM – 6:29 AM
9. 6:30 AM – 6:44 AM
10. 6:45 AM – 6:59 AM
11. 7:00 AM – 7:14 AM
12. 7:15 AM – 7:29 AM
13. 7:30 AM – 7:44 AM
14. 7:45 AM – 7:59 AM
15. 8:00 AM – 8:14 AM
16. 8:15 AM – 8:29 AM
17. 8:30 AM – 8:44 AM
18. 8:45 AM – 8:59 AM
19. 9:00 AM – 9:14 AM
20. 9:15 AM – 9:29 AM
21. 9:30 AM – 9:44 AM
22. 9:45 AM – 9:59 AM
23. 10:00 AM – 10:59 AM
24. 11:00 AM – 11:59 AM
25. 12:00 PM (Noon) – 5:59 PM
26. 6:00 PM – 11:59 PM
27. Refused
28. Don’t know
B.5 At what time do you usually go to bed on nights you do not work the next day or
weekends?
(Single response)
1. 12:00 AM (Midnight)
2. 12:01 AM – 12:59 AM
3. 1:00 AM – 1:59 AM
4. 2:00 AM – 5:00 AM
5. 5:01 AM – 8:59 AM
6. 9:00 AM – 11:59 AM
7. 12:00 PM (Noon) – 6:59 PM
8. 7:00 PM – 7:59 PM
37SLEEP SURVEY 2016
9. 8:00 PM – 8:59 PM
10. 9:00 PM – 9:14 PM
11. 9:15 PM – 9:29 PM
12. 9:30 PM – 9:44 PM
13. 9:45 PM – 9:59 PM
14. 10:00 PM – 10:14 PM
15. 10:15 PM – 10:29 PM
16. 10:30 PM – 10:44 PM
17. 10:45 PM – 10:59 PM
18. 11:00 PM – 11:14 PM
19. 11:15 PM – 11:29 PM
20. 11:30 PM – 11:44 PM
21. 11:45 PM – 11:59 PM
22. Refused 23. Don’t know
B.6 On days you do not work or on weekends, how many hours, not including naps, do you
usually sleep during one night?
(Do not accept ranges)
1. Enter Hours and/or
2. Enter Minutes
3. Refused
4. Don’t know
B.7 How often do you stay up later than you planned or wanted to on weeknights? Would
you say…
(Single response)
1. Every night or almost every night
2. A few nights a week
3. A few nights a month
4. Rarely
5. Never
6. Refused
7. Don’t know
B.8 Thinking about your sleep and sleep habits within the past month, how often have you done the
following in the hour before you went to bed? Would you say that in the past month you…
within an hour of going to bed
Every night A few A few
or almost nights a nights a Don’t
every night week month Rarely Never Refused know
a. Did work relating to your job 05 04 03 02 01 98 99
b. Watched TV 05 04 03 02 01 98 99
c. Listened to the radio or music 05 04 03 02 01 98 99
d. Were on the Internet 05 04 03 02 01 98 99
e. Read 05 04 03 02 01 98 99
38SLEEP SURVEY 2016
f. Had sex 05 04 03 02 01 98 99
g. Exercised 05 04 03 02 01 98 99
h. Spent time with family/friends 05 04 03 02 01 98 99
i. Drank an alcoholic beverage 05 04 03 02 01 98 99
j. Took a hot bath/shower 05 04 03 02 01 98 99
B.9 Do you have any of the following in your bedroom?
Yes No Refused Don’t know
a. Television 01 02 98 99
b. Computer 01 02 98 99
c. Telephone 01 02 98 99
d. Radio/Stereo/DVD 01 02 98 99
B.10 How long, on most nights, does it take you to fall asleep? Would you say …
(Single response)
1. Less than 5 minutes
2. 5 up to 10 minutes
3. 10 up to 15 minutes
4. 15 up to 30 minutes
5. 30 up to 45 minutes
6. 45 minutes up to 1 hour
7. 1 hour or more
8. Depends/Varies
9. Refused
10. Don’t know/Not sure
B.11 Most nights, do you sleep…
(Multiple response)
1. Alone
2. With your significant other
3. With your children
4. With a pet
5. Something else? (Specify)
6. Refused
7. Don’t know
B.12 Most nights, do you prefer to sleep…
(Multiple response)
1. Alone
2. With your significant other
3. With your children
4. With a pet
5. Something else? (Specify)
6. Refused
7. Don’t know
39You can also read