Giving Health Inequality a Voice - Author: Audry Deane MBA For the European Anti-Poverty Network (EAPN) Ireland August 2020 - EAPN Ireland
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Giving Health Inequality a Voice Author: Audry Deane MBA For the European Anti-Poverty Network (EAPN) Ireland August 2020
Acknowledgements EAPN Ireland would first of all like to acknowledge the time given by
participants in the five focus groups in Knocknaheeny in Cork City,
Donegal and Longford, Fettercairn in Tallaght and in Dublin’s north
inner city. Also their honest and openness in discussing their experience
and allowing it to be used for this report. Particular thanks to those
who helped bring the focus groups together locally. We also want to
acknowledge the input of the staff in the Public Interest Law Alliance
of the Free Legal Advice Centres (FLAC) for their input on the right to
health. Finally, to thank Audry Deane for her skills and commitment to
this project as facilitator of the focus groups and as author of the report.
EAPN Ireland, The European Anti-Poverty Network (EAPN) Ireland is a national
100 North King Street, community organisation which was established in 1990. It is a network
Smithfield, Dublin 7; of almost 170 groups and individuals working against poverty. The
+353 (0)1 8745737 mission of EAPN Ireland is to put the eradication of poverty at the top
www.eapn.ie of the Irish and European policy agenda and empower groups working
@EAPNIreland to end poverty to understand and influence policy-making. It is the Irish
member of EAPN (Europe).
This project has received funding from the Irish Human Rights and
Equality Grants Scheme as part of the Commission’s statutory power to
provide grants to promote human rights and equality under the Irish
Human Rights and Equality Commission Act 2014. The views expressed
in this publication are those of the authors and do not necessarily
represent those of the Irish Human Rights and Equality Commission.Executive Summary 4
01
Ireland’s public health system - a broken model
1.1 Rationale for this report 11
1.2 The right to health 12
1.3 Overview of the Irish public health system 13
1.4 Inequality in life expectancy and death rates 13
1.5 Cost of healthcare a barrier to access 14
1.6 Health inequalities - the link to poverty and low income 16
1.7 Health Inequalities - a structural problem 16
1.8 Health inequalities - the role of geography 18
1.9 Poor capacity and long waiting times cause inequalities 19
02
Social Determinants of Health - their role in health inequalities
2.1 Is Healthy Ireland reducing health inequalities? 23
2.2 Are health inequalities addressed in Sláintecare? 26
2.3 Co-creation and a health inequalities index to improve 27
citizen outcomes in Healthy Ireland and Sláintecare
03
Giving health inequalities a voice
3.1 Social Determinants of Health and the link 30
to health inequalities 31
3.2 Long waiting times 32
3.2 Cost and inadequate provision of transport services 32
3.4 Mental health 34
3.5 GPs 34
3.5.1 GPs charging medical card holders for blood tests 36
3.6 Collaboration and joint working 37
3.7 Discrimination, respect and accountability 39
3.8 Medication and equipment 40
3.9 Administrative and structural barriers 41
3.10 Dental services
Conclusion 43
Appendices
Appendix 1 47
Appendix 2 48
Appendix 3 49
EAPN Ireland Giving Health Inequality a Voice 3Executive Summary EAPN Ireland Giving Health Inequality a Voice 4
EAPN Ireland sees at first-hand how the social is needed to address the social determinants of
determinants of health, poverty and ill-health health. Goal Two of the framework is reducing
intersect to create health inequalities. This report health inequalities. EAPN Ireland believes that
was commissioned to make those links apparent placing the eradication of health inequalities within
through listening to people in communities and a behavioural lifestyle strategy is aspirational but
proposing recommendations to improve the health not practical for vulnerable and disadvantaged
outcomes of those we work for and represent by groups as it does not address the root cause of their
strengthening how our national health strategies predicament, structural disadvantage, which results
address health inequalities. from distribution choices and explicit resource
restriction in the public health system. We agree that
The project is funded by the Irish Human Rights behaviour change programmes have a part to play
and Equality Commission and builds on the in improving population health but are convinced
work of the Community Platform on the right to that it is unrealistic to expect people living precarious
health. It involved five focus groups in late 2019 disadvantaged lives to engage with these initiatives.
in Knocknaheeny in Cork City, Donegal, Longford,
Fettercairn in Tallaght and in Dublin’s north inner — EAPN Ireland asks that Healthy Ireland recognises
city. In total more than 50 participants took part in the limited ability of vulnerable groups to
the focus groups. opt into engaging with its programmes and
initiatives and develop more user sensitive,
EAPN Ireland believes that everyone has the right proactive and effective ways of engaging with
to health but is concerned at the lack of an explicit these disadvantaged communities.
right to healthcare in Ireland. The UN Covenant
on Economic, Social and Cultural Rights (ICESCR)
recognises the right to health and defines it in
relation to availability, access to, acceptability and Sláintecare
quality of health facilities, goods and services.
While EAPN Ireland supports the ambition, scale
However, in Ireland the state is failing in its
and breadth of the Sláintecare reforms to deliver
duty to provide adequate healthcare for many
the Right Care, in the Right Place by the Right Team
disadvantaged and marginalised individuals and
at low or no cost, we are concerned that reducing
groups, with the result that they experience worse
health inequalities is not in itself a central goal.1
health outcomes, including lower life expectancy.
We acknowledge the complexity of the challenges,
While we welcome the focus on outcomes and the in particular the unwinding of private health care
impact of policies on people and communities in from public health care settings, but wish to see a
the new Programme for Government, we note that more explicit and cohesive approach to addressing
neither health inequalities nor the need to address the social determinants of health and the negative
the social determinants of health are mentioned role they play in the lives of citizens who experience
anywhere in this Programme. health inequalities. We note the various projects
across the four workstreams which aim to reduce
cost and improve access but recommend a deeper
Health Ireland focus and alignment of effort to combat how difficult
The Healthy Ireland Framework for Improved circumstances and lack of access to resources affect
Health and Wellbeing 2013- 2025 states that vulnerable users of the public health service. We
health and wellbeing are not evenly distributed are also deeply concerned at the significant delay
across Irish society and says that a broad focus in Sláintecare Project 2.4 (to review the current
framework and develop a policy proposal and
EAPN Ireland Giving Health Inequality a Voice 5roadmap for universal eligibility) which was one the recommendations in this report which we offer
of only two projects which experienced a major in a spirit of collaboration.
delay in 2019. This delay in implementing the
entitlement element of the Sláintecare reforms These recommendations come directly from the
is very disappointing for EAPN Ireland as this is people who attended the five EAPN Ireland focus
a critical enabler to reduce health inequalities. It groups held in Cork City, Donegal, Longford,
does not bode well that this core element of the Dublin County and Dublin’s north inner city in late
Sláintecare transformation did not progress in 2019 2019. Participants came from a cross section of
given how inequality of access is embedded in our the disadvantaged communities living in these
current health system, where the complex nature of locations including low income families, lone
eligibility for services and schemes blocks access and parent households, migrants, Traveller and Roma
affordability. and people living with addictions. Specific themes
emerged in these meetings, in particular how
— To reduce the future burden on the health inadequate income and poor access to resources
system EAPN requests a more cohesive impact negatively on people’s lives and health status.
approach across all Government Departments
to streamline and align all actions/ deliverables The recommendations below are informed directly
on the social determinants of health to improve by the lived experience and daily lives of the
effectiveness, efficiency and transparency. participants. EAPN Ireland is deeply grateful for the
honesty and openness of those who shared their
— EAPN Ireland requests the establishment of stories. They willingly contributed so that future
a monitoring index containing both health health policy and services can be more effective
inequality indicators and all measures which in reducing the deep inequalities in both access to
address health inequalities, particularly in health and in outcomes health.
both Healthy Ireland and Sláintecare - and all
other relevant strategies. We propose that the All focus group participants had an intuitive
maintenance of this index should be the remit of understanding of the links between the social
an independent research institute or body. determinants of health and health status and
outcome. Participants wanted health and social
care professionals to both understand how the
social determinants of health impact negatively on
Recommendations from Communities the health status of communities and to show this
understanding in their approach and practice. They
Through its work with disadvantaged communities
recommended that:
across Ireland the European Anti-Poverty Network
(EAPN) Ireland knows that service users are best — Training on the social determinants of health
placed to advise on what supports make a positive should be mandatory for all health and social
difference to their lives and meet their needs. care staff in both acute and community settings.
This is why we decided to capture the voice of Health and social care managers need to have
disadvantaged people, in five focus groups held the autonomy and responsibility to ensure that
across Ireland in late 2019, to hear their stories of their staff undergo training to deepen their
accessing health services. The gaps, failings and ability to engage respectfully and appropriately
deficits of current health policy and service provision with people from different cultural and social
were laid bare in these personal accounts. The backgrounds.
experiences, observations and most importantly the
suggestions from the focus groups form the basis for
EAPN Ireland Giving Health Inequality a Voice 6Participants raised concerns over long waiting times — A one stop phone line for mental health services
as a serious barrier to accessing healthcare as well be rolled out to all regions.
as the additional barriers created by the cost or
— The rotation of mental health doctors should
inadequate provision of transport.
be limited, as consistency is key to forming trust
The corrosive impact of poor mental health on and a positive patient doctor relationship.
individuals, families and communities was a priority
There was a detailed discussion in relation the
issue for participants. People were unanimous that
General Practitioners and recommended to
experiencing poor mental health often stemmed
following.
from their daily struggles dealing with the social
determinants of health - housing, low or no income, — GP training should have a stronger component
poor educational opportunities and attainment, of authentic communication and listening skills
living in deprived areas with no amenities, uncertain as these attributes were identified as core
legal status et al. The interconnectedness between attributes of effective GPs.
poverty, the negative effects of living in poor living
conditions and neglected deprived communities — GPs need to be better informed of what other
and the lack of adequate mental health services was interventions and services are available in their
clearly articulated. There was a majority view that community (both statutory and voluntary).
not having timely access to health services resulted
— GPs need to have a proactive approach to
in people experiencing poorer mental health and
collaborating with local community and
higher levels of stress. The participants made the
voluntary service providers and refer patients if
following recommendations.
appropriate.
— The HSE should collaborate with community
— GPs must be open to investing time in agreeing
leaders and groups in areas with severe social
structured ways to develop relationships and
problems to find solutions which improve the
links with local non statutory service providers
physical and mental wellbeing of residents.
and organisations.
— The provision of 24/7 access to community-
— GPs must stop charging medical card holders for
based wrap around mental health services.
needed blood tests in contravention of national
— Responsive integrated referral management policy.
should be put in place- including Social
Low referral rates from health professionals to
Prescribing and referral to specific community
community-based health services and supports
and voluntary services - to optimise patient
was accepted as a disappointing reality for many
outcomes and avoid acute admissions.
community organisations. The importance of more
— Person-centred support should be provided collaboration and joint working was highlighted
for people, prior to planned mental health with a consensus view that more proactive referrals
appointments, to encourage attendance. to local services, in particular by GPs and Public
Health Nurses, would result in better health and
— The HSE should employ people who have wellbeing outcomes for patients. Participants were
experience of mental health conditions, to work clear that they wanted health care staff to have a
in support roles in the community. deeper knowledge of what services and supports
community organisations in their catchment area
offer. Minority ethnic participants spoke of the need
EAPN Ireland Giving Health Inequality a Voice 7for the health and social care services to reflect their — Sensitive, respectful restorative space must
communities, saying that the best way to achieve be prioritised to build community capacity
this is to employ staff from these communities and to engage productively with statutory health
marginalised groups. services, particularly in very deprived areas.
— Social prescribing should be rolled out and used EAPN Ireland notes that the new Programme for
as a priority service across the HSE and by all Government views enhanced governance and
GPs contracted under the Medical Card Scheme. accountability as key components of the Sláintecare
Resources must be allocated in all Regional reforms. This correlates very closely with how the
Integrated Care Areas using the learning from focus groups felt that issues of discriminate and
the Sláintecare Integrated Fund projects to attitudes needed to be addressed and the strong
increase the use of this model. call for HSE managers to be visible to services users
and for them to be accountable for the attitudes and
— All health and social care professionals working behaviours of those staff working for them.
in primary and community care service settings
should undertake a compulsory community — Cultural and ethnicity training to be provided so
development training module that all health and social care staff are aware of
specific cultural differences in the Traveller and
— HSE should employ people from specific ethnic all ethnic minority communities.
groups to work as paid advocates in their
communities. — HSE managers must be both visible and held
accountable for the level and quality of services
— Language and other supports for groups in their staff provide. Training must be provided to
resettlement programmes should continue as resource managers to enable them to deliver on
long as needed, with people employed from this responsibility.
these communities to act as peer educators who
can help people link into services and supports. — Managers should visibly intervene when poor
behaviour is witnessed or reported, with swift
— Statutory staff must have dedicated time and transparent action taken in the event of a
factored into their work plan to allow time for breach of good practice.
developing relationships, build joint working
processes and knowledge of community groups. — The HSE should employ staff from minority
ethnic groups and from marginalised groups to
— Both statutory and community sectors must specific roles within relevant services.
accept that assumptions, attitudes and
behaviours must change on both sides to — Behaviours and attitudes of staff who deal with
collaborate effectively. service users with different ethnicities, cultures
and religions must be tolerant, respectful and
— Formal processes are needed to ensure show courtesy and dignity.
authentic community representation is factored
into the design and delivery of health and social — Complaints procedures must be clearly
care services. explained and displayed prominently in HSE
settings.
— Structures must be designed, and maintained,
which enable and facilitate both the knowledge The focus group participants raised a number of
of community groups and their feedback, to be issues and made recommendations related to
fed into how local services are designed. medication and equipment.
EAPN Ireland Giving Health Inequality a Voice 8— GPs should ensure that the medication they — Allow GPs to issue repeat prescriptions for
prescribe is covered under the Medical Card people with chronic conditions, avoiding
Scheme to avoid unnecessary stress and the need to attend specialist out-patient
embarrassment for patients. clinics - EAPN Ireland is aware of the ongoing
modernisations in areas of eHealth, medicines
— Instructions on medication must be written in management and multidisciplinary working.
clear English to take into account language and
literacy problems. — Improve access to nutritional advice in primary
care settings, particularly in GP practices where
— Pharmacists should be incentivised to possible.
collaborate proactively with local organisations
to improve service user understanding. — Review conditions covered under the Long-Term
Pharmacists should publicise local groups Illness Scheme.
which support specific groups (those with low
Finally, a number of issues related to dental services
literacy, foreign nationals) to understand their
were raised with the recommendations to:
medication and instructions.
— Improve capacity in the Dental Treatment
— To ensure consistency and patient wellbeing
Service Scheme to reduce waiting time for
for long-term mental health services users who
treatment.
attend out-patient appointments, all prescribing
should be done by a consultant, and not by — Provide weekend access to emergency dental
Senior House Officers, who rotate on a six- services.
monthly basis.
A range of administrative and structural barriers
to accessing healthcare were highlighted and the
participants proposed the following to address some
of these.
— Primary Care Reimbursement Service to improve
the quality and responsiveness of their customer
care service particularly in difficult and complex
cases.
— Prioritise the roll out of the Single Assessment
Tool across all regions.
— Take service user residence into account
when scheduling appointments for tests and
treatment, particularly for those outside Dublin
who must travel.
— Improve communication on how to access
equipment and simplify procurement to reduce
the number of suppliers patients must interact
1 Government of Ireland. (2017). Committee on the Future
with. of Healthcare Sláintecare Report. Available at:
https://tinyurl.com/y3mr7ajo [Accessed 11th November 2019].
EAPN Ireland Giving Health Inequality a Voice 901 Ireland’s public health system - a broken model 1.1 Rationale for this report 1.2 The right to health 1.3 Overview of the Irish public health system 1.4 Inequality in life expectancy and death rates 1.5 Cost of healthcare a barrier to access 1.6 Health inequalities - the link to poverty and low income 1.7 Health Inequalities - a structural problem 1.8 Health inequalities - the role of geography 1.9 Poor capacity and long waiting times cause inequalities EAPN Ireland Giving Health Inequality a Voice 10
1.1 Rationale for this report and strategies can be strengthened to reduce
health inequalities, where access to quality health
Now more than ever the protection and wellbeing of and social services is equitable and not dictated by
vulnerable groups must be central to how the health income and where the right to health is enshrined
services are designed and delivered. and protected in law. This report also builds the
work EAPN Ireland has undertaken as a member of
Across the globe the Covid19 pandemic is throwing
the Community Platform on the right to health and
health inequalities into sharp relief where people
its six principles for an inclusive health policy.
with less means and resources struggle to access
health care and experience worse health outcomes, The purpose of this report is three-fold:
with some paying the ultimate fatal price. In Ireland 1. to show how deeply the social, economic and
those in precarious situations - the unemployed, environmental determinants of health affect
people with disabilities, homeless people, those with both people’s experience of accessing health
addictions, ethnic minorities (particularly Travellers services and their health outcomes
and Roma) and migrants (documented and
undocumented) who cannot access social protection 2. to highlight how current national health
schemes, are very vulnerable. Many people with strategies do not adequately address the
precarious work have lost their poorly paid jobs with challenge of health inequalities
minimal protection and benefits.
3. to contribute recommendations to strengthen
Through its work with member organisations how national policy strategies tackle health
working in disadvantaged communities across inequalities and the right to health
Ireland the European Anti-Poverty Network (EAPN)
Section 1 of the report offers a short overview of
Ireland knows that service users are best placed to
current health and social care policy and services
advise on what supports make a positive difference
showing how the social determinants of health
to their lives and meet their needs. This is why
- in particular socio-economic status and lack of
we decided to capture the voice of disadvantaged
resources - and inequalities of access to public
people, in five focus groups held across Ireland, to
health services impact on health status and
hear their stories of accessing health services. The
outcome. Other reports are cited which demonstrate
gaps, failings and deficits of current health policy and
how the entwined nature of public and private
service provision were laid bare in these personal
healthcare provision reinforce the depth and
accounts. The experiences, observations and most
breadth of health inequalities in Ireland. The section
importantly the suggestions from the focus groups
concludes with a brief critique of the two main health
are the basis for recommendations in this report.
strategies in how they address health inequalities,
They are made with the intention to improve how
namely Healthy Ireland and Sláintecare.
health inequalities are currently being addressed in
Irish national strategies. In section 2 the stories, insights, observations and
concerns from the five focus groups are used to
The focus groups were held in November and
illustrate the deficits and gaps in the public health
December 2019, in Knocknaheeny in Cork City,
system. Recommendations to address health
Donegal, Longford, Fettercairn in Tallaght and in
inequalities and strengthen the right to health are
Dublin’s north inner city. In total more than 50
provided in a spirit of collaborative and constructive
participants took part in the focus groups.
engagement. EAPN Ireland is appreciative of the
EAPN Ireland offers this report as a timely good will and interest of relevant health policy
contribution to influence how current health policy makers and stakeholders who had agreed, pre
EAPN Ireland Giving Health Inequality a Voice 11Covid 19, to participate in a roundtable event where In the 22nd session, (in its General Comment no
these recommendations were to be explored and 14) the UN Committee on Economic Social and
discussed further in a solution focused dialogue to Cultural Rights provided detailed guidance to States
address health inequalities. regarding their obligations to respect, protect and
fulfil the right to health. The Committee also noted
that the right includes the following interrelated and
1.2 The right to health essential features: 3
EAPN Ireland believes that everyone has the right
— Availability. States should ensure the provision
to health. This right relates to both the right of
of enough functioning public health and
individuals to obtain a certain standard of health
individual health care facilities throughout their
and health care, and the State obligation to ensure a
territory, as well as safe water and sanitation
certain standard of public health with the community
facilities, trained and fairly-paid medical
generally.
professionals, and essential medicines.
EAPN Ireland is concerned at the lack of explicit right
— Accessibility. Access to health involves four
to healthcare in Ireland. There is no fundamental
key elements: non-discrimination, physical
right to health in the constitution. Article 45.4.1 of
accessibility, economic accessibility, and
the Irish Constitution states
information accessibility. Health facilities and
The State pledges itself to safeguard with especial services should be accessible to everyone,
care the economic interests of the weaker sections of especially the most vulnerable, without
the community, and, where necessary, to contribute discrimination on any prohibited ground. The
to the support of the infirm, the widow, the orphan, facilities and services, as well as underlying
and the aged 2 determinants of health such as water and
sanitation amenities, must be within safe
But as this article sits under the Directive Principles physical reach. Health care facilities, goods and
of Social Policy it is not binding and is only used for services must be affordable for all, with any
general guidance only. As yet the right to health and payment based on the principle of equity so that
social care services is not defined in Irish legislation. poorer households are not disproportionately
Without legislation access to health will continue to burdened with health-related expenses. States
be discretionary and unequal. must ensure that every person has the right to
seek, receive and impart information on health,
Like many other nations Ireland brought the
in balance with the confidentiality of medical
European Convention on Human Rights into law
information.
in 2003. Previous to this date the UN Covenant on
Economic, Social and Cultural Rights (ICESCR) was — Acceptability. Health facilities should be
ratified in 1989. This covenant recognises the right respectful of medical ethics and the culture of
to health defined in relation to availability, access individuals and communities, as well as attentive
to, acceptability and quality of health facilities, to gender and life-cycle requirements.
goods and services. Article 12 provides the most
comprehensive article on the right to health in — Quality. Health facilities should be scientifically
international human rights law. It recognises “the and medically appropriate and of good quality.
right of everyone to the enjoyment of the highest Among other things, this requires the provision
attainable standard of physical and mental health.” of necessary medicines and equipment, skilled
EAPN Ireland Giving Health Inequality a Voice 12medical professionals, and adequate water and slower access to needed care, not always provided
sanitation. by consultants. In Ireland access to health services
is predicated on income. This results in health
In 2015, during its examination of Ireland’s progress inequalities in Ireland having a serious social
in protecting, respecting and fulfilling rights gradient with those in the lower socio-economic
contained in ICESCR, the Committee expressed groups experiencing worse health outcomes,
concern at the overall deteriorating healthcare morbidity and life expectancy. 4
services and at the negative impact on the access
of disadvantaged and marginalised individuals and While EAPN Ireland fully supports the vision of the
groups to adequate healthcare, in particular: all-party Sláintecare reform blueprint to deliver
universal access in a one tier system we are very
a. The widening disparity between people with aware that the right care in the right place at the
and those without private health insurance in right time is not the reality for people currently trying
accessing medical services, to access the public health system in Ireland. Equal
access to equal care for equal need is not a reality
b. The delay in providing universal health services
for people in the Irish public health system. Life
and community-based health services;
expectancy is poorer for people with low incomes,
c. The lack of oversight of healthcare services; and for those living in deprived areas and for Travellers
in particular, than for the general population.
d. The poor health state of Travellers and Roma,
particularly their life expectancy and infant
mortality which are respectively 15 years less
and more than three times higher than the
general population. “
The differences in life
The shortcomings and deficits listed by the
expectancy between people
ICESCR in 2015 have not been eliminated. Health
inequalities continue to have a very steep social
living in the most disadvantaged
gradient where those with less means depend on the areas compared to those living in
oversubscribed public health system where demand the most affluent is stark.
outstrips supply.
”
1.3 Overview of the Irish public health
system
Ireland remains unique in the EU in not providing 1.4 Inequality in life expectancy and death
universal access to primary care. Ireland’s
rates
acceptance of the high level of duplicate private
health insurance coverage has resulted in a distinct Data from difference sources shows that life
two-tier health care system where those who can expectancy for specific groups in Ireland is lower
afford it buy private health insurance and avail of than for the general population, particularly for
fast tracked access to diagnosis and treatment, Travellers. The differences in life expectancy
while those on limited incomes make do with an between people living in the most disadvantaged
oversubscribed, under resourced public health areas compared to those living in the most affluent
system characterised by long waiting lists and is stark. There are clear differences in life expectancy
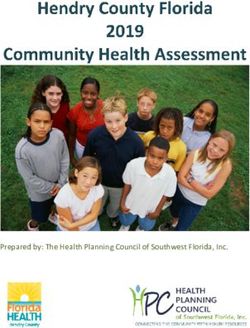
EAPN Ireland Giving Health Inequality a Voice 13related to social class. Figures 1 and 2 below show Standardised death rates per 100,000 of population
how social class and occupation impact on life
expectancy and death rates.
Social Class Persons Males Females
Census 2016 shows that people in the most deprived
areas have the worst life expectancy, with life Professional workers 494 478 451
expectancy for men in the most well off areas living
five years longer than those in the poorest (84.4 Managerial & technical 482 501 470
years and 79.4 years respectively), while for women
the gap in years lost due to location was four. 5 Non-manual 511 590 497
Differences in life expectancy in years from least
deprived to most deprived areas Skilled manual 676 627 673
Males Females Semi-skilled 661 677 637
All 82.0 85.5
Unskilled 796 804 751
First Quintile 84.4 87.7
(least deprived) Others including unknown 841 906 803
Second Quintile 83.2 86.5
Table 2. Source CSO Mortality Differentials in Ireland 2016- 2017 6
Third Quintile 82.2 85.7
1.5 Cost of healthcare a barrier to access
Fourth Quintile 81.9 84.9
Two recent reports show the correlation between
inability to pay and lack of access to needed health
Fifth Quintile 79.4 83.2
(most deprived) care.
Table 1. Source CSO Mortality Differentials in Ireland 2016-2017 The ESRI analysis of the EU SILC 2013 data found that
4% of the population had an unmet health need with
While this is an improvement on the 2010 statistics,
59% citing the cost of care as the reason they did
glaring differences in life expectancy persist related
not access the care they needed, while long waiting
to occupation. The difference in life expectancy
lists were blamed by those with medical cards. This
at birth for men in the professional social class
research found that women, lower income groups
group was 6.1 years higher than for their unskilled
and people with poorer health status were most
counterparts while for women the difference in life
likely to have an unmet need for health care. 7
expectancy was 5 years.
In 2019 research by the Trinity Centre for Health
The gap in death rates for different occupations is
Policy and Management found that there was
also evident. Figure 2 shows that for every 100,000
an increase in the level of unaffordable private
deaths in the population 494 were professional
healthcare spend, from 15% in the period 2009 to
workers, while the death rate was 796 for unskilled
2010 up to 18.8% in 2015 to 2016 period.8 Analysing
workers out of every 100,000 deaths.
data from the Irish Household Budget Survey this
study found that households on the lowest incomes
were disproportionately affected by this increase in
EAPN Ireland Giving Health Inequality a Voice 14private health expenditure. It found that those with These findings clearly show that those on the lowest
the least means selected to pay for private access incomes chose to incur unaffordable expenditure
to outpatient consultations. Given the unacceptably to access timely diagnosis and treatment via private
long waiting times in the public system this is not an health insurance, even though they could not afford
unexpected finding. Other results included: to and already had free access to the public health
system as medical card holders. That 62.3% of
— Over 16% of the spend for medical card holders
households with free access to the public system
went on GP visits, in patient and out-patient
spent their limited income on buying unaffordable
consultations, which are free to this cohort in
access to private care demonstrates how intolerable
the public system
this inequity is for this needy cohort.
— Spend on private health insurance increased the
most in the lowest income quintile in both waves
of the survey
The below table summarises their findings:
2009–2010 2015–2016
Proportion of households experiencing unaffordable out of pocket
payments
Medical Card 63.8% 72.5%
GP card 2.7% 5.8%
No cover 33.5% 21.7%
Proportion of households experiencing unaffordable private health
insurance expenditure
Medical Card 57.2% 62.3%
GP card 3.2% 9.7%
No cover 39.6% 28%
Table 3 Source Private health expenditure in Ireland: Assessing the
affordability of private financing of health care
EAPN Ireland Giving Health Inequality a Voice 151.6 Health inequalities - the link to poverty
and low income
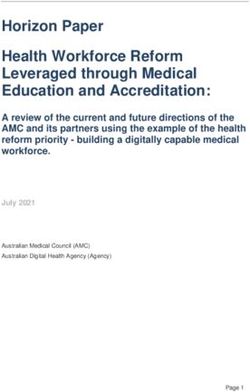
Analysis of the 2017 SILC data found that almost a
third of households which needed medical treatment
found the cost difficult to afford, with 27.4%
reporting dental costs as problematic while 35%
found the cost of medication caused hardship.
0 10 20 30 40 100
80
Medical
60
Dental
40
Cost of 20
Medicines
0
Medical / GP card coverage
Households Households State
without children with children At Risk of Poverty In Consistent Poverty
Figure 1. Households who experienced a financial burden from Figure 2 Medical card and poverty status. Source CSO SILC 2017 10
health expenses. Source CSO SILC 2017 9
Data from the same source shows that 89% of
1.7 Health Inequalities - a structural
people in consistent poverty had medical cards,
problem
while 71% of those at risk of poverty had either a
medical card or a GP Visit Card. Recent reports have highlighted how the hybrid
structure of the Irish health system results in poorer
access and outcomes for those forced to rely on the
public health system. A welcome focus has emerged
on the needs of the ‘twilight’ group of people who
have incomes above the medical card eligibility,
without private health insurance who experience
hardship when they pay for needed heath care.
While the World Health Organisation states that
universal healthcare is the best way to improve
EAPN Ireland Giving Health Inequality a Voice 16global health, Ireland has remained an outlier in Specific Recommendation 1 that Ireland
continuing its complex system of health financing
“Improve accessibility of the health system and
founded on the mix of public/ private provision.11
strengthen its resilience, including by responding
Access, entitlement and eligibility to the various
to health workforce’s needs and ensuring universal
elements of the public health system, and in
coverage to primary care.”
particular to the various schemes is complex and
difficult to navigate. Other recent reports concur with the structural
barriers which impede progress to universal health
Health service users struggle with complicated mean
care. A 2018 report from the European Social Policy
testing systems which are time consuming to apply
Network noted the structural disincentives which
for (and to process) and which exclude many whose
reinforce unequal access and outcomes. 13 Also in
incomes are above social welfare payment rates.
2018 a TASC and FEPS report again drew attention
Signposting within the HSE, given its complexity,
to Ireland’s unique position in Europe in not having
multiple settings and locations is unsatisfactory
universal access to primary care.14 This report
to many service users and HSE staff themselves
critiques the two-tier system and points to the large
acknowledge the difficulties inherent in the different
gap of 21.5% between higher and lower income
schemes and services.
groups in the self-reporting of their health status.
The de Buitléir report published in 2019 sets out This report also highlights the precarious position
an explicit road map to remove private health care of the ‘twilight’ group whose low incomes prevents
from publicly funded hospitals. This report is of them from being able to afford the high costs of out
central importance to the effective delivery of the of pocket health expenses.
Sláintecare reforms. It lays bare the interwoven
A follow up TASC report in 2019 used a case study
nature of how private care is delivered in public
approach to analyse access to autism, lung cancer
hospitals alongside the provision of care to public
and brain tumours.15 That report found clear
patients, thus diverting resources from those waiting
inequities of access to diagnosis and treatment and
for treatment in the public system. This report
long wait times for autism services and no clear
flags the inequities which result from the differing
pathways to diagnosis for brain tumour patients. The
payment models for GPs, consultants and hospitals
report also referenced the National Cancer Registry’s
where payment is a flat rate in the public system,
report which found a higher overall prevalence
while a fee per service model is used for private
of cancer in more deprived populations and that
patients. This dual approach to fee payment results
disadvantaged people were more likely to have other
in perverse incentives and fosters inequalities of
health conditions.16
access and outcome, with public patients in effect
competing against private service users to gain
access to treatment. EAPN Ireland welcomes the
commitment to remove the delivery of private
care from public hospital settings and agrees
with the EU Commission’s 2020 Country Specific
Recommendations for Ireland which state that this
is an “essential” step to achieve the Sláintecare
reforms.12 This document also critiques the reform
progress to date noting that the implementation
remains “vague” and that a monitoring framework
would improve delivery. It recommends in Country
EAPN Ireland Giving Health Inequality a Voice 171.8 Health inequalities - the role of population health care need must dictate resource
geography planning and allocation otherwise health inequalities
will persist.
Geographic variations in availability and access
to health resources play a huge role in people’s EAPN Ireland welcomes the announcement in July
access to health services. Historically the approach 2019 of the six new integrated regional areas (with
to budget allocation has not been based on the a single budget for both community/primary and
level and prevalence of local resulting in different acute sectors) which will use population health data
outcomes dependent on the so-called ‘postcode’ to deliver improved planning and delivery of health
lottery where access differs according to budget and service based on need (see Appendices 2 and 3).
location not need. The timely delivery and resourcing of this structural
reform will be an important enabler in reducing
The ESRI report from July 201917 shows clear health inequalities as real need will be demonstrated
inequalities in supply of all health and social care and resources can be allocated to where they are
services, particularly in the wider Dublin region and most needed.
eastern seaboard area. This report argues that
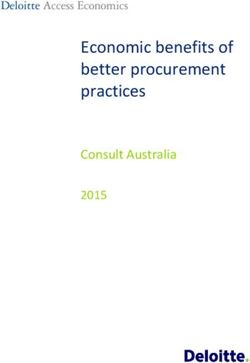
EAPN Ireland Giving Health Inequality a Voice 181.9 Poor capacity and long waiting times Orthodontics: % seen for assessment within 6 months
cause inequalities
100%
Historic underinvestment in primary care, plus the
reduction in services due to austerity measures, 50% 46%
38.5%
has resulted in limited capacity in the public
33.5%
system’s primary and community care services. 0%
This contributes to deepening health inequalities as Q3 Q4 Q1 Q2 Q3
those who cannot afford to buy fast tracked access
Quarter 17/18 Quarter 18/19
to private diagnosis and treatment must endure
long waiting times to access the care they need.
These delays in access are of particular concern, as
Orthodontics: treatment waiting list > four years
many interventions are time sensitive with patients
needing more expensive and complex treatment
20%
later if they do not receive timely interventions. This
is particularly the case in terms of the treatment of 10% 11.3%
children, where delays in accessing time sensitive 6.1%Adult Mental Health - % offered an appointment and seen within 12 weeks
77%
75%
73%
71.1%
70.5%
69%
Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
Month 17/18 Month 18/19
Figure 4. Source: HSE July to September July to September Performance Report
By the end of 2019, there were 7,000 children and relentlessly year on year. In March 2018 the total
teens waiting to see a psychologist, an increase of numbers waiting were 504,111, with 77,547 waiting
20% in one year. In the period 2012 to 2018 there over 18 months.25 In December 2019 there were
was a 24% increase in referrals to the Child and 215,000 children on public waiting lists (hospital and
Adolescent Mental Health Teams, with 2,327 waiting community services) with over one in four waiting
at the end of 2019. over a year for treatment. The breakdown of these
figures show discrepancies in waiting numbers and
In December 2019 there were 19,000 children times which varies significantly region to region
waiting for speech and language therapy in the and hospital to hospital depending on their specific
public health system, with 2,000 waiting more than budget allocation.26
a year and 300 waiting more than two years. North
Dublin had the highest volume of children waiting The ongoing problem of long public waiting lists
at 2,400, while there were none waiting in Dublin as a major cause of health inequalities of access
South East, and ten waiting in Dún Laoghaire.23 and outcome has been noted by the OECD, the
These figures reveal the ongoing variation based on European Observatory on Health Policies and
geography not need with people living in different Systems and also the European Commission.
parts of the same city experiencing very different In its 2020 Irish Country Report the European
waiting times. These delays cause severe difficulties Commission states that substantial investment
for children who must struggle with difficulties which is needed to achieve the Sláintecare mission of
affect all aspects of their lives, not least their ability universal access to healthcare.27 The Health at a
to participate in school, while families who can afford Glance 2019 report identifies high bed occupancy
the cost of private therapist care receive timely rate (at 95% much higher than the EU average of
treatment and have better outcomes. 77%) and high levels of hospitalisation for conditions
which should be treatable in community settings as
The numbers waiting for treatment in public the major causes of long waiting times for elective
hospitals puts the divide between those who surgery alongside legacy low investment in capacity
can afford private care in sharp relief with those in the public system.28
who cannot. In January 2020 there was a total of
556,770 people on waiting lists for treatment in
public hospitals, with 107,040 waiting over eighteen
months.24 These numbers have been increasing
EAPN Ireland Giving Health Inequality a Voice 202 http://www.irishstatutebook.ie/eli/cons/en/html#part14 16 Walsh PM, McDevitt J, Deady S, O’Brien K & Comber H (2016) Can-
cer inequalities in Ireland by deprivation, urban/rural status and age:
3 United Nations, 2000. Committee on Economic, Social and Cultural a report by the National Cancer Registry. National Cancer Registry,
Rights Twenty-second session General Comment No 14. Geneva. Cork, Ireland. Available at: https://tinyurl.com/y39ojn2w [Accessed
Available at: https://tinyurl.com/y7ub5s3f [Accessed 12th March 16th February 2020].
2020].
17 Smith, S., Walsh, B., Wren M A., Barron, S., Morgenroth, E., Eighan,
4 The 2017 study by Maev Ann Wren and Sheelagh Connolly “Unmet J., and Lyon, S. (2019). Geographic Profile of Healthcare Needs and
healthcare needs in Ireland: Analysis using the EU-SILC” found that Non-Acute Healthcare Supply in Ireland. Dublin. ESRI. Available
59% said that the reason they did not access required health care at: https://doi.org/10.26504/rs90 [Accessed 10th February 2020].
was because of the cost. Data on ten public health services were studied, using 2014 data:
GPs, Community Nurses, Public Occupational Therapists, Speech &
5 CSO. (2019). Mortality Differentials in Ireland 2016-2017. Dublin. Language Therapists, Podiatrists, Counsellors & Psychologists, Social
Available at :https://tinyurl.com/y67grm4u [Accessed 12th March Workers, Public Home Care Hours and both and private physiothera-
2020]. pists and nursing home beds.
6 CSO. (2017). Mortality Differentials in Ireland 2016-2017. Dublin. 18 CHOs are community healthcare services outside acute hospitals,
Available at: https://tinyurl.com/y67grm4u [Accessed 12th March such as primary care, social care, mental health, and other health
2020]. and well-being services. These services are delivered through the
HSE and its funded agencies to people in local communities, as close
7 ESRI Research Bulletin. Sheelah Connolly and Maev-Ann Wren. as possible to their homes.
Unmet Healthcare Needs in Ireland. Dublin. ESRI. Available at:
https://tinyurl.com/y39qql9z [Accessed 13th March]. 19 https://www.cso.ie/en/statistics/health/hsefundeddentaltreat-
ments/ The numbers treated fell from 1,227,000 to 1,025,600.
8 Johnston, B., Burke, S., Barry, S., Normand, C., Ní Fhallúin, M.,
Thomas, S 2019. Private health expenditure in Ireland: Assessing 20 https://www.cso.ie/en/releasesandpublications/ep/psilc/surveyon-
the affordability of private financing of health care. ScienceDirect, incomeandlivingconditionssilc2017/healthmodule/
Volume 123, Issue 10, October 2019, Pages 963-969. Available at:
https://doi.org/10.1016/j.healthpol.2019.08.002. This study defined 21 HSE. (2017) Primary Care Eye Services Review Group Report.
households which spend over 40% of their budget (or capacity to Dublin. Available at: https://tinyurl.com/y6sgjpd5 [Accessed 9th
pay) on catastrophic health spend as being pushed into poverty or February].
having an unaffordable need.
22 https://www.hse.ie/eng/services/publications/performancere-
9 CSO. (2017). Survey on Income and Living Conditions (SILC) 2018. ports/july-to-september-quarterly-report.pdf
Available at https://tinyurl.com/y386ovgo [Accessed on 16th March
2020]. 23 https://www.rte.ie/news/ireland/2019/1206/1097362-chil-
dren-waiting-lists/
10 CSO. (2017). Survey on Income and Living Conditions (SILC) 2018.
Available at: https://tinyurl.com/y386ovgo [Accessed on 16th March 24 https://www.ntpf.ie/home/pdf//2020/01/nationalnumbers/out-pa-
2020]. tient/National01.pdf
11 WHO and European Observatory on Health Systems and Policies. 25 https://www.ntpf.ie/home/pdf/2018/03/nationalnumbers/out-pa-
(2014). Health system responses to financial pressures in Ireland tient/National01.pdf
(Studies Series 33). Denmark. Available at: https://tinyurl.com/y5v-
vprh8 [Accessed 25th February 2020]. 26 https://www.rte.ie/news/ireland/2019/1206/1097362-chil-
dren-waiting-lists/
12 European Commission. (2020). COUNCIL RECOMMENDATION
on the 2020 National Reform Programme of Ireland and deliver- 27 European Commission. (2019). COMMISSION STAFF WORK-
ing a Council opinion on the 2020 Stability Programme of Ireland. ING DOCUMENT. Country Report Ireland 2019. Brussels. https://
Brussels. Available at:https://tinyurl.com/yyd5j2hn [Accessed 6th May ec.europa.eu/info/sites/info/files/file_import/2019-european-semes-
2020]. ter-country-report-ireland_en.pdf
13 Buffel, Veerle & Nicaise, Ides. (2018). ESPN Thematic Report on 28 https://www.slideshare.net/OECD_ELS/health-at-a-glance-2019-
Inequalities in access to healthcare Belgium. Available at: https:// chartset
tinyurl.com/yx9zb3dq [Accessed on 14th February].
14 Forster,T., Kentikelenis, A., Bambra, C. (2018). Health Inequalities
in Europe: Setting the Stage for Progressive Policy Action. Dublin.
TASC FEPS. Available at: https://tinyurl.com/yxvvhys4 [Accessed 15th
February 2020].
15 Doyle, K., Forster, T., Kentikelenis, A., Legido-Quigley, H.,Torrecilla,
M. (2019). Reducing Health Inequalities: The Role of Civil Society.
Dublin. TASC FEPS. Available at: https://tinyurl.com/y2o7jjjr [Accessed
16th February 2020].
EAPN Ireland Giving Health Inequality a Voice 2102
Social Determinants
of Health - their role in
health inequalities
2.1 Is Healthy Ireland reducing health inequalities?
2.2 Are health inequalities addressed in Sláintecare?
2.3 Co-creation and a health inequalities index to improve
citizen outcomes in Healthy Ireland and Sláintecare
EAPN Ireland Giving Health Inequality a Voice 22There is now a compelling body of research which — Bring the majority of care into the community
shows that the social determinants of health have
— Create an integrated system of care, with
a very strong causal effect on health outcomes
healthcare professionals working closely
and status. The seminal report by the World
together
Health Organisation’s Commission on the Social
Determinants of Health framed the challenge of — Drive accountability and performance in the
health inequality through the lens of ethics and health service
social justice. Three principles of action were
recommended: — Deliver a health service that has the capacity and
ability to plan for, and manage, changing needs
1. Improve the conditions of daily life – the
circumstances in which people are born,
grow, live, work, and age. 2.1 Is Healthy Ireland reducing health
inequalities?
2. Tackle the inequitable distribution of power,
money, and resources – the structural drivers EAPN Ireland is very aware that Goal Two of the
of those conditions of daily life – globally, Healthy Ireland Framework for Improved Health
nationally, and locally. and Wellbeing 2013 - 2025 is to reduce health
inequalities. This strategy acknowledges that “health
3. Measure the problem, evaluate action, expand
and wellbeing are not evenly distributed across Irish
the knowledge base, develop a workforce that
society” and that
is trained in the social determinants of health,
and raise public awareness about the social This goal requires not only interventions to target
determinants of health.29 particular health risks, but also a broad focus on
addressing the wider social determinants of health
This section of the report looks at how the two
– the circumstances in which people are born, grow,
parallel, but not interconnecting, health strategies -
live, work and age - to create economic, social,
the Healthy Ireland Framework for Improved Health
cultural and physical environments that foster
and Wellbeing 2013 - 2025 and Sláintecare, seek to
healthy living. 30
address health inequalities in Ireland. The former
is a citizen facing strategy which seeks to engage Health inequalities are clearly defined in this
with individuals and communities to take personal framework (p.7) as the
responsibility for their health status and to empower
them to make behaviour and lifestyle changes to differences in health status or in the distribution of
improve their health. The latter is the ambitious ten health determinants between different population
year blue print for transformation of the Irish health groups due to the conditions in which people are
system which aims to deliver universal single tier born, grow, live, work, and age
health care. Its objectives are:
The framework goes on to state that decreasing
— Promote the health of our population to prevent health inequalities will deliver positives for society
illness and that socially targeted interventions are needed
which tackle the specific needs of at-risk groups.
— Create a system where care is provided on the The importance of reporting relevant data at
basis of need, not ability to pay geographic levels to facilitate population health
planning is also noted.
— Move the system from long waiting times to a
timely service
EAPN Ireland Giving Health Inequality a Voice 23The emphasis in Healthy Ireland is on the delivery disadvantaged lives. Placing the eradication of
of outputs; projects, initiatives and programmes health inequalities within a behavioural lifestyle
which are dependent on a willingness and ability by strategy, namely the Healthy Ireland Framework, is
the population to engage in activities which achieve aspirational but unrealistic for low income groups
positive behaviour and lifestyle changes. There is an as it does not address the root cause of their
abundance of actions being delivered countrywide predicament, structural disadvantage, which results
which seek to engage individuals and communities from distribution choices and explicit resource
in behaviour change to improve their health and restriction in the public health system.
wellbeing. These outputs are delivered in a variety
The lives of people experiencing disadvantage are
of ways and platforms across different sectors. Each
very often consumed with the struggle to deal with
HSE Community Healthcare Organisation has its own
the barriers they experience in accessing basic
Healthy Ireland implementation plan, while there are
resources. If a household or individual does not
also regional and county level plans.
have adequate income, housing, are struggling
Despite the plethora of projects and programmes with access to health or education, have literacy
in this framework, EAPN Ireland remains convinced issues, are find themselves in a challenging legal
- through its decades of direct working with people status, their motivation and capacity to engage with
experiencing different types of disadvantage - that a lifestyle changing programme is limited or non-
engaging in initiatives focusing on behaviour and existent. They simply do not have the space, energy
lifestyle change to improve health outcomes and or motivation to opt into self-actualising actions
status is not, and cannot be, a priority for vulnerable which depend on personal responsibility.
groups.
EAPN Ireland considers that Healthy Ireland cannot
Approaches targeting behaviour change, where deliver on its goal to reduce health inequalities
people take personal responsibility for their by providing behaviour and lifestyle change
wellbeing, works for some people. It is unrealistic, interventions alone as people experiencing health
however, to expect this approach to be effective inequalities are largely outside the reach of these
for the majority of households living precarious actions and cannot engage with these activities.
EAPN Ireland Giving Health Inequality a Voice 24You can also read