Prescribing Matters - the City and Hackney GP Website
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
April 2019
Prescribing Matters
The APRIL issue of the City and Hackney CCG Medicines Management Newsletter contains prescribing updates on topics of
current interest for healthcare professionals in practices.
CONTENTS
Page 1 – Virtual reviews (respiratory audit) submission deadline
Page 1 - Preparing for the possibility of a ‘no deal’ EU exit for primary care
Page 2 – End of life medicines (EOLC) update
Page 2 – Pharmacy First
Page 3 – Ghost generics
Page 3 – Gabapentin and pregabalin schedule 3 controlled drugs
Page 3 – TARGET toolkit update
Page 4 – The national flu immunisation programme 2019/20
Page 4 – City and Hackney CCG NRLS error reporting update 2018/19
Page 6 – NHSE PGD update
Page 6 – Levopromazine HCL 25mg / ml injection shortage
Page 7 – MHRA Drug Safety Update April 2019
Page 8 - Contact details
Congratulations to Hetal Dhruve (specialist respiratory pharmacist) who ran the London
Marathon in just over 4 hours. Hetal is raising money for SENSE and donations can be made via
https://uk.virginmoneygiving.com/fundraiser-display/showROFundraiserPage?userUrl=hetal-
dhruve2019&pageUrl=2
Virtual reviews (respiratory audit) submission deadline
Virtual Reviews were carried out by a Specialist Respiratory Pharmacist on 10 patients within each practice as part of
the respiratory audit. Each practice is required to implement actions that may have been identified for the GP to
undertake and document on EMIS.
Practices should email a brief summary of the actions taken by the GP to the Medicines Management Team (MMT)
by the revised deadline of Friday 10th May.
If you did not receive the summary of virtual reviews please contact the Specialist Respiratory Pharmacist
(hetal.dhruve@nhs.net) or MMT (cahccg.cityandhackneymedicines@nhs.net) urgently.
Please note that the summary should provide a very brief outline of issues that were identified / any interventions
made / plans for future interventions to be taken.
The anonimised summary must be sent to the Medicines Management Team in order for the Respiratory Audit to
be considered fully completed. If you have any queries regarding the above, your Practice Support Pharmacist will
be able to assist you.
Preparing for the possibility of a ‘no deal’ EU exit for primary care
NHS England (NHSE) has written a letter to healthcare professionals as a companion to Operational Guidance
published in December by the DHSC regarding EU exit across the health and care sector, setting out actions needed
from the NHS. This letter provides details of the National Supply Disruption Response (NSDR) set up by thePrescribing Matters
Department of Health and Social Care. NSDR systems aim to enhance processes and systems which already exist, for
responding to serious supply disruption events for medical products.
Practices should continue to advise patients to not stockpile medicines, medical devices or clinical consumables.
Practices should raise any issues or concerns to CCG Medicines Management Team (MMT) so that they are
escalated as appropriate.
Continuity of supply
DHSC has been working with suppliers of medicines, medical devices and clinical consumables to identify which
products, ingredients or components are either made in the European Union (EU) or are imported into the U.K. via
the E.U.
Pharmacy and prescription only medicines suppliers and manufacturers have been asked to ensure that they
increase their buffer stocks to hold at least an additional six weeks of stock (over and above usual buffer stock) in the
UK.
Raising concerns about medicines shortages
The DHSC works very closely with manufacturers and wholesalers of medicines to minimise the impact and manage
medicines shortages which can occur for many different reasons which may or may not be related to EU exit.
Actions to take regarding medicines shortages will be shared with practices as necessary through the MMT.
Community pharmacists are expected to report shortages to the DHSC via PSNC. The shortages are collated and fed
back to the primary care teams.
If the community pharmacist is unable to achieve a satisfactory resolution, then these should be escalated at the
earliest opportunity to the MMT.
End of Life Care (EOLC) medicines update
The community pharmacy service which provides 24/7 access to medicines at the end of life is continuing in
2019/20. Plans for a similar service to be commissioned from NHS England have been delayed so our local C&H CCG
service will continue until a replacement is in operation.
Overall feedback on the service has been very good but following an issue when a GP struggled to find the contact
number we are now making the phone number available to GP practices directly. This is 0845 299 3471; please note
• The phone number is only for emergency access to end of life care medicines on the agreed list, when none
of the ten pharmacies providing the service are open
• This service is only for patients registered with a City & Hackney GP practice
• This number must not be given to patients or carers under any circumstances.
The supporting documents for this service have all been updated (see link below) and contain details of the
pharmacies, the courier service and the list of medicines stocked. If you have any queries or feedback about the
service please contact MMT.
https://gps.cityandhackneyccg.nhs.uk/prescribing-guidelines/end-of-life-care-medicines-resource-pack
Pharmacy First
You may remember that NHS England announced plans 12 months ago to decommission this service where patients
can get advice and treatment from their community pharmacies. The CCG has been working with NHSE to make the
case for why a revised service is very much needed as part of our plans to implement the national guidance on OTC
medicines that was published last year (1). The latest is that we remain hopeful that the current NHSE service can
continue until a revised service is available for socially vulnerable people that cannot afford to buy over the counter
medicine. We cannot guarantee if a revised service will be available but we are working diligently to make the case
for a revised service.
1. Guidance on conditions for which over the counter items should not routinely be prescribed in primary care
March 2018 NHS England & NHS clinical commissioners
Page 2 of 9Prescribing Matters
Ghost generics
Ghost-branded generics are generic products which have unintentionally been prescribed with a manufacturer
name. For example, Naratriptan 2.5mg Tablets is the correct generic name; a ghost-branded version is “Naratriptan
2.5mg Tablets (Teva UK Limited).”
When an item is prescribed generically, the dispenser is reimbursed at the national price in the Drug Tariff; but when
a manufacturer is stated by the prescriber, the reimbursement price is usually more expensive.
Prescribers should be careful when selecting products off the EMIS picking list and to beware of being charged
higher price than listed tariff price, for the products they prescribe.
Gabapentin and pregabalin Schedule 3 controlled drugs
Practices should note that from 1st April 2019 gabapentin and pregabalin are Schedule 3 Controlled Drugs (CDs).
Prescriptions are subject to prescription writing requirements for Schedule 3 CDs and it will not be possible to supply
these drugs through repeat dispensing.
Controlled Drug (CD) prescription writing requirements:
To be valid, prescriptions for Schedule 3 CDs must contain the following:
• The dose
• The form
• The strength (where appropriate)
• The total quantity or dosage units of the preparation in both words and figures
Prescribers can now issue computer-generated paper prescriptions for all Controlled Drugs (CDs) including Schedule
2 and 3 CDs; all details except the signature can be computer-generated. The requirement that CD prescriptions
should be written in the prescriber’s own handwriting was removed in November 2005.
Practices in City and Hackney had roll out of controlled drugs in EPS from 25 March 2019 so all GP practices should
now able to prescribe controlled drugs electronically.
Practices should check that roll out of CDs on EPS on EMIS has occurred – please contact EMIS if this has not
happened.
TARGET toolkit update
Practices should note recent updates to the TARGET Toolkit. The toolkit is designed to be used by practices. These
resources can be used flexibly and will enable practices to demonstrate compliance with the Health and Social Care
Act 2008: Code of Practice on the prevention and control of infections and related guidance.
The TARGET Treating Your Infection (TYI) leaflet translations for the RTI and UTI leaflets have been
updated. Additionally translations for the UTI older adult pictorial leaflet and the RTI pictorial leaflet have been
updated. This includes 5 new languages based on user requests over the last two years. The translations have been
uploaded in pdf, but if practices need a word copy please email the TARGET team.
Also online are the newly updated acute cough and UTI clinical scenario PowerPoints and the main presentation,
based on recently updated national treatment guidelines (please follow link above).
Page 3 of 9Prescribing Matters
The national flu immunisation programme 2019/20
DHSC, PH and NHSE have written a letter jointly to practices outlining the national flu immunisation programme
2019/20. This coming winter, the only change to the eligibility criteria is the planned extension of the programme to
school year 6 children. This means that all primary school aged children will now be offered the vaccine for the first
time in England.
In 2019/20 the following are eligible for flu vaccination:
• all children aged two to ten years (but not eleven years or older) on 31 August 2019
• those aged six months to under 65 years in clinical risk groups
• pregnant women
• those aged 65 years and over
• those in long-stay residential care homes
• carers
• close contacts of immunocompromised individuals
Vaccines for the national flu immunisation programme
Based on JCVI advice the range of recommended flu vaccines in 2019/20 has been extended to include those below:
For children aged 2 to 17 years
The live attenuated influenza vaccine (LAIV) continues to be the recommended vaccine, unless contraindicated.
Those contraindicated, and children under the age of 2 years, should be offered a suitable inactivated quadrivalent
influenza vaccine. This year, Public Health England (PHE) has purchased the egg-grown quadrivalent influenza
vaccine (QIVe) for children aged 6 months to less than 2 years, and for those 2 years or above in whom LAIV is
contraindicated.
For those aged 18 to 64 years
There are two vaccines which JCVI advises are equally suitable for use - the standard egg-grown quadrivalent
influenza vaccine (QIVe) and the newly licenced cell-based quadrivalent influenza vaccine (QIVc). Both offer
protection against four strains of flu.
For those aged 65 and over
There are three vaccines that JCVI advised are equally suitable for use. The adjuvanted trivalent influenza vaccine
(aTIV) continues to be recommended for this age group as it is likely to be a more effective vaccine than the
standard dose non-adjuvanted trivalent and egg-based quadrivalent influenza vaccines. Equally suitable, is the newly
licenced cell-based quadrivalent influenza vaccine (QIVc). Whilst also suitable for this age group, the newly licenced
high dose trivalent influenza vaccine (TIV-HD) is not eligible for reimbursement under the NHS flu vaccination
programme because it has a significantly higher list price.
Full document can be accessed here -
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/788903/Annua
l_national_flu_programme_2019_to_2020_.pdf
City and Hackney CCG NRLS Error Reporting Update 2018-19
Thank you to all practices who have shared NRLS reports with MMT. We provide a breakdown of reporting
below. Practices should continue to share patient safety incident reports via NRLS for wider learning and
improving the quality of care we provide our patients.
Fig 1. Number and nature of NRLS incidents reported in 2018/19
41 (out of 42) practices shared at least ONE incident report with MMT
107 incident reports of which 4 were duplicates i.e. 103 unique reports
Page 4 of 9Prescribing Matters
86 of 103 reports are medication related
Of the 17 not related to medicines
1 error is device related ; 1 relates to access to medical review
7 relate to clinical assessment
8 communication related
Fig 2. Incident type and frequency April 2018 – March 2019
Incident Type Number %
Medicine related 86 83.5%
Clinical Assessment/Result Interpretation 1
Clinical Assessment/Diagnosis 6
Documentation / Interface communication 3
Communication, confidentiality 5
Medical device / equipment 1
Access, admission, transfer 1
Total 103
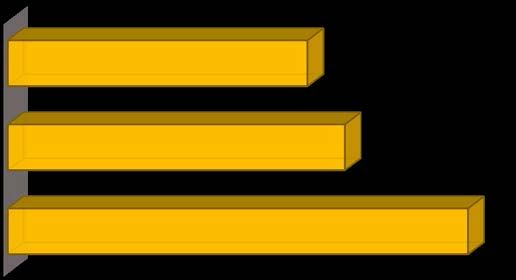
Fig 3. Breakdown of medicines related incident reports
C&H CCG MEDICINE RELATED INCIDENT REPORTS SHARED
WITH CCG VIA NRLS APR
Prescribing Stage 56
Reported as no harm caused 63
Medication Related 86
Page 5 of 9Prescribing Matters
NHSE PGD update
NHS England London Region has published two updated PGDs on its website. This can be accessed
at http://www.england.nhs.uk/london/immunis-team/
The updated PGDs are:
• NHSE PHE Hep B PGD v01.00
Practices should ensure that any registered healthcare professional who is due to administer vaccinations under
these PGDs should be made aware of these updated versions.
If you have any queries, please contact the London Immunisations team via england.londonimms@nhs.net.
Levopromazine hydrochloride 25mg / ml injection shortage
Sanofi, one of the manufacturers of levomepromazine will be out of stock of this product until the end of April.
Levomepromazine hydrochloride 25mg /ml solution for injection is stocked by the City & Hackney pharmacies in the
improving access to medicines at the end of life scheme. If stock of levomepromazine runs out, management options
will need to be determined on a case by case basis, in consultation with the specialist palliative care team.
NICE Bites
NICE Bites March 2019, No 116, includes two antimicrobial prescribing guidelines:
1. Acute exacerbation of bronchiectasis - this guideline sets out an antimicrobial prescribing strategy for
managing and preventing acute exacerbations of bronchiectasis (non-cystic fibrosis). It aims to optimise
antibiotic use and reduce antibiotic resistance.
2. Acute cough - This guideline sets out an antimicrobial prescribing strategy for acute cough associated with
an upper respiratory tract infection or acute bronchitis in adults, young people and children. It aims to limit
antibiotic use and reduce antibiotic resistance.
Page 6 of 9Prescribing Matters
https://www.sps.nhs.uk/wp-content/uploads/2019/03/NICE-Bites-Mar-2019-Bronchiectasis-and-acute-cough-
antimicrobial-prescribing.pdf
MHRA – Drug Safety Update April 2019
Yellow fever vaccine (Stamaril) and fatal adverse reactions: extreme caution needed in people
who may be immunosuppressed and those 60 years and older
MHRA recently received 2 reports of fatal adverse reactions to the yellow fever vaccine (Stamaril). Due to an
increased risk of life-threatening reactions, the vaccine must not be given to anyone with a medical history of
thymus dysfunction or who is immunosuppressed. In addition, extreme caution must be used and a careful risk
assessment conducted before vaccination of people aged 60 years and older due to a substantially increased risk of
such adverse reactions in this age group.
Advice for healthcare professionals:
• As with any live attenuated vaccine, yellow fever vaccine must not be given to people who may be
immunosuppressed
• Yellow fever vaccine is contraindicated in people with a history of thymus dysfunction (including myasthenia gravis
and thymoma)
• Yellow fever vaccine is contraindicated in people who have had their thymus gland removed (thymectomy)
• In people aged 60 years and older, the vaccine should only be given when it is considered that there is a significant
and unavoidable risk of acquiring yellow fever infection
• Professionals who administer yellow fever vaccine must be familiar with any contraindications and special
precautions before proceeding with immunisation.
• If there is any doubt as to whether a person who is due to receive yellow fever vaccine may be immunosuppressed,
immunisation should be deferred until specialist advice has been sought
• Protocols and checklists should be strengthened to avoid inappropriate administration that can lead to severe and
possibly fatal adverse effects; those administering the vaccine should also be familiar with the YF Vaccine Centre
Code of Practice
• Any suspected adverse reactions during immunisations should be reported on a Yellow Card
Risk assessment at vaccination
When a person presents for yellow fever immunisation, it is important that healthcare professionals clearly discuss
with them the individual risks and benefits of the vaccine based on their specific travel itinerary. Sufficient time
should be set aside to ensure that the person is immune competent and has no contraindications to the vaccine,
including a review of full medical history and any available medical records. Any potential history of thymus disease
or thymus removal should be specifically queried. Any decision to administer the vaccine to a person aged 60 years
and older must be based on a significant and unavoidable risk of acquiring yellow fever infection. Provision of the
Patient Information Leaflet would provide a helpful basis for this discussion with potential vaccinees. Risk
assessment checklists should also be used to ensure checks have been completed and patients have been assessed
for immunocompetence.
NaTHNaC recommends that health professionals use a travel risk assessment form to guide the travel health
consultation and, where appropriate, seek specialist advice when a significant medical history is identified. More
Page 7 of 9Prescribing Matters
information on yellow fever, and the YF Vaccine Centre code of practice can be found on the NaTHNaC website -
https://travelhealthpro.org.uk/
Any medication error (for example, vaccination of a contraindicated patient) that results in harm should be reported
via the Yellow Card Scheme. Medication errors in the absence of harm should be reported to NHS England via the
National Reporting and Learning System.
Valproate medicines and serious harms in pregnancy: new Annual Risk Acknowledgement Form
and clinical guidance from professional bodies to support compliance with the Pregnancy
Prevention Programme
The Annual Risk Acknowledgement Form for the valproate Pregnancy Prevention Programme has been updated and
should be used during annual specialist review of all women and girls of childbearing potential on valproate
medicines.
Advice for healthcare professionals:
• use the revised Annual Risk Acknowledgement Form (version dated March 2019) at initiation and annual
review of all girls and women of childbearing potential on valproate medicines (irrespective of indication)
• specialists should comply with guidance on the form if they consider there to be compelling reasons to
indicate their patient is not at risk of pregnancy, including the need to document reasons for this and for the
patient or responsible person to sign to confirm these are correct
• if the absence of pregnancy risk may change (for example, the patient is pre-menarchal), the date for the
next annual discussion of the risks must be documented and the patient or the patient’s family or caregivers
asked to contact the prescriber rapidly if the situation changes
• there is no safe dose of valproate that can be used in pregnancy – see reminder below for key facts about
the risks if pregnancies are exposed to valproate
It is the prescriber’s responsibility to ensure women and girls of childbearing potential (from menarche to
menopause) who are taking a valproate medicine, irrespective of indication, fulfil all the requirements of the
Pregnancy Prevention Programme. These responsibilities include that the patient (or responsible person) and their
specialist must complete the Annual Risk Acknowledgement Form at each year’s annual review.
The Annual Risk Acknowledgement Form has been updated following feedback from healthcare professionals and
stakeholders and should be used for all future reviews of female patients on valproate.
The form can now be used to record when the specialist considers the patient not to be at risk of pregnancy, either
permanently or until the date of the next annual review. Patients or their responsible person must countersign this
section to confirm details given are correct.
How to contact us
For any queries, notifications, alerts and email correspondence please ensure at all times to use our secure team
generic email account: cahccg.cityandhackneymedicines@nhs.net or alternatively contact us on 0203 816 3224.
Reminder: The Medicines Management team should not be emailed directly (to their individual email addresses), as
they maybe on leave, off site, etc. Thus using named individual email addresses may cause an unnecessary and
avoidable delay.
Page 8 of 9Prescribing Matters
For all enquiries and/or concerns that relate to the management and use of Controlled
Drugs: england.londoncdaccountableoffice@nhs.net
All information in this document is summarised from the best currently available sources to help inform your
practice. Every effort has been made to ensure that information is correct at the time of the issue but for more
detailed information please refer to the original material, which is referenced in each case.
Page 9 of 9You can also read