PATIENT SAFETY AND QUALITY IMPROVEMENT LEAD PROGRAMS - Project Summaries 2017-2018
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

PATIENT SAFETY AND QUALITY IMPROVEMENT LEAD PROGRAMS Project Summaries 2017-2018
© The Australian Council on Healthcare Standards Apart from any use as permitted under the Copyright ACT 1968, no part may be reproduced by any process without prior written permission from the Australian Council on Healthcare Standards. Patient Safety Lead Program and Quality Improvement Lead Program Project Summaries 2017-2018 IBSN: 978-1-921806-98-8 (Paperback) ISBN: 978-1-921806-99-5 (E-book) This booklet is available in PDF format via the ACHS website: www.achs.org.au To order a print copy, please contact Communications at: The Australian Council on Healthcare Standards 5 Macarthur Street Ultimo NSW Australia 2007 T. 61 2 9281 9955 F. 61 2 9211 9633 E. communications@achs.org.au www.achs.org.au Editor - I. McManus Designer - C. Party
Contents Foreword 5 Our two lead training programs 6 Patient Safety Lead Program 9 Communication in the age of innovation 10 Review of medication processes in the general medical ward of Beaudesert Hospital with the aim of reducing administration errors 12 Reducing the paperwork: Giving the nurses back to their patients 14 Standardisation of the hospital mortality and morbidity system 16 Multi-resistant organism (MRO) discharge swab compliance improvement project 20 Reducing catheter-acquired urinary tract infections in surgical patients 24 Exploring paediatric inter-hospital transfers across the health service to identify and raise awareness of the clinical risks 26 Quality Improvement Lead Program 31 Impact on service access of an online program for persistent pain management 32 Improving the survey report review process of the Australian Council on Healthcare Standards 36 Review of quality auditing at the Mackay Hospital and Health Service, Queensland 38 Prevention of inadvertent perioperative hypothermia 42 Clinician-led project to reduce in-hospital falls 44 Raising overdose awareness 46 Supporting and partnering with women who decline recommended maternity care 48 Human Services Standards accreditation improvement project 2017 52 Improving the surveyor workforce reappointment process 54 Reducing unplanned readmissions
ACHS Improvement Academy | Project Summaries 2017-2018
ACHS Improvement Academy Faculty for Patient Safety
and Quality Improvement Lead Training Programs
The Improvement Academy would like to acknowledge the contribution of the following Faculty
members who contributed to the success of these programs and the resulting projects contained
in this booklet :
Australian and NZ Expert Faculty International Experts via video
Ms Bernie Harrison - Director ACHS and webinar
Improvement Academy, NSW Dr Brent James - Chief Quality Officer
Dr Cathy Balding - Managing Director of Intermountain Health Care Utah USA
Qualityworks PL, VIC Prof Maxine Power Director of Innovation and
Ms Helen Eccles - ACHS Consultant Assessor / Improvement Science, Salford Royal NHS
Educator, NSW Foundation Trust and Managing Director of
Haelo, UK
Ms Helen Ganley - Principal Data Sanity, NSW
Dr Lynne Maher - Director of Innovation, Ko
Awatea, Auckland
Dr Mark Burgess Project Office, ACHS, NSW
Mr Peter Hibbert - Program Manager,
Australian Institute of Health Innovation,
Dr Tim Smyth - Practice Principal, Health
Sector Law, NSW
4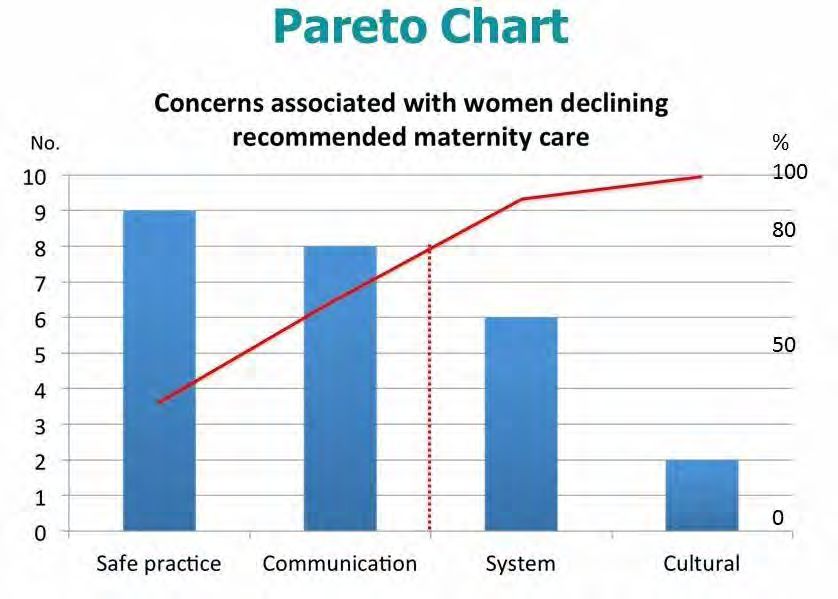
Foreword
Foreword
I am delighted to write this foreword It is important to remember that
for the second ACHS Improvement many people have contributed to
Academy Patient Safety Lead and the Academy’s success since it was
Quality Improvement Lead Program launched, and I wish to personally
Project Summaries booklet, for thank the Academy’s Faculty, and
projects undertaken during 2017 its Director, Bernie Harrison, who
and 2018. have all contributed and shared their
knowledge and expertise.
With the publication of the inaugural
edition of the booklet last year, a We live in an era of ever-expanding
platform was created that allowed knowledge creation, and with it
the many exciting projects achieved some responsibility to ensure new
by graduates to be published and knowledge is put to good purpose.
available to a broader audience.
Whether it is the sharing of lived
The response from those considering experiences, problem-solving or
undertaking a Lead Course when determining a new way forward
seeing the booklet was recognition when the status quo has been around
that the weight of achievement forever, the Improvement Academy’s
from the two respective programs lead Training programs have a very
was certainly worth the level of definite goal. Their aim is to ensure
investment required. participants are exposed to learnings
that are grounded in a specific
The scope of the different projects
framework but are also inventive
undertaken by the two Lead programs
when making a world of difference
is an indication of the reach the
to delivering patient quality and
Improvement Academy has had
safety ideas.
throughout the Australian healthcare
industry, and indeed, for this year – At ACHS we are very proud of what
beyond our shores. has been achieved in a relatively
short period of time with the
Program participants run the gamut
Improvement Academy and trust
of clinicians and quality and safety
that this booklet will impress readers
managerial positions from large
with contemporary health education
metropolitan hospitals to smaller rural
offerings that meet international
and remote services and everything in
best practice in the field of quality
between. This year the complexity of
and safety.
projects has been just as varied as with
the first year, and the core principles of
quality improvement science continue
to underpin the courses.
Dr Christine Dennis
Chief Executive Officer, ACHS
October 2018
5
ACHS Improvement Academy | Project Summaries 2017-2018
Our two lead training programs
The training programs are provided perioperative hypothermia, reducing
predominantly by an Australian- in-hospital falls, raising accidental
based faculty who are recognised overdose awareness, supporting
internationally as experts in the field women who decline recommended
of quality and safety, combining both maternity care, and reducing
practical experience and publication unplanned readmissions
Our two lead training programs
7
ACHS Improvement Academy | Project Summaries 2017-2018
“It has helped me look at things differently and formalising improvement science in day-to-day activities.”
Ajay Valayudhan, Freemantle HS WA
“I liked the diagnostics, there are all these thoughts going through my head on how to improve things with the
key learnings. I like that you can show people how you’ve made your improvements.”
Dianne Conlon, Beaudesert Hospital, WA
“Learning about all the human factors involved in quality improvement science and why projects can fall
over. As well as the ability to network with like-minded people and have my eyes opened to international best
practice, not just my own health service or the state.”
Catherine Frame, Towoomba Hospital, QLD
“The most important thing for me was learning about the diagnostic causes, which is something I can apply
to my ideas. It is being able to show people the problem and share it with different groups, and this course has
given me the opportunity to see that different approaches are possible.”
Ami Horne, Redcliffe Hospital, Brisbane
“Being able to apply a strategic diagnosis to a set problem, and having a process to work through it. I already
have those skills, but now have a better framework to use for a whole service.”
Clare Thomas, Sunshine Coast
“The value of learning improvement methodology processes, how reliability science principles impact on safe
patient outcomes and what happens when methodology isn’t applied. Also, how this can impact on changing
behaviour and culture in the workplace?”
Catherine Manns, Darling Downs, QLD
“As an experienced Quality Lead, this course was a great opportunity to revisit and reinforce theory, and
keep up-to-date with contemporary learnings, to consolidate my practice in embedding quality and safety
initiatives. The course provides a robust framework and strengthens the rationale behind what you need to
do, and why. My advice is to undertake a project currently planned as part of your role – the course was very
helpful in achieving my project’s outstanding results.”
Catherine Ryan, Private Royal Brisbane Women’s Hospital
“I learnt an awful lot, my interest in patient safety and quality has always been there, but I have not worked
in the area. This course has allowed me to link everything together and given me the space to practice. It has
been absolutely invaluable and I would recommend it to anyone.”
Julie Wantling, POWH, Metro North
“I was most excited about the research already completed, the way the data was collected and presented was
advanced leaving no doubt as to the results. Will be introducing these systems to my service.”
Tracy Johnston, Central Queensland Health Service
8
Patient Safety Lead Program
Patient Safety Lead Program
Project Summaries
About the Patient Safety Lead Program
The Patient Safety Lead Training Program (PSL) has been designed for senior staff within healthcare organisations who
lead patient safety activities including: root cause analysis, design of recommendations that lead to improvements in
patient safety, open disclosure, and legal and governance responsibilities for patient safety.
This 12 month program provides practical skills and theories that can be translated back into the workplace.
Participants will have an immersion in the patient safety literature and contemporary approaches to organising for patient
safety. This course will focus on the proactive design elements to reduce risk of harm from health care including: human
factors engineering and reliable design principles and will draw on concepts from other industries which are recognised as
having high reliability e.g. mining, nuclear power and aviation.
It will also provide insights and understanding from studies of patient safety and successful healthcare examples in
building safe and reliable care.
Patient Safety Lead graduation ceremony, held on 17 November 2017 in Sydney
Patient Safety Lead graduation ceremony, held on 23 April 2018 in Brisbane
9
ACHS Improvement Academy | Project Summaries 2017-2018
Communication in the age of innovation
Background ‘communication breakdown’ has been
highlighted in root cause analysis
Retrieval Services Queensland (RCA). This project reviewed the
(RSQ), Queensland Health, is a culture of internal communication,
major component of aeromedical in relation to patient safety, within
retrievals and disaster management. a rapidly growing and evolving
RSQ provides clinical coordination aeromedical hub. This was in
for the aeromedical retrieval and conjunction with the introduction of
transfer of all patients from parts of an on-line clinical and logistics record
northern New South Wales to the system, ‘Brolga’, in October 2017.
Torres Strait. Specialist medical and
nursing coordinators in paediatric,
neonatal and high-risk obstetrics
Measures
support the clinical coordination Data were collected through monthly
of these patients by road in staff-initiated audit requests
metropolitan areas of Queensland. (March – November 2017), a staff
RSQ is also responsible for the communication improvement survey
statewide clinical and operational (November 2017), and pre- and
Catherine Beavis leadership and governance structure post-Brolga surveys (October and
Patient Safety Officer of Queensland Health’s specialised December 2017).
Retrieval Services Queensland and contracted retrieval services
and aeromedical transport providers Design
across the state, ensuring whole-
of-system performance monitoring The project focused on audit
and subsequent policy and system notification and staff communication
enhancement and development. processes. High-order flow charts,
cause-and-effect diagrams and two
surveys were conducted.
Problem/Aim
The following interventions have been
RSQ started the centralised
introduced:
aeromedical hub for Queensland.
Despite communication being the • a monthly safety huddle including
critical feature of the organisation, the patient safety officers from RSQ
internal and external communication and the service providers on
pathways were not formally teleconference for 30 minutes
developed. The main reasons for to raise cases for discussion and
this were rapid expansion, few quickly gain information – this
management staff responsible for was a sub group formed from the
many aspects of the service, and Statewide Integrated Governance
a developing safety and quality Meeting (STIG), where all service
framework. Current literature providers meet to discuss
reiterates the improvement of pertinent clinical governance
organisational culture in the delivery matters.
of safe, reliable patient care and • the RSQ Management Morning
improving safety outcomes. In Huddle – every Monday, a
addition, effective, reliable and safe dynamic, stand-up Huddle is
communication is a foundation conducted via videoconference
of patient safety. Repeatedly, with RSQ’s Townsville office, to
10Patient Safety Lead Program
ensure all senior management • safety huddles during the day shift engagement and an ongoing stability
are able to brief each other about to improve situational awareness in staff notification of cases for
their work, current operational • formation of the Christmas Party audit. At every organisational level,
issues and forward plans. Committee. this initiative has moved RSQ from
• a weekly staff forum. Developing an authoritative to more affiliate
and successfully implementing Results leadership and team style, which is
this forum has been the most more inclusive and transparent and
critical stage leading up to the RSQ staff notification of potential cases allows staff to present ideas, identify
launch of Brolga. This forum has for audit remained steady over the issues and provide solutions.
been used as the main source project period. Results demonstrated
of information dissemination no change in compliance, but this Next steps
regarding Brolga. It has a scope of has recently improved with the
introduction of an electronic records RSQ’s future plans include:
operational, educational, patient
safety and ‘round table’, and has system. Interventions around RSQ • further implementation of
included topics such as wellness internal communications have current quality management and
and emotional intelligence, giving succeeded and a future benefit is the improvement process to transition
staff more personal skills to utilise potential increase in notifications, from incident management
at RSQ and better understanding particularly with the introduction of to outcomes-focused quality
of the challenges it faces. online medical records. improvement
Other interventions to assist in this • maintaining and improving staff
Conclusion communication processes gained
improvement project include:
This project’s aim to create a more from outcomes of the project’s
• formal debriefing to respond to cohesive, engaged workforce at all data
the effect of telehealth on RSQ levels has succeeded. Six months of • moving towards a more innovative
staff highlighted in 2017 and first interventions have demonstrated and research-driven organisation.
conducted on 31 October an increase in staff satisfaction and
11ACHS Improvement Academy | Project Summaries 2017-2018
Review of medication processes in the
general medical ward of Beaudesert
Hospital with the aim of reducing
administration errors
Background Within the next cycle of review of
the environment of the medication
The Australian Commission on room, a move to electronic medical
Safety and Quality in Health Care records was planned and workflow
(the Commission) has published reviews took place for all frequent
abundant resources about elements nursing tasks. This was the ideal
of medication safety to keep opportunity to review draft electronic
patients safe. workflow processes against the
recommendations of the Commission
Problem/Aim outlined in Electronic medication
Beaudesert Hospital is the rural management systems: A guide to safe
hospital of the Logan Bayside Health implementation (3rd edition). The
Network. Reported medication errors team identified the key issue of access
were increasing and were higher than to computers within the medication
the statewide average in the winter of room as a barrier. With only one
2016. computer it was not possible to match
the current processes to the draft
Measures workflows of the electronic medical
Dianne Conlon record. In addition overcrowding of
Administration tasks were reported the medication room environment
Clinical Nurse Consultant Quality as the highest category of issue with was present again as a result o only
and Patient Safety 41/85 = 48% of reported incidents from one computer being available for use.
Beaudesert Hospital, Metro South August 2017 to February 2018. The Patient care was, as a result, delayed
Health, Queensland human factors elements of medication as only one nurse was able to prepare
selection in the environment of a busy medications against the electronic
medication room were identified as record at any time.
the key elements for improvement
by the project team to reduce Further team brainstorming occurred
medication errors. in the review of the draft electronic
workflow processes to find solutions.
Taking the medications to the
Design lockable individual patient bedside
In the first cycle of review, the team cabinets was identified as a solution
identified changes to the medication to altering the environment of the
room environment as a solution to medication room. The medication
combat errors in drug selection. A boxes were selected on admission by
‘zone of silence’ was instigated, and the registered nurse against the order
nursing staff members preparing on the electronic medical record in the
medications were requested to wear medication room, taken to the bedside
‘DO NOT DISTURB’ vests to identify and locked in the patient’s bedside
them to other team members to cabinet. The medications were near
discourage disruptions. These were the patient, and the nurses had access
infrequently used and other strategies to the electronic record where they
were brainstormed by the team. were preparing medications at the
12Patient Safety Lead Program
bedside and would not need to crowd were identified as cost and patient Conclusion
the medication room at any time. movements.. The cost was associated
Selection errors were detected as with an increase in amount of The implementation of electronic
some medications were suitable to be medication boxes available in the medication records, review of the
scanned for reconciliation against the medication room for dispensing to environment of the medication
prescription prior to administration to patient bedside cabinets; however, room, and allocation of medications
ensure that they were accurate. the same amount of medications to the patient bedside cabinets are
would be consumed overall. The risk all strategies that have significantly
of incorrect medications available in reduced medication administration
the bedside cabinet especially when errors. These initiatives in the
patients were discharged or moved to digital environment continue to be
different allocated bed areas was also monitored, reviewed and modified
identified as a risk for implementation to ensure that the processes are
of the strategy patient centred and efficient for
nursing staff caring for patients. These
initiatives are improving medication
Results administration processes, thereby
Medication administration from the having a positive influence on reducing
lockable bedside cabinets using avoidable patient harm as an outcome
the electronic medication chart of health care at Beaudesert Hospital.
was implemented in January 2018.
Initial clinical incident reports Next steps
show a reduction in medication
administration errors for January– Optimisation of these strategies
Barriers to the implementation of this March to 11/38 = 29%. (especially on admission, allocated
strategy for process improvement bed area movements and discharge)
are in progress. Promotion of these
improvements will be conducted
at Medication MAYhem month (May
in-service calendar) and through the
network Medication Safety Committee.
13ACHS Improvement Academy | Project Summaries 2017-2018
Reducing the paperwork: Giving the nurses
back to their patients
Background Measures
Accurate documentation is necessary Initial data collection was conducted
for communication and the delivery through an observational audit over
of safe, quality patient care. However, a shift to gain a ‘snapshot’ of the
nurses have to complete increasing challenges. This revealed that 40–60
amounts of documentation to minutes were required to complete
not only direct patient care but the documentation, with at least 10
also demonstrate compliance at forms completed and duplication of
audit and aid in receiving quality key patient information across six
incentive payments. different forms.
Catherine Frame A template was used to label each form
Problem/Aim with time taken for completion, type of
Nursing Director Clinical
Toowoomba Hospital day surgery procedure being undertaken and the
Governance
unit (DSU) admits and discharges RN years of experience in this clinical
Darling Downs Hospital and Health on average 20–25 patients per day setting. The audit studied the suite
Service, Queensland plus emergency presentations. of documents in the audit and the
Documentation required for the type of duplication across the forms,
admission process can be upwards of quantifying the documentation burden
Left to right: Nursing Director Clinical placed on staff.
10 different forms, all with multiple
Governance – Catherine Frame and Nurse
Unit Manager at the Day Surgery Unit –
pages. As a consequence of increased
Craig Harrower documentation requirements, the Design
DSU has been forced to increase
The planning phase focused on:
its approved registered nurse (RN)
hours by a minimum of two full-time • audit of existing processes
equivalents per week for the last 3 • focus groups
years. This increase was required to • formulation of a documentation
complete the six necessary admissions admission model.
by 7.30 am, critical for ‘start on time’
and maximising theatre utilisation The main interventions were
in line with the hospital and health implemented using Plan-Do-Study-Act
service key performance indicators. (PDSA) cycles:
This equates to approximately 20 • remove all inpatient-based
hours of admitting time required documentation from the DSU
prior to midday to ensure theatre admission model
commences on time for both morning
and afternoon lists. This project aimed • educate DSU nurses on the new
to reduce the burden of paperwork in model
the DSU by removing duplication and • audit schedule against the
in turn increase direct nurse–patient new process, inclusive of
care by 20% within 6 months. documentation
• review clinical incident data in
alignment with the audit schedule.
14Patient Safety Lead Program
Results Conclusion Next steps
The main priorities are to ensure safe Reducing clinical documentation by Phase 2 commenced in May 2018
patient care and accurate clinical eliminating duplication, ensuring with a review occurring at two of
documentation while: that it is specific to the service the seven rural surgical facilities.
being delivered, is an important and The review identified an existing
• reducing documentation
practical option to improve staff streamlined documentation process
duplication
satisfaction and patient flow, and at both rural facilities comparable
• increasing nurse–patient care time reduce the need to increase nurses in to that implemented at the DSU in
• ensuring documentation is any clinical setting. The project was Toowoomba. However, patient flow
appropriate to the service being able to deliver on expected outcomes issues were identified at one of the two
delivered. at no cost to the delivery of quality and sites because of ageing infrastructure,
safe patient care. This improvement which will require further exploration.
Five months after intervention
project was not without its challenges The remainder of the rural surgical
completion, an observational audit
because of age-old mindsets and sites will be reviewed over the coming
revealed that the changes had resulted
significant changes to practice. months to determine which, if any,
in a reduction of 44% in time to
However, the outcomes will ensure implementation from the Toowoomba
complete required documentation,
that these changes continue and Hospital DSU project is required. The
equating to 6 hours of nursing
spread throughout the health service. entire project is due for completion by
documentation time being saved per
These outcomes have streamlined December 2018.
24 hours, and a continued reduction in
documentation and reduced
reported clinical incidents.
workloads that detract from nurse–
patient care time.
15ACHS Improvement Academy | Project Summaries 2017-2018
Standardisation of the hospital mortality
and morbidity system
to NSW health policies and legislation
and there is no rationalisation about
how clinicians should select cases
and what specific format should be
utilised. There are suggestions for case
selection and which data should be
reviewed, such as clinical incidents
where harm was sustained.
Australia has developed a consensus
list of hospital-acquired complications
(HACs) that attract penalties as a
forcing function to reduce the number
of adverse events and improve the
quality of care provided. Significant
resources are deployed to ensure
that the health system supports
the continued good health of
Australians, but despite this effort, an
unacceptable portion of Australian
Anne-Marie (Ami) Horne Background hospital admissions is associated
with an adverse event. One in every
Patient Safety Officer A morbidity and mortality (M&M) nine people admitted to a hospital in
Redcliffe Hospital, Metro North meeting is a regular conference held Australia develops a complication. (1
Hospital and Health Service by an interdisciplinary team in a ) Reviewing all deaths, complications
hospital, and involves peer review and adverse events ensures that HACs
and discussion of issues that occurred undergo scrutinisation and that quality
during the care of a patient, including improvement activities are developed,
adverse events, a complication or and lessons learnt and shared, across
death. The primary purpose of an the facility, thus improving patient
M&M meeting is to allow learning from care and reducing the incidence of
issues by modifying judgment and complications and the severity of
clinical decision-making to prevent adverse events.
the repetition of these events and to
improve patient care. The M&M review
also provides the opportunity to share
Problem/Aim
good practices. Redcliffe Hospital has 256 beds. The
Emergency Department sees an
In 2016, the New South Wales Clinical
average of more than 160 patients
Excellence Commission published a
per day and 20% of patients seen
guideline for the conduct and report
are admitted.
of M&M meetings, which outlined
the key principles and features of an There was a varied processes for
M&M meeting; however, this relates M&M reviews at Redcliffe Hospital.
16Patient Safety Lead Program
Although there was an M&M review • 100% of the clinical areas have Design
process in place, there was a varied scheduled meetings planned for
level of maturity and significant 2018 within four months, A quality improvement (QI) team was
variation including membership, formed consisting of the patient safety
• minutes from the M&M meetings officer, data analyst, director of safety
scheduling, data reviewed, selection
are tabled at the PSC within and quality, mortality and morbidity
of cases, lessons learnt and quality
six months. clinical nurse, clinical director of
improvement plans.
surgery service line and director of
All deaths were reviewed, according Measures medical service (DMS).
to the key performance indicator
(KPI) set by the local health service, Ten clinical departments were A literature review was undertaken
within 14 days after death. There identified to participate in the new to examine M&M review procedures.
was a Death Review Committee; its M&M review project. Four of these There was consensus on what
members reviewed all the deaths, had a process and regular meetings, information should be reviewed in
however, the review of morbidity was either monthly or quarterly. Of the the M&M review process but limited
variable across the system. The death other six, two did not have an M&M information regarding case selection.
review model at the time was clinician review process and occasionally joined
Engagement commenced with each
dependant, as the documentation the other services to participate. In
clinical department director or
had limited structure and was open addition, two other departments were
chairperson of the established M&M
to interpretation. The governing identified during the gap analysis.
review processes. Meetings were held
committee was reviewed, and it was The following issues were identified: to identify the current processes, data
determined that a Quality Assurance currently reviewed and type of data
• Documentation was not
Committee was needed. The Patient which can be provided, and type of
standardised.
Safety Committee (PSC) was deemed documentation utilised.
the most appropriate committee to • Minutes were not collated, to a
central forum Discussion with the QI team, as well as
take over this role.
compiling a cause-and-effect diagram
• There were no TOR.
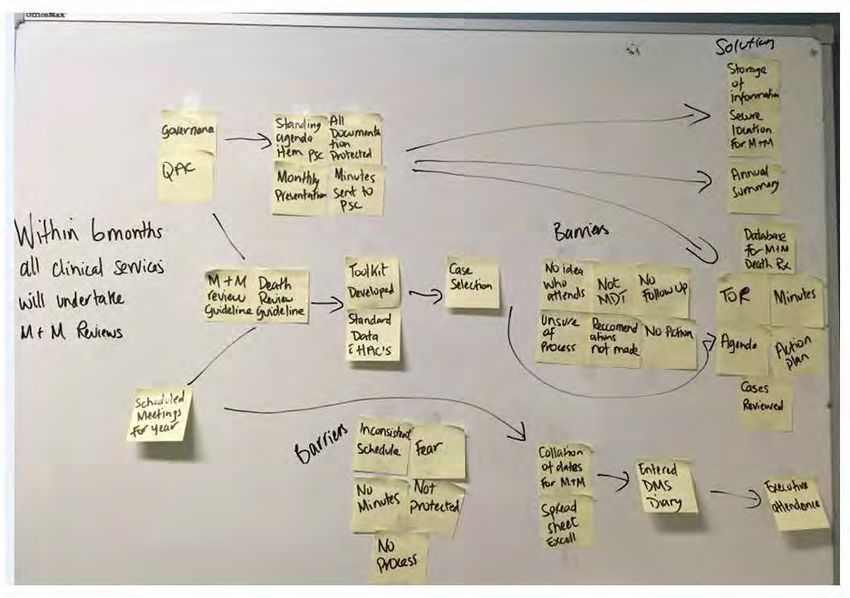
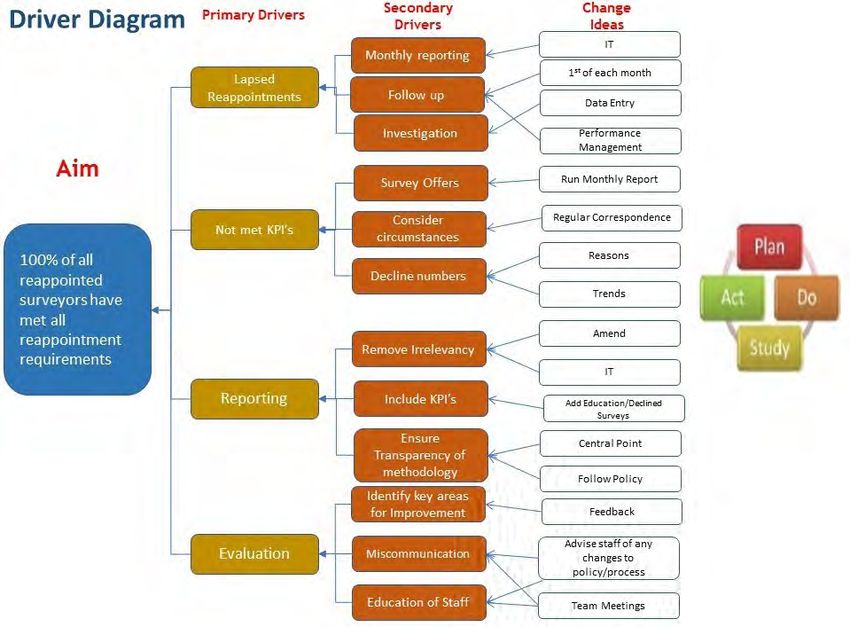
This project aimed to ensure that: and a driver diagram, assisted with
• There was no standardised development of an action plan. The
• M&M and death review guidelines approach for case selection; cases
are developed and endorsed plan consisted of the development of
were often selected according to guidelines for M&M and death reviews,
within three months, clinician preference rather than a toolkit, a dataset including HACs,
• a toolkit is developed and specific criteria. and a schedule of meetings for each
endorsed within two months, • There was a need for more clinical department and presentations
• commencing in January 2018, transparency of shared learnings at the PSC.
each clinical service will present • Death reviews were not always After the guidelines were drafted,
on monthly rotation at the PSC completed within the 14-day KPI. feedback was sought and changes
(governing committee), • The death review form was not made, and the guidelines have been
• 100% of the clinical services have contemporary endorsed and published. Review of
a ‘terms of reference’ (TOR) within the coded data for complications, with
three months, inclusion of the HACs, has provided
criteria for case selection for inclusion
in the M&M review meetings.
17ACHS Improvement Academy | Project Summaries 2017-2018
All of the M&M review reports are Ongoing communication and benchmark reports. Complications are
prepared for submission to a Quality attendance at the M&M review being recorded in the clinical incident
Assurance Committee. meetings ensures that the process management system, and often an
is followed, that lessons are learnt interdepartmental review has occurred
Communication occurred in person
and shared within the team, and that prior to a request for information from
and follow-up either in person or
actions are documented and followed the executive team.
via email; this was vital to ensure
up at the next meeting. Every month,
that all services were involved and Plan-Do-Study-Act (PDSA) cycles were
the chairs and clinical directors receive
were able to provide feedback and used to trial the interventions and
an automated list of complications,
that assistance was offered with the assess compliance with undertaking
HACs and health round table (HRT)
transition to the new documentation. the M&M review process. Review of
18Patient Safety Lead Program
the baseline data in November 2017 • The toolkit has been developed Conclusion
indicated that four out of the 10 clinical and is being utilised.
departments had had an existing The new standardised process for
• Since January, three clinical M&M review has commenced; the new
M&M review process in place for over
departments have presented at process assists with case selection.
five years. These four departments
the PSC. The PSC is vital to ensure that the
changed over to the standardised
templates, which included TOR, • Work is ongoing towards all M&M review process is in place in all
agenda, minutes and case review. A clinical services having a TOR—five departments and to provide ongoing
PowerPoint presentation template was out of 12 have a TOR. review. The process needs further
supplied but has not yet been utilised. embedding in practice.
• Ten out of the 12 clinical services
Meetings are scheduled for the year have provided dates for meetings Next steps
and invitations have been sent to for 2018.
members of the interdisciplinary team. In the future, it is proposed to
• For the past three months, four continue to:
The DMS has also attended these
out of the 12 clinical services have
meetings for the past two months. • encourage interdisciplinary team
sent minutes to the PSC.
Five departments undertook some reviews,
• The DMS has been invited to and
form of review but were not consistent • work towards all clinical services
attended M&M meetings, which
with scheduling meetings, invitations having a TOR and sending the
has been received well by the staff.
outside of the medical profession, or minutes to the PSC,
minuting cases discussed or lessons The following lessons and limitations
learnt. Collaboration with the M&M are noted: • implement the revised death
review chairs has enabled dates to be review documentation and
• Clinician confidence is increasing process,
scheduled, minutes to be compiled to enable broader discussions
and utilisation of the data supplied to within the interdisciplinary team. • purchase a database.
assist with case selection.
• The M&M review process is only
Monitoring is ongoing, involving a Acknowledgements
one component of the patient
monthly review of the number of M&M safety officer’s role, and workload The author thanks the Director of
meetings held per year, minutes sent will determine how much time can Safety and Quality, DMS, clinical
to the PSC and numbers of adverse be spent supporting the clinical director of surgical service line,
events. departments. The M&M review mortality nurse, data analyst and
process will mature and become M&M chairs.
Results embedded in clinical practice,
This project has had the following resulting in less support required. References
outcomes: • The new death review process will 1. Duckett 2018
• Guidelines have been developed commence in May and assist with
and endorsed. case selection and discussion for
the M&M review process.
19ACHS Improvement Academy | Project Summaries 2017-2018
Multi-resistant organism (MRO) discharge
swab compliance improvement project
Background allocation because of the limited
number of isolation rooms available to
The current intensive care unit (ICU) at cohort MRO-positive patients. Further,
St George Hospital, Kogarah, Sydney, the limited number of isolation rooms
has 15 beds (12 multi-bedded, three on the wards also affects discharge
isolation rooms). In addition, the high destination.
dependency unit (HDU) has 12 beds
(eight multi-bedded, four isolation The MRO screening policy at St George
rooms) and the cardiothoracic unit Hospital has recently been updated
(CICU) has five beds (multi-bedded), to comply with the NSW Health policy
making a total of 32 beds. St George directive. At St George ICU, the true
Hospital ICU is moving into a new ICU incidence of ICU-acquired MRO is
on 21 November 2017. The new ICU unknown, as patients have not been
will be a maximum 52 single-bedded swabbed on discharge until recently.
ICU with a mixture of ICU/HDU patients To collect data on MRO acquisition
and a pod dedicated to CICU. rates in the ICU, discharge swabs need
to be performed. Improving MRO
The planned move to the new ICU discharge swab compliance will help
Asako Ito
provided a good research opportunity the process of obtaining data on MRO
Staff Specialist to compare multi-resistant organism acquisition in the ICU. This will help
St George Hospital, (MRO) acquisition rate in the ICU improve patient care by identifying
Kogarah, Sydney before and after a change from a MRO species causing infection in
multi-bedded to a single-bedded ICU. individual patients and preventing
Therefore, a prospective comparative the spread of MROs. A combination of
study of MRO acquisition rate in early detection, isolation, appropriate
the ICU over 2 years (M.A.R.I.) was treatment and prevention of cross-
designed (current ICU, October 2016 – contamination can all contribute to
September 2017, compared with new preventing the spread of MROs.
ICU, February 2018 – January 2019).
As part of the study data collection,
it was noticed that discharge swab
Measures
compliance was poor. This project At the time of ICU admission, usually
was developed as a part of M.A.R.I. to at least two doctors and two nurses
address this problem. take handover from the relevant team.
Working as a team, ICU staff need to
Problem/Aim assess, diagnose and treat the patient
simultaneously. Once the patient is
MRO acquisition in the ICU is an stabilised, doctors enter the patient
important problem. Recently at St and chart medications on the clinical
George Hospital ICU, there was a major information system (CIS) and order
outbreak of vancomycin-resistant routine testing (bloods, thoracic
enterococci (VRE). Such an outbreak radiography) and further imaging
has significant impact on ICU bed according to needs.
20Patient Safety Lead Program
In contrast, discharging patients
from the ICU is usually completed by
one nurse and one junior ICU doctor.
Discharge is often completed under
time pressure, as there is often an
urgent need to transfer more critically
ill patients to the ICU. In addition,
the nurse performing the discharge
usually takes care of the next patient.
Nurses are responsible for taking MRO
swabs (admission and discharge) and
completing microbiology request
forms among other tasks.
Patients admitted to the ICU for more
than 48 hours and who survived
to ICU discharge were recruited.
Methicillin-resistant Staphylococcus
aureus (MRSA)/VRE swab compliance
rate was calculated on admission and
discharge. Discharge swab compliance
rate was persistently lower than
admission swab compliance rate.
The cause of the low MRO discharge
swab compliance is complex and
multi-factorial. Some of the barriers
to compliance are the healthcare
provider, system, patient and cost.
Design
The following interventions were
introduced:
• CIS alert (started in October 2016).
When a person logged into the CIS,
the reminder ‘Don’t forget MRO
swabs on discharge’ came up on
the screen each time. This worked
best among other interventions.
Unfortunately, this was lost as an
alert trigger when a new CIS was
introduced in June 2017
21ACHS Improvement Academy | Project Summaries 2017-2018
• tick box in nursing discharge accounts. It is impossible to inability to concentrate or may not
summary (started in October know how many nurses access have enough time to understand.
2016). This provides a reminder their work email accounts, and Some patients may feel that
in the form of a checklist. with what frequency. Nursing the swabs are too invasive. This
Interestingly, this reminder staff meetings usually take place intervention was introduced
had minimal impact on swab in weekday daytime hours. As in September, and will need
compliance. This may be because the ICU is a 24-hour service with further ongoing monitoring to
nurses are able to discharge a shift work to cover this, many ascertain effectiveness.
patient without ticking a box. nurses are not able to attend
Additionally, this tick box can be these meetings Results
hidden in the large amount of tick • patient information sheet (started Data were collected on 525 patients
box information the nurses are in mid-September 2017). Patent over a 13-month period (October
required to address at the time of refusal was raised at a nursing 2016 – October 2017). The discharge
patient discharge staff meeting. To minimise patient compliance rate has fluctuated but is
• reminder email to nurses/nursing refusal, a patient information still low despite interventions. MRO
staff meeting (intermittent basis). sheet was developed to improve discharge swab compliance is critical
There are over 200 shift-working patients’ understanding of the to obtain accurate data on MRO
nursing staff at St George ICU. importance of MRO swabs. Even acquisition rate in the ICU.
Reminder emails are sent to at discharge, many patients may
the nursing staff’s work email not be fully awake, may have an
22Patient Safety Lead Program
Conclusion Next steps alert that prevents a discharge
summary being printed. The latter
Increasing MRO discharge swab St George ICU plans to move its would likely be more effective to
compliance has been challenging. physical location to a new building increase compliance but may hinder
It will be important to share the St in November 2017. After this move is workflow. Another plan is to examine
George Hospital ICU experience with complete, there will be an opportunity the problem from the nurse and
other ICUs in and out of the health to revisit interventions to increase patient perspectives by qualitatively
area in a collaborative process. This MRO discharge swab compliance. The examining the barriers to compliance
project has the potential to improve CIS alert was an effective intervention, by surveying or interviewing nursing
patient care and reduce cost, so it and ideally this can be configured in staff and patients.
is worthwhile continuing efforts to the new ICU. This could take the form
increase compliance. of a simple alert or a more complex
23ACHS Improvement Academy | Project Summaries 2017-2018
Reducing catheter-acquired urinary tract
infections in surgical patients
Background formed incorporating key personnel
from surgical specialties, exclusive
Australia is falling behind many other of orthopaedics, and an executive
countries when it comes to urinary sponsor was found.
tract infections (UTIs) in hospitals. A
total of 1.7% or 95,000 patients acquire The working group identified a number
a UTI annually in hospital. These of issues that it considered contributed
patients stay about 4 days longer in to the catheter-acquired UTIs, and to
hospital, which equates to 280,000 test these theories, a number of focus
public hospital beds each day. (1) groups were held with frontline staff
for their impressions. Workflow for
The Nepean Hospital Surgical patients attending theatre for minor
Department is part of the American procedures was reviewed, and it was
College of Surgeons National Surgical identified that indwelling catheters
Quality Improvement Program (ACS were being inserted with no evidence
NSQIP). The NSQIP is a data-driven, of the benefits and usually by the
risk-adjusted, outcomes-based most junior medical staff. In addition,
programme to measure and improve the NSW Ministry of Health had
the quality of surgical care. recently released a policy guideline
Data have been collected from the in 2016 outlining best practice, and a
Dianne Jolley Nepean Surgical Department for the procedure for the local health district
Quality and Safety Manager past 18 months and submitted to (LHD) was developed for the insertion
Nepean Hospital, Nepean the NSQIP for evaluation of a range and management of indwelling
of complications including, but not catheters. It was recognised that there
Blue Mountains Local Health
restricted to, morbidity and mortality, were a number of areas to target from
District, NSW the information gathered from the
length of stay, venous thrombosis/
embolism, surgical site infections, UTIs focus groups and from the literature
and readmission rates. reviewed.
The group acknowledged that, in
Problem/Aim addition to an LHD procedure for
From the abovementioned data catheterisation of adult patients
collection, it was identified that the in the acute setting, the following
number of patients acquiring UTIs interventions were required:
following surgery was above the • reduce the number of unnecessary
benchmark and that the majority of catheterisations
these were due to catheterisation
• run a ‘get it off the floor’ campaign
during and after surgery. The division
of surgery embarked on the project • review the equipment available
to reduce the number of catheter- • review the resources available for
acquired UTIs. patients
• improve the education of staff.
Design
The ‘get it off the floor’ campaign was
This improvement plan involved run as a poster competition during
a colorectal surgeon, the quality Urology Week to identify how to
and safety manager, the newly improve compliance with hanging
appointed clinical nurse consultant catheter bags from hangers rather than
(CNC) urology and the NSQIP data placing them on the floor. Education
manager. A working group was workshops were run by the CNC
24Patient Safety Lead Program
urology on aseptic technique and NSQIP data. Below is the NSQIP report, References
catheterisation, and the colorectal which shows a steady reduction
surgeon worked with the surgeons to in UTI from March 2017, when the 1. Mitchell BG, Ferguson JK, Anderson
reduce the number of unnecessary programme began, to July 2018. M, Sear J. Barnett A. Length of stay and
catheterisations in theatre. mortality associated with healthcare-
associated urinary tract infections: a
Conclusion multi-state model. J Hosp Infect 2017;
Results All the initiatives were introduced as 93( 1):92-9.
For October 2016 – October 2017, the a bundle and it is difficult to identify
number of patients with identified any one practice change that has
catheter-acquired UTI at Nepean affected the outcome, but the most
Hospital in the patient cohort for this significant practice change appears
project reduced from 2.91% to 1.71% to be the reduction of unnecessary
of average risk as described by ACS catheterisations in the operating
theatres by the surgeons.
25ACHS Improvement Academy | Project Summaries 2017-2018
Exploring paediatric inter-hospital transfers
across the health service to identify and raise
awareness of the clinical risks
or while being transferred. There have
been a number of clinical incidences
and reviews in morbidity and mortality
meetings, as well as anecdotal
evidence, raising concerns for the
safety of patients involved in IHT.
Problem/Aim
The aim of this project was to
identify the issues/risks that have
led to clinical incidents of paediatric
patients undergoing IHT within the
health service. This information is to
be presented to the Transfer of Care
Committee and Patient Safety and
Quality Council with the intention of:
• suggesting changes to the existing
outcome measures so that they
more accurately reflect patient
outcomes in relation to quality
and safety
• proposing interventions that lead
to improvement in the safety
Dr Clare Thomas Background of IHT.
Paediatrician Patients requiring a higher level of
paediatric care are admitted to a Measures
Sunshine Coast Hospital and paediatric ward at Sunshine Coast Mapping the transfer journey was
Health Service, Queensland University Hospital (SCUH) and require complex because of fragmentation of
an inter-hospital transfer (IHT) if they documentation and the use of multiple
are in one of the four surrounding systems. Despite both digital and
smaller peripheral emergency paper processes in place, data critical
departments. On average, two to three to the clinical process were not easily
patient transfers occur per day, with accessed. Specifically, data relating to
one transfer per week of a high-acuity decision-making, risk stratification and
patient. High-acuity patients, who do skill of staff involved in the transfer
not meet the threshold for specialised process were difficult to obtain even
medical retrieval, often have a high on review of the clinical notes.
risk of deterioration awaiting transfer
26Patient Safety Lead Program
Design imagined (WAI) and work as identified with a review of clinical
done (WAD) incidents. Audits using current
This complexity meant that a number outcome measures showed less
of strategies were implemented to • cause-and-effect diagram to
identify causes of problematic IHT than 50% of documentation was
determine the actual risks: being completed.
• multi-voting to allow clinical staff
• review of 15 clinical incidents to to vote on what they think were Process mapping revealed a lack of
assist in identifying a number the most problematic issues consistency in knowledge of how the
of key issues and themes for current IHT procedure works. Staff
consideration • consumer engagement by
patient and family surveys then identified issues that they felt
• audit of current process (results pending) contributed to the problems in IHT
• completion of iPassport document and this was illustrated in a cause-and-
• survey of staff involved in
• completion of iTransfer document effect diagram. Multi-voting results
escorts providing qualitative and
(results pending) were analysed and displayed in a
quantitative data.
Pareto chart. The top four problems
• working with inter-professional
were ‘safe to receive’, ‘status update’,
focus groups consisting of Results ‘skill level of escort’, and ‘telehealth
medical, nursing, junior and
Themes such as issues with not used’.
senior staff
communication, delays and
• process mapping to map the unrecognised deterioration were
differences between work as
27ACHS Improvement Academy | Project Summaries 2017-2018
‘Skill level of escort’ was further that the right solutions are adopted. Through actively participating in the
explored using survey monkey. Proposed changes include comparison project, staff members are informed
Of concern, 100% of nurses who of the use of telephone and telehealth of the problems and are using this
responded did not have training in consultations for IHT, with the trial knowledge to better mitigate the
how to conduct a paediatric IHT. running over 6 months. Staff will risks for the paediatric patient
The qualitative data revealed a lack be surveyed, and outcomes and undergoing IHT.
of defined criteria for nurse escorts recommendations will be presented to
and that using an escort denudes the the Transfer of Care Committee. Next steps
referring hospital of key staff.
Following the proposed interventions The executive director of Innovation,
there will be a repeat of the Quality, Research and Education has
Conclusion measurement process with newly requested a formal risk analysis and
The data collected are invaluable to developed measurement outcomes has assigned two project officers
inform the interventions required. and comparison of clinical incidents to work with the Paediatric IHT
Agreed suggestions will undergo Plan- pre- and post-intervention. This will Working Group.
Do-Study-Act (PDSA) cycles to ensure undergo multiple PDSA cycles.
28Patient Safety Lead Program
References
1. Australasian College for Emergency
Medicine Joint Faculty of Intensive Care
Medicine, Australian and New Zealand
College of Anaesthetists. Minimum
standards for transport of critically ill
patients. Emerg Med (Fremantle) 2003;
15(2):197-201.
2. Hains IM, Marks A, Georgiou A,
Westbrook JI. Non-emergency patient
transport: what are the quality and safety
issues? A systematic review. Int J Qual
Health Care 2011; 23(1):68-75.
3. Comeau OY, Armendariz-Batiste J,
Woodby SA. Safety first! Using a checklist
for intrafacility transport of adult intensive
care patients. Crit Care Nurse 2015;
35(5):16-25.
4. Newton SM, Fralic M. Interhospital
transfer center model: components,
themes, and design elements. Air Med J
2015; 34(4):207-12.
5. Rouse J. What do ambulance service
personnel perceive to be the process of
and issues with inter-hospital transfers? J
Paramedic Pract 2016; 8(6):294-301.
6. Kate AM, Mark SE, Jeremy SF. The use of
telemedicine to aid in assessing patients
prior to aeromedical retrieval to a tertiary
referral centre. J Telemed Telecare 2008;
14(6):309-14.
7. Desai S, Williams ML, Smith AC.
Teleconsultation from a secondary hospital
for paediatric emergencies occurring at
rural hospitals in Queensland. J Telemed
Telecare 2013; 19(7):405-10.
8. Kyle E, Aitken P, Elcock M, Barneveld M.
Use of telehealth for patients referred to a
retrieval service: timing, destination, mode
of transport, escort level and patient care. J
Telemed Telecare 2012; 18(3):147-50.
29ACHS Improvement Academy | Project Summaries 2017-2018
“Coming from a small hospital the course has been great for me to meet other people. Probably the biggest part
has been the diagnostics, whereas in the past I learnt to go on just a gut feeling. It has been an important step
for me to be able to flesh it out. It has been really good.”
Johanne Davis, Peninsula Private Hospital
“The networking and regular contact with like-minded people has been invaluable. The QIL program has
definitely enhanced my own knowledge of quality improvement and made me think outside the box. How we
engage with our patients, families and greater communities from the very first contact, can be critical to a
liftetime of expectations.”
Galina Ramensky-Manoilof, Redcliff Hospital
“Using the science of quality improvement gave staff a chance that this might work. Having to manage a work-
based project has been critical to the success of the course for me, otherwise it likely wouldn’t have happened. I
also took away a focus on what you can achieve in terms of improvements, not what you can’t do.” (Erin)
“The course has allowed me to consolidate learnings from other courses in a more practical and systematic way.
It has been particularly useful in demonstrating the importance of data pre and post change and how winning
the hearts and minds of staff increases the success and sustainability of changes implemented.” (Stephen)
Erin Finn, Stephen Caddick, Sandy Lewis, West Moreton
“I am really glad to have done the QIL course, to have a new approach, to make new friends and the opportunity
to do quality improvement in a systemised way.”
Helen Yu Pik Ling, Hong Kong Baptist Hospital
“To make myself do the diagnostics, and actually follow the quality improvement process was great. Timing was
key, having the patience to wait for engagement of the correct stakeholders who have competing priorities. With
the right data, it can really drive motivation within the leadership team. I am glad we pursued it, and owned it.
Now they are really keen to own it.”
Sharon Anne McAuley, Lady Cilento Children’s Hospital
The tools and diagnostic processes were invaluable. It has been stronger than a lightbulb moment for me.
Previous education (in quality improvement science) has usually been very solution/implementation focused and
this course is very much about understanding the problem first, so you get the right solutions and they gave us
the tools to do it.”
Katie Robinson, Children’s Health Queensland Hospital and Health Service
30Quality Improvement Lead Program
Quality Improvement Lead Program
Project Summaries
About the Quality Improvement Lead Program
The Quality Improvement Lead Training Program (QIL) has been designed for senior staff within healthcare organisations
who lead quality improvement activities including: patient-based care and co-design; improvements in patient safety,
outcomes, efficiency and access to services; and those who need to design new models of care particularly for chronic and
complex disease management across continuums of care.
Participants will receive an immersion in quality improvement science and theories.
They will gain skills in leading and sustaining change processes, measurement for quality improvement using statistical
process control charts and engaging with consumers in healthcare improvement. This course will focus on clinical practice
improvement and its implementation in healthcare learning from successful international partners including, but not
limited to: Intermountain Healthcare USA and Salford Royal Foundation Trust UK NHS.
Quality Improvement Lead graduation ceremony, held on 1 December 2017 in Sydney
Quality Improvement Lead graduation ceremony, held on 5 May 2018 in Brisbane
31You can also read