Increasing Mastectomy Rates Among all Age Groups for Early Stage Breast Cancer: A 10-Year Study of Surgical Choice
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ORIGINAL ARTICLE Increasing Mastectomy Rates Among all Age Groups for Early Stage Breast Cancer: A 10-Year Study of Surgical Choice Anthony E. Dragun, MD,* Bin Huang, Dr PH, MS, ,à Thomas C. Tucker, PhD, MPH,à and William J. Spanos, MD* *Department of Radiation Oncology, James Graham Brown Cancer Center, University of Louisville School of Medicine, Louisville, Kentucky; Department of Biostatistics, College of Public Health, University of Kentucky, Lexington, Kentucky; and àKentucky Cancer Registry, Markey Cancer Center, University of Kentucky, Lexington, Kentucky n Abstract: First-line surgical options for early stage breast cancer and ductal carcinoma in situ include breast conserv- ing surgery or mastectomy. We analyzed factors that influence the receipt of mastectomy and resultant trends over time. Registry analysis was carried out for 21,869 women who underwent up-front surgical treatment for stage 0, I or II breast cancer between 1998 and 2007 using data from the Kentucky Cancer Registry. We examined the trend of treatment over time and assessed the probability of receiving mastectomy using multivariate logistic regression. Overall, 54.5% of women received breast conservation and 45.5% received mastectomy over a 10-year period (annual BCS rate range: 46.9–61.2%). The overall mastectomy rate substantially decreased from 53.1% in 1998 to 38.8% in 2005 (p < 0.0001), but then increased to 45% in 2007 (p < 0.001). Between 2005 and 2007, the increase in mastectomies in the age groups of
Mastectomy Rates Rising for all Ages • 319
breast cancer screening and public awareness cam- was 20 years old or older; the cancer was the first pri-
paigns have resulted in earlier detection of more mary cancer diagnosed; only AJCC stage 0 (ductal
favorable disease, a paradoxical recent trend toward carcinoma in situ), Stage I and II cases included. Cases
more extensive surgical management has been abstracted from autopsy or death certificate only were
observed (5,7,17,20–23). There is currently a debate excluded.
over whether the reports of increasing mastectomy use The KCR is a population-based registry, and has
are isolated only to individual treatment centers been awarded the highest level of certification by the
(7,17,21,23,24), as larger, population-based studies North American Association of Central Cancer
have failed to show the same trend (5). Registries for an objective evaluation of completeness,
During the last few decades, major cancer centers accuracy, and timeliness every year since 1997. The
in large cities have paved way for significant growth KCR is also part of the Surveillance, Epidemiology,
and spread of multidisciplinary breast cancer care and End Results (SEER) program, which is considered
with access to specialized breast surgeons coupled one of the most accurate and complete population-
with integration of adjuvant local and systemic thera- based cancer registries in the world. The KCR also
pies. In the US, approximately 80% of the population links its database annually with the National Death
lives in or near a major metropolitan center and thus Index (NDI) to capture the most accurate survival
the aforementioned studies are heavily influenced by information.
the inclusion of significant numbers of urban patients For purposes of this analysis, the treatment is cate-
(25). In fact, subset analyses of nearly all national gorized into two groups: Mastectomy or BCS. Mastec-
database studies on this subject indicate that the low- tomy is defined as modified radical mastectomy, total
est relative rates of BCS exist in more sparsely popu- mastectomy or simple mastectomy. BCS is defined as
lated regions, especially the South and ⁄ or Southeast any surgery less than the aforementioned, including
(6,8,10,12,14,16,18,19,26–28). partial mastectomy (with or without nipple resection),
The Commonwealth of Kentucky does not encom- segmental mastectomy, lumpectomy, tylectomy, quad-
pass a city listed among the top 25 incorporated enti- rantectomy or re-excision of the biopsy site for gross
ties (according to the United States Census Bureau) nor or microscopic residual disease.
a top 40 metropolitan statistical area (as defined by the Race, age at diagnosis, urban ⁄ rural status and
United States Office of Management and Budget). In Appalachian status are primary demographic interests
addition, Kentucky does not contain a National Cancer of the study. Urban ⁄ Rural status was based on the
Institute (NCI) designated cancer center. The purpose 2003 Urban-Rural Continuum codes with 1–3 defined
of this study was to quantify the rate of BCS for pre- as urban and 4–9 as rural. The county-level Appala-
invasive and early stage breast cancer in this under- chian status was based on definitions by the Appala-
served southern state, and to identify determinants of chia Regional Commission. Other demographical and
mastectomy along with trends over time. clinical variables included in the study were year at
diagnosis, smoking history, insurance status, survival
status at the end of the study, primary cancer
METHODS sequence number, laterality, stage, nodes examined,
This retrospective population-based registry study ER ⁄ PR status, tumor grade, histology, and tumor size.
was approved by the institutional review board at the The descriptive analysis for demographics and clini-
University of Louisville School of Medicine. The study cal factors was performed. We used chi-squared tests
concept, design, and completion represents a collabo- to examine associations between treatment and vari-
rative effort between investigators at the University of ables described above. Multivariate logistic regressions
Louisville’s James Graham Brown Cancer Center were fitted to evaluate the association between mastec-
(Louisville, KY) and the Kentucky Cancer Registry at tomy utilization and age at diagnosis ⁄ race ⁄ residence
the University of Kentucky’s Markey Cancer Center location while controlling for other covariates. The
(Lexington, KY). Data for female-only breast cancer final model included only covariates with a signifi-
cases diagnosed between 1998 and 2007 were cance level of 0.05 or less. Model goodness of fit, mul-
obtained from the Kentucky Cancer Registry (KCR). ticollinearity, and interactions were also examined. All
The study included 21,869 women who met the analyses were done using SAS Statistical software
following inclusion criteria: age at cancer diagnosis version 9.1 (Cary, NC, USA). All statistical tests were320 • dragun et al.
two sided with a p-value £ 0.05 used to identify statis- Table 1. Demographics, Disease Characteristics,
tical significance. and Surgical Details for all Cases Included in this
Study (N = 21,869)
Variable N %
RESULTS
Age at diagnosis
The study cohort consisted of 21,869 patients whoMastectomy Rates Rising for all Ages • 321
Table 1. (Continued ) (a) Age < 50 years
70.0%
Variable N %
60.0%
Axillary dissection 10,894 49.8
50.0%
Not specified 341 1.6
Primary surgical choice
40.0%
BCS 11,919 54.5
Mastectomy 9950 45.5
30.0%
20.0%
Surgical Choice by Year
10.0%
2500
0.0%
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
2000
BCS Mastectomy
1500
(b) Age 50-69 years
# Casess
70.0%
1000
60.0%
50.0%
500
40.0%
0 30.0%
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
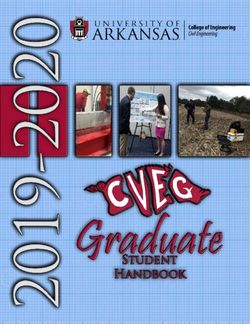
Mastectomy 1114 1165 1069 1143 1064 854 841 814 892 999
BCS 984 1115 1119 1188 1214 1249 1245 1286 1295 1219 20.0%
10.0%
Figure 1. Annual relative rates of primary surgical choice (BCS
versus mastectomy) for all cases of stage 0, I, and II breast cancer 0.0%
from 1998–2007 in the Commonwealth of Kentucky. 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
BCS Mastectomy
specifics, patients were more likely to receive a mas-
(c) Age ≥ 70 years
tectomy if they had stage II disease (p < 0.0001), 70.0%
poorly differentiated tumors(p < 0.0001), lobular can-
60.0%
cers(p < 0.0001), and hormone receptor negative dis-
ease (p < 0.0001). Larger tumor size and more 50.0%
extensive axillary surgery were associated with higher 40.0%
likelihood of receiving a mastectomy (p < 0.0001).
30.0%
Table 3 shows the results of multivariate analysis
including the entire list of variables included in 20.0%
Tables 1 and 2. The most significant independent 10.0%
demographic factors associated with receipt of mastec-
0 0%
0.0%
tomy were, lack of private insurance (p < 0.0001), fol- 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
lowed by rural county of residence (p = 0.0187), and BCS Mastectomy
advanced age (p = 0.0332). With regard to disease
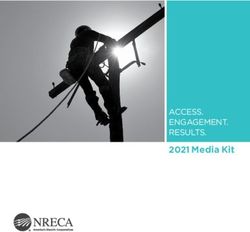
Figure 2. (a–c): Surgical choice by age over the decade of the
specifics, mastectomy was more likely to be adminis- study period for women (a)322 • dragun et al.
Table 2. Univariate Analysis for the Association Table 2. (Continued )
of Demographic and Disease Factors with Pri-
mary Surgical Choice for all Cases Included in Primary surgical choice
this Study (N = 21,869) BCS Mastectomy
Primary surgical choice Variables N % N % p-value
BCS Mastectomy 3.1–4.0 388 29.2 939 70.8
>4.0 243 24.0 768 76.0
Variables N % N % p-value Not specified 1225 59.0 852 41.0
Lymph node surgery
Age at diagnosis None 3399 75.7 1093 24.3Mastectomy Rates Rising for all Ages • 323
cal strategies have had a long evolution over more In a retrospective review of a prospective collective
than 50 years, it was the publication of the 1991 NIH database between 1994 and 2007 at the Moffitt
consensus conference on the treatment of patients Cancer Center, mastectomy rates were shown to
with early stage breast cancer that ushered in this so- decrease between 1994 and 2004 and then signifi-
called ‘‘post-mastectomy’’ era (4). Indeed, prior to the cantly increase from 2004 to 2007 (from 44% to
NIH consensus, only about 35% of women with Stage 60%) (23). Mastectomy was correlated with younger
I and 19% of women with stage II breast cancer age, increasing tumor size, and presence of lympho-
nationwide underwent BCS, however, by 1995, these vascular invasion, but the major determining factor
national numbers increased to approximately 60% was the year of diagnosis with the highest odds ratio
and 40%, respectively (6). of mastectomy as seen between 2004 and 2007 (23).
Despite this sea change, broad discrepancies in the A regional study from the California Cancer Registry
application of BCS versus mastectomy have been showed the recently observed shift away from BCS
observed based on patient demographic and disease- back to mastectomy beginning around the year 2000,
specific characteristics. The mastectomy rate has been and most notable for younger, non-Hispanic White
correlated with factors such as age, lymph node status, women of high socio-economic status (22).
poverty level, educational level, and even widowed Explanations for these recent trends range from
status (7,18). But perhaps most often, mastectomies changing patient attitudes, better surgical techniques,
have been unevenly distributed geographically, with and access to more treatment choices as well as
the highest in the south region compared to regions in increasing perception about future risks of in breast
the northeast and west coast (6,18). Furthermore, tumor recurrence and contralateral tumor recurrences
rural residency designation, even within a region with (21). Another explanation for rising mastectomy rates
high rates of BCS, also predicts for receipt of mastec- has been the increased use of preoperative MRI.
tomy (8,15). A SEER study of surgical choice in A study of over 5,000 patients from the Mayo Clinic
women from 1992–1993 showed that rural residency identified breast MRI as a major independent predic-
was an independent factor affecting the receipt of tive factor of mastectomy (odds ratio = 1.7) for
mastectomy with an odds ratio of 1.58, with an over- patients who underwent surgery between 1997 and
all mastectomy rate of rural patients in the study of 2006. However, mastectomy rates also increased in
59.9 versus 44.9 for non rural patients (15). In a study the same series from 2004 to 2006 among patients
of the New Hampshire Cancer Registry from 1998 to who did not undergo an MRI and thus surgical year
2000, women were more likely to have a mastectomy was an independent predictor for mastectomy (24).
if they lived greater than or equal to 20 miles from a The interest generated by the corroborating studies
radiation therapy facility or if their diagnosis was from multiple institutions recently led to a large popu-
made in the wintertime when daily travel for radiation lation-based (SEER) study conducted by Haberman
therapy after BCS would entail more inconvenience or et al. (5). In this nationwide analysis of over 200,000
hazard (8). patients who underwent surgery between 2000 and
Additional factors play into surgical choice, for 2006 the overall mastectomy rate decreased from
even when BCS is desired by the patient, it may not approximately 41% to 37% (5). However, the same
be advisable (16). A large study performed at the study noted that although the rate of unilateral mas-
University of Michigan specifically quantified the fact tectomy had decreased the rate of contralateral pro-
that although most women with early stage breast phylactic mastectomy had substantially increased (5).
cancer may be considered good candidates for BCS in Although it may appear at first glance that the conclu-
general, approximately one third are ultimately con- sions of this SEER study directly contradict those of
sidered poor candidates secondary to issues related to the aforementioned single institutions, in fact both
tumor size to breast size ratio or other reasons such as observations may be valid.
diffuse microcalcifications on mammography (17). Our current study is in agreement with the national
Even so, the reason most often cited for the choice SEER registry, showing that the absolute mastectomy
of mastectomy in breast conservation candidates is rate is lower than it was compared to a decade ago by
patient choice, and despite better screening, earlier approximately the same magnitude (53.1% in 1998
detection, and patient selection, women seem to be versus 45.0% in 2007). However, when looking
choosing mastectomy in larger numbers (17,21–24). specifically at the last 3–4 years of the analysis—the324 • dragun et al.
same time period of the above-mentioned single insti- must be targeted to these underserved populations to
tution series—the trend in the use of mastectomy is improve treatment choice and access for vulnerable
unmistakably upward. Moreover, our data suggest patient populations. Additional study is warranted to
that this trend is present throughout all age groups quantify additional factors that underlie this surgical
with absolute increase in mastectomy use of approxi- trend in non-underserved populations.
mately 5–8%. Surprisingly, this trend is observed even
among the elderly, in whom radical surgery is poten-
tially more risky and partial mastectomy alone with- SUPPORT ⁄ CONFLICTS OF INTEREST
out the addition of radiotherapy has become a more There was no financial support in the conception,
widely accepted option (29). Our data are confirma- design or completion of this study. There are no con-
tory of other studies, reinforcing that the dispropor- flicts of interest to disclose by any of the authors.
tionate use of mastectomy remains a problem for the
uninsured or underinsured, rural and elderly patients,
all of whom may lack sufficient access to multidisci- REFERENCES
plinary breast care. 1. Fisher B, Jeong JH, Anderson S, Bryant J, Fisher ER,
The strength of our study lies in the ability of the Wolmark N. Twenty-five-year follow-up of a randomized trial com-
paring radical mastectomy, total mastectomy, and total mastectomy
Kentucky Cancer Registry to represent a large cross followed by irradiation. N Engl J Med 2002;347:567–75.
section of academic and community centers within an 2. van Dongen JA, Voogd AC, Fentiman IS, et al. Long-term
underserved Southern US state, where the overall mas- results of a randomized trial comparing breast-conserving therapy
with mastectomy: european Organization for Research and
tectomy rates have always been higher than the
Treatment of Cancer 10801 trial. J Natl Cancer Inst 2000;92:
national average (5,6,15,18). The registry is highly 1143–50.
validated and allows the collection of a large sample 3. Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year fol-
size for population-based analysis. However, all regis- low-up of a randomized study comparing breast-conserving surgery
with radical mastectomy for early breast cancer. N Engl J Med
try studies have limitations related to the lack of 2002;347:1227–32.
breadth and depth of information contained within 4. NIH consensus conference. Treatment of early-stage breast
the full medical record, and ours is no exception. cancer. JAMA 1991;265:391–5.
5. Habermann EB, Abbott A, Parsons HM, Virnig BA, Al-Refaie
Information that is absent from the SEER registry WB, Tuttle TM. Are mastectomy rates really increasing in the
database includes the presence, type and severity of United States? J Clin Oncol 2010;28:3437–41.
medical comorbidities, subspecialization of the 6. Lazovich D, Solomon CC, Thomas DB, Moe RE, White E.
Breast conservation therapy in the United States following the 1990
operating surgeon, and preoperative breast MRI, all
National Institutes of Health Consensus Development Conference
of which have been shown to impact mastectomy on the treatment of patients with early stage invasive breast carci-
rates and may confound this data (7,8,23,24,27,30). noma. Cancer 1999;86:628–37.
Nonetheless, our results suggest that mastectomy rates 7. Al-Refaie W, Kuerer HM, Khuwaja A, et al. Determinants of
mastectomy in breast conservation therapy candidates. Am J Surg
in the Commonwealth of Kentucky have been increas- 2005;190:602–5.
ing across all age groups since 2004, and that the 8. Celaya MO, Rees JR, Gibson JJ, Riddle BL, Greenberg ER.
aforementioned trend first identified at large academic Travel distance and season of diagnosis affect treatment choices
for women with early-stage breast cancer in a predominantly
centers perhaps served as a bellwether for that which rural population (United States). Cancer Causes Control 2006;
is now revealing itself in larger population-based 17:851–6.
databases. 9. Craft PS, Buckingham JM, Dahlstrom JE, et al. Variation in
the management of early breast cancer in rural and metropolitan
Our study concludes that the use of mastectomy for
centres: implications for the organisation of rural cancer services.
primary surgical treatment of early stage breast cancer Breast 2010;19:396–401.
is increasing for all age groups. Radical surgery is dis- 10. Freedman RA, He Y, Winer EP, Keating NL. Trends in
proportionately used in underinsured, rural, and racial and age disparities in definitive local therapy of early-stage
breast cancer. J Clin Oncol 2009;27:713–9.
elderly populations, and there has been little improve- 11. Haggstrom DA, Quale C, Smith-Bindman R. Differences in
ment in this measure over the last decade. Although the quality of breast cancer care among vulnerable populations.
our study population reflects an insured, white sample, Cancer 2005;104:2347–58.
12. Hampton T. Studies address racial and geographic dispari-
the cohort is unique in that it contains a high percent- ties in breast cancer treatment. JAMA 2008;300:1641.
age of patients from underserved rural (40%) and ⁄ or 13. Hershman DL, Buono D, Jacobson JS, et al. Surgeon charac-
Appalachian (25%) geographies. Incentive programs teristics and use of breast conservation surgery in women with early
stage breast cancer. Ann Surg 2009;249:828–33.
focused on multidisciplinary care as a quality endpointMastectomy Rates Rising for all Ages • 325
14. Hokanson P, Seshadri R, Miller KD. Underutilization of 23. McGuire KP, Santillan AA, Kaur P, et al. Are mastectomies
breast-conserving therapy in a predominantly rural population: need on the rise? A 13-year trend analysis of the selection of mastectomy
for improved surgeon and public education. Clin Breast Cancer versus breast conservation therapy in 5865 patients. Ann Surg
2000;1:72–6. Oncol 2009;16:2682–90.
15. Jacobs LK, Kelley KA, Rosson GD, Detrani ME, Chang DC. 24. Katipamula R, Degnim AC, Hoskin T, et al. Trends in mas-
Disparities in urban and rural mastectomy populations: the effects tectomy rates at the Mayo Clinic Rochester: effect of surgical year
of patient- and county-level factors on likelihood of receipt of mas- and preoperative magnetic resonance imaging. J Clin Oncol
tectomy. Ann Surg Oncol 2008;15:2644–52. 2009;27:4082–8.
16. Katz SJ, Lantz PM, Janz NK, et al. Patterns and correlates 25. Blumenthal SJ, Kagen J. MSJAMA. The effects of socioeco-
of local therapy for women with ductal carcinoma-in-situ. J Clin nomic status on health in rural and urban America. JAMA
Oncol 2005;23:3001–7. 2002;287:109.
17. Lee MC, Rogers K, Griffith K, et al. Determinants of breast 26. Hatzell TA, Ricketts TC, Tropman SE, Paskett ED, Cooper
conservation rates: reasons for mastectomy at a comprehensive can- MR. Rural physicians’ understanding of the state-of-the-art in
cer center. Breast J 2009;15:34–40. breast, colon and rectum cancer treatment. Cancer Causes Control
18. Smith GL, Xu Y, Shih YC, et al. Breast-conserving surgery in 1999;10:261–7.
older patients with invasive breast cancer: current patterns of treat- 27. Meden T, St John-Larkin C, Hermes D, Sommerschield S.
ment across the United States. J Am Coll Surg 2009;209:425–33.e2. MSJAMA. Relationship between travel distance and utilization of
19. Tropman SE, Ricketts TC, Paskett E, Hatzell TA, Cooper breast cancer treatment in rural northern Michigan. JAMA
MR, Aldrich T. Rural breast cancer treatment: evidence from the 2002;287:111.
Reaching Communities for Cancer Care (REACH) project. Breast 28. Schroen AT, Brenin DR, Kelly MD, Knaus WA, Slingluff CL
Cancer Res Treat 1999;56:59–66. Jr. Impact of patient distance to radiation therapy on mastectomy
20. Jemal A, Ward E, Thun MJ. Recent trends in breast cancer use in early-stage breast cancer patients. J Clin Oncol
incidence rates by age and tumor characteristics among U.S. women. 2005;23:7074–80.
Breast Cancer Res 2007;9:R28. 29. Hughes KS, Schnaper LA, Berry D, et al. Lumpectomy plus
21. Balch CM, Jacobs LK. Mastectomies on the rise for breast tamoxifen with or without irradiation in women 70 years of age or
cancer: ‘‘the tide is changing’’. Ann Surg Oncol 2009;16:2669–72. older with early breast cancer. N Engl J Med 2004;351:971–7.
22. Gomez SL, Lichtensztajn D, Kurian AW, et al. Increasing mas- 30. Tuttle TM. Magnetic resonance imaging and contralateral
tectomy rates for early-stage breast cancer? Population-based trends prophylactic mastectomy: the ‘‘no mas’’ effect? Ann Surg Oncol
from California. J Clin Oncol 2010;28:e155–7; author reply e8. 2009;16:1461–2.You can also read