Prevalence of Halitosis in Children and Associated Factors: A Systematic Review and Meta-Analysis.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Prevalence of Halitosis in Children and Associated
Factors: A Systematic Review and Meta-Analysis.
Cindy Buj-Acosta
University of Valencia
Verónica García-Sanz
University of Valencia
Carlos Bellot-Arcís
University of Valencia
Vanessa Paredes-Gallardo ( vanessa.paredes@uv.es )
University of Valencia
Beatriz Tarazona-Álvarez
University of Valencia
Miguel Tortajada-Girbés
University of Valencia
José María Montiel-Company
University of Valencia
Article
Keywords: halitosis, mouth breathing, child, pediatrics, systematic review
Posted Date: January 30th, 2023
DOI: https://doi.org/10.21203/rs.3.rs-2433872/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Read Full License
Page 1/17Abstract
Background: Halitosis is a common and well-studied condition throughout the world. There are several
publications on the etiology and prevalence of halitosis in the adult population. However, in children,
studies are inconclusive. This study aims to perform a systematic review and meta-analysis to establish
the prevalence and factors involved in halitosis in the pediatric population.
Methods: A systematic review was conducted in the databases: Scopus, Cocharne Library, Medline, and
Embase, complemented by a manual search. This review was carried out according to PRISMA standards
and registered in PROSPERO (CRD42020183948).
Results: Twenty-five studies met the inclusion criteria for conducting the qualitative synthesis. Twelve
studies were used for quantitative synthesis and meta-analysis. It was estimated that 36.6% of the
children who participated in the studies had halitosis. The presence of oral breathing, coating of the
tongue, gingival inflammation and inadequate oral hygiene were the main risk factors for the
development of halitosis, with an odds ratio of 8.036 (95% CI: 1-44-9), 3.24 (95% CI 1.38-7.62), 1.577
(95% CI 1.14-2.19) and 3.09 (95% CI 2.36-4.04) respectively.
Conclusions: Given the high prevalence of halitosis in children and the many associated risk factors, a
preventive approach is necessary to avoid its the negative social impact.
Introduction
Halitosis, also known as bad breath or oral malodour, has a multifactorial origin [1]. Oral malodour can be
a significant social or psychological obstacle for people who suffer from it [2]. In fact, it is the third most
common reason why patients visit the dentist, following periodontal diseases and dental caries [3].
Studies have shown that between 85–90% of malodour originates within the oral cavity [4], where gram-
negative anaerobic bacteria degrade sulphur-containing amino acids and produce volatile sulphur
compounds (VSCs), the main components being hydrogen sulfide. (H2S), methyl mercaptan (CH3SH), and
dimethyl sulfide [(CH 3)2S] [5, 6]. Among the associated factors are the salivary alterations, coating of the
tongue, insufficient oral hygiene, periodontal disease such as gingivitis, dental caries, oral breathing and
the presence of both fixed and removable orthodontic appliances [7–9]. Extraoral halitosis generally
associated with respiratory and otolaryngologist disorders, such as acute tonsillitis, postnasal drip, and
sinusitis, accounts for 8% of halitosis diagnoses [10].
At present, only one systematic review and meta-analysis in adults has been published [11], where it was
observed that the prevalence varies according to the investigation due to the age of the subjects, the
inclusion criteria and the methods used for the diagnosis of halitosis. However, most publications
conclude that around 30–50% of the population has halitosis [12]. To date, the few studies that have
studied this aspect in children used different heterogeneous methods, and most focused on halitosis
secondary to upper respiratory tract infections [13]. To try to clarify the prevalence and risk factors
Page 2/17associated with the appearance of halitosis in children, the aim of this study was to carry out a
systematic review of the literature.
Methods
The current systematic review of the literature followed the PRISMA guidelines (Preferred Reporting Items
for Systematic Reviews and Meta-Analyses) [14]. The review protocol was registered in the PROSPERO
database (CRD42020183948).
PICO question.
The main PICO question raised in this review was the following: What is the estimated prevalence and
etiological factors associated with the development of halitosis in children?
Inclusion and exclusion criteria
In order to carry out a rigorous systematic review “Articles” and “Articles in press” were introduced.
Systematic reviews, cohort studies, meta-analyses, randomized clinical trials (RCTs) and case-controlled
studies. Retrospective and prospective studies published during the last 23 years (1999–2022) were
included. The literature search was carried out on August 2022. The language in which a study was
published was not an exclusion criteria. On the other hand, case reports, case series, non-systematic
reviews, and editorials were deleted.
Inclusion criteria of this systematic review and meta-analysis were child and adolescent (age range from
3 to 17 years) in their sample, presence of halitosis was analysed using and objective or subjective
method. Those studies in which the patients had problems in the upper respiratory tract, allergic rhinitis,
and adenoid hypertrophy were discarded for inclusion in the review.
Search strategy and selection of articles
An accurate electronic search was conducted to identify the potentially studies in the following
databases: Cochrane Library, Scopus, Embase and Pubmed. A manual search was conducted in
Opengrey literature and the New York Academy of Medicine Grey Literature Report. In some cases, the
authors of the studies were reached by e-mail to request additional information or answer questions. The
search for articles for the present review was conducted in August 2022.
The keywords used to identify the articles that were directly related to our research question were:
“Halitosis” “Oral Malodor” "Bad Breath" combined with words like "children" "adolescents" "preschool
children" "children population" "paediatric population" "prevalence" "risk factors" "prognostic factors"
"influencing factors" and "predictive factors". Two reviewers (CB-A and VG-S) accurately determined the
inclusion of the different articles in the present systematic review by reading the title and abstract. If there
were any discrepancies between them, this was discussed with a third reviewer (BT-A). In addition, a
Page 3/17manual search was carried out among the bibliographic references of the selected articles in the different
databases to locate any additional studies that the primary search could not identify.
Extraction of data from the included articles
The variables that were extracted from each article were: author, year of publication, study design, sample
size, demographic variables (age and sex), objective halitosis measurement, subjective measurements,
and risk factors analysed. Prevalence rates of halitosis in children were quantified, and the country of
publication and the quality were recorded.
Quality evaluation and risk of bias
Study quality was analyzed by the same investigators (CB-A and VG-S), working independently, using the
Newcastle–Ottawa Scale [15]. When there were differences between the two researchers in rating the
quality of the different articles, a third reviewer was asked (BT-A).
Variables and synthesis of the results
Percentages and 95% confidence intervals (CIs) were calculated for the following variables: prevalence of
halitosis in the paediatric population. Odds ratios (ORs) and 95% CIs were recorded for the following
variables: sex, oral respiration, tongue coating, presence of dental plaque, presence of gingival
inflammation, poor oral hygiene, frequency of brushing, and presence of caries.
Statistical analysis
The odds ratios and 95% confidence intervals of risk factors were calculated for the quantitative
synthesis. Heterogeneity was evaluated by means of the Q-test and I2 statistic. For the Q-test, a p value <
0.1 was considered heterogeneous. I2 values between 25% and 50% were considered to indicate slight
heterogeneity, between 50% and 75% to indicate moderate heterogeneity, and those over 75% to indicate
high heterogeneity. Synthesis of the studies included in the meta-analysis was performed using a
random-effects model. Publication bias was evaluated visually in funnel plots and by the existence of
significant differences estimated between studies observed or imputed by means of the ‘trim and fill’
method. The statistical analysis was designed using Comprehensive Meta-Analysis version 3.0 (Biostat
Inc., England, NJ, USA).
Results
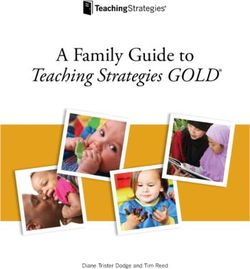
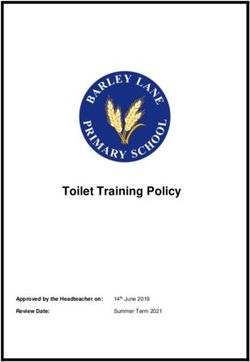
Article selection and flow chart
The electronic database search obtained 398 articles in Scopus, 218 articles in PubMed, 20 articles in
Embase and none in Cochrane, for a total of 636 articles. Searches of grey literature databases found 1
article. An additional reference was added as a result of a manual search. This led to a total of 638
articles, of which 496 were duplicates, leaving 142. After reading the titles and abstracts, another 93
articles were excluded because they did not meet the research objectives of the review, leaving 49 studies.
Page 4/17After a full and detailed reading of the manuscripts, 25 met the inclusion criteria of the review. The
PRISMA flow diagram (Fig. 1) provides an overview of the selection process.
Study characteristics
The 25 studies analysed in the review included 24 cross-sectional clinical studies and one randomized
controlled trial (the article by Keceli et al.) [16]. Most of the studies were of moderate quality according to
the Newcastle–Ottawa assessment (Supplementary Table S1)
Different studies found that the prevalence of halitosis in the paediatric population ranged between 7,6–
86,6%, although not all of the included studies indicated the prevalence of oral malodour in their study
group [7, 17, 18, 19].
All of the studies included in the review had a minimum of 20 patients. The study with the largest sample
size was that of Patil et al., with 900 subjects [20], followed by Alqutami et al., with 785 patients [19]. The
smallest sample was found in the study by Amir et al. (24 patients) [7]. The age of the studies included in
this review ranged from 3 years [21–24] to a mean age of 16 years [25–27]. Regarding the gender of the
subjects included in the studies, most had more boys than girls, except in 6 publications where females
predominated [10, 17, 18, 23, 26, 27]. However, 5 studies did not provide information on the sex of the
patient [19, 28–31], and only 1 study had the same number of girls and boys [32].
Regarding the country of publication, 8 studies were carried out in Turkey [2, 16, 17, 18, 25, 33, 34, 35],
followed by Japan with 4 studies [12, 21, 26, 27]; Italy with 3 studies [13, 32, 36] Brazil, India and Saudi
Arabia with 2 studies; and Korea, Israel, China and Germany, with 1 study that analysed the prevalence
and etiological factors associated with oral malodour in children.
Qualitative synthesis of the studies
All studies together comprised 5620 patients (range 24–900 patients).
Most of the studies were carried out on healthy children. It should be noted that the present review found
publications that analysed the prevalence of oral malodour in children whose parents complained of a
bad oral odour [2, 7, 13, 21, 25, 33]. In the Iscan et al. study, 50% of the patients suffered from type 1
diabetes [35].
Twelve studies were used to evaluate the prevalence of halitosis in the paediatric population.
When comparing halitosis detection methods between the different studies, 13 publications used a
sulphur monitor to measure VSC levels [2, 7, 13, 16, 17, 18, 19, 20, 21, 29, 30, 31, 34], 8 publications used
self-reported halitosis [5, 11, 17, 19, 23, 24, 26, 31], and 19 studies used the organoleptic method to
establish the degree of halitosis in the paediatric population.
Most of the publications aimed to enumerate the etiological factors associated with halitosis, the most
studied of which included: gender [10, 12, 13, 18, 19, 20, 22, 28, 31, 33, 34, 35], the presence of dental
Page 5/17plaque and gingival health [2, 7, 10, 12, 13, 16, 17, 18, 19, 20, 21, 23, 25, 26, 27, 29, 32, 33, 35, 36] the
coating of the tongue [7, 10, 12, 16, 17, 20, 23, 26, 27, 31, 32, 33, 34], mouth breathing [19, 20, 21, 22, 32,
33, 34, 36], the presence of dental caries or by the DFMT, DMFS, dfmt and dfms indices [7, 10, 12, 16, 19,
20, 21, 23, 26, 29, 32, 33, 34, 35], age [12, 13, 20, 28, 33, 34], and frequency of brushing [16, 20, 21, 24, 26,
33, 34]. Only Kim et al. analysed the correlations of obesity, living in a rural area, general health, stress,
frequent alcohol intake, tobacco, soft drinks, fast food and sweets with halitosis [28].
The publication by Petrini et al. related the practice of sports with an oral bad odour [32]. Only the study
by Ueno et al. considered occlusion of the subjects [27]. On the other hand, Erhamza et al. analysed
whether the orthopaedic treatment of rapid maxillary expansion decreased the incidence of halitosis in
the paediatric population [18]. Yildizer et al. and Costacurta et al. compared the existence of halitosis in
children with fixed and removable appliances [17, 36].
Only 6 studies analysed the effect of oral hygiene instructions and tongue brushing in the paediatric
population [2, 7, 16, 20, 25, 33].
The study designs, characteristics of the patients, different ways of measuring both objective and
subjective halitosis, the prevalence of halitosis, etiological factors analysed, and the country of the
studies included in the present review are summarized in Supplementary Table S2.
Quantitative synthesis of the studies
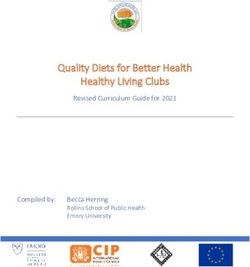
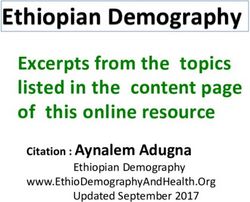
Prevalence of halitosis in the paediatric population
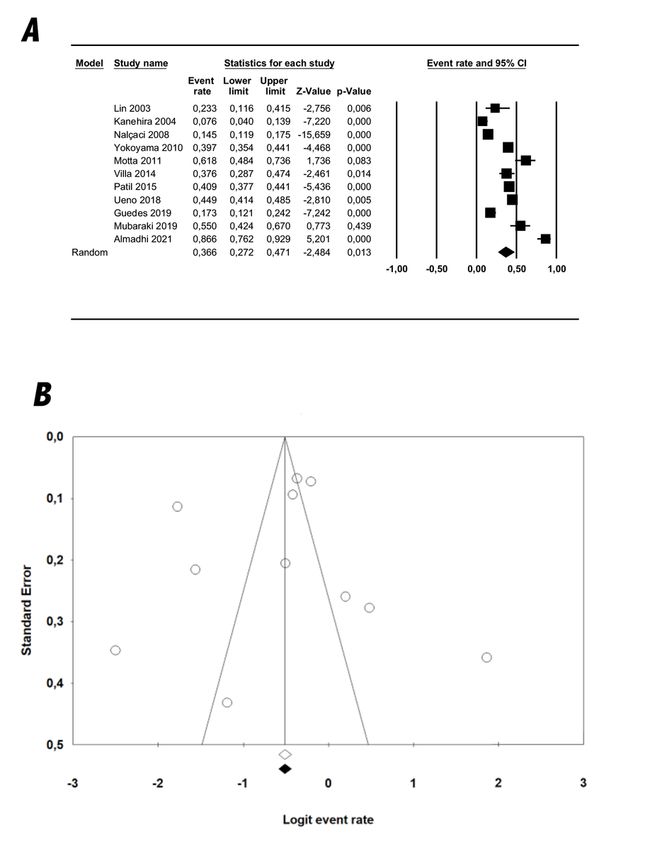
A random effects model estimated that 36,6% of the children who participated in the studies had halitosis
(Fig. 2), with a 95% CI between 27,2% and 47,1%. The I2 value was 100, indicating high heterogeneity
between studies (Q = 271.1; p < 0.001).
Risk factors
Possible risk factors for halitosis in the paediatric population reported in the studies included oral
breathing, oral hygiene index, tongue coating, gingival inflammation, presence of caries, frequency of
brushing and presence of plaque. No association between gender and halitosis was detected in children.
The random effects model was used, giving an estimated OR of 1.13 with a 95% CI between 6.67 and
9.27, which was not significant (p = 0.71). The I2 value was 70.6, which indicates high heterogeneity (Q =
10.22; p = 0.017).
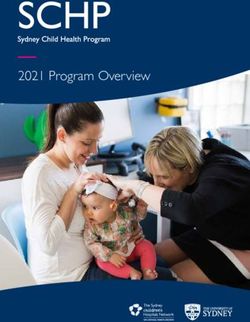
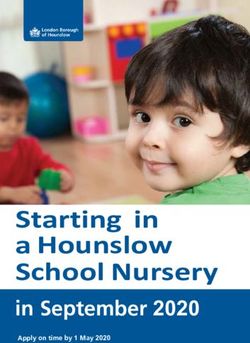
The risk factors that appeared significant in the present meta-analysis were oral breathing, the presence
of tongue coating, and the presence of gingival inflammation (Fig. 3). Mouth breathing showed a higher
risk of presenting halitosis than nasal breathing. A random effects model gave an estimated OR of 8.03,
with a 95% CI between 1.4 and 44.9, which was statistically significant (p = 0.018). The I2 value of 91.84
indicated high heterogeneity (Q = 24.53; p < 0.001). Children who presented tongue coating had a higher
risk of presenting halitosis than those who did not present signs of tongue coating (Fig. 3). A random
Page 6/17effects model gave an estimated OR of 3.24 with a 95% CI between 1.4 and 7.6, which was statistically
significant (p = 0.007). There was high heterogeneity between the studies (I2 = 94.47; Q = 54.3; p = 0.000).
The presence of gingival inflammation was a predictor of halitosis in the paediatric population. Using a
random effects model, an estimated OR of 1.577 was obtained with a 95% CI between 1.14 and 2.19,
which was statistically significant (p = 0.007). There was moderate heterogeneity in the studies (I2 =
56.25, Q = 4.571; p = 0.102). Another predictive risk factor for halitosis was poor oral hygiene since an
estimated OR of 3.088 was obtained with a 95% CI between 2.36 and 4.03, which was highly significant
(p = 0.000). The I2 value was null, indicating an absence of heterogeneity (I2 = 0, Q = 0.088; p = 0.767).
In contrast, risk factors such as tooth decay, brushing frequency, and the presence of dental plaque were
not significant in the meta-analysis.
Table 1 shows the probability of suffering from halitosis when analysed in relation to the presence of risk
factors.
Table 1
Probability of suffering from halitosis in relation to the presence of risk factors.
Risk factor OR 95% CI Q- p- I2 N Number
value value of
Lower Upper (Total) included
limit limit studies
Mouth breathing 8.036 1.438 44.91 24.53 0.018* 91.85 1074 3
Caries 1.185 0.904 1.55 11.27 0.218 64.50 2920 5
Poor oral hygiene 3.088 2.362 4.037 0.088 0.000* 0.000 1050 2
Tongue coating 3.241 1.378 7.622 54.30 0.007* 94.48 2292 4
Gingival 1.577 1.136 2.190 4.571 0.007* 56.24 2142 3
inflammation
Man 1.137 0.570 2.268 10.22 0.716 70.66 1074 4
Women 0.880 0.441 1.755 10.22 0.716 70.66 1074 4
Brushing frequency 1.756 0.964 3.199 3.89 0.066* 74.28 1374 2
(One a day)
Presence of plaque 1.567 1.019 2.410 5.643 0.041* 64.56 1343 3
OR: Odds Ratio; CI: Confidence Interval; * p-value < 0.1 = heterogeneous; I2 > 75 = high heterogeneity
Publication bias
Page 7/17In the present meta-analysis, no publication bias has been detected since, as shown in Fig. 2.b, in the
funnel plots created, the images are symmetrical and without statistically significant differences in the
estimates between studies observed and imputed using the trim and fill method.
Discussion
Halitosis is defined as an unpleasant odour that emanates from the oral cavity and can originate
intraorally and/or extraorally [37]. Its aetiology is multifactorial, affecting both men and women. Despite
its high prevalence, information on the incidence of malodour oral in children remains undefined.
The results of the present systematic review revealed an estimated prevalence of halitosis of 36,6%, a
finding similar to that of Villa et al., who reported a prevalence of 37,4% [13]. However, the prevalence
rates observed in the different studies included in the review were heterogeneous, ranging from 7,6% [19]
to 87% [21]. This variability between the different studies could be due to variations in the methods of
measuring halitosis, the diverse criteria for including or excluding children in the studies, different sample
sizes, and distinct criteria used to consider the presence of halitosis. This is especially true when
comparing the subjective organoleptic method and self-reported halitosis by parents, which is often
unreliable. In fact, it has been suggested that self-reported halitosis tends to underestimate the
prevalence of this condition primarily because subjects cannot detect their own odour or are embarrassed
to report it in interviews [38]. However, Silva et al., concluded in their meta-analysis on the prevalence of
halitosis in adults that the method used for the evaluation of halitosis did not seem to influence the
heterogeneity between the studies and that self-evaluation can be a useful instrument to estimate the
prevalence of halitosis, mainly in large epidemiological studies when it is not possible to use organoleptic
measurements [11].
To date, we can only highlight two systematic reviews published by Bawazir et al., 2021 and Silva et al.,
2022, whose common objective was to determine the etiological factors of halitosis in children [39–40].
Therefore, this publication highlights a significant lack of longitudinal studies in this area.
The present meta-analysis analysed the following etiological factors for the developing of halitosis in
children and adolescents: sex, presence of caries, presence of oral respiration, tongue coating, gingival
inflammation, low frequency of brushing, poor oral hygiene index, and presence of dental plaque. Other
factors, such as age or type of occlusion, could not be analysed, as the studies did not provide the
required information.
Boys showed a higher risk of halitosis than girls, but the result was not significant (p = 0.71). This result
was consistent with previous studies, such as Patil et al., Nalçaci et al. and Kim et al., since men showed
a significantly higher prevalence of halitosis than women in their studies (p < 0.001) [20, 28, 33]. In
contrast, Villa et al. and Zhang et al. suggested that pubertal age in girls was a predictive factor for
halitosis, associating this finding with sexual hormones at this age [13, 31]. On the other hand, the rest of
the studies that analysed sex did not find an association between the presence of volatile sulphur
compounds and sex [10, 16, 21, 22, 27].
Page 8/17Mouth breathing was one of the factors that most contributed to the presence of halitosis in the
paediatric population, since breathing through the mouth leads to a loss of moisture in the tongue and
palate because the oral cavity remains open the greater part of the time, causing halitosis. These findings
were in accordance with authors such as Alquitami et al., Patil et al., Kanehira et al., and Motta et al. [19–
22]. However, Nalçaci et al. did not find any relationship between oral respiration and the presence of
halitosis [33].
It should be noted that the main cause of halitosis was the coating of the tongue located on the posterior
back of the tongue since in all the investigations that analysed the relationship between these variables
[7, 10, 16, 17, 20, 25, 26, 27, 28, 30, 33, 34], a highly significant association between tongue coating and
halitosis was found, considering it to be the greatest risk factor for the appearance of halitosis. Likewise,
authors such as Kara et al., Keceli et al., Patil et al., Çiçek et al., and Nalçaci et al. concluded that brushing
the tongue significantly reduces VSC concentrations more than just brushing the teeth [2, 16, 20, 25, 33]
Regarding the presence of caries as a risk factor in the appearance of halitosis, discrepancies were found,
since authors such as Amir et al., Guedes et al., Almadhi et al., and Nalçaci et al. found a significant
association between oral malodour and the presence of dental caries [7, 10, 23, 33]. However, Almadhi et
al. attributed this association to the fact that the sample selected in their study included children with a
high caries index [23]. On the other hand, Nalçaci et al. related oral malodour with the severity of dental
caries [33] In contrast, authors such as Alqutami et al., Kanehira et al., Patil et al. and Ueno et al. did not
show a correlation between these variables, associating it with the fact that glucose and sucrose can
create an acidic environment that would suppress VSC production [19, 20, 21, 27]. It is important to
highlight the studies by Tanaka et al., 2008 and Ren et al., 2016 whose objective was to evaluate the
supragingival plaque of children to determine the presence of periodontopathic bacteria [41, 42]. An
interesting result was that the group had worse oral hygiene had a greater presence of periodontal
pathogenic bacteria that could be one of the main causes of oral malodour. However, there is a lack of
conclusive studies about.
On the other hand, when the presence of gingival inflammation and poor oral hygiene were analysed in
10 studies [2, 7, 10, 16, 18, 19, 20, 26, 27, 36], bad odour was significantly associated with gingival
pathology and plaque accumulation. The explanation given by the authors for this fact is that the
presence of plaque increases the growth of anaerobic bacteria, which cause the production of VSCs that
lead to halitosis.
Regarding brushing frequency, the studies by Keceli et al., Kanehira et al., Almadhi et al., Yokoyama et al.
and Nalçaci et al. did not find a correlation between these variables, associating these results with poor
brushing technique on the part of children who participated in their studies [16, 21, 23, 26, 33]. In contrast,
in the study by Patil et al., children who brushed twice a day showed a greater reduction in oral malodour
than children who brushed only once a day [20].
One of the main limitations of this review is the heterogeneity of the investigated samples; the different
halitosis measurement methods; and the different clinical indices used to assess the presence of oral
Page 9/17respiration, tongue coating, and caries.
In conclusion, more research is required to analyse the presence of halitosis in the paediatric and
adolescent populations with standardized criteria to determine the causes and risk factors and to design
studies of high methodological quality. Studies should focus on boys and girls with a clearly defined age
range, and the samples should be evenly distributed between the sexes with the same instrument for the
objective measurement of halitosis. The results of our systematic review and meta-analysis provide an
estimate of the prevalence of halitosis in children and adolescents and the associated risk factors. Given
the high rate of halitosis in children population, the social impact on people and multifactorial aetiology,
more longitudinal studies are necessary to help understand its appearance in this population.
Declarations
Data availability: Datasets are available in the manuscript. Any additional information and data are
available upon reasonable request to the corresponding author.
Author Contributions:
All authors made substantial contributions to the formulation of this study. CB-A designed the study, did
the search, data extraction, and analysis, and wrote the paper. VG-S, MT-G, BT-A contributed to the search,
data extraction, quality assessment of included studies, and the narrative synthesis. CB-A contributed to
data analysis. Statistical analyses were carried out by MT-G, JMM-C. VP-G provided supervision to the
project and contributed at all stages. CB-A and BT-A accessed and verified the data. All authors played an
active role in the revision of the manuscript. Final approval was obtained from all authors prior to
submission of the manuscript.
Competing interests:
The authors declare no competing interests.
References
1. Rosenberg, M. The science of bad breath. Sci Am. 4, 72-9 (2002).
2. Kara, C., Tezel, A. & Orbak, R. Effect of oral hygiene instruction and scaling on oral malodor in a
population of Turkish children with gingival inflammation. Int J Pediatr Dent. 16, 399-404 (2006).
3. Loesche, W. The effects of antimicrobial moutrinses on oral malodour and their status relative to use
Food and Drug Administration regulations. Quintessence Int. 30, 311-18 (1999).
4. Pham, T.A., Ueno, M., Zaitsu, T., Takehara, S., Shinada, K. et al. Clinical trial of oral malodor treatment
in patients with periodontal diseases. J Periodontal Res. 46, 722-9 (2011).
5. Tonzetich, J. Production and origin of mal malodour: review of mechanisms and methods of
analysis. J Periodontol. 48, 13-20 (1977).
Page 10/176. Scully, C. & Greenman, J. Halitosis (breath odor). Periodontol 2000. 48, 66-75 (2008).
7. Amir, E., Shimonov, R. & Rosenberg, M. Halitosis in children. J Pediatr. 134, 338-43 (1999).
8. Yaegaki, K. & Sanada, K. Volatile sulfur compounds in mouth air from clinically healthy subjects and
patients with periodontal disease. J Periodontal R. 27, 233–8. (1992).
9. Yaegaki, K. & Sanada, K. Biochemical and clinical factors influencing oral malodor in periodontal
patients. Journal Periodontol. 63, 783-9 (1992).
10. Guedes, C.C., Bussadori, S.K., Weber, R., Motta, L.J., Costa da Motta, A.C. et al. Halitosis: prevalence
and association with oral etiological factors in children and adolescents. J Breath Res. 13, 026002;
https://doi.org/10.1088/1752-7163/aafc6f (2009).
11. Silva, M.F., Leite, F.R.M., Ferreira, L.B., Pola, N.M., Scannapieco, F.A., et al. Estimated prevalence of
halitosis: a systematic review and meta-regression analysis. Clin Oral Invest. 22, 47–55 (2018).
12. Ueno, M., Ohnuki, M., Zaitsu, T., Takehara, S., Furukawa, S. et al. Prevalence and risk factors of
halitosis in Japanese school children. Pediatr Int. 6, 588-92 (2018).
13. Villa, A., Zollanvari, A., Alterovitz, G., Cagetti, M.G., Strohmenger, L. et al. Prevalence of halitosis in
children considering oral hygiene, gender and age. Int. J. Dent Hygiene. 12, 208–12 (2012).
14. Liberati, A., Altman, D.G., Tetzlaff, J., Mulrow, C., Gotzsche, P.C. et al. The PRISMA statement for
reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions:
explanation and elaboration. BMJ. 29, 339 (2009).
15. Wells, G.A., Shea, B., O’Connell, D., Robertso, J., Peterson, J. et al. Loso. The Newcastle-Ottawa Scale
(NOS) for Assessing the Quality of Non-randomized Studies in Meta-analyses. Ottawa Hospital
Research Institute, Ottawa, ON. http://www.ohri.ca/ programs/clinical_epidemiology/oxford.asp
(2019).
16. Keceli, T., Gulmez, D., Dolgun, A. & Tekcicek, M. The relationship between tongue brushing and
halitosis in children: a randomized controlled trial. Oral Dis. 1, 66-73 (2015).
17. Yıldızer, E., Atabek, D. & Güngör, K. Effects of fixed and removable space maintainers on halitosis.
BMC Oral Health. 1, 99 (2016).
18. Erhamza, T. & Ozdiler, F.E. Effect of rapid maxillary expansion on halitosis. Am J Orthod Dentofacial
Orthop. 5, 702-7 (2018).
19. Alquitami, J., Elger, W., Grafe, N., Hiemisch, A., Kiess, W. et al. Dental health, halitosis, and mouth
breathing in 10-to-15-year-old children: A potential connection. Eur J Paediatr Dent. 4, 274-9 (2019).
20. Patil, P.S., Pujar, P., Poornima, S. & Subbareddy, V.V. Prevalence of oral malodour and its relationship
with oral parameters in Indian children aged 7–15 years. Eur Arch Paediatr Dent. 15, 251-8 (2014).
21. Kanehira, T., Takehara, J., Takahashi, D., Honda, O. & Morita, M. Prevalence of oral malodor and the
relationship with habitual mouth breathing in children. J Clin Pediatr Dent. 4, 285-8 (2004).
22. Motta, L.J., Bachiega, J.C., Guedes, C.C., Larania, L.T. & Bussadori, S.K. Association between halitosis
and mouth breathing in children. Clinics. 6, 939-42 (2011).
Page 11/1723. Almadhi, N.A., Sulimany, A.M., Alzoman, H.A. & Bawazir, O.A. Halitosis and Associated Risk Factors in
Children: A Cross-sectional Study. J Contemp Dent Pract. 1, 51-5 (2021).
24. Lin, M.I., Flaitz, C.M., Moretti, A.J, Seybold, S.V. & Chen, J.W. Evaluation of halitosis in children and
mothers. Pediatr Dent. 6, 553–8 (2003).
25. Çiçeck, Y., Orbak, R., Telez, A., Orbak, Z. & Erciyas, K. Effect of tongue brushing on oral malodor in
adolescents. Pediatr Int.45, 719-23 (2003).
26. Yokoyama, S., Ohniki, M., Shinada, K., Ueno, M., Wright, F.A. et al. Oral malodor and related factors in
Japanese senior high school students. J Sch Health. 7, 346-52 (2010).
27. Ueno, M., Shinada, K., Zaitsu, T., Yokoyama, S. & Kawaguchi, Y. Effects of an oral health education
program targeting oral malodor prevention in Japanese senior high school students. Acta Odontol
Scand. 70, 426–31 (2012).
28. Kim, S.Y., Sim, S., Kim, S.G., Park, B. & Choi, H.G. Prevalence and associated factors of subjective
halitosis in korean adolescents. Plos One. 10, e0140214;
https://doi.org/10.1371/journal.pone.0140214 (2015).
29. Sara, M., Rawabi, E., Rawan, M., Razan, A. & Mayar, S. Oral halitosis in Saudi Children. Adv Dent &
Oral Health. 5, 555798; https://doi.org/10.19080/ADOH.2019.10.555798 (2019).
30. Patil, P.S., Pujar, P. & Subbareddy, V.V. Effect of different oral hygiene measures on oral malodor in
children aged 7–15 years. J Indian Soc Pedod Prev Dent. 33, 218–22 (2015).
31. Zhang, Q., Liu, X.N., Chang, Q., AO, S., Zheng, S.G. et al.. Analysis of volatile sulfur compounds
production of oral cavity in preschool children and influencing factors. Beijing Da Xue Xue Bao Yi
Xue Ban. 6, 983-9 (2015).
32. Petrini, M., Costacurta, M., Biferi, V., Benavoli, D., Docimo, R. et al. Correlation between halitosis, oral
health status and salivary ß-galactosidases and time spent in physical activities in children. Eur
Paediatr Dent. 4, 260-4 (2018).
33. Nalçaci, R., Dulgergil, T., Oba, A.A. & Gelgör, I.E. Prevalence of breath malodour in 7- 11-year-old
children living in Middle Anatolia, Turkey. Community Dent Health. 3, 173-7 (2008).
34. Nalçaci, R. & Sönmez, I.S. Evaluation of oral malodor in children. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod. 106, 384-8 (2008).
35. Iscan, T.A., Ozler-Ozler, C., Keceli, T., Dogan, B., Alikasifoglu, A. et al. Oral Health and Halitosis Among
Type 1 Diabetic and Healthy Children. J Breath Res. 3, 036008; https://doi.org/10.1088/1752-
7163/ab8d8b (2020).
36. Costacurta, M., Petrini, M., Biferi, V., Arcuri, C., Spoto, G. et al. The correlation between different
techniques for the evaluation of oral malodour in children with and without orthodontic treatment.
Eur J Paediatr Dent.3, 233–6 (2019).
37. Apatzidou, A.D., Bakirtzoglou, E., Vouros, I., Karagiannis, V. & Konstantinidis, A. Association between
oral malodour and periodontal disease- related parameters in the general population. Acta Odontol
Scand. 71, 189-95 (2012).
Page 12/1738. Bornstein, M.M., Kislig, K., Hoti, B.B., Seemann, R. & Lussi, A. Prevalence of halitosis in the population
of the city of Bern, Switzerland: a study comparing self-reported and clinical data. Eur J Oral Sci. 117,
261–7 (2009).
39. Bawazir, O.A. Risk Factors, Diagnosis, and Management of Halitosis in Children: A Comprehensive
Review. J Contemp Dent Pract. 8, 959–63 (2021).
40. Silva, C.R., Silva, C.C. & Rodrigues, R. Etiology of halitosis in pediatric dentistry. Arch Pediatr. 29, 467-
74 (2022).
41. Tanaka, S., Yoshida, M., Murakami, Y., Ogiwara, T., Shoji, M. et al. The relationship of prevotella
intermedia, prevotella nigrescens and prevotella melaninogenica in the supragingival plaque of
children, caries and oral malodor. J Clin Pediatr Dent. 32, 195-200 (2008).
42. Ren, W., Zhang, Q., Liu, X., Zheng, S., Ma, L. et al. Supragingival plaque microbial community analysis
of children with halitosis. J Microbiol Biotechnol. 26, 2141– 7 (2016).
Figures
Page 13/17Figure 1
Study selection process.
Page 14/17Figure 2
Prevalence of halitosis in the paediatric population in the different studies. A) Forrest plot; B) Funnel plot.
CI confidence interval
Page 15/17Figure 3
Forrest plots for the halitosis associated factors (mouth breathing, tongue coating, gingival inflammation
and poor oral hygiene). CI confidence interval
Supplementary Files
Page 16/17This is a list of supplementary files associated with this preprint. Click to download.
S1.pdf
S2.pdf
Page 17/17You can also read