Questions & Answers Le nuove lineeguida ESC 2019 sull'embolia polmonare
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Le nuove lineeguida ESC 2019 sull’embolia polmonare
Questions & Answers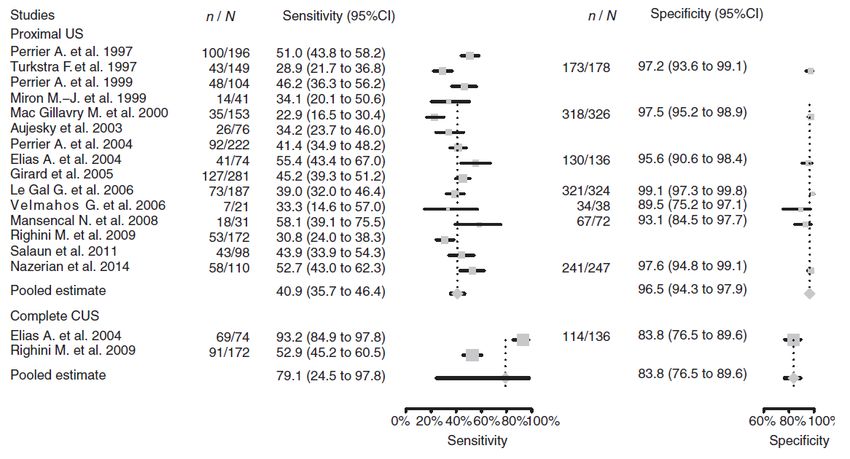
Caso clinico 1 • Paziente di 82 anni con insufficienza respiratoria cronica per fibrosi polmonare in ossigenoterapia domiciliare con CN 4 l/min. Nota PAPs 50 mmHg. Non in terapia anticoagulante. Allergia a mdc. • Giunge per dispnea improvvisa ed incremento del fabbisogno di ossigeno (SatO2 90% con VM 50%). PA 120/80 mmHg, FC 95 bpm. Agli esami ematici lieve leucocitosi neutrofila, non febbre, PCR 2.5. Eco-color-Doppler venoso negativo, PAPs invariata.
Caso clinico 1 Questions: • Quale percorso diagnostico? Rx torace e scintigrafia polmonare? • D-dimero?
Caso clinico 1
Answers
Quale percorso diagnostico?
Patient with suspected Pulmonary
Embolism
With haemodynamic instability Without haemodynamic instability
In suspected high-risk PE, as It is recommended that the
indicated by the presence of diagnostic strategy be based on
haemodynamic instability, clinical probability, assessed either I A
bedside echocardiography or by clinical judgement or by a
I C
emergency CTPA (depending on validated prediction rule.
availability and clinical
circumstances) are The use of validated criteria for
I B
recommended for diagnosis. diagnosing PE is recommended.
©ESC
It is recommended that i.v. Initiation of anticoagulation is
anticoagulation with UFH, recommended without delay in
including a weight-adjusted patients with high or intermediate I C
I C
bolus injection, be initiated clinical probability of PE while
without delay in patients with diagnostic work-up is in progress.
suspected high-risk PE.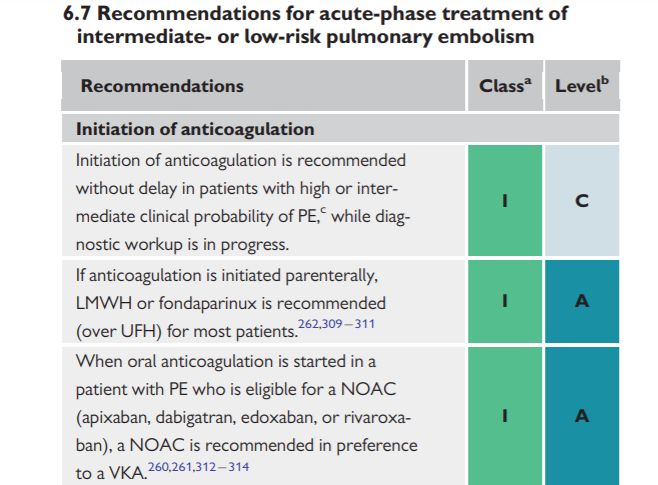
Assessment of clinical (pre-test) probability
Pre-test PE assessment
Clinical judgement By using prediction rules
Revised Geneva Score Wells Score
The combination of:
Variable Score Variable Score
- Symptoms (dyspnoea, chest pain,
syncope or haemoptysis) Age>65 1 Clinical signs/symptoms of 3
- Clinical findings (hypoxaemia, Previous DVT or PE 3 DVT
abnormal chest-X-ray, Recent surgery or fracture 2 PE is the most likely 3
electrocardiografic changes) diagnosis
- Predisposing factors for VTE Active cancer 2
HR >100 bpm 1.5
Unilateral leg pain 3
Immobilitazion/surgery 1.5
Haemoptysis 2
Prior DVT/PE 1.5
HR 75-94 bpm 3
Lacks standardization Haemoptysis 1
HR ≥ 95 bpm 5
Pain or unilateral edema 4 Active cancer 1
- Low or intermediate clinical probability
- High clinical probability
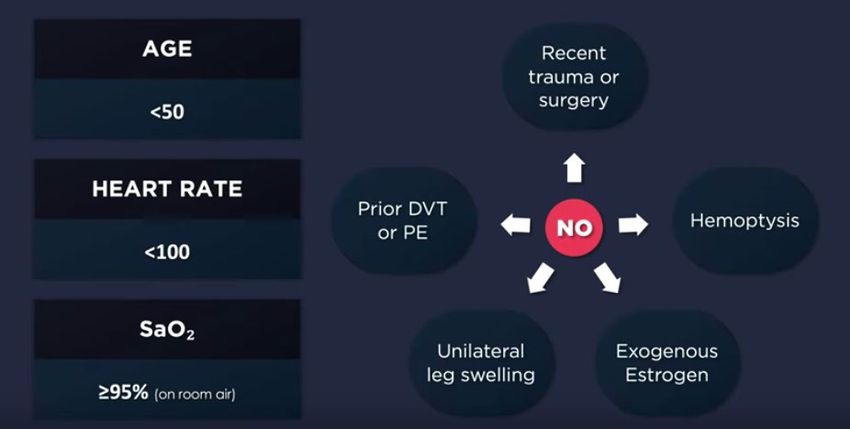
Pulmonary Embolism Rule-out criteria
Every patients with dyspnoea or chest pain admitted to the Emergency Department
Aim: to identify patients who will NOT benefit from further testing
In patients with a low pretest probability of pulmonary embolism, further
evaluation is not recommended when all criteria are met
Penaloza A, et al. Lancet Haematol 2017
Freund Y, et al. JAMA 2018;319:559566
Caso clinico 1
Items Clinical decision
rule points
Original Simplified
version version
Previous PE or DVT 3 1
Heart rate
Clinical probability Original Simplified
75–94 b.p.m. 3 1 version version
≥95 b.p.m. 5 2 Three-level score
Surgery or fracture Low 0–3 0–1
within the past month 2 1
Intermediate 4–10 2–4
Haemoptysis 2 1 High ≥11 ≥5
Two-level score
Active cancer 2 1
PE unlikely 0–5 0–2
Unilateral lower limb 3 1
pain PE likely ≥6 ≥3
Pain on lower limb
deep venous palpation 4 1
and unilateral oedema
Age >65 years 1 1
Patient with suspected Pulmonary Embolism AND
without haemodynamic instability
Low or intermediate clinical probability
Plasma D-dimer measurement,
preferably using a highly sensitive
assay, is recommended in
outpatients/emergency department
I A
patients with low or intermediate
clinical probability, or PE-unlikely, to
reduce the need for unnecessary
imaging and irradiation.
YEARS model
As an alternative to the fixed D-dimer
cut-off, a negative D-dimer test using Signs of DVT
an age-adjusted cut-off (age x 10 μg/L, Haemoptysis
in patients >50 years) should be IIa B
Alternative diagnosis is
considered for excluding PE in patients
less likely than PE
with low or intermediate clinical
probability, or PE-unlikely.
As an alternative to the fixed or age- PE is excluded in patients:
adjusted D-dimer cut-off, D-dimer -without clinical items and D-dimer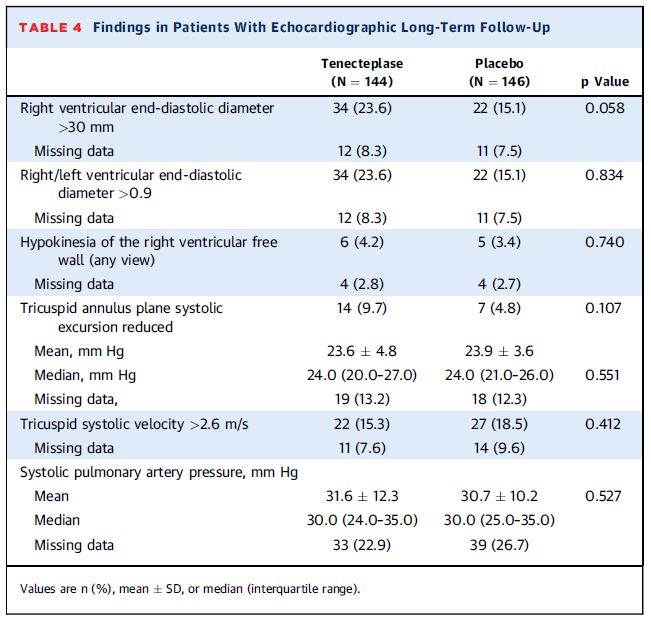
Age-Adjusted D-Dimer Cutoff Levels to
Rule Out PE
The ADJUST-PE Study
3346 patients with suspected PE included
Sequential Diagnostic Strategy
simplified, revised Geneva score or the 2-level Wells score for PE
highly sensitive D-dimer measurement
computed tomography pulmonary angiography (CTPA)
Patients with a D-dimer value between the conventional cut-off of 500 μg/L
and their age-adjusted cut-off (agex10, if age>50) did not undergo CTPA
and were left untreated
Marc Righini, JAMA 2014Age-Adjusted D-Dimer Cutoff Levels to
Rule Out PE
The ADJUST-PE Study
The 3-month failure rate in patients with a D-dimer level higher than 500μg/L but
below the age-adjusted cut-off was 1 of 331 patients (0.3%, 95%CI,0.1%-1.7%)
Marc Righini, JAMA 2014Patient with suspected Pulmonary Embolism AND
without haemodynamic instability
High clinical probability
D-dimer measurement is not recommended in
patients with high clinical probability, as a normal
III A
result does not safely exclude PE, even when using
a highly sensitive assay.Caso clinico 1
Paziente con probabilità clinica intermedia di Embolia
polmonare
D-Dimero= 800 μg/L
Cut-off age adjusted= 820 μg/L (82X10=820)
Non ulteriori test di imaging sono stati effettuati e veniva
esclusa la diagnosi di Embolia polmonareRecommendations Class Level
CTPA
It is recommended to reject the diagnosis of PE (without further testing) if
CTPA is normal in a patient with low or intermediate clinical probability, or I A
PE-unlikely.
It is recommended to accept the diagnosis of PE (without further testing)
if CTPA shows a segmental or more proximal filling defect in a patient with I B
intermediate or high clinical probability.
CT venography is not recommended as an adjunct to CTPA. III B
V/Q scintigraphy
It is recommended to reject the diagnosis of PE (without further testing) if
I A
the perfusion lung scan is normal.
Lower-limb compression ultrasonography (CUS)
It is recommended to accept the diagnosis of VTE (and PE) if a CUS shows a
I A
proximal DVT in a patient with clinical suspicion of PE.
Magnetic resonance angiography (MRA)
MRA is not recommended for ruling out PE. III AMain new recommendations 2019
Diagnosis
D-dimer test using an age-adjusted cut-off, or adapted to clinical
probability, should be considered as an alternative to the fixed IIa
cut-off level.
If a positive proximal CUS is used to confirm PE, risk assessment
IIa
should be considered to guide management.
V/Q SPECT may be considered for PE diagnosis. IIbCaso clinico 2 • Paziente di 74 anni, in anamnesi ipertensione arteriosa in terapia con ramipril. Recente immobilizzazione per lombosciatalgia. • Giunge in Ambulatorio per edema arto inferiore sinistro. All’eco-color-Doppler venoso arti inferiori presenta TVP femorale destra. La sera precedente presentava episodio di dispnea poi regredito. PA 140/85 mmHg, FC 88 bpm, SatO2 96% in aria ambiente.
Caso clinico 2 Questions: • Torna a casa con terapia anticoagulante? • Fareste TC torace? • Altra stratificazione del rischio?
Caso clinico 2
Answers4.10 Compression ultrasonography Lower-limb CUS has largely replaced venography for diagnosing DVT. CUS has a sensitivity >90% and a specificity of 95% for proximal symptomatic DVT. CUS shows a DVT in 30-50% of patients with PE, and finding a proximal DVT in patients suspected of having PE is considered sufficient to warrant anticoagulant treatment without further testing.
2016
15 prospective studies in which
CUS was performed in consecutive
patients with suspected PE: 6991
patients, 30% had PE
A high SP (96%) to PE for
proximal CUS was found. SE 41%.
SE of whole-leg CUS was 79% and
SP 84%.
Proximal CUS cannot be used to
rule out PE. Its high SP allows
confirming PE, which may be
useful in patients with
contraindications to CTPA.Main new recommendations 2019 (1) Diagnosis D-dimer test using an age-adjusted cut-off, or adapted to clinical probability, should be considered as an alternative to the fixed cut-off level. IIa If a positive proximal CUS is used to confirm PE, risk assessment should be considered to guide management. IIa V/Q SPECT may be considered for PE diagnosis. IIb
Indicators of risk
Clinical
Elevated
Early mortality risk Haemo- parameters of PE RV
cardiac
dynamic severity/ dysfunction on
troponin
instability comorbidity: PESI TTE or CTPA
levels
III–V or sPESI ≥1
High + (+) + (+)
Interme- Intermediate–high - + + +
diate Intermediate–low - + One (or none) positive
Assessment
optional; if
Low - - -
assessed,
©ESC
negative
CTPA = computed tomography pulmonary angiography; PESI = Pulmonary Embolism Severity Index; TTE = transthoracic echocardiography.A meta-analysis on 3295 ‘low risk’ patients with acute PE: the presence of RV dysfunction on admission was associated with early mortality (OR 4.19, 95% CI 1.39–12.58)
2019 A central role for RVD RV function in the BNP is no more risk-adjusted RVD mentioned management strategy chart is clearly stated
Home treatment in PE patients: the HOT PE Study
In patients with acute low-risk PE (including absence of RV dysfunction and intracardiac thrombi),
early discharge and home treatment with rivaroxaban was feasible, effective, and safe
Konstantinides, ACC Barco
Congress
Eur2019
Heart J 2019Caso clinico 3 • Paziente di 68 anni giunge a seguito di episodio sincopale e successiva dispnea. • In PS PA: 100/70 mmHg, FC 100 bpm, SatO2 94% con VM 60%. Presenta RVD, PAPs 55 mmHg e troponina elevata. Effettua TC torace con mdc che mostra embolia polmonare dei rami principali.
Caso clinico 3 Questions: • Trombolisi ev? • CDT? • UFH vs LMWH?
Caso clinico 3
Answers7.2.2 Treatment of intermediate-risk pulmonary embolism • Routine full-dose systemic thrombolysis is not recommended, as the risk of potentially life-threatening bleeding complications appears too high for the expected benefits from this treatment. • Rescue thrombolytic therapy or, alternatively, surgical embolectomy or percutaneous catheter-directed treatment should be reserved for patients who develop signs of haemodynamic instability. • In the PEITHO trial, the mean time between randomization and death or haemodynamic decompensation was 1.79 ± 1.60 days in the placebo (heparin- only) arm. Therefore, it appears reasonable to leave patients with intermediate- high-risk PE on LMWH anticoagulation over the first 2 – 3 days and ensure that they remain stable before switching to oral anticoagulation.
Thrombolysis in PE patients: meta-analysis
15 RCTs (2057 pts) comparing systemic thrombolysis + AC vs AC alone
Marti EHJ 2015PEITHO: long-term outcome
709 patients participated in the long-term follow-up (median 37.8 months)
Overall mortality rates 20.3% vs 18.0%
CTEPH was confirmed in 4 (2.1%) vs 6 (3.2%), p =
Konstantinides JACC 2017Changes in recommendations 2014-2019
Recommendations 2014 2019
Rescue thrombolytic therapy is recommended for patients
IIa I
who deteriorate haemodynamically.
Surgical embolectomy or catheter-directed treatment
should be considered as alternatives to rescue
IIb IIa
thrombolytic therapy for patients who deteriorate
haemodynamically.The OPTALYSE PE trial
SBP >90 mmHg)
101 patients R RV/LV diameter ratio ≥0.9 on CTA
proximal PE located in at least 1 main or proximal lobar pulmonary artery
Treatment with USCDT using a shorter delivery duration and lower-dose tPA was associated
with improved RV function and reduced clot burden compared with baseline.
Arm 1 Arm 2 Arm 3 Arm 4
CDT regimen 4 mg per lung 4 mg per lung 6 mg per lung 12 mg per lung
over 2 h over 4 h over 6 h over 6 h
RV/LV (% change at 48h) -24.0 -22.6 -26.3 -25.5
Miller index (% change at 48h) -5.5 -9.2 -14.0 -25.7
Major bleeding (within 72h) 0 3.7 3.6 11.1*
All-cause mortality 30 days 0 0 0 5.6
All-cause mortality 1 year 3.7 0 0 5.6
* one patients with ICH
Tapson JACC 2018Catheter-Directed Thrombolysis
• Trials focused on the evaluation of imaging surrogates for improved short-term
outcomes.
• CDT more rapidly reverses RV dysfunction in patients with acute PE than
anticoagulation alone. The comparative effectiveness of CDT versus systemic
thrombolysis for this end point is unknown.
• Currently, no data support a short-term mortality, or prevention of recurrent PE,
benefit with catheter-based approaches for the treatment of PE.
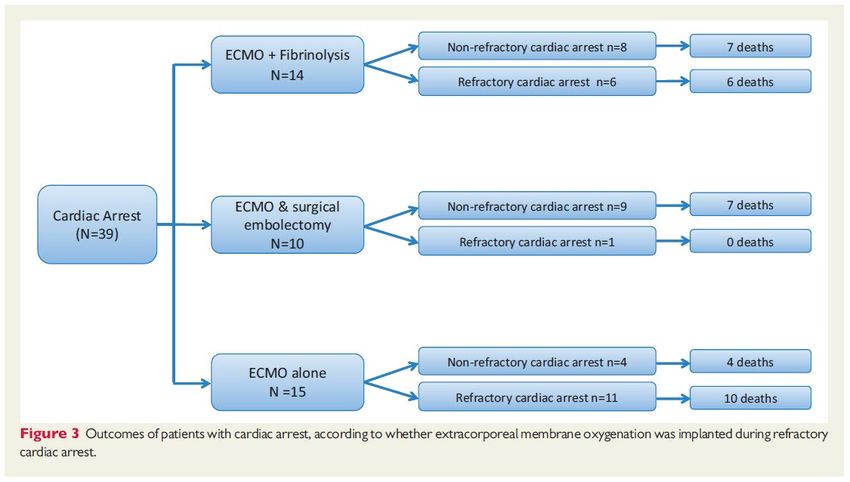
Giri, Circulation 2019Main new recommendations 2019 (3) Treatment in the acute phase When oral anticoagulation is initiated in a patient with PE who is eligible for a NOAC (apixaban, dabigatran, edoxaban, or rivaroxaban), a I NOAC is the recommended form of anticoagulant treatment. Set-up of multidisciplinary teams for management of high-risk and selected cases of intermediate-risk PE should be considered, depending IIa on the resources and expertise available in each hospital. ECMO may be considered, in combination with surgical embolectomy or catheter-directed treatment, in refractory IIb circulatory collapse or cardiac arrest.
ECMO This recommendation is based on the controversial results of case series and of a retrospective cohort study (180 patients included, 52 treated with ECMO). Complications due to the use of ECMO are not negligible.
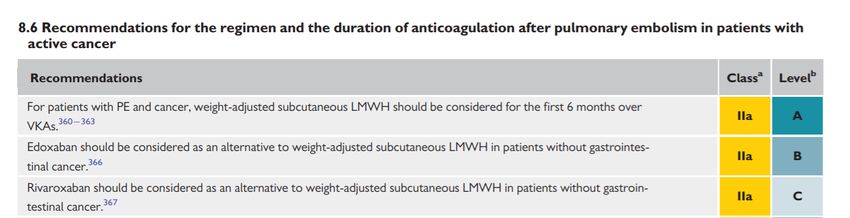
Main new recommendations 2019 (5)
Pulmonary embolism in patients with cancer
Edoxaban or rivaroxaban should be considered as an alternative to LMWH,
IIa
with the exception of patients with gastrointestinal cancer.ASCO- What is the best method for treatment of patients
with cancer with established VTE to prevent recurrence?
Recommendation 4.1.
Initial anticoagulation may involve LMWH, UFH, fondaparinux, or rivaroxaban.
For patients initiating treatment with parenteral anticoagulation, LMWH is preferred over UFH for the initial 5 to 10 days of
anticoagulation for the patient with cancer with newly diagnosed VTE who does not have severe renal impairment (defined as
creatinine clearance < 30 mL/min).
(Type: Evidence based; Evidence quality: High; Strength of recommendation: Strong)
Recommendation 4.2.
For long-term anticoagulation, LMWH, edoxaban, or rivaroxaban for at least 6 months are
preferred because of improved efficacy over vitamin K antagonists (VKAs).
VKA are inferior, but may be utilized if LMWH or direct oral anticoagulants (DOAC) are not accessible.
There is an increase in major bleeding risk with DOAC, particularly observed in GI and potentially GU malignancies. Caution
with DOAC is also warranted in other settings with high risk for mucosal bleeding. Drug-drug interaction should be checked
prior to using a DOAC.
(Type: Evidence based; Evidence quality: High; Strength of recommendation: Strong)
Key, JCO 2019Caso clinico 4 • Paziente di 26 anni 1° gravidanza al 7° mese. • Giunge per episodio di cardiopalmo e dispnea, ECG tachicardia sinusale, non RVD, eco-color-Doppler venoso negativo. PA 100/75 mmHg, FC 120 bpm, SatO2 95% con 4 l/min.
Caso clinico 4 Questions: • D-dimero? Score clinici? • TC torace con mdc?
Caso clinico 4
AnswersDiagnosis
guidelines overview
ACOG 2018 SOGS 2014 RCOG 2015 Au/NZ 2012 ASH 2018
D –dimer testing Is not Should not be Should not be Is not Needs to be
recommended used performed recommended evaluated in
well designed
studies
Clinical prediction -- Should not be -- -- --
rules usedFirst 25%
The rate of symptomatic VTE events
was 0.0% (95% CI, 0.0% to 1.0%)
among untreated women after
exclusion of PE on the basis of Second 11%
negative results on the diagnostic
work-up
Third 4%During follow-up, popliteal DVT was diagnosed in 1 patient (0.21%; 95% CI, 0.04 to 1.2); no patient had PE.
Changes in recommendations 2014-2019 Recommendations 2014 2019 D-dimer measurement and clinical prediction rules should be considered to rule out PE during pregnancy or IIb IIa the postpartum period.
A dedicated diagnostic algorithm
is proposed for suspected PE in
pregnancyEstimated radiation absorbed in procedures used for diagnosing PE
Estimated foetal radiation Estimated maternal radiation
Test exposure (mGy) exposure to breast tissue (mGy)
Chest X-rayCaso clinico 4
mGeneva score 5 (moderate ≈ risk 20-30%)
D-dimero 1180 ng/mL
Criteri YEARS: 1?
Ha eseguito Angio-TC torace, risultata positiva per EP segmentariaTreatment choice
guidelines overview
Acute VTE treatment ACOG 2018 SOGS 2014 RCOG 2015 Au/NZ 2012 ACCP 2012 ASH 2018
LMWH (over UFH) X X X X X X
Againts VKAs -- X X X X X
Against NOACs -- X X -- X X
HIT or heparin fondaparinux consultation fondaparinux, -- fondaparinux, other ASH
allergy argatroban argatroban guidelines
During breastfeeding VKAs, LMWH, -- VKAs, LMWH, -- VKAs, LMWH, VKAs, LMWH,
UFH UFH UFH (alternative UFH,
rather than fondaparinux;
fondaparinux);
against NOAC
against NOAC
Life-threatening PE UFH, UFH, UFH, UFH, UFH, UFH,
thrombolysis thrombolysis thrombolysis, thrombolysis thrombolysis thrombolysis
surgical
embolectomyRecommendations on treatment
Treatment
Therapeutic, fixed dose of LMWH based on early
pregnancy body weight is the recommended therapy
I B
for PE in the majority of pregnant women without
haemodynamic instability.
It is not recommended to insert a spinal or epidural
needle unless at least 24 hours have passed since the III C
last therapeutic dose of LMWH.
It is not recommended to administer LMWH within 4
III C
hours of removal of an epidural catheter.127 cases: 83% massive, 23% with cardiac arrest
Main new recommendations 2019
Pulmonary embolism in pregnancy
Thrombolysis or surgical embolectomy should be considered for pregnant
IIa
women with high-risk PE.
Amniotic fluid embolism should be considered in a pregnant or postpartum
woman with unexplained haemodynamic instability or respiratory deterioration IIa
and disseminated intravascular coagulation.
NOACs are not recommended during pregnancy or lactation. IIICaso clinico 4
Indicators of risk
Clinical
Elevated
Early mortality risk Haemo- parameters of PE RV
cardiac
dynamic severity/ dysfunction on
troponin
instability comorbidity: PESI TTE or CTPA
levels
III–V or sPESI ≥1
High + (+) + (+)
Interme- Intermediate–high - + + +
diate Intermediate–low - + One (or none) positive
Assessment
optional; if
Low - - -
assessed,
negative
Enoxaparina a dosaggio terapeuticoYou can also read