Novità e sequenze terapeutiche nel carcinoma mammario HER2 positivo Terapia neoadiuvante - Claudio Zamagni - AIOM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Novità e sequenze
terapeutiche nel carcinoma
mammario HER2 positivo
Terapia neoadiuvante
Claudio Zamagni
Direttore SSD Oncologia Medica Addarii
Policlinico S.Orsola-Malpighi
Bologna
Claudio Zamagni Pisa 30 settembre 2017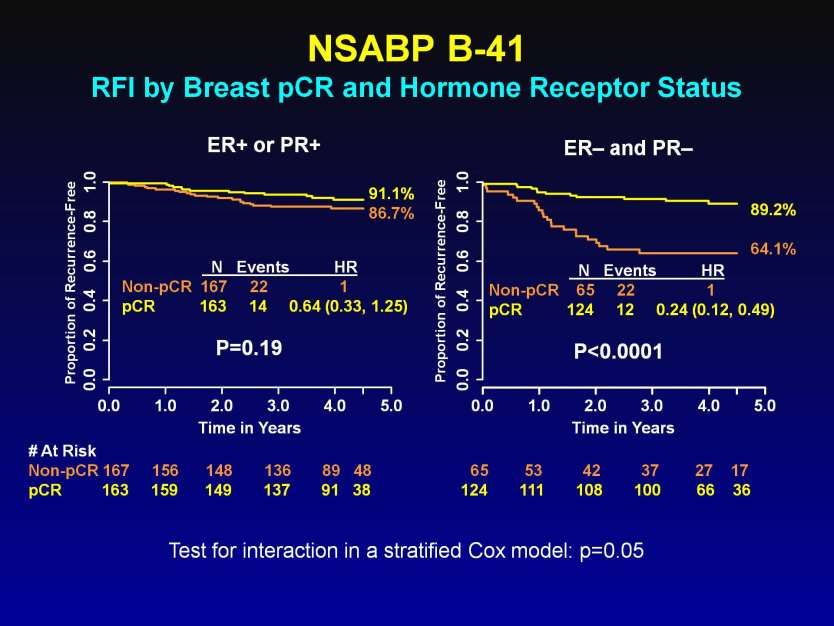
Open questions in HER2+ eBC Anthra/taxane vs taxane alone Dual blockade vs single Long vs short pCR vs no pCR ER+ vs ER- Claudio Zamagni Pisa 30 settembre 2017
Open questions in HER2+ eBC
pCR as a surrogate endpoint
Claudio Zamagni Pisa 30 settembre 2017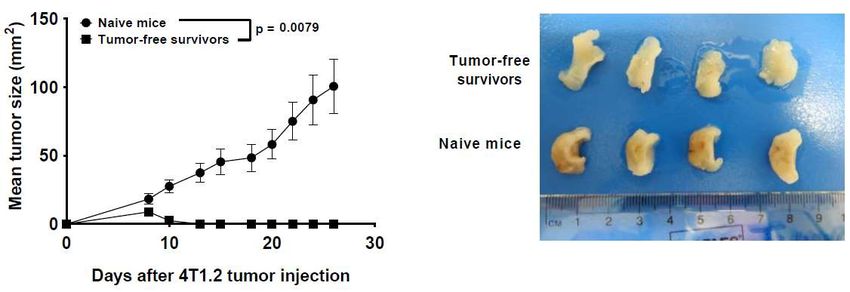
Cortazar P et al, Lancet 2014 Claudio Zamagni Pisa 30 settembre 2017
NSABP B-41 RFI by Breast pCR and Hormone Receptor Status
Presented By Andre Robidoux at 2016 ASCO Annual Meeting
Claudio Zamagni Pisa 30 settembre 2017
Claudio Zamagni Pisa 30 settembre 2017 Cortazar P et al, Lancet 2014
Open questions in HER2+ eBC
De-escalating treatment
Claudio Zamagni Pisa 30 settembre 2017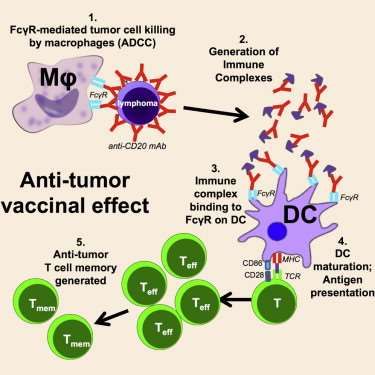
APT Trial
Disease-Free Survival
3-year DFS 98.7% (95% CI 97.6-99.8)
3-y failure rate 1.3% (95% CI 0.2-2.4)
Sequential Poisson test p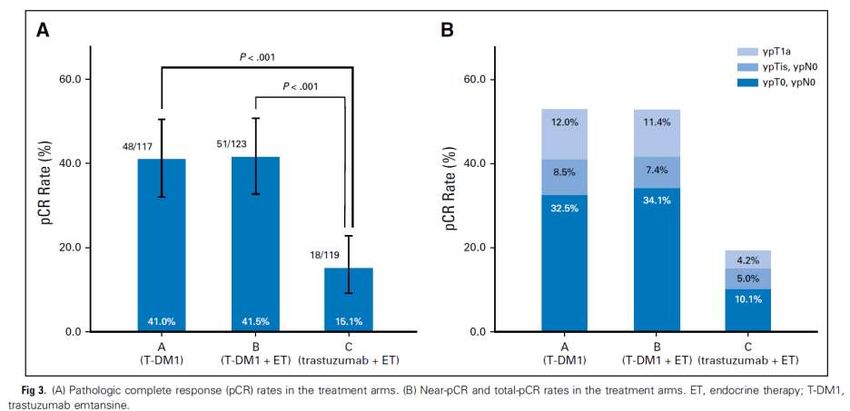
ADAPT HER2+/HR+
Neoadjuvant Phase 2 Trial
*Standard chemo recommended after surgery
Trastuzumab to be completed, for total of one year
Claudio Zamagni Pisa 30 settembre 2017 Harbeck N et al J Clin Oncol 2017
pCR superior in TDM1 arms Claudio Zamagni Pisa 30 settembre 2017 Harbeck N et al J Clin Oncol 2017
Neoadjuvant chemo-free regimens in HER2+ BC
pCR rate (breast and axilla)
* Breast HER2+/ER-
pCR HER2+/ER+
60 T-DM1+P
T-DM1+HT
50
T-DM1
40 T + L + HT T+P+HT
*
30 T+P
20
10 HT+T *
0 12 wks 24 wks
NeoSphere1 Kristine2 ADAPT3 TBCRC 0064 TBCRC 0235 PerELISA6
1. Gianni L, et al. Lancet Oncol 2012; 2. Hurvitz s, et al. ASCO 2016; 3. Harbeck N, et al. ASCO 2015; 4. Rimawi M, et al. J Clin
Oncol 3013; 5. Rimawi M, et al. SABCS 2014; 6. Guarneri V, personal communication
Claudio Zamagni Pisa 30 settembre 2017Open questions in HER2+ eBC
The unmet need for
HER2+ eBC
is treatment tailoring
Claudio Zamagni Pisa 30 settembre 2017HER2 Tumour Heterogeneity
NeoSphere
TH (n=107)
docetaxel (75100 mg/m2)
trastuzumab (86 mg/kg) S
THP (n=107)
U
docetaxel (75100 mg/m2) R
trastuzumab (86 mg/kg)
pertuzumab (840420 mg) G
HP (n=107) E
trastuzumab (86 mg/kg)
pertuzumab (840420 mg) R
TP (n=96) Y
docetaxel (75100 mg/m2)
pertuzumab (840420 mg)
Study dosing: q3w x 4
Gianni L, et al. Lancet Oncol 2012; 13:25–32
Claudio Zamagni Pisa 30 settembre 2017HER2 Tumour Heterogeneity
NeoSphere: Study 50
pCR, % 95% CI
design and main results 40
46
30
TH (n=107)
20
29
docetaxel (75100 mg/m2) 24
trastuzumab (86 mg/kg) S 10
17
THP (n=107)
U 0
TH THP HP TP
docetaxel (75100 mg/m2) R
trastuzumab (86 mg/kg)
pertuzumab (840420 mg) G
HP (n=107) E
trastuzumab (86 mg/kg)
pertuzumab (840420 mg) R
TP (n=96) Y
docetaxel (75100 mg/m2)
pertuzumab (840420 mg)
Study dosing: q3w x 4
Gianni L, et al. Lancet Oncol 2012; 13:25–32
Claudio Zamagni Pisa 30 settembre 2017HER2 Tumour Heterogeneity
NeoSphere: Study 50
pCR, % 95% CI
design and main results 40
As in all other neoadjuvant trials,
46
probability of pCR is significantly
30
20
higher for hormone receptor-
TH (n=107) 29
docetaxel (75100 mg/m2) negative tumours 24
trastuzumab (86 mg/kg) S 10
17
THP (n=107)
U 0
TH THP HP TP
docetaxel (75100 mg/m2) R
trastuzumab (86 mg/kg) 70
pertuzumab (840420 mg) ER- or PR-positive
G 60 ER- and PR-negative
pCR, % 95% CI
HP (n=107) E 50
trastuzumab (86 mg/kg) 63
pertuzumab (840420 mg) R 40
TP (n=96) Y 30
docetaxel (75100 mg/m2) 20 37
pertuzumab (840420 mg)
29 30
Study dosing: q3w x 4 10 26
20 6 17
Gianni L, et al. Lancet Oncol 2012; 13:25–32
0
TH THP HP TP
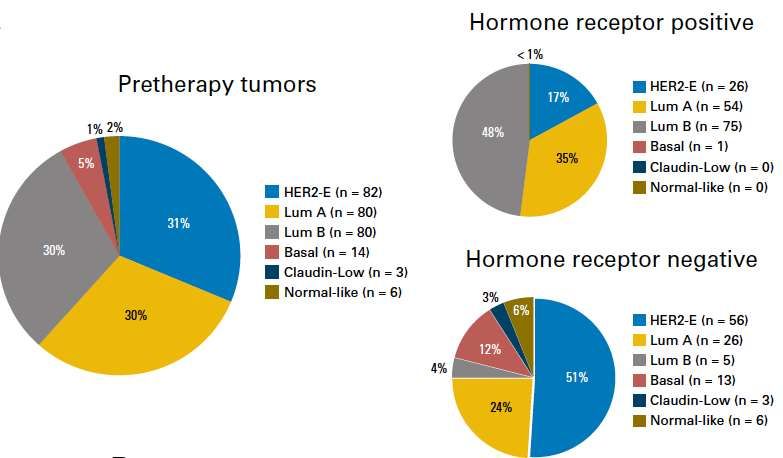
Claudio Zamagni Pisa 30 settembre 2017HER2+ eBC is a heterogeneous disease
Intrinsic subtypes in CALGB 40601
Hormone receptor-positive
Pre-therapy tumours
Hormone receptor-negative
Carey LA, et al., J Clin Oncol 2016; 34:542–549.
Claudio Zamagni Pisa 30 settembre 2017HER2+ eBC is a heterogeneous disease:
Subtypes have different pCR rates with neoadjuvant therapy
Carey LA, et al., J Clin Oncol 2016; 34:542–549.
Claudio Zamagni Pisa 30 settembre 2017Intrinsic sub-types in CALGB 40601 are
different after neoadjuvant therapy
Pre-Treatment Residual Disease
Claudin low Normal-like
Basal like
HER2-E
HER2 Normal Like
enriched
Luminal B
Claudin low
Luminal A Basal-like Lum A
Lum B
Carey LA, et al., J Clin Oncol 2016; 34:542–549.
Claudio Zamagni Pisa 30 settembre 2017Less than 20% concordance between intrinsic
sub-types of primary biopsy and residual disease
Post-treatment
pre-treat HER2-E Lum A Lum B Basal-like Claudin low Normal-like
HER2-E 3 20 0 0 1 0
Lum A 6 1 12 0 0 0
Lum B 0 0 3 0 0 0
Basal-like 0 0 0 3 0 0
Claudin low 0 0 2 0 1 0
Normal-like 3 7 9 1 1 2
NA 13 22 25 5 0 1
Carey LA, et al., J Clin Oncol 2016; 34:542–549.
Claudio Zamagni Pisa 30 settembre 2017Intrinsic sub-types in residual disease after
neoadjuvant therapy – the CALGB 40601 data
Post-treatment
pre-treat HER2-E Lum A Lum B Basal-like Claudin low Normal-like
HER2-E 3 20 0 0 1 0
Lum A 6 Most residual
1 tumours 0
12 0 0
Lum B are0made up0 of luminal
3 0
subtypes 0 0
Basal-like 0 0 0 3 0 0
Claudin low 0 0 2 0 1 0
Normal-like 3 7 9 1 1 2
NA 13 22 25 5 0 1
Carey LA, et al., J Clin Oncol 2016; 34:542–549.
Claudio Zamagni Pisa 30 settembre 2017Residual disease after neoadjuvant therapy
= micrometastasis
Micrometastasis Primary tumour
Residual bulk
disease
Surgery
Drug(s)
Recurrence
Courtesy of Carlos Arteaga, 2013
Claudio Zamagni Pisa 30 settembre 2017A different way to test treatment
according to pCR vs not
control
S
pCR R
U
standard adjuvant HER2-therapy
HER2-directed R
neoadjuvant G
as in the
main design E experimental treatment
R
RD
Y standard adjuvant HER2-therapy
Claudio Zamagni Pisa 30 settembre 2017Slide 19 Claudio Zamagni Pisa 30 settembre 2017
Open questions in HER2+ eBC
New therapies
Claudio Zamagni Pisa 30 settembre 2017Murine models show CDK4/6 implicated in
anti-HER2 therapy resistance
• Following anti-HER2 therapy,
survival of resistant HER2+ model
tumours was dependent on
expression of cyclin D1
• CDK4/6 inhibitors resensitised
tumours to HER2-targeted agents
• Anti-HER2 therapy + CDK4/6
inhibition reduced tumour
proliferation more than either
therapy alone
Goel S, et al. Cancer Cell. 2016; 29;255–269
Claudio Zamagni Pisa 30 settembre 2017Convergence of multiple signals on Rb
checkpoint in breast cancer
• Convergence at cyclin D to drive BC cell proliferation1
– Nuclear hormone, PI3K/AKT/mTOR, MAPK, Wnt/β-catenin, JAK-
STAT, and NF-κB pathways1,2
• Mitogenic signals via ER and HER2 require Cyclin D1
– Cyclin D1 direct ER-target gene required for estrogen-dependent cell
proliferation4,5
– Cyclin D1-deficient mice are resistant to HER2-induced BCs6
– ER+/HER2+ cell lines are most sensitive to CDK4/6 inhibition7
• Cyclin D–CDK4/6–INK4–Rb pathway also disrupted in breast cancer
through:
– CCND1 (cyclin D1) amplification – 35%3
– CDK4 amplification – 16%3
– CDK6 amplification – 17%3
– Loss of p16 – 49%8
– Inactivating alterations of TP53 (p21 activator) – 84% of basal and
27% of non-basal tumours3
• Cyclin D–CDK4/6–INK4–Rb pathway activation is associated with
poor response of BC cells to endocrine therapy9
1. Lange CA, et al. Endocrine-related Cancer 2011;18:C18–C24; 2. Witzel II, et al. Biochem Soc Trans 2010;38:217–222; 3. TCGA, Nature 2012;490:61–70;
4. Lukas J, et al. Mol Cell Biol 1996;16:6917–6925; 5. Prall OW, et al. J Steroid Biochem Mol Biol 1998;65:169-74; 6. Yu Q, et al. Nature 2001;411:1017–1021;
7. Finn RS, et al. Breast Cancer Res 2009;11:R77; 8. Geradts J, Wilson PA. Am J Pathol 1996:149:15–20; 9. Thangavel C, et al. Endocr Relat Cancer 2011;18:333–345.
Claudio Zamagni Pisa 30 settembre 2017MonarcHER: Phase Ib study of abemaciclib in
combination with therapies for patients with mBC
Objectives: Key eligibility criteria:
•The primary objective was to evaluate safety and tolerability of abemaciclib • HR+/HER2- mBC (Parts A-E) or HER2+ (both
in combination with endocrine therapies for HR+ HER2- mBC or HR+ and HR-) mBC (Part F)
trastuzumab for HER2+ mBC
• Post-menopausal status (natural, surgical, or
•The secondary objectives were to assess pharmacokinetics and anti- medical; Parts A-E) or any menopausal status
tumour activity (Part F)
Part A: abemaciclib + letrozole • Parts A-E: no prior systemic chemotherapy for
metastatic disease Part F: ≥1 chemotherapy
Part B: abemaciclib + anastrozole
regimen for metastatic disease
HR+/HER2- mBC Part C: abemaciclib + tamoxifen • Patients receiving exemestane-based therapy
must have received ≥1 nonsteroidal aromatase
Part D: abemaciclib + exemestane
inhibitor for metastatic disease
Part E: abemaciclib + exemestane + everolimus
HER2+ mBC Part F: abemaciclib + trastuzumab
HR, hormone receptor; mBC, metastatic breast cancer
Claudio Zamagni Pisa 30 settembre 2017
Beeram M, et al. ESMO 2016; abstract LBA18MonarcHER: anti-tumour activity
Change in tumour size for patients with measurable disease
Abemaciclib combinations
show clinical activity in HR+
mBC, including HR+/HER2+
HER2+ mBC tumours
Beeram M, et al. ESMO 2016; abstract LBA18
Claudio Zamagni Pisa 30 settembre 2017NA-PHER2: Phase II trial of neo-adjuvant
treatment with palbociclib in HR+/HER2+
eBC
Primary endpoints
• Ki67 changes
frombaseline before
Patients with
therapy, at 2 weeks,
early and locally HPPF x 6 4-weekly cycles and at surgery
advanced HER2+ Herceptin + pertuzumab + • Change in apoptosis
and ER+ (>10%) palbociclib + fulvestrant from baseline before
BC; chemo-naïve
H = Trastuzumab, 8 mg/kg on first dose, 6 mg/kg thereafter x 6;
therapy and at
P = Pertuzumab, 840 mg on first dose, 420 mg thereafter x 6;
Palbociclib 125 mg orally QD. x 21 q. 4 wks. x 5
surgery
Fulvestrant will be given intra-muscle at the dose of 500 mg every 4 weeks
*HER-2, ER, PR and x 5 with an additional 500 mg dose given two weeks after the initial dose
Ki67 centrally confirmed
The total duration of neoadjuvant palbociclib (5 cycles every 4 weeks) and
Secondary
fulvestrant (5 administrations every 4 weeks plus the additional dose given
two weeks after the initial dose) was selected to match as closely as
endpoints
possible the total duration of the six planned 3-weekly administrations of
trastuzumab and pertuzumab
• pCR
• ORR
• Tolerability
Palbociclib is not approved for use in HER2+ disease in Europe
ORR, objective response rate; pCR, pathological complete response defined as
absence of invasive cells in breast and axilla (ypT0-ypTis ypN0) at surgery
Gianni L, et al. SABCS 2016; Poster P4-21-39
Claudio Zamagni Pisa 30 settembre 2017NA-PHER2: Ki67 levels decreased following
treatment
80
-5
Reduction of % Ki67+ cells
Ki67 change 70
60
Baseline Week 2 Surgery
% Ki67+ cells
-15
(n=27) (n=25) (n=22) 50
Geometric 40
31.9 (15.7) 4.3 (15.0) 12.1 (20.0) -25
mean (SD) 30
Mean change –24.0 –10.9 20
–
95% CI (–31.0; –7.1) (–19.3; –2.6) -35
10
Paired T-test –7.11 –2.72 0
–
P-value < 0.0001 0.013 -45
Gianni L, et al. SABCS 2016; Poster P4-21-39
Claudio Zamagni Pisa 30 settembre 2017NA-PHER2: Pathological and clinical
response rate
ITT population (n=30) n (%)
pCR (no invasive cells in breast and axilla) 8 (27%)
pCR in breast only 9 (30%)
Overall clinical response 29 (97%)
• Complete clinical response 15 (50%)
• Partial response 14 (47%)
• Stable disease 3 (3%)
Gianni L, et al. SABCS 2016; Poster P4-21-39
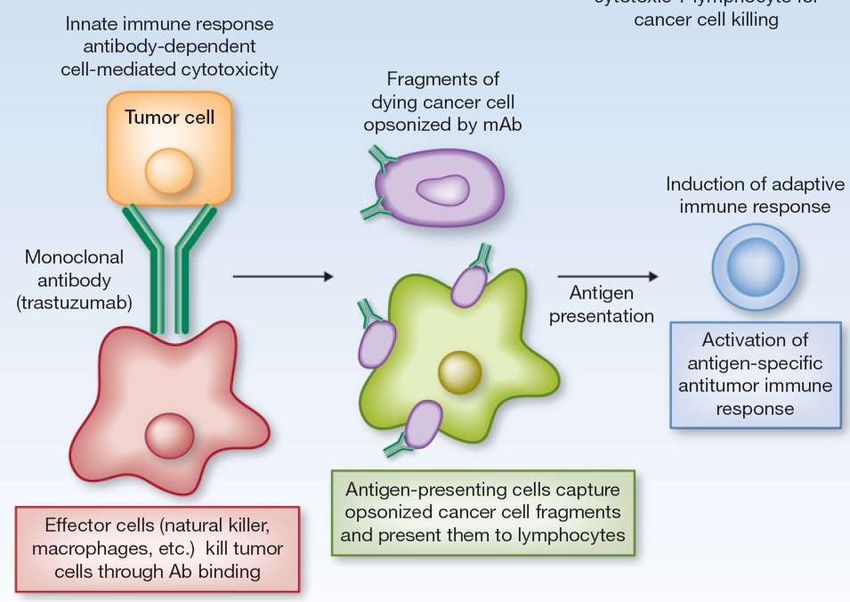
Claudio Zamagni Pisa 30 settembre 2017HER2+ BC is immunogenic Claudio Zamagni Pisa 30 settembre 2017
FcγR–mediated Antigen Presentation and CTL Response
FcɣR
Andre F et al. Clinical Cancer Res 2012Differential Fc-receptor engagement drives
an anti-tumour vaccinal effect
David JD & Jeffrey RV. Cell 2015; 161:1035–1045.
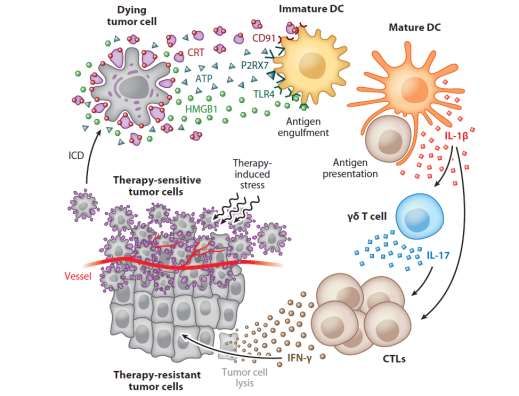
Claudio Zamagni Pisa 30 settembre 2017Must the tumour be present for an
optimal “vaccine-like” effect?
Kroemer G. Annu Rev Immunol 2013
Claudio Zamagni Pisa 30 settembre 2017Randomized Phase II Biomarker Study of Immune-mediated Mechanism of
Action of Neoadjuvant Trastuzumab (either iv or sc) in Patients with HER2-
positive Breast Cancer (ImmunHER)
Eligibility (n = 63) Trastuzumab IV (8 mg/kg loading dose,
Women with followed by 6 mg/kg) plus
histologically confirmed Pertuzumab IV (840 mg loading dose,
HER2-positive breast followed by 420 mg) plus
cancer with locally Docetaxel IV (75→100 mg/m2),
advanced, inflammatory, every 3 weeks for 4 cycles
or early stage tumor
(either greater than 2 R Trastuzumab SC
cm in diameter or node (fixed dose of 600 mg) plus
positive) with no Pertuzumab IV (840 mg loading dose,
evidence of metastatic followed by 420 mg) plus
disease Docetaxel IV (75→100 mg/m2),
Pre-randomization phase: every 3 weeks for 4 cycles
FEC (5FU 500; epirubicin
75; Primary Objective:
CTX 500) x 3 cycles To evaluate variations of host immune response
Primary endpoint:
parameters to either trastuzumab SC or trastuzumab
TIL rate on residual disease after either IV
IV given in combination with pertuzumab and
trastuzumab or SC trastuzumab
ClinicalTrials.gov Identifier: NCT03144947
Claudio Zamagni Pisa 30 settembre 2017
chemotherapy.st cancer.Interaction of pCR with treatment
for EFS in HER2+ groups
• Trastuzumab vs. no Trastuzumab
Stratum Sample size EFS HR (95% CI) p
pCR 45 vs. 23 0.29 (0.11 – 0.78) 0.0135
non pCR 72 vs. 95 0.92 (0.61 – 1.39) NS
quality of pCR different with ADCC competent
• pCR vs. non pCRmonoclonal antibodies
Stratum Sample size EFS HR (95% CI) p
Trastuzumab 45 vs. 72 0.17 (0.08 – 0.38)Neoadjuvant is more effective than adjuvant
therapy with anti-PD-1+anti-CD137
NeoAdj -PD-1/ -CD137 NeoAdj -PD-1/ -CD137
4T1.2 orthotopic or control IgG E0771 orthotopic or control IgG
injection Surgery injection Surgery
Day: 0 17 19 21 23 Day: 0 16 18 20 22
Surgery Surgery
Adj -PD-1/ -CD137 Adj -PD-1/ -CD137
or control IgG or control IgG
100 100
Percent survival
Percent survival
50 50
0 0
0 50 100 150 0 50 100 150 200
Days after 4T1.2 tumour injection Days after E0771 tumour injection
NeoAdj control IgG NeoAdj -PD-1/ -CD137 pNeoadjuvant anti-PD-1+anti-CD137 leads to
systemic expansion of tumor-specific CD8+ T cells
Blood Liver
200 250 p = 0.0012
# gp70 Tetramer CD8
# gp70 Tetramer CD8
200
T cells/ml (x102)
150
T cells (x102)
150
100 pTumour-free survivors after neoadjuvant
immunotherapy have immunological memory
150 Naive mice
p = 0.0079
Mean tumour size (mm2)
Tumour-free survivors Tumour-free
survivors
100
Naive mice
50
0
0 10 20 30
Days after 4T1.2 tumour injection
Neoadjuvant modality is superior to adjuvant delivery of immunotherapy
in model systems and may be the optimal approach to achieve
“vaccine-like” effects and permanent tumour eradication
Liu J Cancer Discovery 2016
Claudio Zamagni Pisa 30 settembre 2017Rationale exists for atezolizumab combinations
in HER2+ BC
• There is evidence of anti-tumour immune response in HER2+ BC
Immune biomarkers at
TILs are associated with Immune effects of HER2
baseline have similarities to
better outcomes for HER2 therapies are observed
TNBC
regimens Neoadjuvant H/K increases PD-L1
Immune (Teff) signature
pCR and DFS (EBC), and CD8+ TILS that are associated
PD-L1 expression
OS (CLEO MBC) with higher pCR (ADAPT HR+)
TILs and CD8 prevalence
• Preclinical synergistic activity is observed for checkpoint inhibitors combined
with anti-HER2 therapies
Internal preclinical data
• K(A) consistent with
published data
• A with (T)HP pending
* αPD-1
** αPD-L1
APTneo phase III trial
Courtesy L. Gianni
Claudio Zamagni Pisa 30 settembre 2017Terapia neoadiuvante tumori HER2+
Take Home message
pCR predittiva di prognosi (fino al 73% di pCR in ER- HER2+)
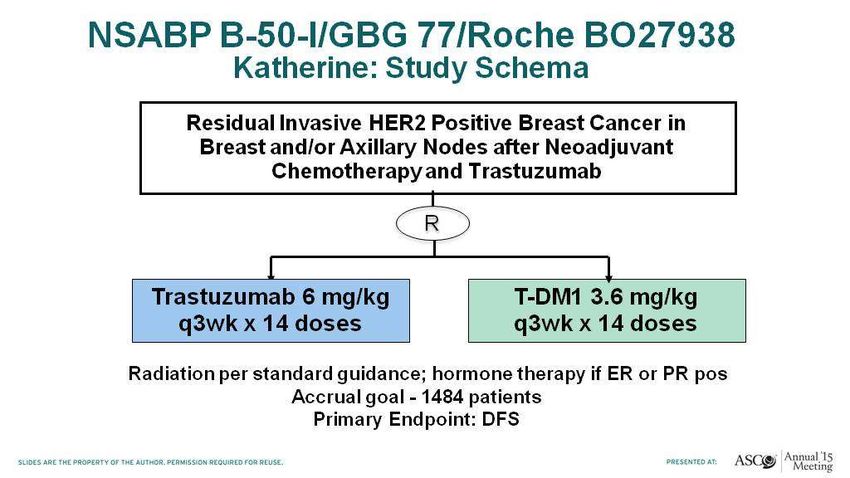
Neoadiuvante fondamentale per selezionare pazienti
a prognosi peggiore (no pCR) per nuovi studi (i.e.
studio Katherine)
Trattamento di scelta nei T2-3 e/o N+, ma proponibile
anche in stadio 1
Lo standard*: CHT + trastuzumab + pertuzumab
*non modificato dai dati dello studio Aphinity
In attesa di CDK4-6i e anti PD1 – PDL1i
Claudio Zamagni Pisa 30 settembre 2017You can also read

















































