Olfactory Neuroblastoma: Everything Radiologists Should Know
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Review article
Olfactory Neuroblastoma:
Everything Radiologists Should Know
Raquel Navas-Campo1 Leticia Moreno Caballero1 Ana Gasos Lafuente1 Pilar Tobajas Morlana1
Eduardo Séez Valero1 María José Gimeno Peribáñez1
1 Hospital Clínico Universitario Lozano Blesa, Zaragoza, Spain
Abstract
Olfactory neuroblastoma (ONB) is a rare malignant tumor that originates from olfactory neuroepithelial cells. Its early
diagnosis is difficult due to the low specificity of symptoms. Imaging tests play an important role in the diagnosis and
surgical planning of ONB; therefore, it is important that radiologists know the characteristic findings and the different
classifications that will help to choose the most appropriate treatment for each tumor.
Keywords
Olfactory neuroblastoma, Esthesioneuroblastoma, Cancer of the Head and Neck, Computed Tomography, Magnetic
Resonance Imaging
Introduction of life and the second peak in the sixth decade of life, some
recent studies support a uniform distribution across all ages,
Olfactory neuroblastoma (ONB) is a rare malignancy of the with a peak in the fifth and sixth decades of life.3,4,6.12,13
upper nasal cavity, also known as esthesioneuroblastoma, Nonspecificity of symptoms and local aggressiveness lead to
esthesioneuroepithelioma, esthesioneurocytoma or olfactory the development of locally advanced disease with submuco-
placode.1 It was first described by Berger et al.2 in 1924, and sal spread to the paranasal sinuses and the anterior cranial
the most widely accepted term at this time is “olfactory neu- fossa through the cribriform plate in a large number of pa-
roblastoma”.3,4 tients.14-16 Metastatic disease affects between 17% and 48%
The exact origin of this tumor, as well as the location and of patients.17 Cervical lymph nodes are the most common
cell type are under debate.5 Proposed anatomic sites of ori- sites of metastasis, with an incidence ranging between 20%
gin include Jacobson organ (vomeronasal organ), the sphe- and 30%, followed by the lung, bone and, rarely, the liver,
nopalatine ganglion, the ectodermal olfactory placode, Loci’s mediastinum, adrenal gland, ovary, spleen or parotid gland or
ganglion, sympathetic ganglia of the nasal mucosa, and the even the breast.12,18-24
nasal mucosa itself. However, the most likely site of origin of Imaging plays an important role in the diagnosis and surgical
ONB is the basal neural cells of the olfactory mucosa.5-7 This planning of ONB. Therefore, it is essential that radiologists
is supported by the fact that neural filaments are present in know the characteristic findings of ONB on the various imag-
tumor cells, as demonstrated by Trojanowaski et al.8 in 1982, ing modalities and the classifications that will help to choose
and by molecular analysis, as demonstrated by Carney et al.9 the most appropriate treatment for each tumor.
in 1995, with the expression of the Drosophila achaete-scute
gene (hASH1), involved in immature olfactory neuronal de-
velopment.5,6,10 Histology and immunohistochemistry
This tumor accounts for approximately 2% to 3% of all intra-
nasal malignancies.11 It affects both genders equally. It may Histologically, ONB is composed of small round blue cells
occur at all ages and, although it was thought to have a bi- slightly larger than mature lymphocytes. These cells pos-
modal age distribution with one peak in the second decade sess round-to-oval-shaped nuclei, with scanty cytoplasm and
Rev. Argent. Radiol. 2020;84(1): 17-31 17Olfactory Neuroblastoma: Everything Radiologists Should Know
sharply defined chromatin. They also have layers of malignant There is growing evidence in literature that this classification
cells organized into lobules through slender vascular fibrous may be used as an indicator for prognosis. High-grade tu-
septa, true neural rosettes (Flexner– Wintersteiner type) and mors in Hyams classification have been found to be associ-
pseudorosettes (Homer Wright type).23 ated with more aggressive locoregional disease and a worst
The differential diagnosis of ONB includes all small round survival outcome than low-grade tumors.4,34,35 Furthermore,
blue cell tumors occurring in the sinonasal tract. These in- Hyams classification may add value to guide the selection of
clude epithelial neoplasms such as sinonasal undifferentiated adjuvant therapy.34
carcinoma, sinonasal neuroendocrine carcinoma, squamous
carcinoma and melanoma; non-epithelial neoplasms such as
rhabdomyosarcoma, lymphoproliferative tumors and benign Clinical manifestations
lesions such as inverted papilloma and schwannoma.25
Differential diagnosis is possible, especially in cases of high- The most common presenting symptoms are nasal obstruc-
grade lesions, only by immunohistochemistry.26 The tumor tion followed by recurrent epistaxis. Other symptoms include
cells of ONB express neuronal markers such as synaptophy- headache, facial pain, hyposmia and rhinorrhea.36.45 Occa-
sin, chromogranin or neuron-specific enolase, as well as cal- sionally, it may occur as an asymptomatic nasal mass that
retinin, which differentiate them from other types of small is found incidentally.45 Advanced stage disease manifests
round blue cell tumors.27,28 with symptoms related to local extension beyond the nose
The cells in the periphery of the lobules are highly reactive and paranasal sinuses, such as epiphora, diplopy, proptosis
for protein S100. Cytokeratin is usually negative, although in and loss of visual acuity.36,43-45 Rarely, patients may present
some isolated cases it may exhibit an irregular expression.29 with symptoms of intracranial involvement, such as frontal
lobe symptoms and seizures.38,45 On rare occasions, paraneo-
plastic symptoms have been reported resulting from ectopic
Histological Classification hormonal secretion, including Cushing syndrome and hypo-
natremia secondary to adrenocorticotropic hormone (ACTH)
The histological grading system proposed by Hyams et al.30 and antidiuretic hormone (ADH) secretion, respectively.45-48
(Table 1) was developed in 1988 as an important tool for Locally, advanced disease may present signs of invasion and
prognosis, both of recurrence and survival..30,31 The criteria destruction of surrounding structures, such as the orbit,
underlying this classification are the mitotic activity, native brain, facial soft tissues and skin.3,6,38
architecture conservation, matrix features, nuclear poly- Because of the nonspecificity of the early symptoms of ONB,
morphism, the existence of rosettes and tumor necrosis.32 there is generally a delay in diagnosis, with an average time
This grading system stratifies tumors into four groups rang- of 6 to 12 months between the onset of symptoms and di-
ing from well differentiated (grade I) to least differentiated agnosis.3,6,19,38,49
(grade IV). This is a subjective complex system and sometimes
definitive separation into grades becomes difficult. For this
reason, there has been a tendency to group these categories Imaging Diagnosis
into low-grade, comprising grades I and II, and high-grade,
comprising grades III and IV, in order to provide and easier Imaging is very important in the diagnosis and staging of
description of these tumors in correlation with prognosis.33 ONB. Generally, a combination of computed tomography
Table 1: The Hyams histological grading system. * HW rosettes: true rosettes (Flexner– Wintersteiner type). * FW Pseudoro-
settes (Homer Wright type).
GRADE Preservation of Mitotic Nuclear Fibrillary Rosettes Necrosis
lobular architecture index polymorphism matrix
I + None None Prominent HW rosettes None
II + Low Moderate Present HW rosettes None
III +/- Moderate Prominent Present FW pseudorosettes Rare
IV +/- High Marked Absent None Frequent
18 Rev. Argent. Radiol. 2020;84(1): 17-31R. Navas-Campo et al.
(CT) and magnetic resonance imaging (MRI) is required for 12).55 On MRI, ONB appears hypointense to gray matter on
an optimal evaluation of the extent of the tumor.38,49 Both T1-weighted images and iso- to hyperintense to gray matter
tests allow diagnosis, definition of the extent and stage of on T2-weighted images (Figs. 10-15).56 The tumor demon-
the tumor and of the surgical approach, and monitoring and strates homogeneous enhancement except for areas of ne-
evaluation of the treatment response. crosis or hemorrhage. In addition, MRI can differentiate the
Thin-slice CT scan (1-mm slice thickness) with reconstruction tumor from entrapped secretions, which are hyperintense on
in coronal and sagittal planes is the best initial imaging test T2-weighted images.53,55 The classic imaging findings include
for assessing ONB. On CT, ONB appears as a homogeneous a “dumbbell-shaped” mass extending across the cribriform
soft-tissue mass in the nasal vault with uniform and moderate plate (Fig. 12), with the narrow portion at the cribriform
contrast enhancement (Figs. 1 and 2). Scattered speckled cal- plate. Peripheral tumor cysts (Figs. 5b, 12, 14, 16) and speck-
cifications may be present (Figs. 2-4, 5a, 6).50 The main value led calcifications are quite characteristic of ONB.1
of CT is that it provides better definition of bone involvement MRI fat-saturated sequences help distinguish tumor from or-
than MRI. CT helps to evaluate bone erosion of the cribriform bital fat and muscle. A smooth margin of the tumor-fat inter-
plate, fovea ethmoidalis and lamina papyracea (Figs. 1-4, 5a, face suggests that the lesion is contained by periorbital fascia
8). However, bone remodeling without erosion may occur in (Fig. 15), while an irregular margin favors frank invasion of
some cases due to the indolent growth pattern.3,35,49 CT scans the orbit.35,49,57 However, the definitive diagnosis of invasion
generally show a lytic pattern and very rarely dominant hy- of dura and periorbital tissues is possible only at surgery.49
perostosis mimicking fibrous dysplasia.51 CT is also useful to Imaging of the neck in patients with ONB is crucial because
assess regional neck and distant metastasis.52,53 neck lymph nodes metastases are found at presentation in
MRI is the imaging modality of choice for a detailed evalua- 5% of patients.33 Furthermore, it has been estimated that
tion of the locoregional extent and staging of the tumor. MRI over 23% of patients may develop cervical lymph node me-
is superior to CT for defining the soft tissue extent (Fig. 9) tastasis.20 Howell et al.52 described a predictable pattern of
with a better assessment of intracranial (Figs. 10-14), orbital metastasis to cervical lymph nodes, typically involving level
(Figs. 14 and 15) and skull base involvement and of perineu- II lymph nodes (93%), with frequent involvement of level I
ral invasion. 53,55 MRI has added value in distinguishing du- lymph nodes (57%), level III lymph nodes (50%) and retro-
ral involvement from brain parenchymal involvement (Fig. pharyngeal lymph nodes (43%).
a b
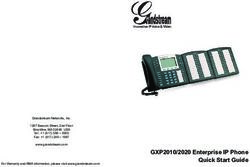
Fig. 1 (a) Axial CT scan of the head without intravenous contrast. Homogeneous soft tissue
space-occupying lesion occupying the left nasal cavity (white asterisk) and extending to the
left choana (black arrow) with bone destruction and extension to the left maxillary sinus (black
asterisk). (b) Axial CT scan of the head with iodinated intravenous contrast. After contrast ad-
ministration, the lesion shows moderate enhancement.
Rev. Argent. Radiol. 2020;84(1): 17-31 19Olfactory Neuroblastoma: Everything Radiologists Should Know
a b
Fig. 2 Axial CT scan of the head (a) without intravenous contrast and (b) with iodinated intra-
venous contrast. Homogeneous soft tissue mass with small speckled calcifications inside (black
arrows), occupying the nasal cavities with bone destruction and extension into both maxillary si-
nuses (black asterisks), as well as caudal extension posterior to the nasopharynx (white asterisk).
a b
Fig. 3 (a) Axial CT scan of the head without intravenous contrast. Bulky soft tissue mass oc-
cupying the nasal cavities and involving both orbits (black asterisks), predominantly the right
orbit and the sphenoidal sinus (white asterisks). The mass contains calcifications (black arrow).
(b) Axial CT scan of the head with iodinated intravenous contrast. After intravenous contrast
administration, the mass presents homogeneous moderate enhancement.
20 Rev. Argent. Radiol. 2020;84(1): 17-31R. Navas-Campo et al.
Fig. 4 Axial CT scan of the head (a) without intravenous contrast and (b) with iodinated intra-
venous contrast. (c) Coronal multiplanar reconstruction (MPR) from CT scan of the head with
iodinated intravenous contrast. Nasal cavity lesion with speckled calcifications inside (black ar-
rows), enhancing with contrast and causing bone destruction with invasion of both orbits (black
asterisks) and of the frontal sinus with frontal intracranial extension (white arrows).
a b
Fig. 5 Axial CT scan of the head without intravenous contrast. (a) Bulky soft tissue mass with
speckled calcifications inside (black arrows) occupying the nasal cavity and causing bone de-
struction extending to the right orbit and frontal sinus (black asterisk). (b) The mass also extends
to the anterior cranial fossa, where it presents cystic content in its posterior pole (white aster-
isk) and perilesional edema (white arrow). Significant mass effect with compression of the left
frontal horn and midline shift to the right. There is also presence of several associated sites of
parenchymal bleeding (white arrowhead).
Rev. Argent. Radiol. 2020;84(1): 17-31 21Olfactory Neuroblastoma: Everything Radiologists Should Know
a b
Fig. 6 (a) Axial CT scan of the head with iodinated intravenous contrast shows soft tissue mass
with small speckled calcifications inside (white arrow), causing bone destruction with extraconal
left intraorbital extension compressing the left medial rectus muscle (black asterisk), as well as
extension to bilateral anterior ethmoidal cells. (b) Axial CT scan of the head with iodinated intra-
venous contrast. Extension of the soft tissue lesion to the left frontal sinus (white asterisk) with
bone destruction (black arrow) and extracranial extension to the anterior fossa.
a b
Fig. 7 (a) Coronal MPR from CT scan of the head with iodinated intravenous contrast. Large soft
tissue mass occupying the left nasal cavity with bone destruction and left intraorbital extension
(black asterisk), extension to the left maxillary sinus (black arrow), destruction of the floor of the
left frontal sinus and destruction of the left cribriform plate and intracranial extension (white
arrow). (b) Coronal MPR from CT scan of the head with bone window. The scan shows destruc-
tion of the lamina papyracea, ethmoidal cells, left lacrimal bone, left orbital plate, left cribriform
plate and the crista galli.
22 Rev. Argent. Radiol. 2020;84(1): 17-31R. Navas-Campo et al.
a b
Fig. 8 Coronal MPR from CT scan of the head with iodinated intravenous contrast (a) soft tissue
window and (b) bone window. Bulky mass occupying the nasal cavities with extension to both
orbits, predominantly to the right orbit (black asterisk) and frontal sinus. Bone destruction of the
lamina papyracea, orbital plate and cribriform plate. Parenchymal intracranial extension with
extensive left frontal involvement (black arrow) and associated edema (white arrow), causing
mass effect with subfalcine herniation and midline shift to the right (white arrowhead).
Fig. 9 Axial MRI of the head. (a) FLAIR sequence. (b) T2-weighted sequence. (c) Diffusion-
weighted sequence and (d) T1-weighted sequence with paramagnetic contrast (Gadolinium).
Space-occupying lesion located in the nasal cavity causing bone destruction and invasion of
the left maxillary sinus (black asterisk). The mass exhibits moderately restricted diffusion and
enhances after paramagnetic contrast administration.
Rev. Argent. Radiol. 2020;84(1): 17-31 23Olfactory Neuroblastoma: Everything Radiologists Should Know
One of the most frequent distant metastases is to bone, based on the TNM system (table 4) with a more detailed de-
with the spine being the most common site (86%).58 Cases scription of the local extension of disease and considering
of asymptomatic bone metastases have been described and, distant metastases and spread to cervical lymph nodes. In T1,
therefore, a bone scan should be included in the diagnostic the tumor involves the nasal cavity and/or paranasal sinuses
work-up.33 (excluding the sphenoid), sparing the most superior eth-
The evaluation of recurrent tumor must include both CT and moidal cells; in T2, the tumor involves the nasal cavity and/or
MRI. The imaging characteristics of the recurrent tumor do paranasal sinuses, including the sphenoid, with extension to
not differ from its appearance at initial presentation. The fol- or erosion of the cribriform plate; in T3, the tumor extends
lowing follow-up protocol has been suggested for an early into the orbit or protrudes into the anterior cranial fossa with
detection of recurrence: contrast-enhanced MRI performed no dural invasion and in T4, the tumor involves the brain.
at 2 to 4 months after completion of all therapy. Then, MRI is Disease is classified as N0 if there is no cervical lymph node
repeated every 4 to 6 months for 5 years and from then on- involvement, as N1 for any form of cervical lymph node in-
wards, annually for the patient’s lifetime.59 The MRI protocol volvement, as M0, if there is no metastasis and as M1 if there
used in our service consists of T1-, T2- and fat-suppressed is evidence of distant metastasis.
T1-weighted images with and without contrast administra-
tion for sinonasal evaluation, and T1-weighted, T2-weighted,
FLAIR, DW-EPI and T1-weighted sequences with contrast ad- Treatment
ministration for brain evaluation. In addition, a chest radio-
graph should be performed annually to exclude the presence The treatment modalities used and the expected outcomes
of metastasis.59 depend on the tumor extension and histological grade. Ex-
cept for cases of very early-stage and limited disease, mul-
timodality therapy offers the best opportunity for cure.5
Imaging classification/Staging Surgery followed by radiation therapy is considered as the
standard therapy by most expert centers.5,39
Several staging systems have been proposed for ONB, but no The traditional surgical approach for ONB is anterior craniofa-
single system is universally accepted. cial resection, involving a bifrontal craniotomy combined with
The first to propose a classification was Kadish. In this clas- a transfacial lateral rhinotomy.63 This surgical procedure is
sification, tumors were divided into three categories accord- performed, if needed, by a team of neurosurgeons and oto-
ing to their extension: Group A, the tumor is confined to the laryngologists. In the last two decades, endoscopic approach-
nasal cavity; Group B, the tumor extends into the paranasal es have gained popularity, producing comparable oncologic
sinuses; and Group C, the tumor extends beyond the para- outcomes, limiting surgical morbidity and the duration of
nasal sinuses.18 hospital stay.64 Initially, these approaches were recommended
This classification was modified in 1993 by Morita et al., 60 only for early-stage disease with minimal invasion of the skull
who added stage D for the spread to cervical lymph nodes base. However, with advances in endoscopic techniques and
and distant metastasis (Table 2).19,61 Some studies have re- reconstruction methods, they are being increasingly used for
ported that the modified Kadish staging system may be a advanced-stage disease with extensive invasion, allowing
useful predictor of survival.12,49 In their study, Jethanametest complete resection.65
et al.12 found that in this classification, lymph node involve- Contraindications for purely endoscopic approaches include
ment and the age at the time of diagnosis were prognostic involvement of the anterior table of the frontal sinus, skin
factors. However, the rarity of the disease makes it difficult to and subcutaneous tissue, the nasolacrimal sac, the carotid
validate the staging systems, and the prognostic value of this artery and extensive intraorbital and brain parenchymal in-
classification has not been confirmed in other studies such as vasion. Furthermore, lateral extension above the orbit and
the one conducted by Konuthula et al.62 palatine invasion are also considered as contraindications for
In 1990, Biller et al61 proposed an additional classification purely endoscopic approaches and, in such cases, traditional
(Table 3), in which T1 indicates that the tumor involves the craniofacial approaches are indicated.63,66 Regardless of the
nasal cavity and paranasal sinuses, excluding the sphenoid, approach, complete resection with negative margins should
with or without erosion of the bone of the anterior cranial be achieved in all cases.63
fossa; in T2 the tumor extends into the orbit or protrudes into Postoperative radiation therapy has been shown to improve
the anterior cranial fossa, in T3 the tumor involves the brain local control of disease. However, no benefit has been dem-
with resectable margins, and in T4 the tumor is unresectable. onstrated in terms of long-term overall survival for adjuvant
Dulgerov and Calcaterra19 proposed in 1992 a classification radiotherapy.13,62,67 Conformed radiotherapy techniques such
24 Rev. Argent. Radiol. 2020;84(1): 17-31R. Navas-Campo et al.
a b
Fig. 10 Coronal MRI of the head. (a) T2-weighted sequence and (b) T1-weighted sequence.
Space-occupying mass of slightly heterogeneous intensity, predominantly hyperintense to gray
matter on T2-weighted sequence and slightly hypointense on T1-weigthted sequence, occupy-
ing the left nasal cavity. The scan shows bone destruction with destruction of the left lamina
papyracea, extraconal left intraorbital extension with compression of the left medial rectus
muscle and no apparent infiltration of the muscle (black arrow), infundibular extension to the
medial wall of the left maxillary sinus (white arrow), destruction of the floor of the left frontal
sinus with extension to the sinus, destruction of the left cribriform plate with extra-axial incra-
cranial extension in the left frontobasal anterior fossa, apparently contained by the dura, with
a doubtful dural disruption that might be an indication of minimal occupation of the subdural
space (white arrowhead).
a b
Fig. 11 Kadish stage C esthesioneuroblastoma. (a) and (b) Coronal T2-weighted MRI of the
head. Bulky space-occupying lesion with heterogeneous signal intensity, located at the level of
the nasal cavity (black asterisk), with bone destruction, invading orbits (white arrow), as well
as paranasal sinuses (black arrow), nasopharynx and anterior brain fossa (white arrowhead),
where peripheral cystic component is noticed (black arrowhead).
Rev. Argent. Radiol. 2020;84(1): 17-31 25Olfactory Neuroblastoma: Everything Radiologists Should Know
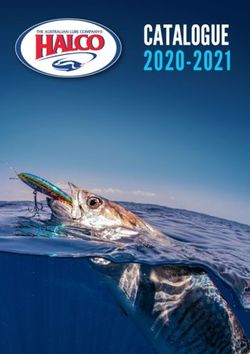
Fig. 12 Axial MRI of the head. (a) T1-weighted sequence shows a lesion that is slightly hypoin-
tense to gray matter, occupies the left frontal sinus (black asterisk) and destroys the posterior
wall of the sinus extending to the anterior cranial fossa (white arrow). (b) On the fat-suppressed
T2-weighted image, the lesion is hyperintense to gray matter. (c) T1-weighted sequence with
paramagnetic (Gadolinium) contrast and (d) fat-suppressed T1-weighted image with paramag-
netic (Gadolinium) contrast. These sequences show a homogeneous enhancement of the lesion
and evidence of subdural infiltration with no extension to the brain.
Fig. 13 Axial MRI of the head. (a) FLAIR sequence. (b) T2-weighted sequence. (c) Diffusion-
weighted sequence and (d) T1-weighted sequence with paramagnetic (Gadolinium) contrast.
Involvement of the anterior cranial fossa by a nasal cavity mass (black asterisk), causing signifi-
cant mass effect at the encephalic level, with presence of peripheral cystic cavity (black arrow)
and significant perilesional edema of finger-like morphology (black arrowhead), causing subfal-
cine herniation (white arrow). The mass has heterogeneous signal intensity, being hyperintense
to gray matter on T2-weighted sequences, exhibiting moderately restricted diffusion and slight
enhancement after paramagnetic contrast administration.
26 Rev. Argent. Radiol. 2020;84(1): 17-31R. Navas-Campo et al.
Fig. 14 Axial MRI of the head. (a) T1-weighted sequence. (b) T2-weighted sequence. (c) T1-
weighted sequence with paramagnetic (Gadolinium) contrast and (d) fat-suppressed T1-
weighted sequence with paramagnetic (Gadolinium) contrast. Space-occupying mass that ap-
pears hypointense to gray matter on T1-weighted sequences and moderately hyperintense on
T2-weighted sequences with heterogeneous contrast enhancement, occupying the left nasal
cavity (black asterisk) and ethmoidal cells and destroying the left orbital plate, with extraconal
intraorbital extension (white asterisk) and compression of the left medial rectus muscle with no
apparent infiltration of the muscle. This can be better visualized on fat-saturated sequences (d),
where a hypointense line can be seen between the lesion and the muscle (tumor-fat interface)
(white arrows), suggesting that the lesion is contained within the periorbital fascia.
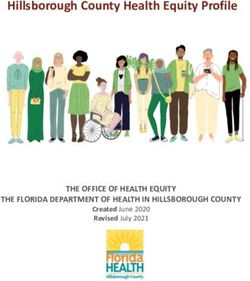
Fig. 15 Axial MRI of the head. (a) FLAIR sequence. (b) T2-weighted sequence. (c) Diffusion-
weighted sequence and (d) T1-weighted sequence with paramagnetic (Gadolinium) contrast.
Space-occupying mass located in the nasal cavity and ethmoidal cells, exhibiting bone destruc-
tion (black asterisk) and extraconal orbital invasion (white asterisk). The mass is slightly hyperin-
tense to gray matter on T2-weighted sequences and exhibits moderate restricted diffusion and
a slight enhancement after paramagnetic contrast administration.
Rev. Argent. Radiol. 2020;84(1): 17-31 27Olfactory Neuroblastoma: Everything Radiologists Should Know
a b
Fig. 16 Axial CT scan of the head (a) without intravenous contrast and (b) with iodinated intrave-
nous contrast. Parenchymal intracranial extension with extensive left frontal involvement occu-
pying the midline. Brain parenchymal mass effect with surrounding edema (white arrows) and
associated subfalcine herniation with midline shift to the right (black arrows). After intravenous
contrast administration, a cystic component is seen in the left frontal region (white asterisk).
Table 2: Kadish classification modified by Morita et al.
STAGE DESCRIPTION
A Tumor confined to the nasal cavity.
B Tumor extends into the paranasal sinuses
C Tumor extends beyond the paranasal sinuses, including the cribriform plate, the skull base,
the intracranial cavity and orbit.
D Tumor with spread to cervical lymph nodes and/or distant metastasis.
Table 3: Biller’s classification.
GRADE DESCRIPTION
T1 Tumor involves the nasal cavity and paranasal sinuses, excluding the sphenoid, with or without erosion
of the bone of the anterior cranial fossa
T2 Tumor extends into the orbit or protrudes into the anterior cranial fossa.
T3 Tumor involves the brain with resectable margins
T4 Unresectable tumor
28 Rev. Argent. Radiol. 2020;84(1): 17-31R. Navas-Campo et al.
Table 4: Classification based on the TNM system by Dulgerov and Calcaterra.
CLASSIFICATION DEFINITION
TUMOR
T1 Tumor involves the nasal cavity and/or paranasal sinuses (excluding the sphenoid) sparing the
most superior ethmoidal cells
T2 Tumor involves the nasal cavity and/or paranasal sinuses, including the sphenoid, with extension
to or erosion of the cribriform plate
T3 Tumor extends into the orbit or protrudes into the anterior cranial fossa with no dural invasion
T4 Tumor involves the brain
LYMPH NODES
N0 No cervical lymph node involvement.
N1 Any form of cervical lymph node involvement
METASTASIS
M0 No metastases
M1 Distant metastases
as intensity-modulated radiotherapy and proton-beam radia- surgery alone and surgery with adjuvant radiotherapy were
tion have shown better outcomes, improving local control compared among the different modified Kadish stages, there
and minimizing toxicity and complications in critical sur- was also no differences in survival between the two groups in
rounding structures.5,68 stages A, B and D. However, for patients with Kadish stage C,
In general, chemotherapy may be considered in patients with surgery with adjuvant radiotherapy had better survival rates
advanced tumor stage, high Hyams grade, extensive regional than surgery alone.62
disease, distant metastasis, positive margins, unresectable
tumors and recurrent tumors.69 There is no standard chemo-
therapy regime for treating ONB. Some authors reported the Conclusion
use of cyclophosphamide, vincristine and doxorubicin, while
others considered the use of cisplatin-based regimens.70 Olfactory neuroblastoma is a rare malignancy. The diagnosis
Cisplatin in combination with etoposide appears to be the of this tumor is based on imaging tests, pathology examina-
most widely accepted regimen used for ONB.71,72 Adjuvant tion and immunohistochemistry. Therefore, radiologists play
chemotherapy may contribute to improve locoregional con- a crucial role in its diagnosis. For this reason, they should be
trol and extend the mean time to relapse. However, it does aware of the characteristic findings on the different imaging
not improve overall survival.68 tests (CT and MRI), and of the various staging systems avail-
Overall survival rates are inconsistent between various stud- able for diagnosing its extension. Optimal therapy depends
ies. Konuthula et. Al62 analyzed survival in 1,107 patients on the tumor extension and histological grade, with the
using data from the National Cancer Database (NCDB) and treatment of choice being multimodality therapy with com-
found that survival with different modalities of treatment was bined surgery and radiation with or without chemotherapy,
not clear because of the low patient numbers. Although a although this depends on each center’s experience.
combination of surgery and radiation therapy has been used
most frequently and has been shown to have a survival of Ethical responsibilities
around 65%, many patients are still being treated with sur- Protection of human subjects and animals. The authors
gery or RT alone, as no statistically significant difference has declare that no experiments were performed on humans or
been shown for the different treatment modalities. When animals for this investigation.
Rev. Argent. Radiol. 2020;84(1): 17-31 29Olfactory Neuroblastoma: Everything Radiologists Should Know
Confidentiality of data. The authors declare that they have 17 Levine PA, McLeanWC, Cantrell RW. Esthesioneuroblastoma: the Univer-
sity of Virginia experience 1960-1985. Laryngoscope. 1986;96(07):742–
followed the protocols of their work center on the publica- 746
tion of patient data. 18 Kadish S, Goodman M, Wang CC. Olfactory neuroblastoma. A clinical
analysis of 17 cases. Cancer. 1976;37(03):1571–1576
Right to privacy and informed consent. The authors de-
19 Dulguerov P, Calcaterra T. Esthesioneuroblastoma: the UCLA experience
clare that no patient data appear in this article. 1970-1990. Laryngoscope. 1992;102(08):843–849
Sources of funding. There have been no sources of funding 20 Rinaldo A, Ferlito A, Shaha AR, Wei WI, Lund VJ. Esthesioneuroblastoma
and cervical lymph node metastases: clinical and therapeutic implications.
for this study. Acta Otolaryngol. 2002;122 (02):215–221
21 Monroe AT, Hinerman RW, Amdur RJ, Morris CG, Mendenhall WM. Radia-
tion therapy for esthesioneuroblastoma: rationale for elective neck irradia-
Conflicts of interest tion. Head Neck. 2003;25(07):529–534
The authors declare no conflicts of interest. 22 Davis RE, Weissler MC. Esthesioneuroblastoma and neck metastasis. Head
Neck. 1992;14(06):477–482
23 Winn HR. Youmans neurological surgery: brain, spine, and peripheral
Acknowledgements nerve trauma in adults and children. Elsevier Health Sciences; 2014
We would like to thank all our colleagues involved in this 24 Larbcharoensub N, Kanoksil W, Cheewaruangroj W, Wiratkapun C, Sita-
thanee C, Sirachainan E. Esthesioneuroblastoma metastasis to the breast:
study for their support and cooperation. A case report and review of the literature. Oncol Lett. 2014;8(04):1505–
1508
25 Schuster JJ, Phillips CD, Levine PA. MR of esthesioneuroblastoma (olfac-
tory neuroblastoma) and appearance after craniofacial resection. AJNR
References Am J Neuroradiol. 1994;15(06):1169–1177
26 Shah K, Perez-Ordóñez B. Neuroendocrine neoplasms of the sinonasal
1 Bell D, Franchi A, Gillison M, Thompson LDR,Wenig BM. Olfactory neuro- tract: neuroendocrine carcinomas and olfactory neuroblastoma. Head
blastoma. En: El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ, Neck Pathol. 2016;10(01):85–94
eds. WHOclassification of head and neck tumors. 4th ed. Lyon: IAC Press; 27 Bell D, Hanna E, Weber R, DeMonte F, Triantafyllou A, Lewis Jr, et al. Neu-
2017:57–59 roendocrine neoplasms of the sinonasal region. Head Neck. 2016;38(Sup-
2 Berger L, Luc R, Richard D. L’esthesioneuroepitheliome Olfactif. Bull Assoc pl 1):E2259–E2266
Fr Etud Cancer. 1924;13:410–421 28 Wooff JC, Weinreb I, Perez-Ordonez B, Magee JF, Bullock MJ. Calretinin
3 Su SY, Bell D, Hanna EY. Esthesioneuroblastoma, neuroendocrine carci- staining facilitates differentiation of olfactory neuroblastoma from other
noma, andsinonasalundifferentiatedcarcinoma:differentiation in diagnosis small round blue cell tumors in the sinonasal tract. Am J Surg Pathol.
and treatment. Int Arch Otorhinolaryngol. 2014;18(02, Suppl 2):S149– 2011;35(12):1786–1793
S156 29 Argani P, Perez-Ordoñez B, Xiao H, Caruana SM, Huvos AG, Ladanyi M.
4 Bell D, Saade R, Roberts D, Ow TJ, Kupferman M, DeMonte F, et al. Olfactory neuroblastoma is not related to the Ewing family of tumors:
Prognostic utility of Hyams histological grading and Kadish- Morita stag- absence of EWS/FLI1 gene fusion and MIC2 expression. Am J Surg Pathol.
ing systems for esthesioneuroblastoma outcomes. Head Neck Pathol. 1998;22(04):391–398
2015;9(01):51–59 30 Hyams V, Batsakis J, Michaels L. Tumors of the upper respiratory tract and
5 Ow TJ, Bell D, Kupferman ME, Demonte F, Hanna EY. Esthesioneuroblas- ear. Armed forces institute of pathology fascicles, 2nd series. Washington:
toma. Neurosurg Clin N Am. 2013;24(01):51–65 American Registry of Pathology Press; 1988
6 Faragalla H, Weinreb I. Olfactory neuroblastoma: a review and update. 31 Wenig BM. Undifferentiated malignant neoplasms of the sinonasal tract.
Adv Anat Pathol. 2009;16(05):322–331 Arch Pathol Lab Med. 2009;133(05):699–712
7 Holbrook EH, Wu E, Curry WT, Lin DT, Schwob JE. Immunohisto- 32 Purdy Stout A, Lattes R. Atlas of tumor pathology. Washington: Armed
chemical characterization of human olfactory tissue. Laryngoscope. Forced Institute of Pathology; 1967
2011;121(08):1687–1701 33 Bradley PJ, Jones NS, Robertson I. Diagnosis and management of esthesio-
8 Trojanowski JQ, Lee V, Pillsbury N, Lee S. Neuronal origin of human es- neuroblastoma. Curr Opin Otolaryngol Head Neck Surg. 2003;11(02):112–
thesioneuroblastoma demonstrated with anti-neurofilament monoclonal 118
antibodies. N Engl J Med. 1982;307(03):159–161 34 Kaur G, Kane AJ, Sughrue ME, Madden M, Oh MC, Sun MZ, et al. The
9 Carney ME, O’Reilly RC, Sholevar B, Buiakova OI, Lowry LD, Keane WM, et prognostic implications of Hyam’s subtype for patients with Kadish stage
al. Expression of the human Achaete-scute 1 gene in olfactory neuroblas- C esthesioneuroblastoma. J Clin Neurosci. 2013;20 (02):281–286
toma (esthesioneuroblastoma). Neurooncol. 1995;26(01):35–43 35 Dublin AB. Imaging characteristics of olfactory neuroblastoma. J Neurol
10 Mills SE. Neuroectodermal neoplasms of the head and neck with emphasis Surg B Skull Base. 2007;17(S1):A091
on neuroendocrine carcinomas. Mod Pathol. 2002;15 (03):264–278 36 Lund VJ, Milroy C. Olfactory neuroblastoma: clinical and pathological as-
11 Barnes L, EvesonJW, Reichart P, SidranskyD. Pathology andgenetics of pects. Rhinology. 1993;31(01):1–6
head and neck tumours. World Health Organization (WHO) Classification 37 Bailey BJ, Barton S. Olfactory neuroblastoma. Management and progno-
of Tumours. Lyon: IARC Press; 2005:168–175 sis. Arch Otolaryngol. 1975;101(01):1–5
12 Jethanamest D, Morris LG, Sikora AG, Kutler DI. Esthesioneuroblastoma: a 38 BakM,Wein RO. Esthesioneuroblastoma: a contemporary review of diagno-
population-based analysis of survival and prognostic factors. Arch Otolar- sis and management. Hematol Oncol Clin North Am. 2012;26(06):1185–
yngol Head Neck Surg. 2007; 133(03):276–280 1207
13 Platek ME, MerzianuM,Mashtare TL, Popat SR, Rigual NR,Warren GW, et 39 Ow TJ, Hanna EY, Roberts DB, et al. Optimization of long-term outcomes
al. Improved survival following surgery and radiation therapy for olfactory for patients with esthesioneuroblastoma. Head Neck. 2014;36(04):524–
neuroblastoma: analysis of the SEER database. Radiat Oncol. 2011;6:41 530
14 Chao KS, Kaplan C, Simpson JR, Haughey B, Spector GJ, Sessions DG, et 40 Holland H, Koschny R, Krupp W, et al. Comprehensive cytogenetic char-
al. Esthesioneuroblastoma: the impact of treatment modality. Head Neck. acterization of an esthesioneuroblastoma. Cancer Genet Cytogenet.
2001;23(09):749–757 2007;173(02):89–96
15 Spaulding CA, Kranyak MS, Constable WC, Stewart FM. Esthesioneuro- 41 Bockmühl U, You X, Pacyna-Gengelbach M, Arps H, Draf W, Petersen
blastoma: a comparison of two treatment eras. Int J Radiat Oncol Biol I. CGH pattern of esthesioneuroblastoma and their metastases. Brain
Phys. 1988;15(03):581–590 Pathol. 2004;14(02):158–163
16 Dias FL, Sa GM, Lima RA, Kligerman J, LeoncioMP, Freitas EQ, et al. Pat- 42 Guled M, Myllykangas S, Frierson HF Jr, Mills SE, Knuutila S, Stelow EB.
terns of failure and outcome in esthesioneuroblastoma. Arch Otolaryngol Array comparative genomic hybridization analysis of olfactory neuroblas-
Head Neck Surg. 2003;129(11):1186–1192 toma. Mod Pathol. 2008;21(06):770–778
30 Rev. Argent. Radiol. 2020;84(1): 17-31R. Navas-Campo et al.
43 Modesto A, Blanchard P, Tao YG, Rives M, Janot F, Serrano E, et al. Multi- 1993;32(05):706–714, discussion 714–715
modal treatment and long-term outcome of patients with esthesioneuro- 61 Biller HF, LawsonW, Sachdev VP, Som P. Esthesioneuroblastoma: surgical
blastoma. Oral Oncol. 2013;49(08):830–834 treatment without radiation. Laryngoscope. 1990;100 (11):1199–1201
44 Suriano M, De Vincentiis M, Colli A, Benfari G, Mascelli A, Gallo A. En- 62 Konuthula N, Iloreta AM, Miles B, Rhome R, Ozbek U, Genden EM, et al.
doscopic treatment of esthesioneuroblastoma: a minimally invasive ap- Prognostic significance of Kadish staging in esthesioneuroblastoma: An
proach combined with radiation therapy. Otolaryngol Head Neck Surg. analysis of the National Cancer Database. Head Neck. 2017;39(10):1962–
2007;136(01):104–107 1968
45 Ward PD, Heth JA, Thompson BG, Marentette LJ. Esthesioneuroblasto- 63 Gallia GL, Reh DD, Salmasi V, Blitz AM, KochW, Ishii M. Endonasal endo-
ma: results and outcomes of a single institution’s experience. Skull Base. scopic resection of esthesioneuroblastoma: the Johns Hopkins Hospital
2009;19(02):133–140 experience and review of the literature. Neurosurg Rev. 2011;34(04):465–
46 Josephs L, Jones L, Marenette L, McKeever P. Cushing’s syndrome: 475
an unusual presentation of olfactory neuroblastoma. Skull Base. 64 Hanna E, DeMonte F, Ibrahim S, Roberts D, Levine N, Kupferman M. Endo-
2008;18(01):73–76 scopic resection of sinonasal cancers with and without craniotomy: onco-
47 Koo BK, An JH, Jeon KH, Choi SH, Cho YM, Jang HC, et al. Two cases of logic results. Arch Otolaryngol Head Neck Surg. 2009;135(12):1219–1224
ectopic adrenocorticotropic hormone syndrome with olfactory neuroblas- 65 Diaz EM Jr, Johnigan RH 3rd, Pero C, El-Naggar AK, Roberts DB, Barker JL,
toma and literature review. Endocr J. 2008;55(03): 469–475 et al. Olfactory neuroblastoma: the 22-year experience at one comprehen-
48 Plasencia YL, Cortés MB, Arencibia DM, Dámaso TM, Contreras IL, sive cancer center. Head Neck. 2005;27(02): 138–149
Pino AO, et al. Esthesioneuroblastoma recurrence presenting as a syn- 66 Su SY, Kupferman ME, DeMonte F, Levine NB, Raza SM, Hanna EY. Endo-
drome of inappropriate antidiuretic hormone secretion. Head Neck. scopic resection of sinonasal cancers. Curr Oncol Rep. 2014; 16(02):369
2006;28(12):1142–1146 67 Kane AJ, Sughrue ME, Rutkowski MJ, Aranda D, Mills SA, Buencamino R,
49 Dulguerov P, Allal AS, Calcaterra TC. Esthesioneuroblastoma: a meta-anal- et al. Posttreatment prognosis of patients with esthesioneuroblastoma. J
ysis and review. Lancet Oncol. 2001;2(11):683–690 Neurosurg. 2010;113(02):340–351
50 Manelfe C, Bonafé A, Fabre P, Pessey JJ. Computed tomography in olfac- 68 Schwartz JS, Palmer JN, Adappa ND. Contemporary management
tory neuroblastoma: one case of esthesioneuroepithelioma and four cases of esthesioneuroblastoma. Curr Opin Otolaryngol Head Neck Surg.
of esthesioneuroblastoma. J Comput Assist Tomogr. 1978;2(04):412–420 2016;24(01):63–69
51 Ahmed M, Knott PD. Hyperostotic esthesioneuroblastoma: rare variant 69 Folbe A, Herzallah I, Duvvuri U, Bublik M, Sargi Z, Snyderman CH, et al.
and fibrous dysplasia mimicker. Korean J Radiol. 2014;15 (01):156–160 Endoscopic endonasal resection of esthesioneuroblastoma: a multicenter
52 HowellMC, Branstetter BF IV, Snyderman CH. Patterns of regional spread study. Am J Rhinol Allergy. 2009;23(01): 91–94
for esthesioneuroblastoma. AJNR Am J Neuroradiol. 2011; 32(05):929– 70 Loy AH, Reibel JF, Read PW, Thomas CY, Newman SA, Jane JA, et al. Es-
933 thesioneuroblastoma: continued follow-up of a single institution’s experi-
53 Ahmad A, Branstetter BF IV. CT versus MR: still a tough decision. Otolar- ence. Arch Otolaryngol Head Neck Surg. 2006;132(02):134–138
yngol Clin North Am. 2008;41(01):1–22, v 7 Saade RE, Hanna EY, Bell D. Prognosis and biology in esthesioneuro-
54 Ling FTK, Kountakis SE. Advances in imaging of the paranasal sinuses. blastoma: the emerging role of Hyams grading system. Curr Oncol Rep.
Curr Allergy Asthma Rep. 2006;6(06):502–507 2015;17(01):423
55 Branstetter BF IV,Weissman JL. Role ofMRand CT in the paranasal sinuses. 72 Bhattacharyya N, Thornton AF, Joseph MP, Goodman ML, Amrein PC.
Otolaryngol Clin North Am. 2005;38(06):1279–1299, x Successful treatment of esthesioneuroblastoma and neuroendocrine car-
56 Som PM, Lidov M, Brandwein M, Catalano P, Biller HF. Sinonasal esthe- cinoma with combined chemotherapy and proton radiation. Results in 9
sioneuroblastoma with intracranial extension: marginal tumor cysts as a cases. Arch Otolaryngol Head Neck Surg. 1997;123(01):34–40
diagnostic MR finding. AJNR Am J Neuroradiol. 1994;15(07):1259–1262 73 Loy AH, Reibel JF, Read PW, Thomas CY, Newman SA, Jane JA, et al. Es-
57 Sievers KW, Greess H, Baum U, Dobritz M, Lenz M. Paranasal sinuses and thesioneuroblastoma: continued follow-up of a single institution’s experi-
nasopharynx CT and MRI. Eur J Radiol. 2000;33(03): 185–202 ence. Arch Otolaryngol Head Neck Surg. 2006;132(02):134–138
58 Koka VN, JulieronM, Bourhis J, Janot F, Le Ridant AM, Marandas P, et al. 74 Saade RE, Hanna EY, Bell D. Prognosis and biology in esthesioneuro-
Aesthesioneuroblastoma. J Laryngol Otol. 1998;112(07): 628–633 blastoma: the emerging role of Hyams grading system. Curr Oncol Rep.
59 Slevin NJ, Irwin CJ, Banerjee SS, Gupta NK, Farrington WT. Olfactory 2015;(17):1–5
neural tumours–the role of external beam radiotherapy. J Laryngol Otol. 75 Bhattacharyya N, Thornton AF, Joseph MP, Goodman ML, Amrein PC.
1996;110(11):1012–1016 Successful treatment of esthesioneuroblastoma and neuroendocrine car-
60 Morita A, Ebersold MJ, Olsen KD, Foote RL, Lewis JE, Quast LM. Es- cinoma with combined chemotherapy and proton radiation: results in 9
thesioneuroblastoma: prognosis and management. Neurosurgery. cases. Arch Otolaryngol Head Neck Surg. 1997;123(01):34–40
Rev. Argent. Radiol. 2020;84(1): 17-31 31You can also read