Original Article Clinical efficacy of Rose Yurong decoction in patients with lung meridian wind-heat type of rosacea
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Int J Clin Exp Med 2020;13(9):6916-6922 www.ijcem.com /ISSN:1940-5901/IJCEM0114581 Original Article Clinical efficacy of Rose Yurong decoction in patients with lung meridian wind-heat type of rosacea Hongqun Mao, Guoqi Wei Department of Dermatology, Hangzhou Fuyang Hospital of Traditional Chinese Medicine, Hangzhou 311400, Zhejiang Province, China Received May 19, 2020; Accepted July 7, 2020; Epub September 15, 2020; Published September 30, 2020 Abstract: Objective: To explore the clinical effect of Rose Yurong Decoction in patients with wind-heat type of rosa- cea. Methods: The medical records of 109 patients with lung meridian wind-heat type of rosacea were collected retrospectively. They were divided into group A which received routine western medicine treatment and group B which was given Rose Yurong Decoction in addition to routine western medicine. The clinical efficacy, skin lesions, self-report scores, skin hydration, hemoglobin content and skin elasticity, and occurrence of adverse reactions of the two groups before and after treatment were compared. The recurrence was recorded during follow-up. Results: After 8 weeks of treatment, the papule pustules, telangiectasia, flushing erythema score, total lesion score, self- report score, hemoglobin content and recurrence in group B were lower than those in group A. The total effective rate, skin hydration and skin elasticity in group B were higher than those in group A (P

Clinical efficacy of Rose Yurong decoction
achieve satisfactory therapeutic efficacy [12]. q.d. Enteric-coated capsules (Yongxin Pharma-
There are a variety of TCM prescriptions for the ceutical Industry (Kunshan) Co., Ltd. H200-
clinical treatment of lung meridian wind-heat 30627, 0.1 g * 10 capsules) at 30 min after
type of rosacea, including Loquat Qingfei De- meals for 8 weeks. Patients were instructed to
coction, Qingfei Chuci Prescription, Decoction wash their face with warm water every night
of Ephedra, Almond, Licorice and Gypsum, etc., and use a moisturizing cream (Kunming Be-
and different prescriptions have various thera- thany Biological Technology Co., Ltd 50 g) for 8
peutic effects, so it is necessary to explore an weeks.
effective prescription for the treatment of this
disease. Group B received the same treatment as group
A and was additionally treated with Rose Yurong
In order to improve the therapeutic effect of decoction. The prescription consisted of
lung meridian wind-heat type of rosacea and Licorice 5 g, Chinese yam 20 g, Coix seed 20 g,
reduce side effects, this study added Rose rice bean 15 g, Albizia flower 3 g, Poria 15 g,
Yurong Decoction to the treatment regimen on Rehmannia glutinosa 10 g, red peony root 10 g,
basis of the theories explained above and rose buds 3 g, Light-yellow Sophora root 12 g,
explored the effects. Scutellaria baicalensis 10 g, honeysuckle 15 g,
Chinese trumpet creeper 3 g, densefruit pittany
Materials and methods root-bark 15 g, loquat leaf 10 g, and white mul-
berry root-bark 10 g. For patients with yellowish
Data
complexion and frequent tiredness, white pe-
The clinical data of 109 patients with lung ony root and Codonopsis pilosula were added
meridian wind-heat type of rosacea in our hos- into the prescription. For those with heavy men-
pital were collected retrospectively and divided strual bleeding, celosia and sophora japonica
into two groups based on the treatment meth- were added. For those with black period blood
od. Group A (n=54) received Doxycycline Hy- clots and hypomenorrhea, motherwort, angeli-
clate Enteric-Coated Capsules combined with ca or salvia was added. For patients with de-
hydroxychloroquine tablets. Group B (n=55) pression or with irritable moods, Chinese Th-
were treated with Rose Yurong Decoction in orowax root and radix gentianae were added.
addition to treatment similar to group A. (1) For patients with reduced appetite and loose
Inclusion criteria: patients who signed the stools, atractylodes were added. The above
informed consent; patients without contraindi- decoction was cooked with water for oral
cations for medication; patients with wind-heat administration in the morning and evening, 30
in the lung meridian; those who did not receive min after meal for 8 weeks.
tretinoin preparation, estrogen or glucocorti-
Outcome measurements
coids within the past 2 months or antibiotics
within 1 month before enrollment; or patients
(1) Skin lesion scoring: Before treatment and
without kidney, liver, immune system and car-
after 8 weeks of treatment, the severity of skin
diovascular system diseases. This study was
lesion, including papule pustules, telangiecta-
approved by the medical ethics committee
sia, and flushing, was scored. Zero indicates no
of Hangzhou Fuyang Hospital of Traditional
skin lesions and 1, 2, 3 represents mild, moder-
Chinese Medicine. (2) Exclusion criteria: pa-
ate and severe lesions, respectively. The total
tients who received other treatment options
points are the sum of lesion scoring [13]. (2)
during the observation period; patients with the
Self-report score: Before treatment and after 8
presence of seborrheic dermatitis, psoriasis,
weeks of treatment, patients scored their dis-
acne vulgaris, and actinic diseases; patients
comfort in terms of eye discomfort, tingling,
with history of alcohol dependence; and pa-
itching, dryness, burning sensation. Zero and 1
tients with poor compliance.
indicate no discomfort and the presence of one
Methods symptom. The total score is the sum of score of
every symptom [14]. (3) Efficacy evaluation: The
Group A was given b.i.d. hydroxychloroquine total score was the sum of the self-report score
sulfate tablets (H19990263, Shanghai Zhongxi and skin lesion score. Efficacy index = (total
Pharmaceutical Co., Ltd., 0.1 g×14 tablets) and score before treatment-total score after treat-
6917 Int J Clin Exp Med 2020;13(9):6916-6922Clinical efficacy of Rose Yurong decoction
Table 1. Comparison of baseline data [(%)]/(±) Deviation (mean ± SD) and
Group A Group B compared by t test when con-
Data t/X2 P forming to the normal distribu-
(n=54) (n=55)
Gender (Cases) Male 10 (18.52) 12 (21.82) 0.184 0.668 tion; otherwise, Mann-Whitney
Female 44 (81.48) 43 (78.18) U test was used. Count data
were expressed as [n (%)] and
Age (year) 38.15 (1.09) 38.19 (1.12) 0.189 0.851
compared by X2 test. P0.05)
(Table 1).
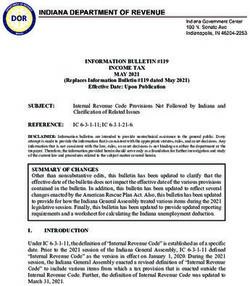
Comparison of skin lesion
scores
There was no significant differ-
ence in skin lesion scores in-
cluding papule pustules, te-
langiectasia, flushing erythe-
ma score and total lesion
Figure 1. Comparison of skin lesion scores. Skin lesion scores showed no scores between the two gr-
significant differences between two the groups before treatment (P>0.05) oups before treatment (P>
and differed significantly after 8 weeks of treatment (PClinical efficacy of Rose Yurong decoction Table 2. Comparison of self-report scores globin content than group A Group Before treatment After 8 weeks of treatment (P
Clinical efficacy of Rose Yurong decoction
Table 4. Comparison of the occurrence of adverse reactions has the functions of activating blood
Number Stomach circulation, moisturizing skin, cooling
Group Diarrhea Anorexia Total incidence blood, detoxifying, and clearing away
of cases ache
Group A 54 2 (3.70) 3 (5.56) 1 (1.85) 6 (11.11) wind and heat. Rehmannia glutinosa
Group B 55 1 (1.82) 2 (3.64) 4 (7.27) 7 (12.73) can nourish the spleen and stom-
X 2
0.068
ach, clearing away heat and promot-
ing salivation; Chinese yam, Coix
P 0.795
seed and Poria have the functions of
replenishing the lungs, nourishing
Table 5. Comparison of the recurrence rate the spleen and stomach, strengthening the
between two groups spleen and eliminating dampness; rice bean
Group Number of cases Recurrence rate and red Peony root suppress hyperactive liver,
Group A 54 16 (29.63)
activate blood circulation and remove blood
stasis; Light-yellow Sophora root, Scutellaria
Group B 55 2 (3.64)*
baicalensis, and Densefruit Pittany root-bark
X2 13.353
can dispel wind and arrest inching, kill insects
P 0.000 and detoxifies, and clears away heat and damp-
Note: *indicates comparison with group A, PClinical efficacy of Rose Yurong decoction
ing facial skin lesions and symptoms of rosa- sensus document on the treatment algorithm
cea [30]. for rosacea. Actas Dermosifiliogr 2019; 110:
533-545.
In conclusion, Rose Yurong decoction could [7] Walsh RK, Endicott AA and Shinkai K. Diagno-
effectively improve rosacea and reduce the sis and treatment of rosacea fulminans: a
recurrence rate with high safety. comprehensive review. Am J Clin Dermatol
2018; 19: 79-86.
Although certain conclusions have been drawn, [8] Zip C. The role of skin care in optimizing treat-
this study also has the limitation of using a ment of acne and rosacea. Skin Therapy Lett
2017; 22: 5-7.
small sample size, which requires further stud-
[9] Steinhoff M, Schmelz M and Schauber J. Facial
ies on the basis of a larger sample size and lon-
erythema of rosacea-aetiology, different patho-
ger follow-up period. physiologies and treatment options. Acta Derm
Venereol 2016; 96: 579-586.
Disclosure of conflict of interest [10] Forton FMN and De Maertelaer V. Rosacea
and demodicosis: little-known diagnostic signs
None. and symptoms. Acta Derm Venereol 2019; 99:
47-52.
Address correspondence to: Hongqun Mao, Depart-
[11] Gether L, Overgaard LK, Egeberg A and Thys-
ment of Dermatology, Hangzhou Fuyang Hospital of sen JP. Incidence and prevalence of rosacea: a
Traditional Chinese Medicine, No. 2-4, Guihua Road, systematic review and meta-analysis. Br J Der-
Fuchun Street, Fuyang District, Hangzhou 311400, matol 2018; 179: 282-289.
Zhejiang Province, China. Tel: +86-13067719078; [12] Holmes AD, Spoendlin J, Chien AL, Baldwin H
E-mail: hongqunmao56@163.com and Chang ALS. Evidence-based update on ro-
sacea comorbidities and their common physi-
References ologic pathways. J Am Acad Dermatol 2018;
78: 156-166.
[1] Anzengruber F, Czernielewski J, Conrad C, Feld- [13] Choi JE, Werbel T, Wang Z, Wu CC, Yaksh TL
meyer L, Yawalkar N, Häusermann P, Cozzio A, and Di Nardo A. Botulinum toxin blocks mast
Mainetti C, Goldblum D, Läuchli S, Imhof L, cells and prevents rosacea like inflammation. J
Brand C, Laffitte E and Navarini AA. Swiss S1 Dermatol Sci 2019; 93: 58-64.
guideline for the treatment of rosacea. J Eur [14] Saleem MD. Revisiting rosacea criteria: where
Acad Dermatol Venereol 2017; 31: 1775-1791. have we been, where are we going, and how
[2] Gallo RL, Granstein RD, Kang S, Mannis M, will we get there? Dermatol Clin 2018; 36:
Steinhoff M, Tan J and Thiboutot D. Standard 161-165.
classification and pathophysiology of rosacea: [15] Tan J, Almeida LM, Bewley A, Cribier B, Dlova
the 2017 update by the National Rosacea So- NC, Gallo R, Kautz G, Mannis M, Oon HH, Raja-
ciety Expert Committee. J Am Acad Dermatol gopalan M, Steinhoff M, Thiboutot D, Troielli P,
2018; 78: 148-155. Webster G, Wu Y, van Zuuren EJ and Schaller
[3] Gonzalez-Hinojosa D, Jaime-Villalonga A, Agui- M. Updating the diagnosis, classification and
lar-Montes G and Lammoglia-Ordiales L. De- assessment of rosacea: recommendations
modex and rosacea: is there a relationship? from the global ROSacea COnsensus (ROSCO)
Indian J Ophthalmol 2018; 66: 36-38. panel. Br J Dermatol 2017; 176: 431-438.
[4] Alexis AF, Callender VD, Baldwin HE, Desai SR, [16] Oussedik E, Bourcier M and Tan J. Psychoso-
Rendon MI and Taylor SC. Global epidemiology cial burden and other impacts of rosacea on
and clinical spectrum of rosacea, highlighting patients’ quality of life. Dermatol Clin 2018;
skin of color: review and clinical practice expe- 36: 103-113.
rience. J Am Acad Dermatol 2019; 80: 1722- [17] Cices A and Alexis AF. Patient-focused solu-
1729, e1727. tions in rosacea management: treatment chal-
[5] Yuan X, Huang X, Wang B, Huang YX, Zhang YY, lenges in special patient groups. J Drugs Der-
Tang Y, Yang JY, Chen Q, Jian D, Xie HF, Shi W matol 2019; 18: 608-612.
and Li J. Relationship between rosacea and di- [18] Long J, Li J, Yuan X, Tang Y, Deng Z, Xu S, Zhang
etary factors: a multicenter retrospective case- Y and Xie H. Potential association between ro-
control survey. J Dermatol 2019; 46: 219-225. sacea and cancer: a study in a medical center
[6] Salleras M, Alegre M, Alonso-Usero V, Boixeda in southern China. J Dermatol 2019; 46: 570-
P, Domínguez-Silva J, Fernández-Herrera J, 576.
García-Navarro X, Jiménez N, Llamas M, Nadal [19] Aksoy B, Ekiz Ö, Unal E, Ozaydin Yavuz G, Gonul
C, Del Pozo-Losada J, Querol I, Salgüero I, M, Kulcu Cakmak S, Polat M, Bilgic Ö, Baykal
Schaller M and Soto de Delás J. Spanish con- Selcuk L, Unal I, Karadag AS, Kilic A, Balta I,
6921 Int J Clin Exp Med 2020;13(9):6916-6922Clinical efficacy of Rose Yurong decoction
Kutlu Ö, Uzuncakmak TK and Gunduz K. Sys- [25] Saleem MD and Wilkin JK. Evaluating and opti-
temic comorbidities associated with rosacea: a mizing the diagnosis of erythematotelangiec-
multicentric retrospective observational study. tatic rosacea. Dermatol Clin 2018; 36: 127-
Int J Dermatol 2019; 58: 722-728. 134.
[20] Gazi U, Gureser AS, Oztekin A, Karasartova D, [26] Florez-White M. Acne and rosacea: special
Kosar-Acar N, Derici MK, Artuz F, Mumcuoglu considerations in the treatment of patients
KY and Taylan-Ozkan A. Skin-homing T-cell re- with latin american ancestry. J Drugs Dermatol
sponses associated with Demodex infestation 2019; 18: s124-126.
and rosacea. Parasite Immunol 2019; 41: [27] Chang YS and Huang YC. Role of Demodex
e12658. mite infestation in rosacea: a systematic re-
[21] Forton FMN and De Maertelaer V. Papulopus- view and meta-analysis. J Am Acad Dermatol
tular rosacea and rosacea-like demodicosis: 2017; 77: 441-447, e446.
two phenotypes of the same disease? J Eur [28] Singam V, Rastogi S, Patel KR, Lee HH and Sil-
Acad Dermatol Venereol 2018; 32: 1011- verberg JI. The mental health burden in acne
1016. vulgaris and rosacea: an analysis of the US Na-
[22] Hung CT, Chiang CP, Chung CH, Tsao CH, Chien tional Inpatient Sample. Clin Exp Dermatol
WC and Wang WM. Risk of psychiatric disor- 2019; 44: 766-772.
ders in rosacea: a nationwide, population- [29] Incel Uysal P, Akdogan N, Hayran Y, Oktem A
based, cohort study in Taiwan. J Dermatol and Yalcin B. Rosacea associated with in-
2019; 46: 110-116. creased risk of generalized anxiety disorder: a
[23] Jørgensen AR, Egeberg A, Gideonsson R, Wein- case-control study of prevalence and risk of
stock LB, Thyssen EP and Thyssen JP. Rosacea anxiety in patients with rosacea. An Bras Der-
is associated with Helicobacter pylori: a sys- matol 2019; 94: 704-709.
tematic review and meta-analysis. J Eur Acad [30] Williamson T, Cameron J, McLeod K, Turner B,
Dermatol Venereol 2017; 31: 2010-2015. Quillen A, LaRose A, Lott J and Gaiser A. Con-
[24] Porriño-Bustamante ML, Fernández-Pugnaire cerns and treatment satisfaction in patients
MA and Arias-Santiago S. A cross-sectional being treated with azelaic acid foam for rosa-
study of rosacea and risk factors in women cea. J Drugs Dermatol 2019; 18: 381-386.
with frontal fibrosing alopecia. Acta Derm Ve-
nereol 2019; 99: 1099-1104.
6922 Int J Clin Exp Med 2020;13(9):6916-6922You can also read