Practice parameter: Screening and diagnosis of autism
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Special Article
Practice parameter: Screening and
diagnosis of autism
Report of the Quality Standards Subcommittee of the
American Academy of Neurology and the
Child Neurology Society
P.A. Filipek, MD; P.J. Accardo, MD; S. Ashwal, MD; G.T. Baranek, PhD, OTR/L; E.H. Cook, Jr., MD;
G. Dawson, PhD; B. Gordon, MD, PhD; J.S. Gravel, PhD; C.P. Johnson, MEd, MD; R.J. Kallen, MD;
S.E. Levy, MD; N.J. Minshew, MD; S. Ozonoff, PhD; B.M. Prizant, PhD, CCC-SLP; I. Rapin, MD;
S.J. Rogers, PhD; W.L. Stone, PhD; S.W. Teplin, MD; R.F. Tuchman, MD; and F.R. Volkmar, MD
Article abstract—Autism is a common disorder of childhood, affecting 1 in 500 children. Yet, it often remains unrecog-
nized and undiagnosed until or after late preschool age because appropriate tools for routine developmental screening and
screening specifically for autism have not been available. Early identification of children with autism and intensive, early
intervention during the toddler and preschool years improves outcome for most young children with autism. This practice
parameter reviews the available empirical evidence and gives specific recommendations for the identification of children
with autism. This approach requires a dual process: 1) routine developmental surveillance and screening specifically for
autism to be performed on all children to first identify those at risk for any type of atypical development, and to identify
those specifically at risk for autism; and 2) to diagnose and evaluate autism, to differentiate autism from other develop-
mental disorders.
NEUROLOGY 2000;55:468–479
This statement has been endorsed by the American Academy of Audiology, the American Occupational Therapy Association, the American Speech–
Language–Hearing Association, the Autism National Committee, Cure Autism Now, the National Alliance for Autism Research, and the Society for
Developmental Pediatrics.
From the Departments of Pediatrics and Neurology (Dr. Filipek), University of California, Irvine, College of Medicine; Department of Pediatrics (Dr.
Accardo), New York Medical College, Valhalla; Department of Pediatrics (Dr. Ashwal), Loma Linda University School of Medicine, California; Departments of
Allied Health Sciences (Dr. Baranek) and Pediatrics (Dr. Teplin), University of North Carolina at Chapel Hill; Departments of Psychiatry (Dr. Cook) and
Pediatrics (Drs. Cook and Kallen), University of Chicago, Illinois; Department of Psychology (Dr. Dawson), University of Washington, Seattle; Department of
Neurology and Cognitive Science (Dr. Gordon), The Johns Hopkins Medical Institutions, Baltimore, Maryland; Departments of Otolaryngology (Dr. Gravel),
Neurology and Pediatrics (Dr. Rapin), Albert Einstein College of Medicine, Yeshiva University, Bronx, New York; Department of Pediatrics (Dr. Johnson),
University of Texas Health Science Center, San Antonio; Department of Pediatrics (Dr. Levy), University of Pennsylvania School of Medicine, Philadelphia;
Department of Psychiatry and Neurology (Dr. Minshew), University of Pittsburgh School of Medicine, Pennsylvania; Departments of Psychology and
Psychiatry (Dr. Ozonoff), University of Utah, Salt Lake City; Center for Study of Human Development (Dr. Prizant), Brown University, Providence, Rhode
Island; Department of Psychiatry (Dr. Rogers), University of Colorado Health Sciences Center, Denver; Department of Pediatrics (Dr. Stone), Vanderbilt
University Medical Center, Nashville, Tennessee; Department of Neurology (Dr. Tuchman), University of Miami School of Medicine, Florida; and Depart-
ment of Child Psychiatry and the Child Study Center (Dr. Volkmar), Yale University School of Medicine, New Haven, Connecticut.
Supported by the National Institute of Child Health and Human Development; the National Institute of Deafness and Communication Disorders; the
National Institute of Mental Health; the National Institute of Neurologic Disorders and Stroke; the NIH Office of Behavioral and Social Sciences Research;
the Maternal and Child Health Bureau, Health Resources; and Services Administration, Department of Health and Human Resources. Supported in part by
HD28202/ HD27802/ HD35458 (P.A.F.), HD35482 (E.H.C. and F.R.V.), HD34565 (G.D.), HD36080 (J.S.G.), HD35469 (N.J.M.), HD35468 (S.J.R.) and
HD03008 (F.R.V.) from the National Institute of Child Health and Human Development; DC00223 (J.S.G.) from the National Institute of Deafness and
Communication Disorders; MH01389/ MH52223 (E.H.C.), MH47117 (G.D.), and MH50620 (W.L.S.) from the National Institute of Mental Health; NS35896
(P.A.F.), NS33355 (N.J.M.), NS20489 (I.R.), from the National Institute of Neurologic Disorders and Stroke, and by the NIH Office of Behavioral and Social
Sciences Research, National Institutes of Health, Bethesda, MD. Supported by MCJ-369029 (P.J.A.) from the Maternal and Child Health Bureau, Health
Resources and Services Administration, Department of Health and Human Resources. The Panel also gratefully acknowledges the unrestricted educational
grants provided for this endeavor by the AAN Foundation, Janssen Pharmaceutica, the SK Corporation, Abbott Laboratories, Novartis, and Athena
Neurosciences, Inc.
The authors and coauthors have read and agree with the content of this publication and acknowledge their compliance with the “Disclosure” requirements of
Neurology. There is no pertinent financial interest of any author (i.e., ownership, equity position, stock options, patent-licensing arrangements), consulting
fees, or honoraria associated with this publication or its products.
Approved by the AAN Quality Standards Subcommittee on April 1, 2000. Approved by the AAN Practice Committee on May 3, 2000. Approved by the AAN
Board of Directors on June 9, 2000.
Address correspondence and reprint requests to QSS, American Academy of Neurology, 1080 Montreal Avenue, St. Paul, MN 55116; phone: 1-800-879-1960.
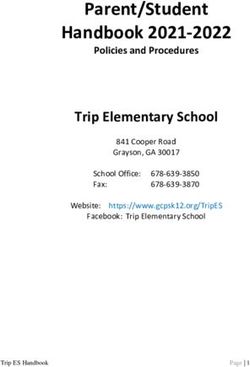
468 Copyright © 2000 by AAN Enterprises, Inc.Figure. Practice parameter algorithm.
Autism, autistic spectrum, and pervasive develop- half of the families reported that the school system and
mental disorders encompass a wide continuum of as- other parents were the major source of assistance over
sociated cognitive and neurobehavioral disorders, time, rather than the medical health care community.
including the core-defining features of impaired so- The diagnosis of autism often is not made until 2 to 3
cialization, impaired verbal and nonverbal communi- years after symptoms are recognized, primarily because
cation, and restricted and repetitive patterns of of concerns about labeling or incorrectly diagnosing the
behavior (table).1 Between 60,000 and 115,000 chil- child. Identifying children with autism and initiating in-
dren under 15 years of age in the United States meet tensive, early intervention during the preschool years re-
diagnostic criteria for autism based on recent preva- sults in improved outcomes for most young children with
lence estimates of 10 to 20 cases per 10,000 people. autism.3-7 Early diagnosis of autism and early interven-
In 1,300 families recently surveyed, the average age tion facilitates earlier educational planning, provisions for
at diagnosis of autism was about 6 years, despite the family supports and education, management of family
fact that most parents felt something was wrong by stress and anguish, and delivery of appropriate medical
18 months of age and usually sought medical assis- care and treatment.3-7
tance by age 2 years.2 Fewer than 10% of the chil- Clinically identifying children with autism re-
dren were diagnosed at initial presentation; another quires two levels of investigation, each addressing a
10% were either told to return if their worries per- distinct component of patient management (figure).1
sisted, or that their child “would grow out of it.” The The first level, Routine Developmental Surveillance
rest were referred to another professional (at a mean and Screening Specifically for Autism, should be per-
age of 40 months), of which only 40% were given a formed on all children and involves first identifying
formal diagnosis, 25% were told “not to worry,” and those at risk for any type of atypical development,
25% were referred to a third or fourth professional. followed by identifying those specifically at risk for
Almost 20% reported that they either had to exert autism. Mental retardation or other medical or neu-
considerable pressure to obtain the referrals or pay rodevelopmental conditions require separate evalua-
privately. Over 30% of parents referred to subse- tions and are not within the scope of this document.
quent professionals reported that no help was offered The second level, Diagnosis and Evaluation of Au-
(e.g., with education, therapy, or referrals to parent tism, involves a more in-depth investigation of already
support groups), and only about 10% reported that a identified children and differentiates autism from
professional explained their child’s problems. Almost other developmental disorders. In-depth diagnosis and
August (2 of 2) 2000 NEUROLOGY 55 469Table Diagnostic Criteria for 299.00 Autistic Disorder vestigation, specific clinical questions were defined (see
A. A total of six (or more) items from (1), (2), and (3), with two
Appendix 2), clinical evidence was summarized, and
from (1), and at least one each from (2) and (3): diagnostic recommendations were developed.
Evidence and recommendations are presented in
1. Qualitative impairment in social interaction, manifest by at
least two of the following:
three sections. The first two sections, Level One:
Routine Developmental Surveillance and Screening
• Marked impairment in the use of multiple nonverbal
Specifically for Autism, and Level Two: Diagnosis
behaviors, such as eye-to-eye gaze, facial expression, body
postures, and gestures, to regulate social interaction and Evaluation of Autism, first present the empiric
data for each question and are followed by recom-
• Failure to develop peer relationships appropriate to
developmental level
mendations linked to the specific evidence. Each is
followed by a section on Recommendations for Re-
• Lack of spontaneous seeking to share enjoyment,
search. The third section, Consensus-Based General
interests, or achievements with other people (e.g., by lack
of showing, bringing, or pointing out objects of interest)
Principles of Management, presents additional rec-
ommendations based on broad consensus. Additional
• Lack of social or emotional reciprocity
information about autism, including behavioral as-
2. Qualitative impairment in communication, as manifest by pects associated with the core defining deficits,
at least one of the following: methodology, and clinical evidence are described in
• Delay in, or total lack of, the development of spoken the background paper.1 Specific information about the
language (not accompanied by an attempt to compensate recommended developmental screening and diagnostic
through alternative modes of communication such as
tools can be found at http://www.aan.com under AAN
gesture or mime)
Resources: Practice Statements: Official AAN Practice
• In individuals with adequate speech, marked impairment in Statements: Autism, Screening and diagnosis of.
the ability to initiate or sustain a conversation with others
• Stereotyped and repetitive use of language, or Description of the process. Experts in the sur-
idiosyncratic language
veillance/screening and diagnosis of autism were se-
• Lack of varied, spontaneous make-believe, or social lected by 11 professional organizations (see
imitative play appropriate to developmental level Appendix 1) and convened in June 1998 and January
3. Restrictive repetitive and stereotypic patterns of behavior, 1999. They reviewed and evaluated the quality of the
interests, and activities, as manifested by at least one of the evidence from the published literature, developed a
following: consensus of evidence-based management recom-
• Encompassing preoccupation with one or more stereotyped mendations, and published a comprehensive back-
and restricted patterns of interest that is abnormal either ground paper on the surveillance, screening, and
in intensity or focus
diagnosis of autism.1 Evidence reviewed for this pa-
• Apparently inflexible adherence to specific nonfunctional rameter was identified through literature searches
routines or rituals using MEDLINE and PsychINFO. Relevant articles
• Stereotyped and repetitive motor mannerisms (e.g., hand were included from all languages using the following
or finger flapping or twisting, or complex whole-body search terms: autistic; OR autism; OR pervasive, and
movements) NOT treatment. This search produced over 4,000 ci-
• Persistent preoccupation with parts of objects. tations, from which 2,750 studies met the following
B. Delays or abnormal functioning in at least one of the inclusion criteria: clinical papers published since
following areas, with onset prior to age 3 years: 1990; review papers and meta-analyses developed for
1. Social interaction DSM-IV; and the overview of the National Institutes
2. Language as used in social communication
of Health State of the Science Conference on Autism
in 1995. Relevant book chapters and books were also
3. Symbolic or imaginative play
included, as identified by the expert panel.
C. The disturbance is not better accounted for by Rett’s disorder The strength of the evidence for each relevant ar-
or childhood disintegrative disorder. ticle and book chapter was ranked using the defined
The other pervasive developmental disorders include criteria shown in Appendix 3. Recommendations
Asperger’s disorder, Rett syndrome, childhood disintegrative were thereby derived based on the strength of the
disorder, pervasive developmental disorder—not otherwise evidence and stratified (Standard, Guideline, or
specified (PDD-NOS), or atypical autism.
Practice Option) as defined in Appendix 3.
Reprinted with permission from the Diagnostic and Statistical
Manual of Mental Disorders, 4th edition. Washington, DC:
Level one: routine developmental surveillance
American Psychiatric Association, 1994:70 –71.
and screening specifically for autism. Analysis
Detailed information on other PDD diagnoses can be found in the of the evidence. When and how often should devel-
comprehensive background paper.1 opmental surveillance/screening be performed? Ap-
proximately 25% of children in any primary care
practice show developmental issues. However, fewer
evaluation are important in determining optimal inter- than 30% of primary care providers conduct standard-
ventional strategies based on the child’s profile of ized screening tests at well-child appointments.8-10 The
strengths and weaknesses. For these two areas of in- American Academy of Pediatrics (AAP) stresses the
470 NEUROLOGY 55 August (2 of 2) 2000importance of a flexible, continual developmental age. Retrospective analysis of home videotapes have
surveillance process at each well-child visit, and rec- also identified behaviors that distinguish infants
ommends eliciting and valuing parental concerns, with autism from other developmental disabilities as
probing regarding age-appropriate skills in each de- early as 8 months of age.28-30
velopmental domain, and observing each child.11 Current screening methods may not identify chil-
What are the appropriate developmental screen- dren with milder variants of autism, those without
ing questionnaires that provide sensitive and specific mental retardation or language delay, such as verbal
information? Developmental screening tools have individuals with high-functioning autism and As-
been formulated based on screening of large popu- perger’s disorder, or older children, adolescents, and
lations of children with standardized test items. Sensitive young adults.
and specific developmental screening instruments in- Is there an increased risk of having another child
clude: the Ages and Stages Questionnaire, the BRIG- with autism (recurrence)? The incidence of autism
ANCE威 Screens, the Child Development Inventories, and in the general population is 0.2%, but the risk of
the Parents’ Evaluations of Developmental Status.1 having a second (or additional) autistic child increases
The Denver-II (DDST-II, formerly the Denver De- almost 50-fold to approximately 10 to 20%.31-34
velopmental Screening Test-Revised) has been the What tools are available with appropriate psycho-
traditional tool used for developmental screening, metric properties to specifically screen for autism?
but research has found that it is insensitive and Appropriately sensitive and specific autism screen-
lacks specificity. The Revised Denver Pre-Screening ing tools for infants and toddlers have only recently
Developmental Questionnaire (R-DPDQ) was de- been developed, and this continues to be the current
signed to identify a subset of children who needed focus of many research centers. The Checklist for
further screening. However, studies have shown that Autism in Toddlers (CHAT) for 18-month-old infants,
it detected only 30% of children with language im- and the Autism Screening Questionnaire for children
pairments and 50% of children with mental 4 years of age and older, have been validated on
retardation.12-15 large populations of children. However, it should be
How are conventional developmental milestones noted that the CHAT is less sensitive to milder
defined? Conventional developmental language symptoms of autism, as children later diagnosed
milestones are based on normative data from numer- with PDD-NOS, Asperger’s, or atypical autism did
ous standardized language instruments for infants.16-19 not routinely fail the CHAT at 18 months.27,35
Lack of acquisition of the following milestones within The Pervasive Developmental Disorders Screen-
known accepted and established ranges is considered ing Test–II (PDDST-II) for infants from birth to 3
abnormal: no babbling by 12 months; no gesturing years of age, the Modified Checklist for Autism in
(e.g., pointing, waving bye-bye) by 12 months; no Toddlers (M-CHAT) for infants at 2 years of age, and
single words by 16 months; no 2-word spontaneous the Australian Scale for Asperger’s Syndrome for
(not just echolalic) phrases by 24 months; and any older verbal children, are currently under develop-
loss of any language or social skills at any age. Fail- ment or validation phases.1
ure to meet these milestones is associated with a What screening laboratory investigations are
high probability of a developmental disability. available for developmental delay, with or without sus-
Do parents provide reliable information regarding picion of autism? Formal audiologic evaluation. The
their child’s development? Several studies encom- Committee on Infant Hearing of the American Speech–
passing 737 children showed that parental concerns Language–Hearing Association developed guidelines
about speech and language development, behavior, for the audiologic assessment of children from birth
or other developmental issues were highly sensitive through 36 months of age.36 They recommended that
(i.e., 75% to 83%) and specific (79% to 81%) in detect- all children with developmental delays, particularly
ing global developmental deficits.20-22 However, the those with delays in social and language development,
absence of such concerns had modest specificity in have a formal audiologic hearing evaluation. Three
detecting normal development (47%).20 An additional studies have documented that conductive, sensorineu-
study that combined parental concern with a stan- ral, or mixed hearing loss can co-occur with autism,
dardized parental report found this to be effective for and that some children with autism may be incorrectly
early behavioral and developmental screening in the thought to have peripheral hearing loss.37,38 In addi-
primary care setting.23 tion, transient conductive hearing loss associated with
Can autism be reliably diagnosed before 36 otitis media with effusion can also occur in children
months of age? Because there are no biological with autism.
markers for autism, screening must focus on behav- Audiologic assessment of such children requires
ior. Recent studies comparing 109 autistic and 33 modifications of traditional test techniques and envi-
typically developing children demonstrated that ronments (e.g., operant test procedures).39,40 Electro-
problems with eye contact, orienting to one’s name, physiologic procedures are useful for estimating
joint attention, pretend play, imitation, nonverbal hearing sensitivity and for examining middle ear,
communication, and language development are mea- cochlear, and VIIIth nerve or auditory brainstem
surable by 18 months of age.24-27 These symptoms are pathway integrity.41,42 Evoked otoacoustic emissions
stable in children from toddler age through preschool are useful for examining cochlear (sensory) function,
August (2 of 2) 2000 NEUROLOGY 55 471and is a frequency-specific, as well as a time- and cation, and play skills, and the occurrence of
cost-efficient procedure.43 Frequency-specific audi- maladaptive behaviors. Screening should be per-
tory brainstem response (ABR) is the single most formed not only for autism-related symptoms but
useful electrophysiologic procedure for use in esti- also for language delays, learning difficulties, so-
mating hearing thresholds, and has been demon- cial problems, and anxiety or depressive symp-
strated to be highly correlated with behavioral toms (Guideline).
hearing thresholds in children who hear normally 6. Screening specifically for autism should be per-
and in children who have sensorineural hearing formed on all children failing routine developmen-
loss.42 tal surveillance procedures using one of the
Lead screening. Children with developmental de- validated instruments—the CHAT or the Autism
lays who spend an extended period in the oral–motor Screening Questionnaire (Guideline).
stage of play (where everything “goes into their 7. Laboratory investigations recommended for any
mouths”) are at increased risk for lead toxicity, espe- child with developmental delay and/or autism in-
cially in certain environments. The prevalence of clude audiologic assessment and lead screening
pica in this group can result in high rates of substan- (Guideline). Early referral for a formal audio-
tial or recurrent exposure to lead. The National Cen- logic assessment should include behavioral audio-
ter for Environmental Health of the Centers for metric measures, assessment of middle ear
Disease Control and Prevention recommends that function, and electrophysiologic procedures using
children with developmental delays, even without experienced pediatric audiologists with current
frank pica, should be screened for lead poisoning.44 audiologic testing methods and technologies
Blood lead levels in children with autism are elevat- (Guideline). Lead screening should be performed
ed.1 In one study, the mean blood lead level in 18 in any child with developmental delay and pica.
autistic children was higher than in 16 nonautistic Additional periodic screening should be consid-
“psychotic” children or in 10 normal siblings; 44% of ered if the pica persists (Guideline).
the autistic and psychotic children had lead levels
Recommendations for research.
significantly above the mean compared with control
subjects.45 In a more recent study, 17 autistic chil- 1. Develop and validate appropriate autism screen-
dren treated for lead poisoning were compared with ing tools with adequate sensitivity and specificity
30 children without autism. The autistic children in children younger than 1 year of age that could
were older at diagnosis, had higher lead levels, and be used by a wide range of practitioners.
most were reexposed despite close monitoring of 2. Current methods of screening for autism may not
their environment.46 identify: 1) children with milder variants of the
disorder; 2) children without mental retardation
Level one evidence-based recommendations. or language delay, such as verbal individuals with
Clinical practice recommendations. high functioning autism and Asperger’s disorder;
or 3) older children, adolescents, and young
1. Developmental surveillance should be performed adults. Additional tools are needed to help iden-
at all well-child visits from infancy through tify and evaluate these groups of patients.
school-age, and at any age thereafter if concerns 3. Studies are needed to provide insight into the
are raised about social acceptance, learning, or emergence of early auditory behaviors that are
behavior (Guideline). considered atypical and may be prevalent in chil-
2. Recommended developmental screening tools in- dren with autism. Studies are also needed on the
clude the Ages and Stages Questionnaire, the audiologic characteristics of individuals with au-
BRIGANCE威 Screens, the Child Development In- tism to help assess peripheral hearing sensitivity
ventories, and the Parents’ Evaluations of Devel- and suprathreshold responses.
opmental Status (Guideline).
3. Because of the lack of sensitivity and specificity, the Level two: diagnosis and evaluation of autism.
Denver-II (DDST-II) and the Revised Denver Pre- Analysis of the evidence. Who should diagnose au-
Screening Developmental Questionnaire (R-DPDQ) tism? Although educators, parents, and other
are not recommended for appropriate primary-care health care professionals identify signs and symp-
developmental surveillance (Guideline). toms characteristic of autism, a clinician experienced
4. Further developmental evaluation is required in the diagnosis and treatment of autism is usually
whenever a child fails to meet any of the following necessary for accurate and appropriate diagno-
milestones (Guideline): babbling by 12 months; sis.25,47,48 Clinicians must rely on their clinical judg-
gesturing (e.g., pointing, waving bye-bye) by 12 ment, aided by guides to diagnosis, such as DSM-IV
months; single words by 16 months; two-word and the Tenth Edition of the International Classifica-
spontaneous (not just echolalic) phrases by 24 tion of Diseases (ICD-10), as well as by the results of
months; loss of any language or social skills at various assessment instruments, rating scales, and
any age. checklists. These instruments and criteria should be
5. Siblings of children with autism should be care- used by practitioners not as experienced in the diag-
fully monitored for acquisition of social, communi- nosis of autism.
472 NEUROLOGY 55 August (2 of 2) 2000What are the medical and neurologic concerns in the lowest. However, the PIQ–VIQ split is severity
evaluating children with autism? Familial preva- dependent. When Full Scale IQ (FSIQ) and VIQ are
lence. Family studies have shown that there is a both above 70, 80% of autistic individuals will have
50-fold to 100-fold increase in the rate of autism in no significant VIQ–PIQ disparity, and the remainder
first-degree relatives of autistic children. Within are evenly divided between those with PIQ ⬎ VIQ
these families, there are also elevated rates of social and those with PIQ ⬍ VIQ.76
difficulties; higher incidences of cognitive, communi- The DSM-IV defines the diagnosis of mental retar-
cation, learning and executive function deficits; in- dation as the combination of subaverage intellectual
creased stereotyped behaviors; and anxiety, affective, functioning (IQ ⬍ 70) and concurrent deficits in
language, and pragmatic disorders.33,49-55 Monozygotic adaptive functioning. Autistic individuals have
twin pair studies have also shown a high concordance poorer adaptive function than would be predicted by
rate (60%) for DSM-IV Autistic Disorder, 71% for the IQ alone.77
broader autistic spectrum phenotype, and 92% for an Sensorimotor deficits. Impairments of gross and
even broader phenotype of social and communication fine motor function are reported as being common in
deficits with stereotyped behaviors that nonetheless autistic individuals, and are recognized as hypoto-
were clearly differentiated from normal. In contrast, nia, limb apraxia, or motor stereotypies. Motor defi-
no concordance for autism was noted in dizygotic cits are more severe in individuals with lower IQ
twin pairs and only 10% were concordant for some scores.78 Hand or finger mannerisms, body rocking,
form of cognitive, social or language deficit.56,57 or unusual posturing are reported in 37% to 95% of
Large head circumference without frank neuropa- individuals, and often manifest during the preschool
thology. Children with autism have a larger head years.24,58,78 Sensory processing abilities are aberrant
circumference; only a small proportion have frank in 42% to 88% of autistic individuals and include
macrocephaly.33,57-61 Large head size may not neces- preoccupation with sensory features of objects, over-
sarily be present at birth, but may appear in early to or underresponsiveness to environmental stimuli, or
mid-childhood, perhaps indicating an increased rate paradoxical responses to sensory stimuli.79
of brain growth. Neuroimaging studies in autism Neuropsychological, behavioral, and academic im-
also found larger brain volumes without associated pairments. Specific neuropsychological impair-
neuropathology.62,63 ments can be identified, even in young children with
Association with tuberous sclerosis complex (TSC) autism, that correlate with the severity of autistic
and less often with Fragile X (FraX) syndrome. Sev- symptoms.80 Performance on tasks that rely on rote,
enteen to over 60% of mentally retarded individuals mechanical, or perceptual processes are typically
with TSC are also autistic, and these patients com- spared; deficient performance exists on tasks requir-
monly have epilepsy.64-67 In contrast, the number of ing higher-order conceptual processes, reasoning, in-
autistic individuals with TSC has been estimated to terpretation, integration, or abstraction. Dissociations
be between 0.4% and 3%.66 This rate increases to 8% between simple and complex processing are reported in
to 14% if epilepsy is also present.66 the areas of language, memory, executive function, mo-
Clinical studies report that 3% to 25% of patients tor function, reading, mathematics, and perspective-
with FraX have autism.68-70 However, no evidence of taking.80-83 There is no reported evidence that confirms
FraX in autistic individuals was found using cytoge- or excludes a diagnosis of autism based on these cogni-
netic (not DNA analysis) techniques;71 with molecu- tive patterns alone.
lar genetic analyses, only a few autistic individuals When and what laboratory investigations are indi-
were shown to have FraX.72 cated for the diagnosis of autism? Genetic testing. A
What are the specific deficits of the autistic child’s chromosomal abnormality reported in possibly more
developmental profile? Speech, language, and ver- than 1% of autistic individuals involves the proximal
bal and nonverbal communication. Verbal and non- long arm of chromosome 15 (15q11-q13), which is a
verbal communication deficits seen in autism are far greater frequency than other currently identifiable
more complex than simple speech delay, but overlap chromosomal disorders.84-86 Those with the 15q ab-
with developmental language disorders or specific normalities typically have moderate to profound
language impairments. Expressive language func- mental retardation. The duplication is usually ma-
tion ranges from complete mutism (as often seen in ternally inherited, either pseudodicentric 15 (inverted
children 2 to 3 years of age) to verbal fluency, though duplication 15) or other atypical marker chromosomes,
verbal abilities are often accompanied by many er- with one or two extra copies of the area roughly corre-
rors in word meaning (semantics) or language and sponding to the typical Angelman syndrome (AS)/
communicative deficits in social contexts (social- Prader Willi Syndrome (PWS) deletion region of
pragmatics).73-75 approximately four million base pairs. Conversely, AS
Cognitive deficits. Many autistic individuals is usually due to a deletion of maternally inherited
demonstrate a particular pattern on intellectual 15q11-q13 material and has been found in patients
tests that is characteristic of autism, i.e., perfor- with autism and profound mental retardation.85,87
mance IQ (PIQ) higher than verbal IQ (VIQ), and Metabolic testing. Inborn errors in amino acid,
specific intersubtest scatter, with Block Design typi- carbohydrate, purine, peptide, and mitochondrial
cally the highest subtest and Comprehension usually metabolism, as well as toxicologic studies have been
August (2 of 2) 2000 NEUROLOGY 55 473studied, but the percentage of children with autism trace elements, celiac antibodies, allergy testing who have a metabolic disorder is probably less (and (particularly food allergies for gluten, casein, can- some experts agree that it is considerably less) than dida, and other molds), immunologic or neurochemi- 5%.88,89 cal abnormalities, micronutrients such as vitamin Electrophysiologic testing. The prevalence of epi- levels, intestinal permeability studies, stool analysis, lepsy in autistic children has been estimated at 790 to urinary peptides, mitochondrial disorders (including 14%,91 whereas the cumulative prevalence by adult- lactate and pyruvate), thyroid function tests, or hood is estimated at 20% to 35%.90,91 Seizure onset erythrocyte glutathione peroxidase studies.1 peaks in early childhood and again in adolescence. Mental retardation, with or without motor abnor- Level two: evidence-based recommendations. malities and family history of epilepsy, was a signif- Clinical practice recommendations. icant risk factor for the development of seizures in 1. Genetic testing in children with autism, specifi- autistic individuals.92-95 cally high resolution chromosome studies (karyo- It is unclear whether there is a relationship be- type) and DNA analysis for FraX, should be tween autism and an early regressive course (before performed in the presence of mental retardation 36 months), childhood disintegrative disorder ([CDD] (or if mental retardation cannot be excluded), if after 36 months), Landau–Kleffner syndrome, and there is a family history of FraX or undiagnosed electrical status epilepticus during slow wave sleep mental retardation, or if dysmorphic features are (ESES). Autism with regression and CDD have both present (Standard). However, there is little like- been associated with seizures or epileptiform sleep- lihood of positive karyotype or FraX testing in the deprived EEG (with adequate sampling of slow wave presence of high-functioning autism. sleep).96-98 A higher incidence of epileptiform EEG 2. Selective metabolic testing (Standard) should be abnormalities in autistic children with a history of initiated by the presence of suggestive clinical and regression has been reported when compared to au- physical findings such as the following: if leth- tistic children with clinical epilepsy.97 Seizures or argy, cyclic vomiting, or early seizures are evi- epileptiform discharges were more prevalent in chil- dent; the presence of dysmorphic or coarse dren with regression who demonstrated cognitive features; evidence of mental retardation or if men- deficits. Regression in cognition and language in ad- tal retardation cannot be ruled out; or if occur- olescence associated with seizure onset has also been rence or adequacy of newborn screening for a observed, but little is known about its cause or prev- birth is questionable. alence. There may be a causal relationship between 3. There is inadequate evidence at the present time a subgroup of children with autistic regression and to recommend an EEG study in all individuals EEG-defined “benign focal epilepsies.”99 There is in- with autism. Indications for an adequate sleep- sufficient evidence to suggest a role for event-related deprived EEG with appropriate sampling of slow potentials or magnetoencephalography in the evalu- wave sleep include (Guideline) clinical seizures ation of autism. or suspicion of subclinical seizures, and a history Neuroimaging. CT studies, ordered as standard of regression (clinically significant loss of social assessments of children diagnosed with autism during and communicative function) at any age, but espe- the 1970s and 1980s, reported a wide range of brain cially in toddlers and preschoolers. imaging abnormalities and suggested that there was 4. Recording of event-related potentials and magne- an underlying structural disorder in patients with au- toencephalography are research tools at the tism. This view changed when Damasio et al.100 demon- present time, without evidence of routine clinical strated that such abnormalities were incidental to utility (Guideline). coexisting anatomic disorders unrelated to autism. A 5. There is no clinical evidence to support the role of very low prevalence of focal lesions or other structural routine clinical neuroimaging in the diagnostic abnormalities was found; their inconsistent localization evaluation of autism, even in the presence of marked them as coincidental. Prevalence of lesions on megalencephaly (Guideline). MRI in children with autism is similar to normal con- 6. There is inadequate supporting evidence for hair trol subjects.101 CT and MRI studies of autistic subjects analysis, celiac antibodies, allergy testing (partic- screened to exclude those with disorders other than ularly food allergies for gluten, casein, candida, autism confirmed the absence of significant structural and other molds), immunologic or neurochemical brain abnormalities.63 abnormalities, micronutrients such as vitamin Functional imaging modalities such as functional levels, intestinal permeability studies, stool anal- MRI (fMRI), single-photon emission CT (SPECT), or ysis, urinary peptides, mitochondrial disorders positron-emission tomography (PET) are currently (including lactate and pyruvate), thyroid function only research tools in the evaluation of autism. tests, or erythrocyte glutathione peroxidase stud- There is no evidence to support a role for functional ies (Guideline). neuroimaging studies in the clinical diagnosis of au- tism at the present time.1 Recommendations for research. Other tests. There is insufficient evidence to sup- 1. Studies are needed to further identify the useful- port the use of other tests such as hair analysis for ness of electrophysiologic techniques to clarify the 474 NEUROLOGY 55 August (2 of 2) 2000
role of epilepsy in autism, especially in children neurocutaneous abnormalities (requiring an ultravi-
with a history of regression. olet [Wood’s] lamp examination); gait; tone; reflexes;
2. Additional studies to examine potential genetic cranial nerves; and determination of mental status,
and/or environmental factors and their relation- including verbal and nonverbal language and play.
ship to the etiology of autism are needed. Evaluation and monitoring of autism. The im-
3. Continuing efforts might focus on identifying con- mediate and long-term evaluation and monitoring of
tributing genes to determine whether the behav- autistic individuals requires a comprehensive multi-
ioral syndromes (which constitute the basis of disciplinary approach, and can include one or more
DSM-IV and ICD-10) have actual biological validity. of the following professionals: psychologists, neurolo-
4. Evaluation of environmental factors (e.g., nonspe- gists, speech–language pathologists and audiologists,
cific infections or other immunologically mediated pediatricians, child psychiatrists, occupational thera-
events) that might contribute to triggering the pists, and physical therapists, as well as educators
expression of autistic symptoms or regression re- and special educators. Individuals with mild autism
quires additional study. should also receive adequate assessments and appro-
priate diagnoses.
Consensus-based general principles of manage- Reevaluation within 1 year of initial diagnosis and
ment. The following recommendations are based on continued monitoring is an expected aspect of clini-
consensus agreement by the participating organiza- cal practice because relatively small changes in the
tions involved in the development of this parameter.1 developmental level affect the impact of autism in
Surveillance and screening. In the United the preschool years. In general, there is no need to
States, states must follow federal Public Law 105-17: repeat extensive diagnostic testing; however,
the Individuals with Disabilities Education Act follow-up visits can be helpful to address behavioral,
Amendments of 1997–IDEA’97, which mandates im- environmental, and other developmental concerns.
mediate referral for a free appropriate public educa- Speech, language, and communication evaluation.
tion for eligible children with disabilities from the A comprehensive speech–language– communication
age of 36 months, and early intervention services for evaluation should be performed on all children who
infants and toddlers with disabilities from birth fail language developmental screening procedures by
through 35 months of age. a speech–language pathologist with training and ex-
Diagnosis. The diagnosis of autism should in- pertise in evaluating children with developmental
clude the use of a diagnostic instrument with at least disabilities. Comprehensive assessments of both pre-
moderate sensitivity and good specificity for autism. verbal and verbal individuals should account for age,
Sufficient time should be planned for standardized cognitive level, and socioemotional abilities, and
parent interviews regarding current concerns and should include assessment of receptive language and
behavioral history related to autism, and direct, struc- communication, expressive language and communi-
tured observation of social and communicative behav- cation, voice and speech production, and in verbal
ior and play. Recommended instruments include1: individuals, a collection and analysis of spontaneous
Diagnostic parental interviews language samples to supplement scores on formal
language tests.
The Gilliam Autism Rating Scale
Cognitive and adaptive behavior evaluations. Cog-
The Parent Interview for Autism nitive evaluations should be performed in all chil-
The Pervasive Developmental Disorders Screening dren with autism by a psychologist or other trained
Test–Stage 3 professional. Cognitive instruments should be appro-
The Autism Diagnostic Interview–Revised priate for the mental and chronologic age, provide a
full range (in the lower direction) of standard scores
Diagnostic observation instruments and current norms independent of social ability, in-
The Childhood Autism Rating Scale clude independent measures of verbal and nonverbal
The Screening Tool for Autism in Two-Year-Olds abilities, and provide an overall index of ability. A
measure of adaptive functioning should be collected
The Autism Diagnostic Observation Schedule-
for any child evaluated for an associated cognitive
Generic
handicap. Consensus-based recommendations for us-
Medical and neurologic evaluation. Perinatal ing specific instruments include the Vineland Adap-
and developmental history should include mile- tive Behavior Scales and the Scales of Independent
stones; regression in early childhood or later in life; Behavior–Revised.1
encephalopathic events; attentional deficits; seizure Sensorimotor and occupational therapy evalu-
disorder (absence or generalized); depression or ma- ations. Evaluation of sensorimotor skills by a qual-
nia; and behaviors such as irritability, self-injury, ified experienced professional (occupational therapist
sleep and eating disturbances, and pica. The physi- or physical therapist) should be considered, includ-
cal and neurologic examination should include: longi- ing assessment of gross and fine motor skills, praxis,
tudinal measurements of head circumference and sensory processing abilities, unusual or stereotyped
examination for unusual features (facial, limb, stat- mannerisms, and the impact of these components on
ure, etc.) suggesting the need for genetic evaluation; the autistic person’s life. An occupational therapy
August (2 of 2) 2000 NEUROLOGY 55 475evaluation is indicated when deficits exist in func- Donald J. Siegel, PhD, and the assistance of Cheryl Jess, Jody
Sallah, and Starr Pearlman, PhD, in this endeavor. Special grati-
tional skills or occupational performance in the areas tude is extended for the additional assistance of Michael L. Gold-
of play or leisure, self-maintenance through activi- stein, MD, and Roy Elterman, MD.
ties of daily living, or productive school and work
tasks. Although not routinely warranted as part of Appendix 1
all evaluations of children with autism, the Sensory Participating Organizations and Authors
Integration and Praxis Tests may be used on an in- Pauline A. Filipek, MD—Chair (Child Neurology Society,
dividual basis to detect specific patterns of sensory American Academy of Neurology and American Academy of Pedi-
atrics); Judith S. Gravel, PhD (American Academy of Audiology);
integrative dysfunction. Edwin H. Cook, Jr., MD, and Fred R. Volkmar, MD (American
Neuropsychological, behavioral, and academic as- Academy of Child and Adolescent Psychiatry); Isabelle Rapin,
sessments. These assessments should be performed MD, and Barry Gordon, MD, PhD (American Academy of Neurol-
ogy); Stuart W. Teplin, MD, Ronald J. Kallen, MD, and Chris
as needed, in addition to the cognitive assessment, to Plauche Johnson, MEd, MD (American Academy of Pediatrics);
include social skills and relationships, educational Grace T. Baranek, PhD, OTR/L (American Occupational Therapy
functioning, problematic behaviors, learning style, Association); Sally J. Rogers, PhD, Sally Ozonoff, PhD, and Wendy
motivation and reinforcement, sensory functioning, L. Stone, PhD (American Psychological Association); Geraldine
Dawson, PhD (American Psychological Society); Barry M. Prizant,
and self-regulation. Assessment of family resources PhD, CCC-SLP (American Speech–Language–Hearing Associa-
should be performed by appropriate psychologists or tion); Nancy J. Minshew, MD, and Roberto F. Tuchman, MD
other qualified health care professionals and should (Child Neurology Society); Susan E. Levy, MD (Society for Devel-
include assessment of parents’ level of understand- opmental and Behavioral Pediatrics); Pasquale J. Accardo, MD
(Society for Developmental Pediatrics); and Stephen Ashwal, MD
ing of their child’s condition, family (parent and sib- (Child Neurology Society, American Academy of Neurology Qual-
ling) strengths, talents, stressors and adaptation, ity Standards Subcommittee).
resources and supports, as well as offer appropriate Representatives were named from the following associations:
Barbara Cutler, EdD, and Susan Goodman, JD (Autism National
counseling and education. Committee); Cheryl Trepagnier, PhD (Autism Society of America);
Daniel H. Geschwind, MD, PhD (Cure Autism Now); and Charles
Disclaimer. The Quality Standards Subcommittee T. Gordon, MD (National Alliance for Autism Research). The Na-
tional Institutes of Health also named liaisons to serve on this
(QSS) of the American Academy of Neurology (AAN) committee, including Marie Bristol–Power, PhD (National Insti-
seeks to develop scientifically sound, clinically rele- tute of Child Health and Human Development); Judith Cooper,
vant practice parameters for the practice of neurol- PhD (National Institute of Deafness and Communication Disor-
ogy. Practice parameters are strategies for patient ders); Judith Rumsey, PhD (National Institute of Mental Health);
and Giovanna Spinella, MD (National Institute of Neurological
management that assist physicians in clinical deci- Disorders and Stroke).
sion making. A practice parameter is one or more
specific recommendations based on analysis of evi- Appendix 2
dence of a specific clinical problem. These might in- Clinical questions addressed for surveillance, screening
clude diagnosis, symptoms, treatment, or procedure and diagnosing children with autism
evaluation. This evidence-based review addresses Routine developmental surveillance and screening for autism
the major management issues health care providers 1. When and how often should developmental surveillance/screen-
face in surveying, screening, and diagnosing children ing be performed?
with autism. The clinical evidence is reviewed, man- 2. What are the appropriate developmental screening question-
naires that provide sensitive and specific information?
agement recommendations provided, and areas of 3. How are conventional developmental milestones defined?
continued research identified. This statement is pro- 4. Do parents provide reliable information regarding their child’s
vided as an educational service of the American development?
5. Can autism can be reliably diagnosed before 36 months of age?
Academy of Neurology. It is based on an assessment 6. Is there an increased risk of having another child with autism
of current scientific and clinical information. It is not (recurrence)?
intended to include all possible proper methods of 7. What screening laboratory investigations are available for de-
care for choosing to use a specific procedure. Neither velopmental delay, with or without suspicion of autism?
8. What tools are available with appropriate psychometric proper-
is it intended to exclude any reasonable alternative ties to specifically screen for autism?
methodologies. The AAN recognizes that specific pa- Diagnosis and evaluation of autism
tient care decisions are the prerogative of the patient
and the physician caring for the patient, based on all 1. Who should diagnose autism?
2. What are the medical and neurologic concerns in evaluating
of the circumstances involved. children with autism?
3. What are the specific deficits of the autistic child’s developmen-
Acknowledgment tal profile?
4. When and what laboratory investigations are indicated for the
The authors thank the following people who contributed to this diagnosis of autism?
endeavor by their participation in the NIH State of the Science in
Autism: Screening and Diagnosis Working Conference, June 15 to
17, 1998: George Anderson, PhD, Anthony Bailey, MD, W. Ted Appendix 3
Brown, MD, Susan E. Bryson, PhD, Rebecca Landa, PhD, Jeffrey Definitions for strength of the evidence
Lewine, PhD, Catherine Lord, PhD, William McIlvane, PhD, Jo- Class I. Must have all of a through d. a) Prospective study of a
seph Piven, MD, Ricki Robinson, MD, Bryna Siegel, PhD, Vijendra well-defined cohort which includes a description of the nature of
K. Singh, PhD, Frank Symons, PhD, and Max Wiznitzer, MD. The the population, the inclusion/exclusion criteria, demographic char-
current authors, participants and NIH Liaisons also participated acteristics such as age and sex, and seizure type. b) The sample
in this working conference. The Panel acknowledges with grati- size must be adequate with enough statistical power to justify a
tude the valuable consultations of Frances P. Glascoe, PhD, and conclusion or for identification of subgroups for whom testing does
476 NEUROLOGY 55 August (2 of 2) 2000or does not yield significant information. c) The interpretation of 13. Greer S, Bauchner H, Zuckerman B. The Denver Develop-
evaluations performed must be done blinded to outcome. d) There mental Screening Test: how good is its predictive validity?
must be a satisfactory description of the technology used for eval- Dev Med Child Neurol 1989;31:774 –781. (Class II).
uations (e.g., EEG, MRI). 14. Diamond KE. Predicting school problems from preschool de-
Class II. Must have a or b. a) Retrospective study of a well- velopmental screening: A four-year followup of the Revised
defined cohort which otherwise meets criteria for class 1a, b and Denver Developmental Screening test and the role of parent
1d. b) Prospective or retrospective study which lacks any of the report. J Div Early Child 1987;11:247–253. (Class I).
following: adequate sample size, adequate methodology, a descrip- 15. Sciarillo WG, Brown MM, Robinson NM, Bennett FC, Sells
tion of inclusion/exclusion criteria, and information such as age, CJ. Effectiveness of the Denver Developmental Screening
sex and characteristics of the seizure. Test with biologically vulnerable infants. J Dev Behav Pedi-
Class III. Must have a or b. a) A small cohort or case report. b) atr 1986;7:77– 83. (Class I).
Relevant expert opinion, consensus, or survey. 16. Fenson L, Dale P, Reznick S, et al. MacArthur communica-
A cost-benefit analysis or a meta-analysis may be class I, II, or tive development inventories. San Diego, CA: Singular Pub-
III, depending on the strength of the data upon which the analysis lishing, 1993.
is based. 17. Hedrick DL, Prather EM, Tobin AR. Sequenced inventory of
communication development–revised edition. Seattle, WA:
Definitions for strength of the recommendations University of Washington Press, 1984.
Standard. A principle for patient management that reflects a 18. Ireton H, Glascoe FP. Assessing children’s development us-
high degree of clinical certainty (usually requires one or more ing parents’ reports. The Child Development Inventory. Clin
Class I studies that directly address the clinical question, or over- Pediatr 1995;34:248 –255. (Class I).
whelming Class II evidence when circumstances preclude random- 19. Bricker D, Squires J. The ages & stages questionnaires, sec-
ized clinical trials). ond edition. Baltimore, MD: Paul H. Brookes Publishing
Guideline. A recommendation for patient management that Company, 1999.
reflects moderate clinical certainty (usually requires one or more 20. Glascoe FP. It’s not what it seems. The relationship between
Class II studies or a strong consensus of Class III evidence). parents’ concerns and children with global delays. Clin Pedi-
Practice option. Strategy for patient management for which atr 1994;33:292–296. (Class I).
clinical utility is uncertain (inconclusive or conflicting evidence or 21. Glascoe FP, Sandler H. Value of parents’ estimates of chil-
opinion). dren’s developmental ages. J Pediatr 1995;127:831– 835.
(Class I).
22. Glascoe FP. Parents’ concerns about children’s development:
Appendix 4 prescreening technique or screening test? Pediatrics 1997;99:
American Academy of Neurology Quality Standards Subcommittee 522–528. (Class I).
Members: Gary Franklin, MD, MPH—Co-Chair; Catherine A. 23. Glascoe FP, Dworkin PH. The role of parents in the detection
Zahn, MD—Co-Chair; Milton Alter, MD, PhD; Stephen Ashwal, of developmental and behavioral problems. Pediatrics 1995;
MD (facilitator); John Calverley, MD; Richard Dubinsky, MD; Jac- 95:829 – 836. (Class III).
queline French, MD; Michael Glantz, MD; Michael K. Greenberg, 24. Lord C. Follow-up of two-year-olds referred for possible au-
MD; Gary Gronseth, MD; Deborah Hirtz, MD; Robert G. Miller, tism. J Child Psychol Psychiatry 1995;36:1365–1382. (Class
MD; James Stevens, MD; William Weiner, MD; and Wendy Ed- II).
lund, AAN Manager, Clinical Practice Guidelines. 25. Stone WL, Lee EB, Ashford L, Brissie J, Hepburn SL, Coon-
rod EE, Weiss BH. Can autism be diagnosed accurately in
children under three years? J Child Psychol Psychiatry 1999;
References 40:219 –226. (Class II).
1. Filipek PA, Accardo PJ, Baranek GT, et al. The screening 26. Charman T, Swettenham J, Baron–Cohen S, Cox A, Baird G,
and diagnosis of autistic spectrum disorders. J Autism Dev Drew A. Infants with autism: An investigation of empathy,
Disord 1999;29:437– 482. pretend play, joint attention, and imitation. Dev Psychol
2. Howlin P, Moore A. Diagnosis of autism. A survey of over 1997;33:781–789. (Class II).
1200 patients in the UK. Autism 1997;1:135–162. (Class II). 27. Cox A, Klein K, Charman T, et al. The early diagnosis of
3. Rogers SJ. Empirically supported comprehensive treatments autism spectrum disorders: use of the autism diagnostic in-
for young children with autism. J Clin Child Psychol 1998;27: terview– revised at 20 months and 42 months of age. J Child
168 –179. (Class III). Psychol Psychiatry 1999;40:705–718. (Class II).
4. Lovaas OI. Behavioral treatment and normal educational 28. Mars AE, Mauk JE, Dowrick P. Symptoms of pervasive de-
and intellectual functioning in young autistic children. J velopmental disorders as observed in prediagnostic home
Consult Clin Psychol 1987;55:3–9. (Class II). videos of infants and toddlers. J Pediatr 1998;132:500 –504.
5. McEachin JJ, Smith T, Lovaas OI. Long-term outcome for (Class II).
children with autism who received early intensive behavioral 29. Werner E, Dawson G, Osterling J, Dinno J. Recognition of
treatment. Am J Ment Retard 1993;97:359 –372. (Class II). autism spectrum disorders before 1 year of age. A retrospec-
6. Ozonoff S, Cathcart K. Effectiveness of a home program in- tive study based on home videotapes. J Autism Dev Disord
tervention for young children with autism. J Autism Dev 2000;30:157–162. (Class II).
Disord 1998;28:25–32. (Class II). 30. Baranek GT. Autism during infancy: A retrospective video
7. Sheinkopf SJ, Siegel B. Home-based behavioral treatment of analysis of sensory-motor and social behaviors at 9-12
young children with autism. J Autism Dev Disord 1998;28: months of age. J Autism Dev Disord 1999;29:213–224. (Class
15–23. (Class III). II).
8. Majnemer A, Rosenblatt B. Reliability of parental recall of 31. Szatmari P, Jones MB, Tuff L, Bartolucci G, Fisman S, Ma-
developmental milestones. Pediatr Neurol 1994;10:304 –308. honey W. Lack of cognitive impairment in first-degree rela-
(Class II). tives of children with pervasive developmental disorders.
9. Dworkin PH. British and American recommendations for de- J Am Acad Child Adolesc Psychiatry 1993;32:1264 –1273.
velopmental monitoring: the role of surveillance. Pediatrics (Class II).
1989;84:1000 –1010. (Class III). 32. Jorde LB, Mason–Brothers A, Waldmann R, et al. The
10. Glascoe FP, Dworkin PH. Obstacles to effective developmen- UCLA–University of Utah epidemiologic survey of autism:
tal surveillance: errors in clinical reasoning. J Dev Behav genealogical analysis of familial aggregation. Am J Med
Pediatr 1993;14:344 –349. (Class III). Genet 1990;36:85– 88. (Class I).
11. American Academy of Pediatrics Committee on Children 33. Bolton P, Macdonald H, Pickles A, et al. A case-control fam-
with Disabilities. Screening infants and young children for ily history study of autism. J Child Psychol Psychiatry 1994;
developmental disabilities. Pediatrics 1994;93:863–5. (Class 35:877–900. (Class I).
III). 34. Piven J, Gayle J, Chase GA, Fink B, Landa R, Wzorek MM,
12. Glascoe FP, Byrne KE, Ashford LG, Johnson KL, Chang B, Folstein SE. A family history study of neuropsychiatric disor-
Strickland B. Accuracy of the Denver-II in developmental ders in the adult siblings of autistic individuals. J Am Acad
screening. Pediatrics 1992;89:1221–1225. (Class I). Child Adolesc Psychiatry 1990;29:177–183. (Class II).
August (2 of 2) 2000 NEUROLOGY 55 477You can also read