Paying for Value in Behavioral Health: What California Can Learn from Other States' Medicaid Programs
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Paying for Value in Behavioral Health:
What California Can Learn from Other States’
Medicaid Programs
FEBRUARY 2020
AUTHORS
Robert Belfort, JD, and Adam Striar, MPA, Manatt, Phelps & Phillips
Contents
About the Authors
This paper was prepared for the California I. Key Findings. . . . . . . . . . . . . . . . . . 3
Health Care Foundation by the law firm Total Cost of Care Models a Poor Match for
of Manatt, Phelps & Phillips, LLP (Manatt). Behavioral Health Providers
Robert Belfort, JD, is a partner at Manatt who Promising Practices: Episodic and Bundled
focuses on the representation of health care Payment Models
providers, health plans, and other health care
What About Cost Savings?
companies on regulatory and transactional
matters. Belfort counsels clients on value-
II. Background. . . . . . . . . . . . . . . . . . 4
based purchasing arrangements and other
innovative contracting models. Adam Striar, Introduction
MPA, is a manager with Manatt who provides Defining VBP
policy analysis, research, and operational
support to health care stakeholders includ- III. Landscape Assessment: Medicaid
ing state governments, health care providers, Behavioral Health VBP. . . . . . . . . . . . . 7
and foundations. Vermont
New York
About the Foundation
The California Health Care Foundation is Tennessee
dedicated to advancing meaningful, measur-
able improvements in the way the health care IV. Lessons Learned. . . . . . . . . . . . . . . 18
delivery system provides care to the people of Behavioral Health Providers Are Unlikely to Lead
California, particularly those with low incomes Total Cost of Care Arrangements
and those whose needs are not well served Early Signs That Episodes/Bundles Improve Access
by the status quo. We work to ensure that and Potentially Quality
people have access to the care they need,
Moving from Access and Quality Improvement to
when they need it, at a price they can afford.
Cost Containment
CHCF informs policymakers and industry
V. Considerations for Advancing Behavioral
leaders, invests in ideas and innovations,
Health VBP in Medi-Cal. . . . . . . . . . . . 22
and connects with changemakers to create
a more responsive, patient-centered health Challenges
care system. Opportunities
For more information, visit www.chcf.org. VI. Final Thoughts. . . . . . . . . . . . . . . . 25
Appendices . . . . . . . . . . . . . . . . .26
A. Overview of Medi-Cal Behavioral Health Financing
and Care Delivery Systems
B. Interviewees
Endnotes . . . . . . . . . . . . . . . . . . . . . 30
California Health Care Foundation www.chcf.org 2I. Key Findings
State Medicaid programs are actively pursuing mod- are being encouraged and expected to form account-
els of behavioral health value-based purchasing (VBP). able care organizations (ACOs) and other entities that
To obtain a general understanding of the scope and can assume risk for the total cost of care.
nature of these activities, reviews were conducted of
well-publicized initiatives in three state Medicaid pro- The total cost of care model appears ill-suited for
grams that have adopted different types of behavioral behavioral health providers for several reasons: the
health VBP models: complexity of dividing responsibility for total cost
of care across physical health and behavioral health
Vermont. The state’s hub and spoke model has providers, lack of capital and infrastructure to man-
increased access to addiction treatment in the state, age downside risk, the inability of behavioral health
while the more recent Mental Health Payment Reform, providers to influence the full continuum of care, and
Residential Substance Use Disorder Treatment Case the lack of standardized managed care contracting
Rate, and Applied Behavior Analysis Case Rate meth- templates for behavioral health VBP. In many states,
odologies are attempting to expand behavioral health though, behavioral health providers and the networks
VBP to new types of services. they form may have an opportunity to participate in
total cost of care VBP arrangements as subcontractors
New York. The Behavioral Health VBP Readiness to or partners with larger, integrated provider orga-
Program has invested considerable resources to assist nizations that are driven by hospitals or primary care
behavioral health providers with forming networks organizations.
that can participate in total cost of care and other VBP
arrangements.
Promising Practices: Episodic and
Tennessee. The state’s Health Home program — Bundled Payment Models
Tennessee Health Link — has improved the ability of In contrast, this review found evidence of state sup-
community mental health centers to serve high-need port of and initial success with episodic or bundled
members, while the Episodes of Care program has payment VBP models, which focus on a discrete
demonstrated a promising new approach to VBP for behavioral health treatment, event, or diagnosis.
discrete behavioral health conditions. There are early signs that these models can enhance
access to certain types of behavioral health services
and improve the quality of care. And the models are
Total Cost of Care Models a Poor
adaptable to states, like California, that carve out
Match for Behavioral Health behavioral health coverage under Medicaid.
Providers
This review of these diverse initiatives suggests that
states have either assumed from the outset or con- What About Cost Savings?
cluded through experience that behavioral health However, while episodic or bundled payment behav-
providers are unlikely to be lead contractors in total ioral health VBP models have shown early promise
cost of care VBP arrangements (i.e., arrangements in improving access and quality outcomes without
in which a group of providers assumes financial risk increasing overall Medicaid expenditures, it is still
for the total cost of care for an attributed population, unclear if they can generate meaningful cost sav-
regardless of where services are delivered). This view ings. If these models are going to be adopted widely
is markedly different than the predominant vision across state Medicaid programs, they may need to be
being articulated by state Medicaid agencies and the adjusted to better target cost reduction in addition to
Medicare program for physicians and hospitals, which improvement of access and quality.
Paying for Value in Behavioral Health: What California Can Learn from Other States’ Medicaid Programs www.chcf.org 3total cost of care for an assigned population or for a
II. Background bundle of physical health services. However, given the
significant share of Medicaid dollars spent on enroll-
Introduction ees with serious mental illness (SMI) and substance use
In recent years, state Medicaid programs and the disorders (SUDs), there is increasing interest among
US health care system as a whole have shifted from state Medicaid programs in exploring ways to expand
traditional fee-for-service (FFS) payment methodolo- VBP to behavioral health providers and services.
gies toward VBP models. While FFS rewards providers
based on the volume of their services, VBP aims to This report attempts to offer guidance to state
incent the delivery of high-quality medical care and Medicaid programs and other stakeholders on the les-
improve outcomes while reducing unnecessary health sons learned by states that have sought to develop
care spending. To date, most VBP efforts have focused innovative behavioral health VBP initiatives. Section III
on physical health, with organizations led by large summarizes the recent experiences of three states
health systems or other integrated networks of physi- whose Medicaid programs have experimented with
cians typically assuming financial accountability for the different types of behavioral health VBP models:
Medicaid Managed Care Behavioral Health Delivery Models
Carve-out model. Enrollees receive coverage of behav- 2021 will require individuals with significant behavioral
ioral and physical health services from different payers. health needs to enroll in Behavioral Health Intellectual/
Under these models, coverage of behavioral health Developmental Disability Tailored Plans, which will be
services may be provided through either a separate operated by entities separate from the state’s Standard
managed care plan or through FFS. Examples include Plans (which will enroll most Medicaid enrollees begin-
California, which provides coverage for physical health ning in 2020).
and non-specialty mental health services through main-
Separate product lines for enrollees with significant
stream managed care plans (MCPs), specialty mental
behavioral health needs. Enrollees with significant
health services through county mental health plans
behavioral health needs receive all health care cover-
(MHPs), and SUD treatment through county Drug Medi-
age, including physical and behavioral health, through
Cal delivery systems.
specialized managed care products, which may be oper-
Fully integrated managed care. Medicaid enrollees ated by insurance carriers that also offer mainstream
receive coverage of all physical and behavioral health managed care products in the same state. Examples
services through the same managed care plan. There include New York, which delivers an integrated physical
are no carve-out plans or separate managed care plans health, mental health, and SUD benefit through several
for individuals with significant behavioral health needs. specialized managed care products (in addition to offer-
Examples include Washington, which covers physical ing mainstream managed care plans for most Medicaid
and behavioral health care needs for most Medicaid enrollees). In New York, individuals with significant
enrollees through its Integrated Managed Care delivery behavioral health needs receive coverage through
system. separate Health and Recovery Plans (HARPs), while indi-
viduals living with HIV/AIDS have the option to enroll
Specialized MCOs for enrollees with significant
in HIV Special Needs Plans (SNPs). Medicaid MCOs are
behavioral health needs. Enrollees with significant
permitted to offer more than one product line simulta-
behavioral health needs receive all health care cover-
neously, and several operate both HARPs and HIV SNPs
age, including physical and behavioral health, through
in addition to mainstream managed care plans.
special, separate managed care entities. Examples of
this model include North Carolina, which beginning in
Sources: Margaret Tatar and Athena Chapman, The Medi-Cal Program: An Overview, CHCF, February 2019, www.chcf.org; “Apple Health Managed
Care,” Washington State Health Care Authority, n.d., www.hca.wa.gov; “Behavioral Health I/DD Tailored Plan,” North Carolina Dept. of Health and
Human Services, n.d., medicaid.ncdhhs.gov; and “Health and Recovery Plans (HARPs),” New York State Office of Mental Health, n.d., www.omh.ny.gov.
California Health Care Foundation www.chcf.org 4Vermont, New York, and Tennessee. The descrip- but include retrospective accountability for cost and
tions and assessments of these models are based on quality; this can include models with accountability
interviews with key stakeholders in each state and a for total cost of care or more narrowly defined models
broad review of publicly available materials. Section IV focused on discrete bundles of services or episodes of
synthesizes key lessons learned from these states, treatment. Category 4, the most sophisticated level,
including their challenges, successes, failures, and includes models that establish defined budgets for
adjustments. Finally, Section V includes a discussion providers for a certain population; this includes models
of California-specific considerations. This includes an such as global budgets or capitated arrangements.2
overview of the existing Medi-Cal behavioral health
system, with a focus on managed care structures and Estimates suggest that the majority of health care pay-
existing payment methodologies for behavioral health ments are now made through VBP arrangements. As
services. The conclusion synthesizes key lessons for of 2017, 59% of payments were made through HCP-
Medi-Cal based on the analysis of other states’ efforts. LAN category 2 arrangements or higher, with 34%
of payments falling into categories 3 or 4. Adoption
To create meaningful and appropriate incentives, a has been most widespread in Medicare Advantage
state’s behavioral health VBP model must align with and Medicare FFS, with 50% and 38% of payments
the delivery and payment model for behavioral health falling into categories 3 and 4, respectively, in 2017.
services in that state’s Medicaid program. Thus, for However, commercial and Medicaid payers are not far
purposes of evaluating behavioral VBP options, it is behind, with 28% and 25% of payments falling into
important to keep in mind that there are four primary categories 3 and 4, respectively, in 2017.3
models that states have adopted to cover behavioral
health under Medicaid. These models are summarized
below. Section V discusses the relevance of California’s
model in particular.
Less than one of every five dollars
spent on behavioral health care
Defining VBP is tied to VBP.
VBP arrangements take a number of forms but share
the central aim of tying reimbursement to perfor- While overall adoption of VBP has progressed in recent
mance on measures of quality, clinical outcomes, and/ years, VBP efforts have largely been concentrated on
or cost. A common framework for categorizing VBP physical health providers and services. For example,
is the Alternative Payment Model (APM) framework, many state Medicaid programs have developed ACO
developed by the Health Care Payments Learning and models, which are typically led by hospitals and/or
Action Network (HCP-LAN). The framework organizes PCP groups that agree to assume responsibility for
VBP models into four categories with escalating lev- the total cost of care. The same is true for Medicare,
els of financial accountability and required provider which has invested heavily in the development of the
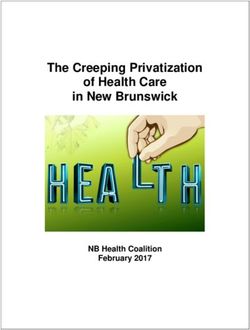
sophistication (see Figure 1, page 6).1 similarly structured Medicare Shared Savings Program.
Although behavioral health may be included in the
Category 1 includes FFS arrangements with no link to benefit package that the ACO is responsible for man-
quality or value; until recently, most payment arrange- aging, behavioral health providers rarely play a leading
ments for health care services fell into this category. role in these arrangements. Less than one of every five
Category 2 includes pay-for-reporting and pay-for- dollars spent on behavioral health care is tied to VBP,
performance models, which allow providers to earn with most such arrangements falling into HCP-LAN
incentive payments from payers on top of regular FFS category 2. Only about one in 10 payments is linked
payments. Category 3 includes shared-risk models, to capitated or other population-based arrangements,
which preserve the underlying FFS payment structure or episodic or bundled payment models.4
Paying for Value in Behavioral Health: What California Can Learn from Other States’ Medicaid Programs www.chcf.org 5Figure 1: The Updated APM Framework
Figure 1. Framework for Alternative Payment Models
Source: Alternative Payment Model: APM Framework, Health Care Payment Learning and Action Network/MITRE Corporation, 2017, hcp-lan.org (PDF).
Overview and Introduction to the 2017 APM Framework Refresh
A LAN Guiding Committee was established in May 2015 as the collaborative body charged with
advancing the alignment of payment approaches across and within the public and private sectors of the
U.S. health care system. This alignment will accelerate the adoption and dissemination of meaningful
financial incentives to reward providers that deliver higher-quality and more affordable care. The LAN’s
mission is to accelerate the health care system's transition to alternative payment models (APMs) by
combining the innovation, power, and reach of the public and private sectors.
California Health Care Foundation
Approved for Public Release; Distribution Unlimited. Case Number 17-2546 3
www.chcf.org
© 2017 The MITRE Corporation. ALL RIGHTS RESERVED
6Vermont
Landscape
III. Vermont has long been a leader in pursuing inno-
Assessment: Medicaid vative payment and delivery strategies to improve
health care outcomes and reduce costs. In 2016, the
Behavioral Health VBP state received authority from the federal government
In order to assess the progress of behavioral health to launch the Vermont All-Payer ACO Model, which
VBP models to date, a comprehensive scan of related allows the state to operate a unique Medicare ACO
programs and payment models was conducted across model and commits it to achieving targets across all
three states: Vermont, New York, and Tennessee. major payers related to health care quality and out-
These states were selected for their commitment to comes, growth in per capita health care spending, and
innovative behavioral health payment and care deliv- provider participation.5
ery models and for their varied Medicaid delivery
system structures; this allowed the drawing of a broad In recent years, the state has also pursued a number
range of lessons relevant to behavioral health VBP. of strategies to advance VBP specifically for behavioral
health services. In 2012, the state launched the “hub
The landscape assessment relies on publicly available and spoke” model for delivering and financing med-
documents — such as managed care contracts, pro- ication-assisted treatment (MAT) for individuals with
vider manuals, policy guidance, and waiver documents opioid use disorder (OUD). This model has been highly
— about each state’s initiatives to describe key details successful in Vermont in improving access to treat-
of their models. Also, interviews were conducted with ment and has since been adopted by multiple states,
Medicaid officials and other stakeholders in each state including California. Beginning in 2019 Vermont also
to gather feedback on successes and challenges asso- rolled out several other initiatives aimed at advancing
ciated with the different VBP approaches. For a full list VBP for behavioral health services, including its Mental
of interviewees, refer to Appendix B. Health Payment Reform initiative, episodic payments
for residential SUD treatment, and a new case rate
payment methodology for applied behavior analysis
(ABA) services.
Figure 2. States and Programs of Focus
Vermont
• Hub and Spoke Model
• Mental Health Payment Reform
• Residential SUD Case Rate
• Applied Behavioral Analysis Case Rate
New York
• Behavioral Health VBP Readiness Program
Tennessee
• Tennessee Health Link
• Episodes of Care
Source: Manatt, Phelps & Phillips.
Paying for Value in Behavioral Health: What California Can Learn from Other States’ Medicaid Programs www.chcf.org 7Hub and Spoke Model:
SUMMARY • Vermont Bundled Rate for MAT
Managed Care Structure The hub and spoke model aims to improve access to
In 2017, Vermont received authority under the MAT for individuals with OUD by creating closer links
state’s Section 1115(a) Medicaid demonstration between different types of MAT providers across the
waiver to implement a unique Medicaid delivery sys- state, while providing funding for enhanced services.
tem model with greater flexibility to align with the
state’s All-Payer ACO initiative. Under the waiver,
Under this model, “hubs” are federally recognized
the state now operates a public managed care–like
delivery model, with the Department of Vermont OTPs with the necessary staff and expertise to treat
Health Access (DVHA) serving as a nonrisk prepaid high-acuity OUD cases and individuals in the early
inpatient health plan subject to all applicable federal stages of recovery. Hubs provide daily dosing and
managed care regulations. Through this model, the therapeutic services and are authorized to dispense
Vermont Agency of Health Services makes capitated all FDA-approved medications indicated for treat-
payments to DVHA, which contracts with Medic-
ing OUD, including methadone. To supplement
aid providers and other public agencies to deliver
service to Medicaid beneficiaries and performs the traditional MAT services, hubs may provide enrollees
functions of traditional managed care plans, includ- with additional services authorized under a Medicaid
ing administering utilization controls and providing Health Home state plan amendment, including com-
care management.6 prehensive care management, care coordination,
Behavioral Health VBP Models
referral to community and support services, transi-
Hub and spoke model. Opioid Treatment Programs
tional care management, and individual and family
(OTPs) serve as “hubs” for delivering all facets supports. Hubs also serve the critical function of sup-
of MAT and are reimbursed through a bundled porting office-based opioid treatment (i.e., outside of
rate for OTP services and separately for Medicaid the OTP setting) by providing training and expert con-
Health Home services. Community-based provid- sultation to primary care providers and other clinicians
ers delivering MAT services (the “spokes”) receive
treating individuals with OUD in the community (i.e.,
Medicaid-financed, specialized staffing support at
no cost to the practice, and consultation and referral
the “spokes”).
support from the hubs.
Spokes are general medical practices with clini-
Mental health payment reform. Community mental
health centers receive a prospective monthly case
cians who are authorized through a federal waiver
rate based on an expected caseload and are also to prescribe or dispense buprenorphine;7 under the
eligible to receive value-based incentive payments Vermont model, the spokes have access to additional
for performance on outcome measures. staff resources as well as referral and consultation
Residential SUD case rate. Residential SUD treat- links to the hubs. Spokes are generally primary care
ment providers are provided a per-admission or family medicine practices that treat low-acuity OUD
rate based on the individual’s SUD diagnosis and patients and those who have transitioned out of a hub;
comorbidities that covers the entire length of an treatment typically includes medication prescribing in
individual’s stay regardless of the number of days.
addition to weekly or monthly visits. To stimulate par-
ABA case rate. Behavior analysts and other pro- ticipation in the model and support community-based
viders treating individuals with autism spectrum providers treating individuals with OUD, all spokes
disorder are paid a prospective monthly payment
have access to one full-time equivalent nurse and one
for all ABA cases during the month based on the
expected number of treatment days.
licensed mental health or addiction counselor per 100
patients. The additional staffing support is financed by
the Medicaid program and made available to spokes
at no cost. These staff members provide specialized
support services for patients with OUD, including coun-
seling and care management supports. Depending
California Health Care Foundation www.chcf.org 8on practice size, support staff may be embedded a separate monthly Health Home rate for patients that
full-time within a specific practice or may split their receive at least one Health Home service during the
time between multiple smaller sites. Spokes also have month. Spokes and local pharmacies are reimbursed
access to expert consultation on OUD treatment best as usual; spokes bill Medicaid on a FFS basis for evalu-
practices from the hubs and may refer complex cases ation and management services, while pharmacies bill
to a hub regardless of insurance status.8 Medicaid for prescribed medications. To finance the
support staff for the spokes, Medicaid pays admin-
The hub and spoke model relies on several different istrative contractors known as Local Administrative
payment streams to support the program’s enhanced Agents (LAAs) to undertake all hiring and staff deploy-
staffing configuration and additional support services. ment functions (i.e., nurses and counselors supporting
Vermont Medicaid pays the hubs a monthly bundled spokes are employed by the LAA, which deploys them
rate for each enrolled OTP patient; this covers meth- into the community based on practice need). Vermont
adone dispensing and counseling services, while Medicaid currently pays LAAs $163.75 per member
buprenorphine and naltrexone are acquired separately per month, which is based on the number of unique
under a “buy and bill” model.9 Hubs may also bill for patients for whom Medicaid paid an OUD medication
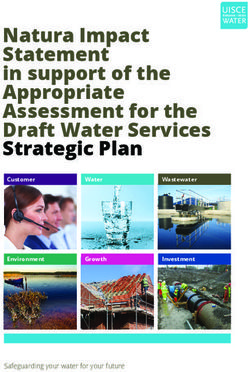
Figure 3. Hub and Spoke Model
Department of Vermont Health Access (Medicaid)
Division of Alcohol and Drug Abuse Programs
PMPM payments
Local Administrative Agents
Support staff salaries
• OTP bundled payments
FFS payments
• PMPM Health Home payments
MAT Support Staff
1 FTE nurse and 1 FTE mental health /
addiction counselor per 100 members
(no cost to spokes)
Hubs Spokes
PATIENTS
INFORMATION
CONSULTATION
TRAINING
• Regional OTPs • PCPs, outpatient addiction programs, pain management
• Specialize in addiction treatment, including high- clinics, and other local providers
intensity MAT • Prescribe buprenorphine and dispense oral and
• Dispense methadone, buprenorphine, and oral injectable naltrexone
and injectable naltrexone • Provide specialized nursing, counseling, and
• Provide Health Home services care management
Source: “Hub and Spoke,” Vermont Blueprint for Health, n.d., blueprintforhealth.vermont.gov.
Paying for Value in Behavioral Health: What California Can Learn from Other States’ Medicaid Programs www.chcf.org 9pharmacy claim over the previous three-month period. allowed them to provide the full complement of MAT
Spoke providers have access to support staff based on support services beyond just medication and counsel-
patient volume at no cost to the practice.10 ing. As a result, the number of OTPs in Vermont has
increased from five before the launch of the program
Evidence from Vermont suggests that the hub and to nine as of 2019; the program has also managed to
spoke model has been successful in promoting access completely eliminate wait lists (which were as long as
and improving quality, with patients treated under the 500 enrollees in 2014) despite doubling the number
model showing substantial improvements in health of individuals engaged in treatment since program
status. Program participants report substantial reduc- launch.13 On the spoke side, access to additional sup-
tions in opioid and other illicit drug use, increased port staff (i.e., nurses and mental health / addiction
housing stability, and improved family life and emo- counselors) at no cost has also substantially reduced
tional health. Evidence also suggests that the program barriers to waivered PCPs offering MAT services. This
has been roughly cost neutral, despite substantial allows practices to focus on treating patients while
investments in additional services, and may be lead- minimizing nonreimbursable time spent on manag-
ing to reduced spending growth over time.11 Despite ing the care of more complex patients. Finally, robust
additional expenditures under the model, a 2018 collaboration between hubs and spokes ensures that
evaluation by the Vermont Blueprint for Health found spokes are properly equipped to deal with complex
no statistically significant difference in total per mem- cases that may require the expertise of addiction spe-
ber per year (PMPY) spending in 2017 for individuals cialists, and small primary care practices are much
receiving MAT ($17,122) compared to those receiv- more likely to accept patients with an OUD in need of
ing other OUD treatment ($16,256). While PMPY MAT as a result.14 The number of MAT prescribers in
payments for pharmacy and spoke staffing were, as spokes has doubled since the launch of the program,
expected, higher for individuals receiving MAT, this from 114 in 2013 to 235 in 2018.15
was largely offset by reductions in spending else-
where, including on inpatient services ($2,117 for the Other Behavioral Health VBP Initiatives:
MAT group vs. $3,513 for the non-MAT group) and Case Rate Payments
outpatient services ($1,139 vs. $2,008). Furthermore, Building on the success of the hub and spoke model,
expenditures on the MAT group have grown more Vermont launched several new behavioral health VBP
slowly since 2011 than expenditures for individuals models in 2019 under the authority of the state’s
with OUD who are not engaged in MAT (5% from 2011 Section 1115 demonstration waiver. These models rely
through 2018 compared to 9.8%).12 This suggests that on case rate payment methodologies for different sets
while the hub and spoke model has not yet been a of services and attempt to align financial incentives
vehicle for reducing overall Medicaid expenditures, for providers to encourage the provision of evidence-
it has improved health outcomes and access to care based, high-quality care while reducing growth in
without substantially increasing costs. And if expendi- health care spending. While representatives from the
tures for individuals receiving treatment through the Vermont Medicaid program were hopeful that these
model continue to grow more slowly, the program programs will help to drive improvements in cost and
could demonstrate net savings in the near future. quality, demonstrated outcomes are not yet available
since the programs were only implemented in 2019.
Stakeholders closely involved with the design of the
model cite several key factors underlying its success Mental Health Payment Reform:
in improving access to treatment and improving treat- Case Rate Payment Methodology for Community
ment outcomes, even without evidence to date of Mental Health Centers
overall cost savings. The enhanced OTP bundled rate The Vermont Department of Mental Health (DMH)
combined with Medicaid Health Home payments has is responsible for directing publicly funded mental
created greater financial certainty for the hubs and health services in the state, including providing for the
California Health Care Foundation www.chcf.org 10delivery of mental health services to Medicaid enroll- Most services provided by DAs and SSAs are cov-
ees as a contractor to the Vermont Medicaid program ered under the case rate. For adults, this includes
and administering state-funded mental health ser- emergency services, community rehabilitation and
vices. Under this dual mandate, DMH contracts in each treatment, and outpatient services. For children, it
region of the state with private, nonprofit community includes emergency services, enhanced family treat-
mental health centers known as Designated Agencies ment, outpatient services, and transitional living
(DAs) for adults, and Specialized Service Agencies programs, and employment and life skill programs18
(SSAs) for children and families. DAs and SSAs are DAs/SSAs may also receive outlier payments on a
responsible for ensuring needed services are avail- case-by-case basis in situations where an individual’s
able to eligible individuals in their respective regions treatment is likely to significantly impact utilization
through delivery of services, program planning, ser- covered by the case rate. A limited set of services
vice coordination, and outcome monitoring. Currently, continues to be paid for outside of the case rate; this
there are 10 DAs and two SSAs in Vermont.16 includes school-based services, job training programs,
eldercare, care at private nonmedical institutions, and
The DMH Mental Health Payment Reform initiative, certain other services funded with state general fund
which launched at the beginning of 2019, established dollars or federal grants.19
a new payment methodology that covers the majority
of mental health services delivered by DAs and SSAs Residential SUD Case Rate:
through a single per member per month (PMPM) Per-Admission Case Rate
case rate payment. The goals of this initiative include DVHA also launched in 2019 a new case rate payment
driving improvements in quality and outcomes while methodology for residential SUD treatment. In contrast
delivering more predictable payments to providers, to the previous per diem payment model for resi-
simplifying the billing process, and providing flexibility dential treatment, the new methodology reimburses
to deliver services in accordance with patient-specific residential treatment providers with a per-admission
needs. The new payment methodology provides pro- rate that covers the entire length of an individual’s
spective case rate payments for both children and residential stay, including both residential detoxifica-
adults based on a target caseload for each DA and tion and residential treatment. The goal of the new
SSA. Each month, DA/SSAs receive a lump sum pay- methodology is to complement existing policies that
ment for all case rate services regardless of the actual encourage providers to align treatment decisions with
volume or intensity of services provided. Prospective the American Society of Addiction Medicine (ASAM)
payments are determined by dividing each DA/ criteria and provide a disincentive for providers to
SSA’s expected annual budget allocation by a target keep individuals in residential treatment for longer
caseload developed using historic data to arrive at than is clinically appropriate.20
a prospective PMPM amount. At least annually, pro-
spective case rates are reconciled against each DA/ The new methodology provides a per-admission rate
SSA’s actual caseload; DA/SSAs that serve a caseload of between $3,532 and $4,803, with variation in the
of at least 90% of their target caseload based on his- payment amount based on the SUD primary diagno-
toric data may keep all prospective payments, but sis and certain co-occurring clinical and social factors
funds may be recouped by DMH if a DA/SSA serves (similar to diagnosis-related group payment method-
less than 90% of the target caseload. The case rates ologies used by Medicare and other payers). Providers
are also supplemented by separate value-based pay- receive an enhanced per-admission rate for individuals
ments, which DMH finances by withholding a portion diagnosed with alcohol or benzodiazepine addiction
of the approved adult and child case rate allocations. (an increase of approximately 14% per admission rela-
DAs and SSAs can access value-based payments by tive to other SUD diagnoses). For all SUD diagnoses,
successfully reporting on required measures and based the base rate (i.e., the rate paid for individuals with
on performance outcomes across select measures.17 no co-occurring disorders) can be further increased by
Paying for Value in Behavioral Health: What California Can Learn from Other States’ Medicaid Programs www.chcf.org 11up to 19% depending on co-occurring diagnoses that on DSRIP investments, the state has since established
can be expected to increase the duration and intensity a goal of having 80% to 90% of Medicaid payments
of residential treatment.21 For residential stays of less delivered through VBP arrangements by 2020. To
than three days, providers are reimbursed $220 per facilitate movement toward the state’s ambitious VBP
diem.22 goals, the state’s “VBP Roadmap” establishes model
guidelines intended to help MCOs and providers be
Applied Behavior Analysis Case Rate: successful in a more value-oriented delivery system.
Tiered Monthly Case Rate The roadmap outlines a variety of population-based
Vermont also implemented a new case rate reim- models, where providers take on responsibility for the
bursement methodology in 2019 for its ABA benefit. total cost of care for attributed members, and bun-
Eligible Medicaid enrollees include individuals under dled/episodic arrangements, where providers assume
age 21 with a diagnosis of autism spectrum disorder responsibility for outcomes and the total cost of care
or an early childhood disability with Medicaid as their associated with a specific illness, medical event, or
sole source of coverage (ABA is reimbursed on a FFS condition. However, the roadmap also notes that pro-
basis for those with insurance coverage in addition viders and payers are free to develop “off-menu” VBP
to Medicaid). To access the case rate, qualified pro-
viders undergo a consultation with a DVHA autism
specialist or designee.23 During the consultation, each SUMMARY • New York
enrollee is assigned to 1 of 14 “tiers” corresponding
Managed Care Structure
to higher reimbursement based on the number of
Since 1997, New York has operated a statewide
recommended treatment hours. Once consultations
Medicaid managed care program that is mandatory
are complete, providers receive a single prospective for most low-income adults and children. Histori-
payment covering all ABA components including cally, the program covered most acute, primary, and
assessment, treatment plan development, direct treat- specialty care services in addition to a limited set
ment, program supervision, parent/caregiver training, of behavioral health and long-term care benefits;
and team conferences for all ABA cases for the follow- most behavioral health services were covered sepa-
rately through the FFS program. In 2015, the state
ing month. Providers are required to submit “shadow
began integrating most behavioral health benefits
claims” during the course of treatment, which don’t into managed care, including through mainstream
trigger payment but are used for program monitoring managed care products and specialized Health and
and year-end reconciliation.24 Recovery Plans (HARPs) for individuals with signifi-
cant behavioral health needs. HARPs, which are
optional for eligible individuals, cover all Medicaid
New York physical and behavioral health benefits in addition
to home and community-based services, Health
New York has taken substantial steps in recent years Home care management, and other enhanced
to advance VBP in its Medicaid program. In 2014, benefits. Medicaid MCOs in New York are permitted
the state received waiver authority from the Centers to offer more than one product line simultaneously,
for Medicare & Medicaid Services (CMS) to imple- and several operate both HARPs and mainstream
ment one of the most ambitious Delivery System managed care plans.
Reform Incentive Payment (DSRIP) programs in the Behavioral Health VBP Models
country. The waiver authorized the state to make Behavioral Health VBP Readiness Program. State-
up to $8 billion in incentive payments to networks approved Behavioral Health Care Collaboratives
of providers with the goals of (1) reducing unneces- (BHCCs) receive payments to finance the develop-
sary emergency department (ED) utilization while ment of infrastructure necessary for success in VBP
arrangements, including organizational structures,
spurring the development of more integrated, high-
data analytic capacity, quality oversight, and clinical
quality care delivery networks and (2) preparing the
integration.
delivery system for wider adoption of VBP. Building
California Health Care Foundation www.chcf.org 12arrangements as long as these arrangements advance New York stakeholders report that the Behavioral
the state’s overall payment reform goals. Through this Health VBP Readiness Program has begun to spur
approach, the state has attempted to strike a balance development of critical VBP capabilities among behav-
between standardization and allowing providers and ioral health providers. For example, MCO and BHCC
payers the flexibility to innovate.25 representatives noted that the program has facilitated
the development of critical IT and analytic infrastruc-
As part of this broader shift toward value, the state ture among behavioral health providers, both through
is beginning to promote VBP in behavioral health organic development of technology platforms and
as well, with a focus in the VBP Roadmap on driving through partnerships with external organizations.
behavioral health integration along with other delivery A representative from the New York State Office of
system reform goals. The state has also launched a Mental Health (OMH) noted that participants have
Behavioral Health VBP Readiness Program, which pro- made substantial progress on organizational gover-
vides infrastructure funding to non-hospital-affiliated nance structures, which are necessary for organizing
behavioral health providers to help them build the and overseeing clinical programs and the financial
capacity to succeed in a more value-oriented delivery management of VBP arrangements (i.e., risk manage-
system. ment, distribution of savings and losses, etc.). The
OMH representative also noted that some clinical
Behavioral Health VBP Readiness Program: integration efforts have been developed as a result of
Infrastructure Payments to Behavioral the program, including patient triaging arrangements
Health Providers between EDs and behavioral health providers, shared
The Behavioral Health VBP Readiness Program, staffing plans in rural areas, and enhanced use of tele-
launched in 2017–18, provides approved Behavioral medicine to facilitate 24/7 access to behavioral health
Health Care Collaboratives (BHCCs) with the opportu- care.27
nity to access up to $60 million in funding over three
years with the goal of improving their ability to contract Despite these successes, stakeholders in New York
with Medicaid MCOs. BHCCs are networks of behav- said there has been little progress on actual VBP con-
ioral health providers that deliver the full complement tracting between BHCCs and MCOs to date. While
of behavioral health services to Medicaid enrollees. both the MCO and BHCC representatives expressed a
BHCCs may be led by a variety of entities, including desire to develop new behavioral health VBP contracts,
licensed nonhospital community-based mental health they said that there are still not enough incentives for
and SUD treatment providers, designated behavioral MCOs to engage in behavioral health–specific VBP
health home and community-based service providers, contracting.28 While the state’s overarching VBP tar-
and behavioral health independent practice associa- gets create a general incentive for MCOs to engage
tions (IPAs). Readiness Program funding is directed in VBP contracting, stakeholders argued that most are
to BHCCs through Medicaid MCOs and can be used able to reach the targets through VBP arrangements
to support both planning and implementation of with hospitals or medical groups, and don’t need to
behavioral health VBP-related initiatives, and to foster contract with BHCCs to get there.29
relationships among BHCC members, engage exter-
nal consultants, and analyze data. In order to access all Stakeholders also cited a lack of readymade VBP
available program funding by the end of year three of contracting templates specific to behavioral health
the program (SFY 2019–20), all BHCC network provid- provider groups as a limiting factor. Medicaid MCOs
ers will need to either be participating subcontractors frequently enter into total cost of care contracting
in a HCP-LAN level 3B or higher arrangement (with arrangements with large health systems and other
the BHCC contracted at level 3A or higher) or be physical health providers, which has led to the devel-
the primary contracted entity in a level 3B or higher opment of standardized approaches and templates,
arrangement.26 but both BHCC and MCO representatives noted that
Paying for Value in Behavioral Health: What California Can Learn from Other States’ Medicaid Programs www.chcf.org 13there are few analogous resources specific to behav- Tennessee
ioral health VBP. Relatedly, both the BHCC and MCO The Tennessee Health Care Innovation Initiative was
representatives stressed that attribution remains a launched in 2013 with the goals of improving quality
persistent challenge for behavioral health providers, and reducing costs in TennCare (Tennessee’s Medicaid
since Medicaid enrollees are already attributed to program). The initiative is focused on three primary
PCPs, and MCOs cannot pay out “duplicate” savings payment and delivery system transformation strate-
to behavioral health providers. BHCCs generally have gies: primary care transformation, episodic payments
less experience with managing financial risk, which for certain discrete episodes of care, and a quality-
requires the ability to track claims expenses in real improvement and VBP initiative for long-term services
time, forecast patient costs, track expenses against a and supports (LTSS). Within the primary care transfor-
budget, and other capabilities. However, stakehold- mation and episodic payment strategies, Tennessee
ers acknowledged that funding through the program has implemented several targeted programs aimed at
may help these organizations develop this capacity by advancing VBP for behavioral health services.33
allowing them to hire staff with the necessary exper-
tise, purchase or develop new analytic tools, or take
other steps. SUMMARY • Tennessee
Managed Care Structure
Finally, representatives from the MCO stressed that
Tennessee was the first state in the nation to enroll
successful risk-sharing arrangements require con-
all Medicaid enrollees in managed care.34 Most
trol over the “whole dollar.” While behavioral health individuals enroll through one of three statewide
conditions drive a substantial share of physical health mainstream managed care plans, which are respon-
spending, a relatively small share of total health care sible for delivering all physical and behavioral health
spending goes toward direct financing of behavioral benefits. The state also offers several specialized
health services. One study found, for instance, that managed care products for those with intellectual
or developmental disabilities, aging or disabled
hospital costs per episode are 40% higher on average
members in need of LTSS, and parents of children
for patients with behavioral health comorbidities.30 in state custody. The state currently does not offer a
However, another found that only 15 cents of every separate managed care product for individuals with
dollar spent on treating individuals with behavioral significant behavioral health needs (i.e., they enroll
health comorbidities goes toward behavioral health in mainstream plans).
care.31 As such, the MCO representatives argued, Behavioral Health VBP Programs
ACOs and other VBP contractors need to be willing to Tennessee Health Link. Medicaid Health Home
make investments in behavioral health care that could model where Community Mental Health Centers
lead to savings on physical health spending in order to receive activity payments for the delivery of Health
be successful under VBP models. However, the repre- Home services and outcome-based payments for
sentatives acknowledged that this model may not be quality performance and continuous improvement
on select utilization measures.
workable for smaller, independent behavioral health
agencies that are not affiliated with a major health Episodes of Care. Providers with control over
system, since they are not able to access savings on the care for a particular episode of treatment or
diagnosis may receive retrospective shared-savings
physical health spending.32
payments or be required to make risk-sharing
payments if actual episode costs differ from a
benchmark; the program has operationalized
48 episodes to date, including two behavioral
health episodes: attention deficit and hyperactivity
disorder (ADHD) and oppositional defiant disorder
(ODD).
California Health Care Foundation www.chcf.org 14Tennessee Health Link: Incentive Payments efficiency metrics, Health Links need to demonstrate
for Community Mental Health Centers continuous improvement in hospital utilization, which
Tennessee Health Link was launched in 2016 as the they may not directly control, in order to fully realize
state’s Medicaid Health Home for adults with serious outcome payments in each year.39
mental illness (SMI) and children with serious emotional
disturbance; currently, the program serves approxi- A representative from a network of CMHCs par-
mately 70,000 enrollees.35 Health Links are required ticipating in the Health Link program noted that the
to deliver the core set of Medicaid Health Home ser- program has provided substantial resources for the
vices, including comprehensive care management, network’s practices to provide enhanced services to
care coordination, health promotion, transitional individuals with significant behavioral health needs.
care, patient and family support, and referrals to The representative highlighted the CCT provided
social supports (LTSS). To be eligible to participate, through the program as being useful for facilitating
a practice must be a recognized Community Mental coordination across provider settings, particularly with
Health Center (CMHC) or other provider experienced PCPs engaged in the state’s Patient-Centered Medical
in treating TennCare members with high behavioral Home (PCMH) program, and identifying assigned
health needs.36 Practices must also agree to adopt the enrollees in need of greater engagement.40 They also
state’s Care Coordination Tool (CCT), a cloud-based, noted that achieving outcome payments is feasible for
cross-payer tool for accessing up-to-date claims and most Health Links, and that outcome payments repre-
admissions, discharge, and transfer (ADT) data on sent a significant share of their total revenue through
attributed members, and participate in two years of the program. However, the representative did express
practice-transformation training.37 Most eligible enroll- concern that the outcome payments were beginning
ees are assigned to a Health Link panel by their MCO to show diminishing returns due to the requirement
using an algorithm that accounts for existing provider for continuous improvement on efficiency metrics.41
relationships and certain other factors; enrollees may
also be assigned through a referral by a discharging Episodes of Care: Retrospective Episodic
hospital or through an attestation by the Health Link Payments for Discrete Treatment Episodes
itself (enrollees may also choose to opt out of the The Episodes of Care program attempts to hold pro-
program).38 viders accountable for the cost and quality of care
associated with specific episodes of treatment. To
Health Links are eligible to receive payments through date, the state has rolled out payments through the
several funding streams. For the first two years of program for 48 discrete treatment episodes, while
participation, Health Links are eligible for practice- an additional 7 have been designed but not yet
transformation payments, which support practices in implemented. Episodes typically comprise all care
making necessary clinical and organizational changes associated with an acute treatment event, such as a
to be successful under the program. Health Links also coronary artery bypass graft, acute asthma exacerba-
receive PMPM “activity payments” for each mem- tion, or total joint replacement; the program has also
ber receiving qualified Health Link services in a given operationalized 2 episodes focused on behavioral
month. Finally, Health Links also have the ability to earn health care: attention deficit hyperactivity disorder
outcome payments based on quality and “efficiency” (ADHD) and oppositional defiant disorder (ODD).42
performance. The quality component of the outcome
payment requires meeting or exceeding performance Two-sided risk under the Episodes of Care program
thresholds across 10 quality metrics. The efficiency is mandatory for TennCare providers; any TennCare
component is calculated based on improvement over provider determined to have the greatest ability to
the previous year across two measures: ED visits per influence the cost and quality of care associated with
1,000 member months and inpatient discharges per a particular episode has the opportunity to earn sav-
1,000 member months. As a result of the design of the ings or may be required to pay back losses. Providers
Paying for Value in Behavioral Health: What California Can Learn from Other States’ Medicaid Programs www.chcf.org 15determined to have the greatest influence over a $ Identifying the Quarterback. Each episode is
particular episode, known as “Quarterbacks,” are linked to a “Quarterback” provider who becomes
automatically held accountable for savings and losses accountable for savings and losses associated with
associated with the episode by the enrollee’s man- the episode. Quarterback status can be assigned
aged care plan. The Episodes of Care program does in several ways, depending on the episode. The
not affect how Medicaid providers bill; Medicaid pro- Quarterback can be the provider associated with the
viders continue to submit FFS claims as normal, even procedure triggering the episode (e.g., the clinician
for procedures that will trigger an episode. Payments or group performing a total joint replacement, for
are then calculated and distributed/recouped retro- the joint replacement episode) or the provider with
spectively by the managed care plan. the plurality of related visits for a particular diagno-
sis (e.g., the provider with the plurality of visits for
The methodology for assigning savings and losses ADHD or ODD during the episode window, for the
varies by episode, with the process for tracking and ADHD and ODD episodes).44
evaluating episode spending guided by detailed
business requirements set forth by TennCare and $ Identifying included expenditures. Each episode
operationalized by the state’s Medicaid managed care includes a list of specific claim types that are
plans. Each episode is constructed using several key included in the total episode spend. In general,
steps:43 included claims are those directly associated with
treating the triggering diagnosis or follow-ups to
$ Identifying an episode trigger. Episodes are “trig- the triggering procedure.
gered” by claims that include specific services or
diagnoses related to 1 of the 48 episodes identi- $ Developing episode-specific spending bench-
fied under the program (e.g., the ADHD and ODD marks. Quarterbacks may earn savings if
episodes are triggered by certain primary care– risk-adjusted expenditures related to the episode
related claims with either ADHD or ODD listed as fall below a “commendable” threshold but are
a diagnosis). required to pay back losses if related expenditures
exceed a level determined to be “acceptable”
$ Identifying the episode window. This step identifies (regardless of where such services were deliv-
a timeframe in which claims (and associated expen- ered or by whom).45 For the 2019 performance
ditures) may be attributed to a specific episode. period, “acceptable” thresholds are established
The window for ADHD and ODD episodes is 179 by TennCare such that the Quarterbacks with the
days after the trigger start date (this is known as the highest risk-adjusted average annual costs across
“trigger window”). Episodes can also include ser- TennCare will owe risk-sharing payments; each
vices that occur during a specified time prior to the MCO sets its own “commendable” thresholds such
episode trigger (e.g., related labs, tests, and medi- that total savings and losses will be equal.46
cations) or after the trigger window (e.g., postnatal
services). Not all episodes, including the ADHD
and ODD episodes, include pre-trigger and post-
trigger services.
California Health Care Foundation www.chcf.org 16Detailed specifications for the ADHD and ODD epi- total cost of care related to ADHD and ODD treatment,
sodes are described in Table 1. small caseloads and the relatively low per-episode
spending serve to limit the incentive to focus on care
While TennCare has sought to provide opportunities improvements, since the total pool of available sav-
for behavioral health providers to participate in the ings is relatively small (only approximately $1.8 million
Episodes of Care program through the ADHD and in savings were achieved across 27,000 ADHD and
ODD episodes, a provider from Tennessee stated that ODD episodes in 2018; comparatively, approximately
the program has had only a limited impact on their $13.5 million in savings were achieved on the perinatal
practice. The representative noted that shared-sav- episode).47 While Health Link is viewed by behavioral
ings payments associated with the ADHD and ODD health providers as a true behavioral health VBP pro-
episodes were dwarfed by FFS payments and those gram, these providers generally consider Episodes
made through the Health Link program. The represen- of Care to be a physical health VBP program, even
tative also noted that, while it is possible to influence though it includes some behavioral health episodes.48
Table 1. Tennessee Episodes of Care Program — ADHD and ODD Episode Specifications
ADHD ODD
Episode Professional claims with an ADHD primary or Professional claims with an ODD primary or secondary
Trigger secondary diagnosis* coupled with certain primary diagnosis† coupled with certain primary care–related
care–related procedure codes procedure codes
Episode $ 179 days following the episode trigger $ 179 days following the episode trigger
Window $ May be extended if a related hospitalization $ May be extended if a related hospitalization
beginning within the window extends beyond the beginning within the window extends beyond the
179th day 179th day
Quarterback Provider with the plurality of visits for ADHD during the Provider with the plurality of visits for ODD during the
episode window episode window
Included $ Hospitalizations, outpatient, professional, and $ Hospitalizations, outpatient, professional, and
Expenditures long-term care claims with a primary or secondary long-term care claims with a primary or secondary
diagnosis* for ADHD diagnosis† for ODD
$ Certain related pharmacy claims $ Certain related pharmacy claims
Thresholds Acceptable: $788 Acceptable: $2,685
Commendable thresholds determined by each MCO Commendable thresholds determined by each MCO
Potential $ Use of assessments to ensure diagnostic accuracy $ Use of assessments to ensure diagnostic accuracy
Sources of and age-appropriateness of treatment and age-appropriateness of treatment
Value‡ $ Appropriate prescribing $ Reductions in the use of medication for non-comor-
bid ODD patients
$ Reductions in unnecessary diagnostic testing and
lab work $ Efficient and cost-effective use of case management
$ Efficient and cost-effective follow-up treatment
*With ADHD-specific symptoms as the primary diagnosis.
†
With ODD-specific symptoms as the primary diagnosis.
‡
For each episode, TennCare outlines key areas where providers may have opportunities to improve the quality and cost of care related to the episode.
Sources: Detailed Business Requirement: Attention Deficit and Hyperactivity Disorder Episode, Tennessee Division of TennCare, April 30, 2019,
www.tn.gov (PDF). Detailed Business Requirement: Oppositional Defiant Disorder Episode, Tennessee Division of TennCare, April 30, 2019, www.tn.gov (PDF).
2019 Episodes of Care Cost and Quality Thresholds, Tennessee Division of TennCare, n.d., www.tn.gov (PDF).
Paying for Value in Behavioral Health: What California Can Learn from Other States’ Medicaid Programs www.chcf.org 17You can also read