Oral Health and Teledentistry Interest during the COVID-19 Pandemic
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Journal of
Clinical Medicine
Article
Oral Health and Teledentistry Interest during the
COVID-19 Pandemic
Magdalena Sycinska-Dziarnowska 1 , Marzia Maglitto 2 , Krzysztof Woźniak 1 and Gianrico Spagnuolo 2,3, *
1 Department of Orthodontics, Pomeranian Medical University in Szczecin, Powstańców Wielkopolskich Street
72, 70111 Szczecin, Poland; magdadziarnowska@gmail.com (M.S.-D.); krzysztof.wozniak@pum.edu.pl (K.W.)
2 Department of Neurosciences, Reproductive and Odontostomatological Sciences, University of Naples
“Federico II”, 80131 Napoli, Italy; mar.maglitto@gmail.com
3 Institute of Dentistry, I. M. Sechenov First Moscow State Medical University, 119435 Moscow, Russia
* Correspondence: gspagnuo@unina.it
Abstract: Background: The COVID-19 pandemic outbreak has significantly changed access to dental
treatments. Methods: The data related to oral health and teledentistry topics were collected from the
open database Google Trends. The analyzed material was collected from 19 June 2016 to 6 June 2021
among anonymous search engine users. The following expressions were analyzed: “dental care”,
“emergency dental care”, “oral health”, ”periodontitis”, “teledentistry”, “is it safe to go to the dentist”,
and “COVID-19” and ”PPE dentist”. Results: During the first lockdown in 2020, a significant increase
in “emergency dental care” phrase queries was detected, with a simultaneous decrease in regular
“dental care” questions, as well as a peak in the queries for “periodontitis” preceded by lower interest
in “oral health.” The number of searches stated for “teledentistry” increased during the time of the
pandemic 5 times and for and “PPE dentist” 30 times. The risk of visiting the dental studio was seen
in almost 40 times increase in the query “is it safe to go to the dentist.” Conclusions: The COVID-19
Citation: Sycinska-Dziarnowska, M.;
imprinted a stigma on oral health care. In this difficult epidemiological situation, teledentistry might
Maglitto, M.; Woźniak, K.; Spagnuolo,
G. Oral Health and Teledentistry
become a helpful solution.
Interest during the COVID-19
Pandemic. J. Clin. Med. 2021, 10, 3532. Keywords: oral health; teledentistry; Google Trends; COVID-19 pandemic
https://doi.org/10.3390/
jcm10163532
Academic Editors: 1. Introduction
Hans-Peter Howaldt and Sameh Attia
In late June 2021, about 182 million COVID-19 cases were reported globally, with
almost 4 million people deaths [1]. It seems very likely that the COVID-19 pandemic had
Received: 22 July 2021
an impact on oral health-related behaviors. The stringent measures undertaken to limit
Accepted: 10 August 2021
the spread of COVID-19 disease with social distancing rules made access to dental offices
Published: 11 August 2021
more troublesome. The risk of contagion can be reduced by introducing teledentistry [2].
Teleconsultation, which begins with an online triage, was a compromise that limited patient
Publisher’s Note: MDPI stays neutral
access but also ensured effective treatment and relief from symptoms [3].
with regard to jurisdictional claims in
According to some studies, routine dental care and emergency dental care have been
published maps and institutional affil-
iations.
immensely influenced by the waves of COVID-19 [4–7]. The large impact of the COVID-
19 pandemic on dentistry was shown in the study conducted by Soltani et al., in which
as many as 659 articles published by dental journals were found in PubMed regarding
implications of the COVID-19 pandemic in dentistry [8]. Moreover, many people did not
want to visit the dental studios due to the fear of virus transmission. Moreover, as proved
Copyright: © 2021 by the authors.
in many studies in pre-pandemic time, the prolonged lack of regular oral health check-
Licensee MDPI, Basel, Switzerland.
ups may lead to periodontitis [9,10]. Another unprecedented situation happened during
This article is an open access article
the COVID-19 pandemic. Greater demand for personal protective equipment (PPE) was
distributed under the terms and
detected globally and led to a shortage in masks, gloves, and almost all PPE [11]. Difficult
conditions of the Creative Commons
Attribution (CC BY) license (https://
access to PPE was significant and obvious in the early phase of the COVID-19 pandemic.
creativecommons.org/licenses/by/
In order to minimize the viral spread risk during the current COVID-19 pandemic and
4.0/).
J. Clin. Med. 2021, 10, 3532. https://doi.org/10.3390/jcm10163532 https://www.mdpi.com/journal/jcm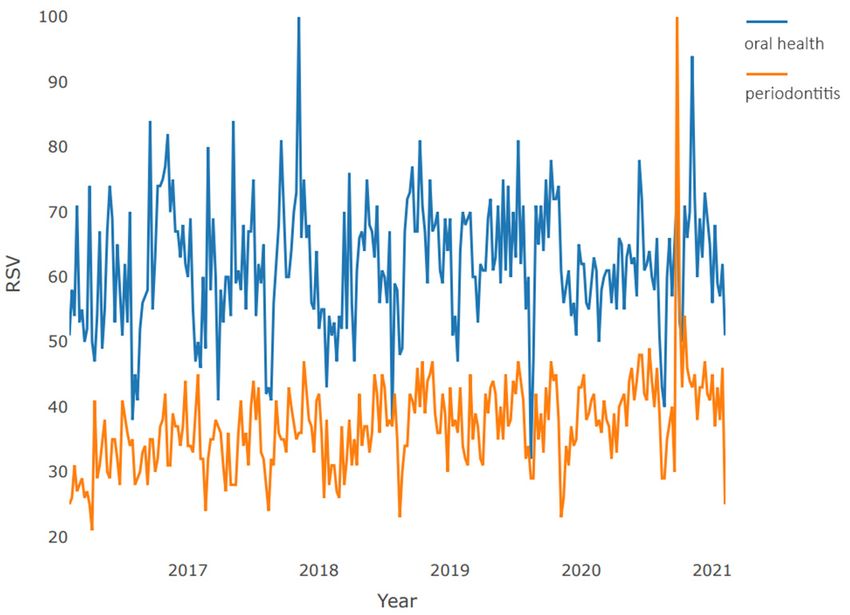
J. Clin. Med. 2021, 10, 3532 2 of 12
post-pandemic times, the global project to define the best organization of dental offices was
conducted [12].
Rapid changes in the epidemiological situation might be easily and strongly visible in
the surveillance of the more widely used search engines, for example, the Google search
engine, the most used engine with the vast majority of the market share, as much as
92.26% [13].
The aim of this study was to analyze the impact of the COVID-19 pandemic on oral
health and the interest in teledentistry.
2. Materials and Methods
The data for the study were collected from the open database—Google Trends (GT)
service among anonymous search engine users related to oral health and teledentistry
subjects [14,15]. Each data record represents a weekly worldwide number of queries
processed by Google engine and available according to the selected time period. In the
study, the analyzed material was collected from 19 June 2016 to 6 June 2021. All data
imported from GT represent queries were normalized to the time and location. The
resulting numbers are scaled on a range of 0 to 100, where 100 is the maximum number of
searches in a stated period of time. The following expressions were analyzed: “dental care”,
“emergency dental care”, “oral health”, “periodontitis”, “COVID-19” and ”PPE dentist”, as
well as the phrases “teledentistry” and “is it safe to go to the dentist”, were investigated to
check the interest for online consultations.
The data analysis was divided into two sections. The first section provides the detailed
level description of data, its structure, and main samples characteristics needed in order to
perform further calculations. In the second section, the pairwise correlation between data
series was analyzed. For each time series data, the trend, cyclical, and random fluctuations
analyses were performed. The purposes of this section were as follows:
• To present pairwise time series visualizations;
• To perform time series decompositions indicating the trend, cyclical, and random fluctuations;
• To analyze the cross-correlation between chosen time series pairs with statistically
significant estimation;
• To evaluate a pairwise of mutual influence (where possible).
To estimate the dynamics rate (hereinafter), the comparisons of two mean rates for
two periods were made: first one for the period before the 22–23 January 2020, when the
World Health Organization (WHO) Director gathered an Emergency Committee to discuss
whether the new virus outbreak determined a public health emergency of worldwide
concern [16] (that refers to dates from 19 June 2016 to 19 January 2020 in our weekly split
data set) and the second one from 19 January 2020 to 6 June 2021. For simplicity, we further
refer to those periods as before and during the pandemic. In the study, we aimed to check
the time before the official pandemic onset, as the search engines may have shown some
interest in the subject before official regulations were made.
For the qualitative and quantitative analysis of the correlation, the time series collec-
tions were divided into the following 4 pairs:
• “Dental care”–“emergency dental”;
• “Oral health”–“periodontitis”;
• “Teledentistry”–“is it safe to go to the dentist”;
• “COVID-19”–“PPE-dentist”.
All statistical estimations with data visualizations were programmed by the “R”
programming language [17] with “R studio” version 1.4.1106 open-source software for
data science, scientific research, and technical communication [18].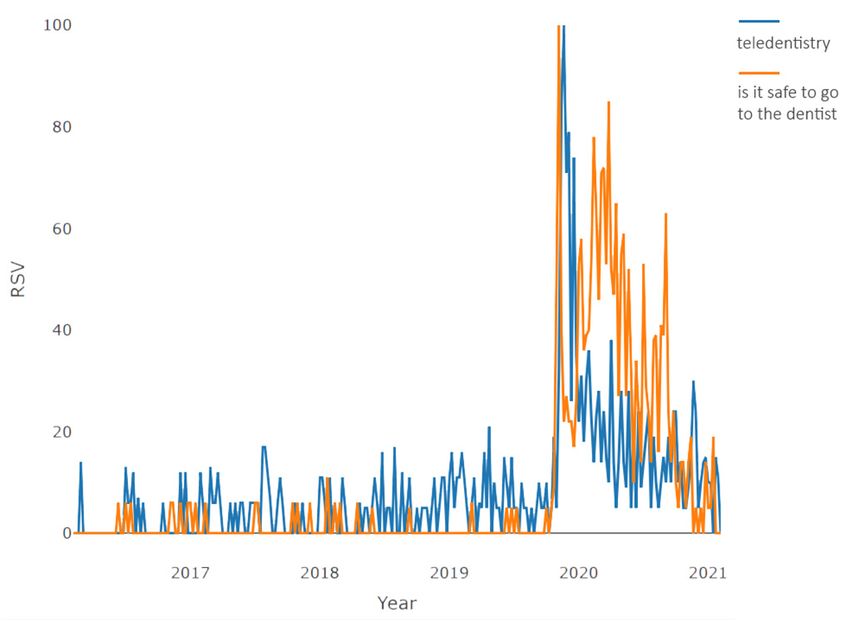
J. Clin. Med. 2021, 10, 3532 3 of 12
J. Clin. Med. 2021, 10, x FOR PEER REVIEW 3 of 12
3. Results
3.1. Time Series Visualizations
3.1. Time Series Visualizations
A graphical illustration of time series was presented by a paired graph of the dynam-
A graphical illustration of time series was presented by a paired graph of the dynamics
ics of requests in the study period. For the purposes of analyzing the trend, cyclical, and
of requests in the study period. For the purposes of analyzing the trend, cyclical, and
random fluctuations, the time series were decomposed for each collection separately.
random fluctuations, the time series were decomposed for each collection separately.
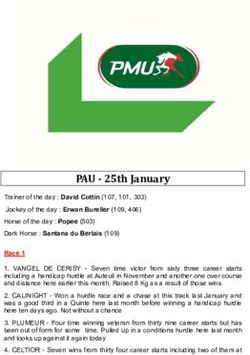
The pairwise time series visualization of “dental care”–“emergency dental care” is
The pairwise time series visualization of “dental care”–“emergency dental care” is
presented in Figure 1a. The plot clearly shows a high proportion of uncertainty in demand
presented in Figure 1a. The plot clearly shows a high proportion of uncertainty in demand
fordental
for dentalservices
servicesatatthe
thevery
verybeginning
beginningofof2020.
2020.This
Thisisisevidenced
evidencedbybya asharp
sharpdecline
declineinin
demand for planned dental procedures with a simultaneous sharp increase
demand for planned dental procedures with a simultaneous sharp increase in demand in demand for
for emergency ones. However, this phase had a short-term character, and during the1–
emergency ones. However, this phase had a short-term character, and during the next
2 months,
next the structure
1–2 months, of demand
the structure returned
of demand to its normal
returned state. state.
to its normal
(a) (b)
Figure
Figure 1.1.Pairwise
Pairwisecomparison
comparisonofofweekly
weeklyrequests
requestsduring
during2016–2021:
2016–2021:(a)(a)“dental
“dentalcare”–“emergency
care”–“emergencydental
dentalcare”;
care”; (b)
(b) “oral
“oral
health”–“periodontitis”.
health”–“periodontitis”.
Thepairwise,
The pairwise,time timeseries
seriesvisualization
visualizationofof“oral
“oralhealth”–“periodontitis”
health”–“periodontitis”isispresented
presented
ininFigure
Figure1b.1b.TheTheplotplotshows
showslargelargeinterest
interestgrowth
growthwhenwhenregarding
regarding“periodontitis”
“periodontitis”with with
thepeak
the peakatatthe
thebeginning
beginningofofthe theyear
year2020
2020with
withstable
stableand
andslight
slightgrowth
growthininthe
thenumber
numberofof
questionsasked
questions askedduringduringthe theanalyzed
analyzedperiod.
period.TheThenumber
numberofofqueries
queriesfor
for“oral
“oralhealth”
health”isis
more stable. A peak in “periodontitis” queries was detected after
more stable. A peak in “periodontitis” queries was detected after the hard lockdown and the hard lockdown and
the
thelower
lowerinterest
interestininthe the“oral
“oralhealth”
health”subject.
subject.
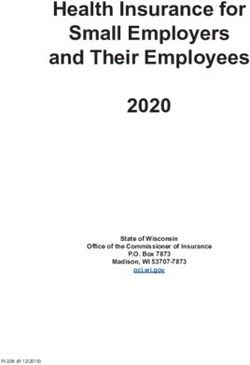
Furthermore,
Furthermore,the pairwise,
the pairwise, time series
time visualization
series visualizationof “teledentistry”–“is
of “teledentistry”–“is it safe to goto
it safe
togothetodentist” is presented
the dentist” in Figure
is presented 2a. Both
in Figure 2a.terms
Both under
terms consideration rarely occurred
under consideration rarely oc-
incurred
the pre-pandemic
in the pre-pandemic time. Only at theatbeginning
time. Only of 2020
the beginning diddid
of 2020 these concepts
these concepts become
become
widespread.
widespread. The plot clearly shows a peak when the request for both terms reachesitsits
The plot clearly shows a peak when the request for both terms reaches
maximum.
maximum.The Thedemand
demandfor forthe
the“teledentistry”
“teledentistry”term termthen
thenbegins
beginstotodecline
declineexponentially
exponentially
until
until the end of the period under review, reaching levels preceding thepandemic,
the end of the period under review, reaching levels preceding the pandemic,and andthe
the
expression
expression“is “isititsafe
safetotogogototothe
thedentist”
dentist”isischaracterized
characterizedbybysteady
steadydemand
demandthroughout
throughout
almost
almostallallofof2020,
2020,reaching
reachinglocallocalhighs
highsduring
duringperiods
periodsofoflockdowns
lockdownsand andexacerbations
exacerbationsofof
restrictions.
restrictions. However, at the end of the period under review, requests forthis
However, at the end of the period under review, requests for thisterm
termalso
also
reached a minimum, slightly exceeding pre-pandemic
reached a minimum, slightly exceeding pre-pandemic levels. levels.
J. Clin. Med. 2021, 10, x FOR PEER REVIEW 4 of 12
J. Clin. Med. Med.10,
2021,
J. Clin. 3532
2021, 10, x FOR PEER REVIEW 4 of 124 of 12
(a) (b)
(a) (b)
Figure 2. Pairwise comparison of weekly requests during 2016–2021: (a) “teledentistry”–“is it safe to go to the dentist”; (b)
Figure 2. Pairwise
2. Pairwise comparison of weekly requests during 2016–2021: (a) “teledentistry”–“is it safe to go to the dentist”; (b)
comparison
Figure
“COVID-19”–“PPE dentist”. of weekly requests during 2016–2021: (a) “teledentistry”–“is it safe to go to the dentist”;
“COVID-19”–“PPE dentist”.
(b) “COVID-19”–“PPE dentist”.
The pairwise,
The pairwise,timetimeseries visualizationofof“COVID-19”–“PPE
series visualization “COVID-19”–“PPE dentist”
dentist” is presented
is presented in in
The pairwise, time series visualization of “COVID-19”–“PPE dentist” is presented in
Figure 2b.2b.
Figure Both
Bothexpressions
expressions came intouse
came into useimmediately
immediately with
with the the onset
onset of theofpandemic.
the pandemic.
Figure 2b. Both expressions came into use immediately with the onset of the pandemic.
TheThe
demand
demand curve
curvefor for“COVID-19”
“COVID-19” isischaracterized
characterized byby
thethe presence
presence of three
of three globalglobal
highs highs
Thethat
demand curve
occurred forjunction
“COVID-19” is characterized by the presence of at
three global highs
that occurred atatthe
the junction of 2019–2020,
2019–2020,ininthethefirst quarter
first of 2020,
quarter and
of 2020, andtheatjunction
the junction
thatofoccurred
2020/2021,at which
the junction of 2019–2020,
corresponds to in the first pandemic
quarter ofwaves.
2020, The
and at the“PPEjunction
of 2020/2021, which corresponds tothe
thetime
timeofofglobal
global pandemic waves. topic
The topic “PPE
of 2020/2021,
dentist” whichforcorresponds
standing personal to the equipment
protective time of globalwas pandemic waves.
characterized by the The topic
greatest de-“PPE
dentist” standing for personal protective equipment was characterized by the greatest de-
dentist”
mandstanding for personal
at the beginning of the protective equipment
pandemic; over the nextwas1.5 characterized
years, the level by of the greatest
interest
mand at the beginning of the pandemic; over the next 1.5 years, the level of interest
demand at the
dropped beginninguntil
exponentially, of the
the pandemic; over under
end of the period the next 1.5 years,
review, where the level
it again of interest
reached
dropped exponentially,
the pre-pandemic
until the end of the period under review, where it again reached
level.until the end of the period under review, where it again reached
dropped exponentially,
the pre-pandemic level.
the pre-pandemic level.
3.2. Trends Analysis
3.2.Trends
3.2. Trends Analysis
Analysis
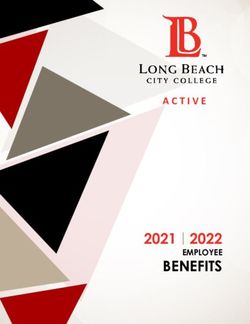
Regarding the “dental care” time series, during the period under consideration, there
areRegarding
two periods the
Regarding theof“dental“dental
trend growthcare”Figure
care” timeseries,
time series, during
3a: the during
first (more the
the periodunder
under
pronounced)
period from consideration, there
the beginningthere
consideration,
are of
two2018 to the
periods beginning
of trend of
growth2019, and
Figure the second
3a: the (more
first (moresmoothed) from
pronounced)
are two periods of trend growth Figure 3a: the first (more pronounced) from the beginning the beginning
from the of
beginning
2020. to
of2018
2018 There was no downtrend
thebeginning
beginning 2019,during
of2019, andthe thesecond
the pandemic period.
(more Regarding
smoothed) fromthe “emergency
thebeginning
beginningofof
of to the of and second (more smoothed) from the
dental
2020. There care”
Therewas time
wasno series
nodowntrend (Figure
downtrendduring 3b), the
duringthe direction
thepandemic is multidirectional
pandemicperiod. (with
period.Regarding
Regarding local
theups and
“emergency
2020. the “emergency
downs) with a general upward trend. After reaching the minimum in 2018 through mid-
dentalcare”
dental care” timeseries
series(Figure
(Figure3b), 3b), thedirection
direction ismultidirectional
multidirectional(with (withlocal
localups
ups and
2020, theretime
was a significant increase,the
followed by aisshort-term moderate decline (proba- and
downs)
downs) with
bly during
a
with athe general
general upward
generalupward
lockdown).
trend.
trend. After
An After
upward
reaching
reaching
trend was
the minimum
theobserved
minimum since
in
inthe 2018
2018 through
through
second
mid-
half mid-
2020,
2020, there
of there was a significant
was a reached
2020, which significant increase, followed
increase, followed
its maximum values at the by
by end a short-term
a short-term moderate
moderate
of the period decline (proba-
decline (probably
under review.
bly during
during the general
the general lockdown).
lockdown). An upward
An upward trend trend
waswas observed
observed sincesince
the the second
second halfhalf
of
of 2020,
2020, which
which reached
reached its maximum
its maximum values
values at the
at the endend of the
of the period
period under under review.
review.
(a) (b)
Figure 3. Decomposition of time series (month granularity): (a) “dental care”; (b) “emergency dental care”.
(a) (b)
Figure3.3.Decomposition
Figure Decompositionof
oftime
timeseries
series(month
(monthgranularity):
granularity):(a)
(a)“dental
“dentalcare”;
care”;(b)
(b)“emergency
“emergencydental
dentalcare”.
care”.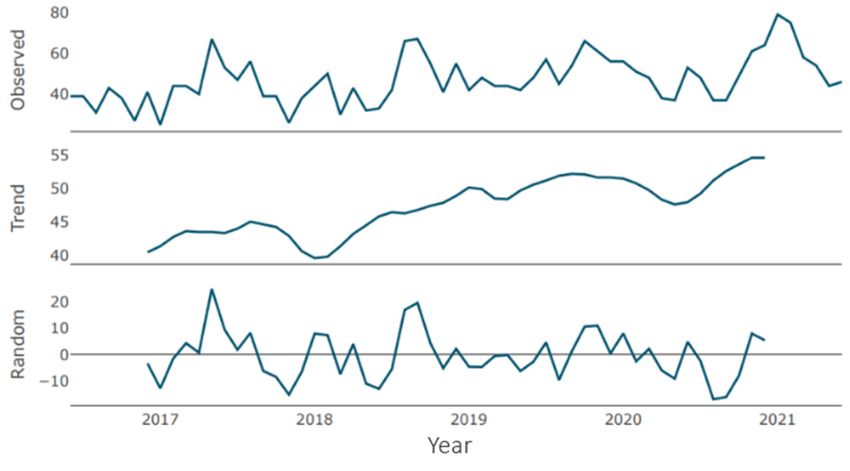
J. Clin. Med. 2021, 10, x FOR PEER REVIEW 5 of 12
J.J. Clin.
Clin. Med.
Med. 2021,
2021, 10,
10, 3532
x FOR PEER REVIEW 55 of
of 12
12
Regarding
Regardingthe the“oral
“oralhealth”
health”timetimeseries,
series,during
duringthe theperiod
periodunder
underconsideration,
consideration,there there
are Regarding the “oral health” time series, during the period under consideration, there
are two periods of trend growth Figure 4a: the first (minor one) from the
two periods of trend growth Figure 4a: the first (minor one) from the beginning
beginning of of
are two
2017 to theperiods
beginningof trend
of growth
2018, and Figure
the 4a: the
second (a first (minor one)
pronounced one) from
frommid-2018
the beginning to of
early
2017 to the beginning of 2018, and the second (a pronounced one) from mid-2018 to early
2017 to
2020. the beginning of 2018, and the second (a pronounced one) from mid-2018 to early
2020. Periods
Periods of of growth
growth are are followed
followed by by periods
periods of of decline
decline withwith similar
similar severity
severity and and du-du-
2020.
ration. Periods of growth are followed by periods of decline with similar severity and
ration. Since
Since the the beginning
beginning of of the
the pandemic,
pandemic, aa negative
negative trend
trend waswas recorded
recorded withwith small
small
duration.
periods Since the beginning of the pandemic, a negative trend wasnorecorded with small
periods of of stabilization
stabilization with with aa tendency
tendency to to smooth
smooth out.out. There
There were
were no upward
upward trends.
trends. In In
periods ofthe
mid-2021, stabilization
level of with aistendency
demand close to thetominimum
smooth out. valuesThere
for were
the no upward
period under trends.
review.
mid-2021,
In mid-2021, the the
level of demand
level ofthedemand is close to theto
is close minimum
theseries valuesvalues
minimum for the for
period
the under
period review.
under
Furthermore,
Furthermore, regarding
regarding the “periodontitis”
“periodontitis” time
time series (Figure
(Figure 4b),
4b), for
for most
most of
of the
the period
period
review.
under Furthermore,
review, the trend regarding the “periodontitis” time series (Figure 4b), for most of
under
the review,
period under trend was
thereview, was
the
characterized
characterized
trend was
as
as moderately
moderately
characterized as
growing
growing with
moderately with small
small corrections
growing corrections
with small
and
and short
short declines.
declines. Since
Since the
the beginning
beginning of
of 2019,
2019, there
there has been
has2019, protracted
beenthere
protracted growth,
growth, which
which
corrections
reached its and short
maximum declines.
during the Since the
pandemic. beginning
At the end ofof the period has
under been protracted
review, there
reached
growth, its
whichmaximum
reached during
its trend, the
maximum pandemic.
during At the end
the pandemic. of the period
At the under
end oflevels review,
the period there
under
is a slight
is a slight decrease
decrease in the
in the trend, inwhich,
which, however,
however, exceeds
exceeds the demand
theexceeds
demandthe levels of the pre-
of thelevels
pre-
review,
pandemic there is
period. a slight decrease the trend, which, however, demand
pandemic period.
of the pre-pandemic period.
(a)
(a) (b)
(b)
Figure 4. Decomposition of time series (month granularity): (a) “oral health”; (b) “periodontitis”.
Figure 4. Decomposition of time series
Figure 4. Decomposition of(month granularity):
time series (a) “oral health”;
(month granularity): (b) health”;
(a) “oral “periodontitis”.
(b) “periodontitis”.
Regarding
Regarding the the “teledentistry”
“teledentistry” timetime series
series (Figure
(Figure 5a),
5a), until
until thethe second
second half half ofof 2019,
2019,
the trend
the trend waswas an
was an almost
analmost flat
almostflat curve,
flatcurve, with
curve,with a barely
witha abarely
barelynoticeable
noticeable
noticeable increase,
increase,
increase, which
which
which is replaced
is replaced
is replaced by
by
abysharp
a sharp
a sharp growth
growth phase
growth
phase lasting
phase about
lasting
lasting about a year.
about The
a year.
a year. growth for
The growth
The growth the specified
forspecified
for the period
the specified was
periodperiod about
was aboutwas
20
20 points.
about
points. Then,
Then, the
20 points. the growth
Then, phase
the growth
growth was
was replaced
phasephase by
by aa moderate
was replaced
replaced decline
by a moderate
moderate decline phase,
decline
phase, which
phase,
which con-
which
con-
tinued
continueduntil the
until end
the of
end the
of period
the under
period under review.
review. Similarly,
Similarly, in
tinued until the end of the period under review. Similarly, in the “is it safe tointhe
the “is
“isititsafe
safe toto go
go to
to the
the
the
dentist”
dentist” time
time series
series (Figure
(Figure 5b),5b), until
until the
the second
second half
half of
of 2019,
2019, the
the trend
trend was
was
trend was flataa flat
flat line
line with
with
aa zero
zero value,
value, which
which waswas replaced
replaced byby aa phase
phase of of sharp
sharp growth
growth that
that lasted
lasted forforabout
for aboutaaayear.
about year.
year.
The growth for
The growth for the the indicated
the indicated period
indicated period was
period was about
was about 40
about 40 points.
40 points. Then, the
points. Then, the growthgrowth
growth phase phase gave
phase gave
gave
way
way to
way to aaa moderate
to moderate decline
moderate decline phase,
decline phase, which
phase, which lasted
which lasted until
lasted until the
until the end
the end of
end of the
of the period
the period under
period under review.
under review.
review.
(a)
(a) (b)
(b)
Figure
Figure5. Decomposition
Decompositionof time
timeseries
series(week
(weekgranularity):
granularity):(a)
(a)for
for“teledentistry”;
“teledentistry”;(b)
(b)for
for“is
“isitititsafe
safeto go
gototothe
thedentist”.
Figure 5.5.Decomposition ofoftime series (week granularity): (a) for “teledentistry”; (b) for “is safe totogo to the dentist”.
dentist”.
J.J. Clin.
Clin. Med. 2021, 10, 3532
x FOR PEER REVIEW of 12
6 of 12
The
The trend
trend line
line for
for both
both expressions
expressions in
in Figure
Figure 6a,b—“COVID-19”
6a,b—“COVID-19” and and “PPE
“PPE dentist”—
dentist”—
repeats the pattern of the previous pair. Until mid-2019, a horizontal
repeats the pattern of the previous pair. Until mid-2019, a horizontal line at line at the
the 00 level
level is
is
observed, after which the annual growth phase with a maximum increase
observed, after which the annual growth phase with a maximum increase of up to 30 points of up to 30
points is observed.
is observed. The growth
The growth phase phase is replaced
is replaced by a moderate
by a moderate decline
decline phase,phase,
whichwhich con-
continues
tinues until
until the endthe
of end of the period
the period underunder consideration
consideration (the volume
(the volume of decline
of decline for “COVID-
for “COVID-19”—
19”—5 points, for “PPE dentist”—10
5 points, for “PPE dentist”—10 points). points).
(a) (b)
Figure 6. Decomposition of time series
Figure 6. Decomposition (week
of time granularity):
series (a) for “COVID-19”;
(week granularity): (b) for “dentist
(a) for “COVID-19”; (b) forPPE”.
“dentist PPE”.
3.3. Cyclical
3.3. Cyclical and
and Random
Random Fluctuations
Fluctuations Indications
Indications Analysis
Analysis
In the
In the “dental
“dental care”
care” time
time series
series (Figure
(Figure 3a),3a), there
there isis aa single
single negative
negative peakpeak of
of average
average
severity in the second half of 2018. There were no positive peaks
severity in the second half of 2018. There were no positive peaks in the similar intensity. in the similar intensity.
When
When regarding
regarding the the “emergency
“emergency dental dental care”
care” timetime series
series Figure
Figure 3b,
3b, there
there are
are two
two peaks:
peaks:
the most pronounced at the beginning of the period (breaking through the 20 marks) and
the most pronounced at the beginning of the period (breaking through the 20 marks) and
slightly less
slightly less pronounced
pronounced in in the
the second
second halfhalf ofof 2018
2018 (approaching
(approaching the the 2020 marks).
marks). Negative
Negative
peaks
peaks ofof similar
similar intensity
intensity were
were notnot observed.
observed.
Regarding the “oral health”
Regarding the “oral health” time series time series (Figure
(Figure 4a),4a), there
there are
are several
several cycles
cycles ofof low
low
severity breaking
severity breaking through
through the the 10-point
10-point mark markin inboth
bothdirections.
directions.Moreover,
Moreover,ininthe the“perio-
“peri-
odontitis” time series (Figure 4b), there are several peaks of average severity approaching
dontitis” time series (Figure 4b), there are several peaks of average severity approaching
the 10-point mark in both directions. The most pronounced is the positive cycle at the end
the 10-point mark in both directions. The most pronounced is the positive cycle at the end
of the period under consideration.
of the period under consideration.
In the “teledentistry” time series (Figure 5a), there is one pronounced cycle with an
In the “teledentistry” time series (Figure 5a), there is one pronounced cycle with an
increase in the parameter of about 60 points, and there is one pronounced cycle with an
increase in the parameter of about 60 points, and there is one pronounced cycle with an
increase in the parameter of more than 40 points when describing the “is it safe to go to the
increase in the parameter of more than 40 points when describing the “is it safe to go to
dentist” time series (Figure 5b).
the dentist” time series (Figure 5b).
Two pronounced cycles are clearly visible in the “COVID-19” time series in Figure 6a—at
Two pronounced cycles are clearly visible in the “COVID-19” time series in Figure
the junction of 2019/2020 and in the first half of 2020, with an increase of about 35 points. No
6a—at the junction of 2019/2020 and in the first half of 2020, with an increase of about 35
pronounced negative peaks are observed. A series of peaks regarding the expression “PPE
points. No pronounced negative peaks are observed. A series of peaks regarding the ex-
dentist” at the junction of 2019/2020 with gains of more than 50 points is clearly visible. No
pression “PPE
pronounced dentist”
negative at the
peaks werejunction
recorded of (Figure
2019/2020 6b).with gains of more than 50 points is
clearly visible. No pronounced negative peaks were recorded (Figure 6b).
3.4. Changes in Request Average during COVID-19 Pandemic
3.4. Changes in Request Average during COVID-19 Pandemic
The mean of “dental care” time series request rate in the pre-pandemic period has
a rateThe
of mean of “dental
79.9; during the care” time series
pandemic, the meanrequest rate
rate was in increased
the pre-pandemic
to 80.2. period
Thus, hasfroma
rate of 79.9; during
the pandemic onset the pandemic,
to the present,the themean
“dental ratecare”
was requests
increasedmean to 80.2.
rateThus, from the
has remained
pandemic onset
particularly to the present,
unchanged the “dental
(the increasing ratecare” requests
is about 0.4%).mean rate has remained
Moreover, the mean partic-
of the
ularly unchanged
“emergency dental(the
care”increasing
time series rate is about
request rate0.4%).
in theMoreover,
pre-pandemic the mean
periodofhas
thea “emer-
rate of
gency dental
48.73, and care”the
during time series request
pandemic, the meanraterate
in the pre-pandemic
increased to 52.6. period has athe
Thus, from rate of 48.73,
pandemic
and
onset to the present, the main rate of “emergency dental care” increased by 7.9%.onset
during the pandemic, the mean rate increased to 52.6. Thus, from the pandemic The
to the of
mean present, the health”
the “oral main rate of “emergency
time series requestdental rate in care” increased by 7.9%.
the pre-pandemic Thehas
period mean of
a rate
the “oralduring
of 62.0; health” thetime series request
pandemic, the mean raterate
in the pre-pandemic
changed periodfrom
to 61.8. Thus, has the
a rate of 62.0;
pandemic
during
onset tothe
the pandemic,
present, thethe mean
“oral rate requests
health” changedmean to 61.8.
rateThus, from particularly
remained the pandemic onset to
unchanged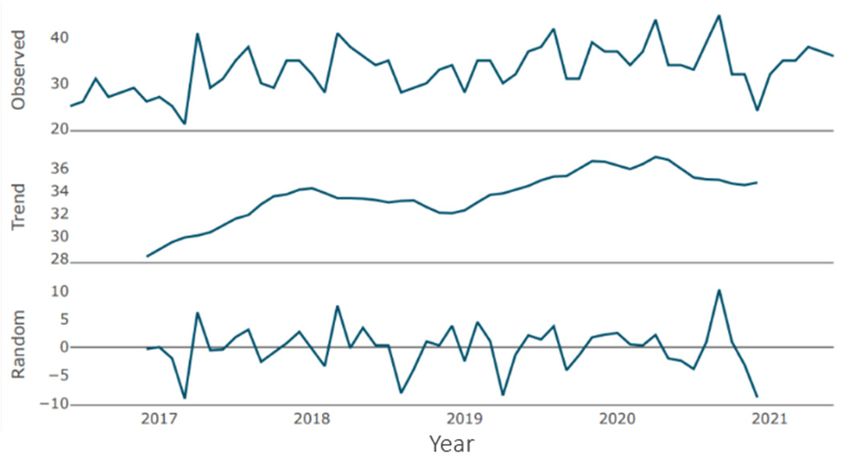
J. Clin. Med. 2021, 10, x FOR PEER REVIEW 7 of 12
J. Clin. Med. 2021, 10, 3532 7 of 12
the present, the “oral health” requests mean rate remained particularly unchanged (the
decreasing rate is about 0.3%). The mean of the “periodontitis” request rate in the pre-
pandemic period has a rate of 35.7; during the pandemic, the mean rate changed to 41.1.
(the decreasing rate is about 0.3%). The mean of the “periodontitis” request rate in the
Thus, from the pandemic onset to the present, the main rate of “periodontitis” increased
pre-pandemic period has a rate of 35.7; during the pandemic, the mean rate changed
by 15.1%. Moreover, the mean of the “teledentistry” time series request rate in the pre-
to 41.1. Thus, from the pandemic onset to the present, the main rate of “periodontitis”
pandemic period has a rate of 4.3; during the pandemic, the mean rate changed to 21.4.
increased by 15.1%. Moreover, the mean of the “teledentistry” time series request rate in
Thus, from the pandemic onset to the present, the “teledentistry” requests mean rate char-
the pre-pandemic period has a rate of 4.3; during the pandemic, the mean rate changed
acterized by a 5 times increase. The mean of the request rate for the “is it safe to go to the
to 21.4. Thus, from the pandemic onset to the present, the “teledentistry” requests mean
dentist” time series in the pre-pandemic period has a rate of 0.8; during the pandemic, the
rate characterized by a 5 times increase. The mean of the request rate for the “is it safe
tomean
go torate
the changed to 31.9.
dentist” time Thus,
series from
in the the pandemic
pre-pandemic onsethas
period to the present,
a rate of 0.8; the requests
during the
mean rate is characterized by an increase of almost 40 times. The mean
pandemic, the mean rate changed to 31.9. Thus, from the pandemic onset to the present, of the “PPE den-
tist”
the requestmean
requests rate inrate
theispre-pandemic
characterizedperiod has a rateofofalmost
by an increase 0.8; during the pandemic,
40 times. The mean theof
mean rate changed to 24.0. Thus, from the pandemic onset to the present,
the “PPE dentist” request rate in the pre-pandemic period has a rate of 0.8; during the “PPE den-
the
tist” request
pandemic, themean
meanraterateischanged
characterized
to 24.0.by an increase
Thus, from theofpandemic
30 times. onset
Whentoregarding the
the present,
“COVID-19”
the timerequest
“PPE dentist” series, this
meanexpression did not exist by
rate is characterized before the pandemic.
an increase of 30 times. When
regarding the “COVID-19” time series, this expression did not exist before the pandemic.
3.5. Cross-Correlation
3.5. Cross-Correlation
The time series pair “dental care”–“emergency dental” cross-correlation function
plotTheis shown in Figure
time series pair 7a. Therecare”–“emergency
“dental are a number of significant correlations onfunction
dental” cross-correlation both sides plotof
is0.shown
All significant
in Figure correlations
7a. There areare positive,
a number of from whichcorrelations
significant it follows, onan both
increase
sidesinofone pa-
0. All
rameter leads
significant to an increase
correlations in another.
are positive, from There
whichisit no significant
follows, correlation
an increase in oneatparameter
h = 0. Fur-
thermore,
leads the time in
to an increase series pair “oral
another. Therehealth”–“periodontitis”
is no significant correlation cross-correlation function the
at h = 0. Furthermore, plot
time seriesin
is shown pair “oral7b.
Figure health”–“periodontitis”
The correlation magnitude cross-correlation
and the number function plot is shown
of significant in
correla-
Figure
tions are7b. greater
The correlation magnitude
on the left side of 0. andThethemost
number of significant
dominant correlationsoccurs
cross-correlation are greater
at h =
on−2.the
The leftcorrelation
side of 0. The most dominant
is positive, indicating cross-correlation
that an above-average h = −2.
occurs at value ofThe
“oralcorrelation
health” is
islikely
positive, indicating
to lead that an above-average
to an above-average value of value of “oral health”
“periodontitis” about is likely tolater.
2 months lead to an
Addi-
above-average value of “periodontitis” about 2 months later. Additionally,
tionally, a below-average value of “oral health” is associated with a likely below-average a below-average
value of “oral health”
“periodontitis” valueisabout
associated
2 months withlater.
a likely below-average
Moreover, the time“periodontitis” value about
series pair “teledentistry”–
2“is
months
it safelater.
to goMoreover, the time
to the dentist” series pair “teledentistry”–“is
cross-correlation function plot is itshownsafe toingoFigure
to the7c.dentist”
There
cross-correlation function plot
are a number of significant is shown only
correlations in Figure
on the7c. There
right sideare
of a0.number of significant
All significant correla-
correlations only onFinally,
tions are positive. the right
theside
timeofseries
0. Allpair
significant correlationsdentist”
“COVID-19”–“PPE are positive. Finally,
cross-correla-
the time series pair “COVID-19”–“PPE dentist” cross-correlation
tion function plot is shown in Figure 7d. There are a number of significant correlations function plot is shown on
inboth
Figure 7d. There are a number of significant correlations on both sides
sides of 0. There is also a significant correlation at h = 0. All significant correlations of 0. There is
also
are apositive,
significant from correlation
which it at h = 0. All
follows, an significant
increase incorrelations
one parameter are positive,
leads to from which itin
an increase
follows, an increase in one parameter leads to an increase in another.
another. An above-average value of “COVID-19” is highly likely to lead to an above-av- An above-average
value
erageofvalue“COVID-19” is highlyabout
of “PPE dentist” likely 4toweeks
lead tolater.
an above-average value of “PPE
Since both expressions existeddentist”
in GT
about 4 weeks later. Since both expressions existed in GT searches
searches for less than 2 years, the use of month granularity was impossible, which is why,for less than 2 years, the
use of month granularity was
in this case, a week granularity was used.impossible, which is why, in this case, a week granularity
was used.
(a) (b)
Figure 7. Cont.
J. Clin. Med. 2021, 10, 3532
x FOR PEER REVIEW 8 of 12
(c) (d)
Figure 7.
Figure 7.Cross-correlation plots:
Cross-correlation (a) “dental
plots: care”–“emergency
(a) “dental dental”dental”
care”–“emergency (granularity: month); (b)
(granularity: “oral health”–“periodon-
month); (b) “oral health”–
“periodontitis” (granularity: month); (c) “teledentistry”–“is it safe to go to the dentist” (granularity:(d)
titis” (granularity: month); (c) “teledentistry”–“is it safe to go to the dentist” (granularity: month); “COVID-19”–“PPE
month); (d) “COVID-
dentist” (granularity:
19”–“PPE week).
dentist” (granularity: week).
4. Discussion
Discussion
The aim of the study was to investigate the impact of the the COVID-19
COVID-19 pandemic on
oral health and teledentistry subjects. To the best of our knowledge, this is one of the few
studies [19,20] tracing
tracing thetheGTGTexpressions
expressionsconnected
connectedwith withoral oralhealth
healthduring
during thethe
COVID-19
COVID-
pandemic.
19 pandemic. TheThefirstfirst
noticeable outcome
noticeable outcome of the
of research
the researchwas wasa large increase
a large in emergency
increase in emer-
dentaldental
gency care questions
care questionsaskedasked
during the spring
during lockdown
the spring lockdown in 2020 withwith
in 2020 a simultaneous
a simultane-
decrease
ous in regular
decrease in regular dental care
dental queries.
care queries. Our
Ourresults
resultsstrongly
stronglyshow showthat thatthe
the COVID-19
COVID-19
pandemic had significantly influenced dental-care-seekingdental-care-seeking behavior. According According to the
recommendations and
recommendations and because
because of of the
the fear
fear surrounding
surrounding the the epidemic,
epidemic, peoplepeople were were averse
averse
to be outside and less willing to visit dental studios. Moreover,
to be outside and less willing to visit dental studios. Moreover, dental care was not dental care was not widely
widely
available during
available duringthe theearly
earlyphase
phaseof of
thethepandemic,
pandemic, with
witha large number
a large of patients
number expected
of patients ex-
to seek emergency dental service only when urgent care
pected to seek emergency dental service only when urgent care was needed [5]. was needed [5]. In line with our
In line
study,our
with thestudy,
outcomes of the study
the outcomes conducted
of the by FaccinibyetFaccini
study conducted al. indicate
et al.that during
indicate thatthe hard
during
lockdown, 64.6% of dentists carried out only emergency treatments,
the hard lockdown, 64.6% of dentists carried out only emergency treatments, with 26.1% with 26.1% of dentists
stilldentists
of maintaining the routine planned
still maintaining the routine appointments, and with 9.3%
planned appointments, of dental
and with 9.3% offices
of closed
dental
for the duration of the lockdown. An increase in urgent dental
offices closed for the duration of the lockdown. An increase in urgent dental procedures procedures was noted by
44.1%
was of the
noted by dentists.
44.1% of the It occurred
dentists. most often most
It occurred due to the due
often lower availability
to the for a longer
lower availability for
period of time for regular dental care. The main causes of emergency
a longer period of time for regular dental care. The main causes of emergency appoint- appointments were
toothache,
ments weredental trauma,
toothache, dentalor trauma,
broken restorations [21]. Similarly,
or broken restorations a study conducted
[21]. Similarly, a study con- in
Beijing, in
ducted China, withChina,
Beijing, 2537 patients
with 2537 involved
patientsin involved
the study,inindicated
the study, that at the beginning
indicated that at theof
the COVID-19 pandemic, 38% fewer patients sought dental emergency care than before.
beginning of the COVID-19 pandemic, 38% fewer patients sought dental emergency care
Dental problems and oral infection increased from 51.0% in the pre-pandemic period to
than before. Dental problems and oral infection increased from 51.0% in the pre-pandemic
71.9% during the COVID-19 pandemic period [5]. A finding in line with our study is that
period to 71.9% during the COVID-19 pandemic period [5]. A finding in line with our
the COVID-19 pandemic outbreak had strongly influenced the emergency dental services.
study is that the COVID-19 pandemic outbreak had strongly influenced the emergency
The large influence of COVID-19 disease on oral cavity was shown in the study conducted
dental services. The large influence of COVID-19 disease on oral cavity was shown in the
by Gherlone et al., as 83.6% of patients reported anomalies of the oral cavity, such as dry
study conducted by Gherlone et al., as 83.6% of patients reported anomalies of the oral
mouth or salivary gland ectasia, that lasted even up to 3 months after hospitalization due
cavity, such as dry mouth or salivary gland ectasia, that lasted even up to 3 months after
to COVID-19 [22].
hospitalization due to COVID-19 [22].
According to recent studies, people with serious medical conditions such as diabetes,
According to recent studies, people with serious medical conditions such as diabetes,
heart diseases, lung or kidney chronic disease, and older persons were at high risk for de-
heart diseases, lung or kidney chronic disease, and older persons were at high risk for
veloping more severe COVID-19 infection. On the other hand, poor oral health and hygiene
developing
may increase more
the severe
risk ofCOVID-19
developinginfection. On the other hand,
the abovementioned medical poor oral health
problems. and hy-
Therefore,
giene may increase the risk of developing the abovementioned
improving oral health among the whole population may lead to a lower risk of developing medical problems. There-
fore, improving oral health among the whole population may
systemic diseases and, in this way, reduce the morbidity due to COVID-19 [9,23]. In lead to a lower risk of the
de-
veloping
study among systemic
a groupdiseases
of 568and, in thisthe
patients, way, reduce
higher riskthe
of morbidity
intensive care dueunit
to COVID-19
admission[9,23].
with
In the study among a group of 568 patients, the higher
the need for assisted ventilation and worse disease outcomes, leading even risk of intensive care unit toadmission
the death
with the needpatients,
of COVID-19 for assisted wasventilation
associated and withworse disease outcomes,
periodontitis. Similarly, leading
COVID-19 even to the
patients
death of COVID-19 patients, was associated with periodontitis.
with periodontitis had significantly higher blood levels of D-dimer and C-reactive protein Similarly, COVID-19 pa-
tients with periodontitis had significantly higher blood levels of D-dimer and C-reactive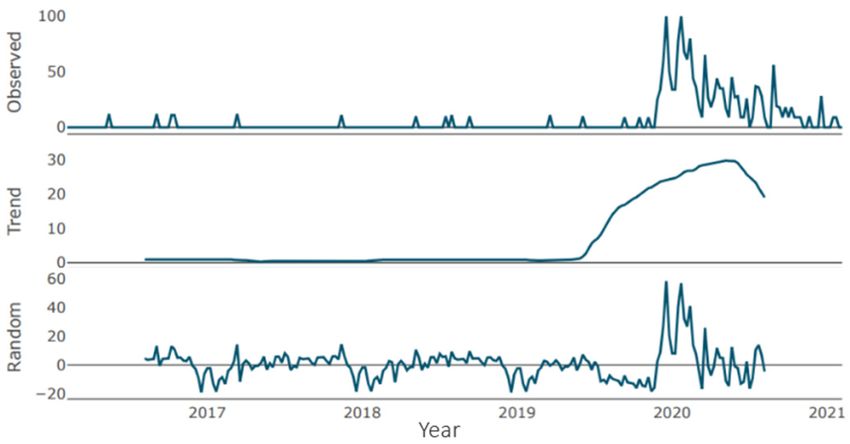
J. Clin. Med. 2021, 10, 3532 9 of 12
and white blood cells [24]. After a lower level of interest in oral health was detected in
the number of queries asked in GT during the hard lockdown, in the conducted study, we
detected a peak in periodontitis questions and about a 15% interest growth in the subject.
During the pandemic, telemedicine represented an opportunity to improve accessibil-
ity to medical treatments. According to some studies, teledentistry could be comparable to
face-to-face visits for oral screening, especially in areas with limited access to oral health
care. In fact, the identification of oral pathologies via teleconsultations is widely possible
and valid [25]. The online examination using intraoral scans may become helpful in de-
tecting dental problems. The remote assessment of intraoral scans can allow an efficient
screening and the correct triage of patients. Improved intraoral scans can provide even
three-dimensional images with true colors [26]. Nowadays, to minimize contact with the
patient and to ensure patient safety clinicians may follow up with patients online, for
example, through video calls. In the present study, a 5-time increase in query rates for
teledentistry during the COVID-19 pandemic was detected because of the anxiety to visit
the dentist. The query “is it safe to go to the dentist” increased the question rate during
the pandemic almost 40 times. It may indicate the usefulness of such a digital tool during
epidemiological threats. The screening for other chronic viral infections was previously
conducted in dental offices, for example, for HCV virus [27]; such easy, free-of-charge
prevention campaigns may use teleconsultation in the post-pandemic time.
In addition, specific recommendations and lots of preventive measures against COVID-19
were undertaken in dental offices with infection control strategies. The urgent need for den-
tal emergency care required fast delivery of the appropriate PPE. The initial shortage and
distribution challenges of PPE was seen globally [11,28], as well as the large interest in PPE
connected with dentists was observed in our study, with a 30-time increase of requests mean
rate. The patient management protocols were applied to reduce the risk of infection and to
prevent the spread of the cross-infection, for example, clinical triage for patient screening
with a questionnaire on recent disease symptoms, body temperature measurement, avoiding
crowding in the waiting room, a hand sanitizer available to patients before entering the oper-
ating rooms, and the use of PPEs and oral rinses with hydrogen peroxide before the dental
treatment [29–32]. The WHO recommended the use of FFP3 masks according to the European
terminology or N100, according to the United States nomenclature [33]. Members of the
oral healthcare team should be acquainted with the COVID-19 transmission and preventive
measures, as the oral cavity is an important site for COVID-19 infection and a potential route
of virus transmission [34]. Cross-infection control measures should be applied to all patients
because asymptomatic COVID-19 persons may also need emergency dental treatment [35].
This study has some limitations. Firstly, the analyzed data were collected from one
search engine; nevertheless, Google engine has nearly four billion users worldwide and
covers more than 90% of all queries on the internet, with near 7 billion queries per day. With
4.39 billion internet users worldwide, the number of Google users is globally nearly four
billion [36]. In our study, the GT request sample size for 5 years period is about big data
collections. Thus, the nature of the data and sample size is appropriate for the purpose and
nature of the study. Moreover, when considering the overlapping of expressions meaning,
in a small sample, it might be discussed as a limitation; however, the sample of expressions
gathered in the presented study is huge, the time of observation is long, and therefore,
it should not induce significant changes in results. Secondly, the study was carried out
globally, in order not to add too much manual categorization, by providing expressions in
different languages. When adding queries in many languages across countries, it becomes
more difficult to choose the best fitting expression used in a specific country. Finally, there
are no strict rules on how to analyze the GT in health care research [37]; on the other hand,
the GT data are recognized by the scientific community as a reliable source on the basis of
which scientific papers in various fields are published [38,39]. Because of the anonymized
approach of data collection, GT enables the analysis and forecasting of sensitive topics
especially in medicine [37,40–43]. Because of using the revealed and not stated users’
preferences, it is possible to obtain information that would be otherwise impossible to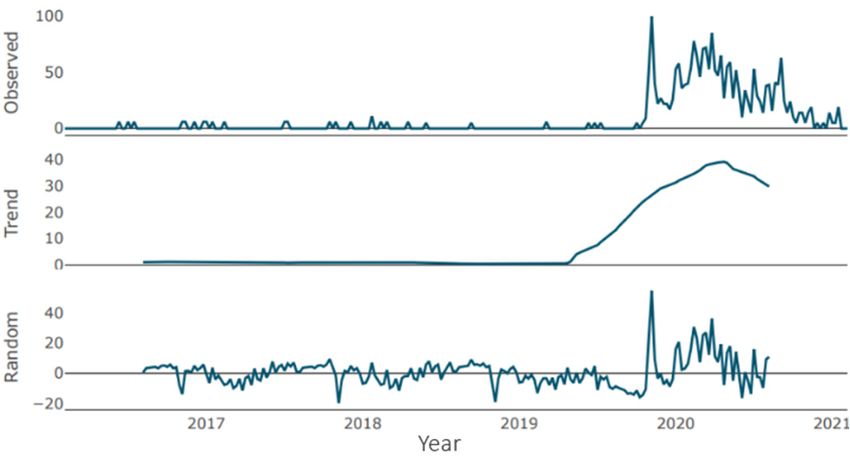
J. Clin. Med. 2021, 10, 3532 10 of 12
collect. Moreover, GT offers a substantial promise for the global monitoring of diseases in
countries that lack clinical surveillance but have sufficient internet coverage to allow for
surveillance via digital epidemiology [44].
5. Conclusions
1. Firstly, according to the search queries analysis from GT, the COVID-19 pandemic
had a large impact on oral health problems;
2. Moreover, emergency dental care became more required during the onset of pandemic
and hard lockdown than regular dental care;
3. Finally, teledentistry gained in popularity during the lockdowns according to globally
asked questions in GT service.
Author Contributions: Conceptualization, M.S.-D. and G.S.; methodology, M.S.-D.; software, M.S.-
D.; validation, M.S.-D. and M.M.; formal analysis, M.S.-D.; investigation, M.S.-D.; resources, M.S.-D.;
data curation, M.S.-D.; writing—original draft preparation, M.S.-D.; writing—review and editing,
M.S.-D., K.W., M.M., and G.S.; visualization, M.S.-D. and M.M.; supervision, G.S. All authors have
read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Institutional Review Board Statement: Not applicable.
Informed Consent Statement: Not applicable.
Data Availability Statement: The data presented in this study are available on request from the
corresponding author.
Conflicts of Interest: The authors declare no conflict of interest.
References
1. Worldometer—COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/?utm_
campaign=homeAdvegas1 (accessed on 28 June 2021).
2. Barca, I.; Novembre, D.; Giofrè, E.; Caruso, D.; Cordaro, R.; Kallaverja, E.; Ferragina, F.; Cristofaro, M.G. Telemedicine in Oral and
Maxillo-Facial Surgery: An Effective Alternative in Post COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7365.
[CrossRef]
3. Beauquis, J.; Petit, A.; Michaux, V.; Sagué, V.; Henrard, S.; Leprince, J. Dental Emergencies Management in COVID-19 Pandemic
Peak: A Cohort Study. J. Dent. Res. 2021, 100, 352–360. [CrossRef]
4. Cagetti, M.G.; Balian, A.; Camoni, N. Guglielmo Campus Influence of the COVID-19 Pandemic on Dental Emergency Admissions
in an Urgent Dental Care Service in North Italy. Int. J. Environ. Res. Public Health 2021, 18, 1812. [CrossRef]
5. Guo, H.; Zhou, Y.; Liu, X.; Tan, J. The impact of the COVID-19 epidemic on the utilization of emergency dental services. J. Dent.
Sci. 2020, 15, 564–567. [CrossRef]
6. Yu, J.; Zhang, T.; Zhao, D.; Haapasalo, M.; Shen, Y. Characteristics of Endodontic Emergencies during Coronavirus Disease 2019
Outbreak in Wuhan. J. Endod. 2020, 46, 730–735. [CrossRef] [PubMed]
7. Chakraborty, T.; Jamal, R.; Battineni, G.; Teja, K.; Marto, C.; Spagnuolo, G. A Review of Prolonged Post-COVID-19 Symptoms and
Their Implications on Dental Management. Int. J. Environ. Res. Public Health 2021, 18, 5131. [CrossRef] [PubMed]
8. Soltani, P.; Baghaei, K.; Tafti, K.T.; Spagnuolo, G. Science Mapping Analysis of COVID-19 Articles Published in Dental Journals.
Int. J. Environ. Res. Public Health 2021, 18, 2110. [CrossRef] [PubMed]
9. Campisi, G.; Bizzoca, M.E.; Muzio, L.L. COVID-19 and periodontitis: Reflecting on a possible association. Head Face Med. 2021,
17, 1–6. [CrossRef] [PubMed]
10. Echeverría, J.J.; Echeverría, A.; Caffesse, R.G. Adherence to supportive periodontal treatment. Periodontology 2019, 79, 200–209.
[CrossRef]
11. Mandrola, J. COVID-19 e dispositivi di protezione individuale: Qualcuno di noi morirà per la loro carenza. Recent. Prog. Med. 2020.
[CrossRef]
12. Campus, G.; Diaz-Betancourt, M.; Cagetti, M.G.; Carvalho, J.C.; Carvalho, T.S.; Cortés-Martinicorena, J.F.; Deschner, J.; Douglas,
G.V.; Giacaman, R.A.; Machiulskiene, V.; et al. Study Protocol for an Online Questionnaire Survey on Symptoms/Signs, Protective
Measures, Level of Awareness and Perception Regarding COVID-19 Outbreak among Dentists. A Global Survey. Int. J. Environ.
Res. Public Health 2020, 17, 5598. [CrossRef]
13. Top 10 Search Engines In The World (2021 Update). Available online: https://www.reliablesoft.net/top-10-search-engines-in-
the-world/ (accessed on 11 May 2021).
14. Google Trends. Available online: https://trends.google.com/trends (accessed on 20 August 2020).J. Clin. Med. 2021, 10, 3532 11 of 12
15. Wikipedia Google Trends. Available online: https://en.wikipedia.org/wiki/Google_Trends (accessed on 20 August 2020).
16. Archived: WHO Timeline—COVID-19. Available online: https://www.who.int/news/item/27-04-2020-who-timeline---covid-
19 (accessed on 15 May 2021).
17. R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed
on 11 August 2021).
18. RStudio|Open Source & Professional Software for Data Science Teams—RStudio. Available online: https://www.rstudio.com/
(accessed on 17 April 2021).
19. Sycinska-Dziarnowska, M.; Paradowska-Stankiewicz, I. Dental Challenges and the Needs of the Population during the COVID-19
Pandemic Period. Real-Time Surveillance Using Google Trends. Int. J. Environ. Res. Public Health 2020, 17, 8999. [CrossRef]
20. Sofi-Mahmudi, A.; Shamsoddin, E.; Ghasemi, P.; Bahar, A.M.; Azad, M.S.; Sadeghi, G. Association of COVID-19-imposed
lockdown and online searches for toothache in Iran. BMC Oral Health 2021, 21, 1–7. [CrossRef]
21. Faccini, M.; Ferruzzi, F.; Mori, A.A.; Santin, G.C.; Oliveira, R.C.; De Oliveira, R.C.G.; Queiroz, P.M.; Salmeron, S.; Pini, N.I.P.;
Sundfeld, D.; et al. Dental Care during COVID-19 Outbreak: A Web-Based Survey. Eur. J. Dent. 2020, 14, S14–S19. [CrossRef]
22. Gherlone, E.; Polizzi, E.; Tetè, G.; De Lorenzo, R.; Magnaghi, C.; Querini, P.R.; Ciceri, F. Frequent and Persistent Salivary Gland
Ectasia and Oral Disease After COVID-19. J. Dent. Res. 2021, 100, 464–471. [CrossRef] [PubMed]
23. Botros, N.; Iyer, P.; Ojcius, D.M. Is there an association between oral health and severity of COVID-19 complications? Biomed. J.
2020, 43, 325–327. [CrossRef]
24. Marouf, N.; Cai, W.; Said, K.N.; Daas, H.; Diab, H.; Chinta, V.R.; Hssain, A.A.; Nicolau, B.; Sanz, M.; Tamimi, F. Association
between periodontitis and severity of COVID-19 infection: A case–control study. J. Clin. Periodontol. 2021, 48, 483–491. [CrossRef]
[PubMed]
25. Alabdullah, J.H.; Daniel, S.J. A Systematic Review on the Validity of Teledentistry. Telemed. e-Health 2018, 24, 639–648. [CrossRef]
[PubMed]
26. Steinmeier, S.; Wiedemeier, D.; Hämmerle, C.H.F.; Mühlemann, S. Accuracy of remote diagnoses using intraoral scans captured
in approximate true color: A pilot and validation study in teledentistry. BMC Oral Health 2020, 20, 1–8. [CrossRef] [PubMed]
27. Tecco, S.; Parisi, M.R.; Gastaldi, G.; Polizzi, E.; D’Amicantonio, T.; Zilocchi, I.; Gardini, I.; Gherlone, E.; Lazzarin, A.; Capparè, P.
Point-of-care testing for hepatitis C virus infection at an Italian dental clinic: Portrait of the pilot study population. New Microbiol.
2019, 42, 133–138. [PubMed]
28. Dave, M.; Seoudi, N.; Coulthard, P. Urgent dental care for patients during the COVID-19 pandemic. Lancet 2020, 395, 1257.
[CrossRef]
29. Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus Disease 19 (COVID-19): Implications for Clinical
Dental Care. J. Endod. 2020, 46, 584–595. [CrossRef]
30. Villani, F.A.; Aiuto, R.; Paglia, L.; Re, D. COVID-19 and Dentistry: Prevention in Dental Practice, a Literature Review. Int. J.
Environ. Res. Public Health 2020, 17, 4609. [CrossRef] [PubMed]
31. Giudice, R.L.; Giudice, R.L. The Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) in Dentistry. Management of
Biological Risk in Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 3067. [CrossRef]
32. Gherlone, E.; Polizzi, E.; Tetè, G.; Capparè, P. Dentistry and COVID-19 Pandemic: Operative Indications Post-Lockdown. New
Microbiol 2021, 44, 1–11.
33. World Health Organization. Infection Prevention and Control of Epidemic- and Pandemic-Prone Acute Respiratory Infections in
Health Care. Available online: https://apps.who.int/iris/bitstream/handle/10665/112656/9789241507134_eng.pdf (accessed on
5 May 2021).
34. NIH COVID-19 Autopsy Consortium; HCA Oral and Craniofacial Biological Network; Huang, N.; Pérez, P.; Kato, T.; Mikami, Y.;
Okuda, K.; Gilmore, R.C.; Conde, C.D.; Gasmi, B.; et al. SARS-CoV-2 infection of the oral cavity and saliva. Nat. Med. 2021,
27, 892–903. [CrossRef] [PubMed]
35. Odeh, N.D.; Babkair, H.; Abu-Hammad, S.; Borzangy, S.; Abu-Hammad, A.; Abu-Hammad, O. COVID-19: Present and Future
Challenges for Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 3151. [CrossRef] [PubMed]
36. Revealing Google Statistics and Facts to Know in 2020. Available online: https://review42.com/resources/google-statistics-and-
facts/ (accessed on 13 July 2021).
37. Nuti, S.V.; Wayda, B.; Ranasinghe, I.; Wang, S.; Dreyer, R.P.; Chen, S.I.; Murugiah, K. The Use of Google Trends in Health Care
Research: A Systematic Review. PLoS ONE 2014, 9, e109583. [CrossRef] [PubMed]
38. Mavragani, A.; Ochoa, G. Google Trends in Infodemiology and Infoveillance: Methodology Framework. JMIR Public Health
Surveill. 2019, 5, e13439. [CrossRef]
39. Fabbian, F.; Rodríguez-Muñoz, P.; López-Carrasco, J.; Cappadona, R.; Rodríguez-Borrego, M.; López-Soto, P. Google Trends on
Obesity, Smoking and Alcoholism: Global and Country-Specific Interest. Healthcare 2021, 9, 190. [CrossRef] [PubMed]
40. Liu, M.; Caputi, T.L.; Dredze, M.; Kesselheim, A.S.; Ayers, J.W. Internet Searches for Unproven COVID-19 Therapies in the United
States. JAMA Intern. Med. 2020, 180, 1116–1118. [CrossRef] [PubMed]
41. Pelat, C.; Turbelin, C.; Bar-Hen, A.; Flahault, A.; Valleron, A.J. More Diseases Tracked by Using Google Trends. Emerg. Infect. Dis.
2009, 15, 1327–1328. [CrossRef] [PubMed]You can also read