Radiology - Department of Radiological ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Radiology
NEWSLETTER FOR THE DEPARTMENT OF RADIOLOGICAL SCIENCES
SUMMER 2020
i An Innovative Approach to Prostate Cancer Imaging
i Prostate Artery Embolization to Treat Benign Prostatic Hyperplasia (BPH)
WHAT’S i Targeting the Invisible by using Advanced Imaging in Interventional Radiology
INSIDE: i CTi Core Lab Provides Advanced Image Analysis for Cancer Research Trials
i UCI Health Imaging Center Open in Yorba Linda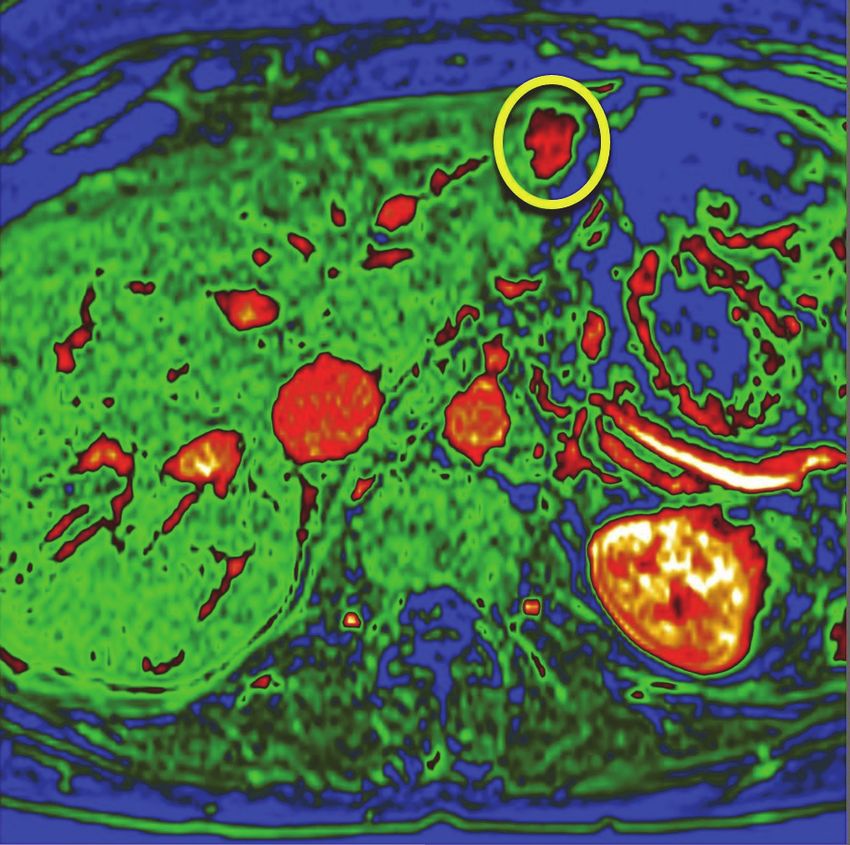
All Hands (and machines) on Deck:
How UCI is using Artificial Intelligence (AI) to help with COVID-19
Daniel Chow, MD
In July 2018, Drs. Peter Chang and Daniel Chow founded the Center for Artificial Intelligence in
Diagnostic Medicine (CAIDM) with the support of UCI’s School of Medicine and its Radiological
Sciences Department. The vision has been to develop, validate, and deploy clinically relevant AI
tools to improve health and well-being. Soon after CAIDM’s inception, Dr. Chang began to validate
and implement tools to speed up critical diagnoses in the emergency department. Shortly after, Drs.
Chang and Chow joined Drs. Suzanne Sandmeyer and Leslie Thompson to form the Precision
Health through Artificial Intelligence through an Academic Initiative at UCI. A vital mission of the
initiative is to focus on the clinical challenge and question and identifying beforehand how exciting
technologies such as AI can provide next-level healthcare.
While the group has focused on new innovations
in stroke, dementia, and cancer, the COVID-19
pandemic presented a new critical care need
that required swift action. To date, COVID-19
has infected over 3.9 million Americans and
claimed over 143,000 death. Recognizing the
crisis, the AI group at UCI quickly pivoted to
develop new data-driven tools to identify
vulnerable patients. This work has been
supported by an award from UCI’s COVID-19
Basic, Translational, and Clinical Research
Funding Opportunity . In under 6-months, the
groups’ work has already had an immediate
impact on our healthcare system, community,
and patients. First, the group quickly worked with
hospital leadership and staff to standardize a
COVID-19 severity lab panel to ensure that
critical labs would be ordered consistently and have
a downstream effect of providing high-quality
Chair’s Message
datasets. Second, the team developed, validated, These are some of the most
and deployed a data-driven decision support tool trying times in healthcare.
built on our institutions’ COVID-19 dataset, which Dealing with a pandemic as we
provides a risk score for the likelihood of requiring move forward with our clinical,
critical care. This tool is among the first to be used in research and teaching goals is
a live clinical setting and has helped UCI health challenging, to say the least.
clinicians triage patients with COVID-19. Also, the However, despite all the
application is continually updated as UCI’s obstacles we face, Team
experience with COVID-19 increases. Third, the Radiology has kept its focus on
group has curated a rich database and has been what is most important to all of
able to provide insightful maps to demonstrate areas us: our patients. The mission of the Department of
of risk in our communities, assisting the institution to Radiological Sciences is to provide exceptional
optimize care. care to our patients, to develop new imaging
technologies and image-guided therapies and to
COVID19 is not over, stressing the importance of (1) train the next generation of leaders in radiology.
wearing a mask when out and (2) distancing We are proud to be the only academic radiology
physically when out socially. Our scientists, department in Orange County and hope you enjoy
clinicians, and staff are focused on helping the reading about some of our current state of the art
community in this pandemic. research and clinical services.
References: Sincerely,
1. https://news.uci.edu/2018/10/12/ai-in-the-er/
Vahid Yaghmai, MD, MS, FSAR
2. https://news.uci.edu/2020/05/21/predicting-a-patients-path/ Professor and Chair of Radiological Sciences
2
An Innovative Approach to
Prostate Cancer Imaging
Tatiana Kain, MD
Recent data suggests that 1 in 9 men are diagnosed with prostate cancer during their lifetime and
one in 45 men will die from the disease. While diagnosis, management and treatment of these
patients have improved over the past decade, there is much more that needs to be done. Up to 25%
of patients with prostate cancer may have detectable lymph node metastases, which are correlated
with a higher risk of recurrence and lower survival. Conventional imaging techniques such as CT
and MRI have low sensitivity and specificity for detection of metastasis and as such are not ideal for
staging of primary or recurrent prostate cancer. Pelvic lymph node dissection is considered the gold
standard in assessing the presence pelvic lymph node metastasis, but its use is limited to the
surgical period.
The prostate-specific membrane antigen (PSMA) The study will assess the impact of rhPSMA-7.3 18F
receptor is over-expressed in the majority of prostate PET on the staging of prostate cancer and on the
cancer and as such an accurate marker for clinical management of patients with biochemical
metabolic processes and identification of metastasis. recurrent prostate cancer post radical prostatectomy
Currently, 68GA PSMA PET tracers are being used or post radiation therapy. rhPSMA originated from
in many centers to image prostate cancer patients, the Technical University of Munich, Germany, and
but there are many disadvantages to this
radionucleotide including the short half-life time and
high production cost. This is of particular importance
in smaller hospitals that lack the patient volume to
justify an onsite 68Ge/68Ga generator.
The demand for better and more cost-effective
tracers led to development of 18F PSMA. As
compare to 68GA, these newly developed tracers
have a longer half time, a higher positron yield,
better signal to noise ratio, and better contrast
resolution resulting in increased sensitivity for lesion
detection. Because of the longer half-life, 18F PSMA
compounds also have the advantage of being used
at sites that cannot produce radiotracers due to
regulatory issues and centers without access to a
radionucleotide generator.
The division of Nuclear Medicine of the Department
of Radiological Sciences is now participating in
prospective multi-national LIGHTHOUSE Phase 3 Image from Eiber et al. 18 F-rhPSMA-7 PET for the Detection of
Biochemical Recurrence of Prostate Cancer After Radical
single arm clinical trials for investigating the safety Prostatectomy. J Nucl Med 2020 May;61(5):696-701.
and efficacy of rhPSMA-7.3 (18F) in men with newly
diagnosed prostate cancer. The principle
investigator of the UCI site is Dr. Edward Uchio has been utilized clinically for the diagnostic imaging
from the Department of Urology. of men with both primary and recurrent prostate
cancer. In the future, rhPSMA compounds will also
rhPSMA-7.3 (18F) is a radiohybrid PSMA-targeted be labeled with radioisotopes such as 177Lu and
receptor ligand which attaches to and is internalized 225
Ac for therapeutic use.
by prostate cancer cells. The trial is designed to
evaluate the sensitivity, specificity and positive The division of NM is happy to take part in this multicenter
predictive value of rhPSMA-7.3 (18F) to detect study that evaluates the safety and efficacy of rhPSMA-
metastatic regional pelvic lymph nodes and compare 7.3 (18F), a highly innovative PET tracer that has
the PET findings to histopathology. In addition, the the potential to significantly enhance the clinical outcome
study is designed to evaluate for metastatic disease of patients with prostate cancer.
in patients with negative conventional imaging.
3
Prostate Artery Embolization to Treat
Benign Prostatic Hyperplasia (BPH)
James Katrivesis, MD
Prostate artery embolization (PAE) is a novel exciting procedure that provides dramatic relief of the
symptoms of benign prostatic hyperplasia (BPH). This treatment is offered by interventional
radiology. Its popularity is increasing with increasing literature supporting its efficacy. Many men who
are not candidates for the traditional urologic surgeries due to medical comorbidities are eligible for
PAE.
A case report from DeMeritt in 2000 described a
symptoms from BPH. He discovered that the
patient’s hematuria and urinary symptoms
dramatically improved after PAE. It was not until
have been performed, demonstrating the
effectiveness of PAE in treating BPH.
frequency, urgency, and nocturia. Medical
Left: Cone Beam CT 3D reconstruction of internal iliac artery.
Workup for BPH usually involves checking PSA and Arrow indicates the prostate artery. Right: Angiogram of the prostate
obtaining biopsy to evaluate for prostate cancer. Use artery.
of prostate MRI has dramatically increased and
helps identify suspicious lesions and gives detailed
measurements of the prostate. A prostate is Cone beam CT with 3D reconstructions is commonly
considered enlarged if it weighs more than 30 used to identify and assist in a successful PAE. The
grams. Many urologic surgeries are limited by the images below demonstrate a prostate artery arising
size of the prostate. For example, TURP is generally from a proximal internal pudendal artery. There is a
not offered when the prostate is > 100 grams. very short shared origin with the vesicular artery.
Without the help of the advanced CBCT imaging,
PAE works for any size prostate. At UCI Department accessing these small tortuous branches would be
of Radiological Sciences we have successfully near impossible. Once the vessel is catheterized, it
treated patients with prostate volumes ranging from is embolized to complete stasis with particles.
37 gm up to 325 grams. The embolization procedure
is performed on an outpatient basis. Vascular A few hours after the procedure the patient is
access can be from either the femoral artery or the discharged home. Most patients will start to see
radial artery. Mapping the pelvic arterial supply and results within a few weeks and many will be able to
identifying the branches can be complicated and stop using BPH medications within a few months.
requires expertise. This is especially true for older We are excited to offer this life changing procedure
patients with atherosclerotic disease. Collateral here at UCI. Please don’t hesitate to contact us with
branches arising for the prostatic arteries can any questions or if you would like to refer a patient.
communicate with branches to the bladder, rectum,
or penile region. These have to be identified and
protected to avoid non-target embolization.
4
Targeting the Invisible
by using Advanced Imaging in Interventional Radiology
Nadine Abi-Jaoudeh, MD
PET scans and contrast enhanced magnetic resonance imaging (MRI) have improved lesion
detection but definitive diagnosis and/or molecular profiling still requires biopsy specimens. These
procedures are performed with ultrasound and computed tomography guidance. The challenge of
targeting a lesion visible on imaging technologies not available in the procedure room is resolved
with the use of navigation technologies. Using fusion, images from pre-procedural modalities can be
registered to intra-procedural ultrasound, CT or even CBCT enabling advancement of a needle or an
ablation probe to the lesion.
Publications by the UCI IR physicians have shown Figure 2: Renal cell
carcinoma (blue mesh) is
that these technologies allow targeting lesions not localized among benign
visible on conventional imaging and/or targeting kidney tumors by fusion of
specific area in a lesion such as guiding a biopsy the contrast enhanced
MRI and intraprocedural
needle into the PET avid area or the non-necrotic cone beam CT. This
portion of a lesion. A prospective randomized trial by enables localization of the
target tumorand planning
Dr Abi-Jaoudeh comparing navigation technologies of the treatment.
to conventional imaging for lesions seen on
ultrasound or CT demonstrated that use of these
technologies reduced the time and the number of
needle repositioning required to reach a target.
Needle repositioning are associated with increased
risk of complications and, therefore, this technology
improves patient safety.
These image fusion techniques can be used to plan
ablation and embolization procedures. The tumor predicated ablation zone can be displayed to ensure
can be segmented on advanced intra-procedural coverage of the tumor with a safety margin. Finally,
imaging, the ablation probe trajectories can be once completed the ablation zone is segmented to
planned in advance and displayed in real time. The confirm complete treatment coverage of the tumor.
The use of image fusion and navigation technologies
resulted in changes in number of ablation probes
and/ or duration of ablation in 1/3 of patients with
technical effectiveness at one month of 96.1%.
During embolization, these technologies have been
shown to improve detection of the number of vessels
supplying a tumor that need to be treated. The post
embolization scans can be overlaid to the pre-
treatment scan to ensure that the entire tumor has
been treated. Complete tumor coverage by
embolization has been shown to increase the rate of
complete response and progression free survival in
patients with hepatocellular carcinoma. Therefore,
use of these advanced imaging technologies is
correlated with improved patient outcome.
Another potential advantage of these technologies is
possibility of reduction in contrast use and radiation.
Indeed, in the prospective biopsy trial, the skin entry
Figure 1: A large hepatocellular carcinoma was segmented (blue radiation dose decreased by 29%. Also, there was a
mesh) as were two smaller tumors (green mesh). The vessels supplying
the tumors are shown in various colors guiding the physician to the treat-
50mL reduction in contrast use compared to
ment area. The conventional image is displayed in grey scale in the conventional imaging.
background.
5
CTi Core Lab Provides Advanced Image
Analysis for Cancer Research Trials Roozbeh Houshyar, MD
Clinical Trials Imaging Core Lab (CTi Core Lab) is a research
service unit within the Department of Radiological Sciences at
University of California, Irvine – School of Medicine with the goal
of providing advanced image analysis for oncologic clinical trials.
Sub-specialty trained board-certified radiology faculty and other
imaging professionals provide a unique set of knowledge and
skills that are not available in many cancer centers. CTi Core Lab
staff includes physicians and scientists who have undergone
systematic training and evaluation in clinical research. CTi Core
Lab’s mission is to provide solutions and expert imaging for
clinical research trials through consistent, standardized, and high
-quality medical image analysis. CTi Core Lab workflow includes
quality control to ensure reproducible, accurate, reliable, and
unbiased measurements. The quality assurance process includes
image quality evaluation, protocol adherence testing, and time-
point verification.
CTi Core Lab experts review and design imaging protocols for
investigator and industry initiated oncologic clinical trials. They also
provide a comprehensive set of quantitative imaging services for
clinical and research purposes. Our experts can 1) tailor imaging
protocols to satisfy trial objectives and maximize effectiveness of image
analysis in therapy assessment, and 2) select appropriate imaging
biomarkers for assessing response to therapy in oncology trials. These
make CTi Core Lab an excellent partner for all clinical oncology trial
needs.
Our core competency includes exceptional quality medical image
analysis. We provide therapy assessment response for various cancers
such as colon, head and neck, liver, lung, lymphoma, pancreatic,
prostate, and sarcoma. We offer quantitative measurements of lesions
according to accepted and published techniques and assessment
criteria standards such as RECIST, mRECIST, iRECIST, PERCIST,
WHO, CHESON, RANO, LUGANO, and PCWG3.
Imaging analysis for any research trial can be provided in two-, three-
and four-dimensions . This includes imaging obtained by state of the art
Computed Tomography (CT), Magnetic Resonance Imaging (MRI), and
Positron Emission Tomography (PET) scanners.
Our research focus is on the development, testing and evaluation of
new imaging biomarkers using advanced imaging techniques,
automated imaging solutions to obtain functional and structural
characteristics of tumor sand applications of artificial intelligence to the
detection and staging of cancers. We collaborate with our translational
imaging scientists to discover the best methods for assessing response
to therapy.
-With contributions from Permjeet Singh, MPH, CCRP, CPH, CHES
Clinical Research Coordinator
6
UCI Health Imaging Center
Open in Yorba Linda Julie Limfueco
UCI Health Imaging Yorba Linda
UCI Health Imaging at Yorba Linda offers a
wide variety of imaging studies with state of the
art equipment. With a newly constructed patient
-focused clinical site and convenient parking,
patients have access to a new location in North
Orange County for their imaging needs. We
offer the following imaging services at this
location:
x 3D Screening and Diagnostic Mammography
x 3T MRI
x Ultrasound
x Diagnostic X-ray Exams
Nestled in the UCI Health Yorba Linda Women’s
3T Siemens MAGNETOM Vida
Breast Center area is our 3D Mammography
unit. This system provides high quality 3D images
for diagnosis, a more comfortable mammography Please contact the following Patient Scheduling
experience for patients and enhanced workflow for Centers for appointments. We look forward to
technologists. We offer same or next day assisting you with your healthcare needs.
appointments for screening mammography. All
breast imaging studies are interpreted by sub- UCI Health Yorba Linda
specialized UCI Health breast radiologists. Patient Contact/Scheduling center
(714) 790-8600
Our 3 T Siemens Magnetom Vida MRI is the first Monday-Friday 8:00 a.m.- 5:00 p.m.
state of the art, wide bore 3T MRI scanner with
BioMatrix technology- which means more comfort UCI Health Imaging
for patients, high quality personalized exams and Patient Contact/Scheduling Center
shorter scan times. Protocols are designed and (714) 456-7237 or (714) 456-RADS
images are interpreted by our sub-specialty trained Monday - Friday 7:00 a.m. - 5:30 p.m.
UCI Health radiologists.
7
Giving
Find us on:
At UCI Health, our team is dedicated to a research-driven approach to
exceptional patient care. When it comes to innovations in clinical and radiology.uci.edu
research programs, our patients are the ones who make it all possible.
If you are considering a gift to support the Department of Radiological
@uciradiology
Sciences or adding UCI Health as a beneficiary of your estate, we look
forward to working with you to accomplish your philanthropic goals.
Please contact us today to learn more about joining us in building a @uci_radiology
brilliant future together.
facebook.com/UCIRadiology
Jared Bigman, Health Advancement
714-456-7066 | jbigman@uci.edu
OUR LOCATIONS
UCI Medical Center UCI Health—Newport Beach
101 The City Drive South 401 Old Newport Blvd., Suite 201
Orange, CA 92868 Newport Beach, CA 92663
Gottschalk Medical Plaza UCI Health—Yorba Linda
1 Medical Plaza Drive 18637 Yorba Linda Blvd.
Irvine, CA 92697 Yorba Linda, CA 92886
Pacific Medical Plaza Administration (714) 456-6921
1640 Newport Blvd., Suite 200 Scheduling (714) 456-7237
Costa Mesa, CA 92627 (714) 456-RADS
The Administration office is currently working remotely. Please leave a message
and a staff member will return your call at the earliest convenience. Thank you.
8

You can also read

















































