Novel Coronavirus from China: Nuisance Cold Virus or the next - SARS? Thomas M. Kerkering, MD, FACP, FIDSA Professor of Medicine Section of ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Novel Coronavirus from China:
Nuisance Cold Virus or the next
SARS?
Thomas M. Kerkering, MD, FACP, FIDSA
Professor of Medicine
Section of Infectious Diseases
Virginia Tech Carilion School of Medicine
Professor, Public Health Program Virginia Tech
⚫ On December 31, 2019, the World
Health Organization(WHO) was alerted
to several cases of pneumonia in Wuhan
City, Hubei Province of China, and the
virus detected did not match any other
known virus.
⚫ On January 7th, Chinese authorities
confirmed that they had identified a new
virus, a coronavirus, and in the family of
viruses that include the common cold,
SARS, MERS, and is named “2019-
nCoV” (Now: COVID-19)
⚫ On January 14, the sequence of COVID-
19 was published online, and we read of
14 healthcare workers infected in China
⚫ How does it relate to other Coronaviruses ⚫ What is it’s infectivity? ⚫ What is the incubation period? ⚫ What are the clinical signs & symptoms ⚫ What is the source of the COVID-19? ⚫ What is the mortality rate? ⚫ What measures can we take to prevent it? ⚫ Will it result in a pandemic? ⚫ Will we have a vaccine?
CORONAVIRUSES
◼ Isolated in 1960 from a child with a common cold
among an outbreak in which Rhinovirus was not
isolated*
◼ 2 human strains known (prior to SARS) 229E and
OC43
◼ Etiology of “winter colds” and uncommon cause of
self-limited Pneumonia
◼ Nosocomial outbreaks among newborns and
elderly
*Kendall, EJC, et al. Br Med J. 1962:82-86


Pneumonia with Coronavirus
OC43 in Adult Recruits
Respiratory signs and symptoms
# with results (%)
Cough 11/11 100%
Sore throat 8/11 72%
Fever > 102oF 6 54%
Sputum 6 54%
Rales 5 45%
Pneumonia (x-ray) 4 36%
Wenzel, RP, et.al. Rev Resp Dis 1974;109:621
Signs and Symptoms Coronaviruses usually cause “common cold” symptoms like: • runny or stuffy nose, • sneezing, • sore throat, • headache, • cough, • mild fever, • body aches. Infection can sometimes lead to an ear infection or trigger an asthma flare-up in a person with asthma. More serious lung problems such as pneumonia are less common and happen most often in the elderly and in people with weakened immune systems.

How It's Spread Scientists don’t know much about how coronaviruses (other than SARS) are spread. Most likely, they are spread person to person through coughs, sneezes, laughs – anything that produces a spray that can be inhaled by someone else. Close personal contact (e.g., a handshake or a kiss) is another likely way to spread coronavirus infection.
Classification Coronaviruses have a crown or halo-like appearance of the envelope glycoproteins. Most human coronaviruses fall into one of two serotypes: OC43-like and 229E-like. Multiplication It is thought that human coronaviruses enter cells, predominantly, by specific receptors. Aminopeptidase-N and a sialic acid- containing receptor have been identified to act in such a role for 229E and OC43 respectively. After entering the host cell, the uncoated genome is transcribed and translated. The mRNAs form a unique “nested set” sharing a common 3′ end. New virions form by budding from host cell membranes. Pathogenesis Transmission is usually via airborne droplets to the nasal mucosa. Virus replicates locally in cells of the ciliated epithelium, causing cell damage and inflammation. Coronaviruses are extremely fastidious and grow only in differentiated respiratory epithelial cells. Infected cells become vacuolated, show damaged cilia, and may form syncytia. Cell damage triggers the production of inflammatory mediators, which increase nasal secretion and cause local inflammation and swelling. These responses in turn stimulate sneezing, obstruct the airway, and raise the temperature of the mucosa.
Host Defenses Although mucociliary activity is designed to clear the airways of particulate material, coronaviruses can successfully infect the superficial cells of the ciliated epithelium. Only about one-third to one-half of infected individuals develop symptoms, however. Interferon can protect against infection, but its importance is not known. Because coronavirus infections are common, many individuals have specific antibodies in their nasal secretions, and these antibodies can protect against infection. Most of these antibodies are directed against the surface projections and neutralize the infectivity of the virus. Cell-mediated immunity and allergy have been little studied, but may play a role. Epidemiology The epidemiology of coronavirus colds has been little studied. Waves of infection pass through communities during the winter months, and often cause small outbreaks in families, schools, etc.. Immunity does not persist, and subjects may be re-infected, sometimes within a year. The pattern thus differs from that of rhinovirus infections, which peak in the fall and spring and generally elicit long-lasting immunity. About one in five colds is due to coronaviruses. The rate of transmission of coronavirus infections has not been studied in detail. The virus is usually transmitted via inhalation of contaminated droplets, but it may also be transmitted by the hands to the mucosa of the nose or eyes.
Electron micrograph showing
human coronavirus 229E
Coronavirus virion structure shown with structural proteins.
N: Nucleocapsid protein; S: Spike protein, M: Membrane
protein, HE: Hemagglutinin-Esterase and E: Envelope proteinInfluenza A Receptors
The receptor specificities of human, equine, swine
and avian influenza A viruses differ, suggesting
that the distribution of species specific receptors in
animals and birds and the ability of HA to bind to
these receptors might be a determinant of the
host range and tissue tropism of influenza A viruses.
A single mutation in an amino acid sequence in the HA
nucleotide could result in the virus being able to “jump”
species.Influenza viruses that are common in
various animals
H1N1, H3N2 Swine
H1N1, H2N2, H3N2 Humans
H7N7, N3N8 Horses
H7N7, H4N5 Seals
H10N4 Mink
H5 & H7 Ducks
From Pringle, IDN, Eickhoff, ed
* Avian receptor is a 2,3 sialic acid receptor.
* Human receptor is a 2,6 sialic acid receptor.Incidental hosts Incidental hosts
Fecal spreaders
Large numbers Virus mixers
Assist in spread With both human
To humans And bird virus receptors
◼ Swine receptors are both
Incidental hosts 2, 3 and 2, 6 receptorsThen, in 2003, a new respiratory pathogen
PATIENT CASE
A male patient was admitted February
22, 2003 to a Hong Kong hospital in
respiratory distress.
He had symptoms of a respiratory
tract infection since February 15 in
Guangdong Province, China. He died
the following day.PATIENT CASE
Differential Diagnosis
◼ Influenza A, B
◼ “Avian Flu”
◼ Adenovirus
◼ Hantavirus
◼ Parainfluenza
◼ ARDSSearch for Pathogen
◼ Lung Pathology Syncytial Giant Cells
◼ Lack of isolation of
Influenza A or B,
Parainfluenza,
Adenovirus
◼ Virus isolation on
Vero 6 cells with
classic “rounding up”
Kaye M, Druce J, Tran T, et al. EID. 2006; 12 (1): 128-133.Electron Microscopy
Search for Pathogen
◼ EM Coronavirus morphology from
Canadian and Hanoii cases
◼ IFA Seroconversions with paired sera
No non-ill controls with antibody
◼ Viral Sequences – Coronavirus-like
Agent–distinct from known
human isolates OC43 and
229EClinical Features of the Canadian
Patients with SARS at Presentation
Variable
Investigations # with results (%)
◼ Infiltrate on chest ◼ 9 / 9 (100)
radiography
◼ Oxygen saturation on ◼ 7 / 9 (78)
room air < 95%
◼ Leukopenia (cell count ◼ 2 / 9 (22)Coronavirus - SARS
◼ Incubation period from exposure to fever
2-16 da (Mean 6 da)
◼ Biphasic Disease
◼ Radiographic picture consistent with
atypical pneumonia
◼ Virus shed in sputum and feces
◼ Case Fatality Rate: 4 – 7% initially; up to
15% among elderly
https://www.cdc.gov/sars/about/faq.htmlSARS: 10 Yrs Later
⚫ During 2003, 8096 people in 29 countries got
SARS, and 774 died
⚫ Only 8 people in the US had SARS, and none
of them died
⚫ In six months, the global SARS outbreak cost
the world an estimated $40 billion
⚫ The last known case was in 2004
https://www.cdc.gov/dotw/sars/Nine Years Later, 2012, another respiratory disease appeared Most people confirmed to have MERS-CoV infection have had severe respiratory illness with symptoms of: • fever • cough • shortness of breath • ~diarrhea and nausea/vomiting. In many patients with MERS, more severe complications followed, such as pneumonia and kidney failure. Mortality of 30-40%
Pre-existing conditions among people who got MERS have included: • diabetes • cancer • chronic lung disease • chronic heart disease • chronic kidney disease Some infected people had mild symptoms (such as cold-like symptoms) or no symptoms at all. The symptoms of MERS start to appear about 5 or 6 days after a person is exposed, but can range from 2 to 14 days.
Wait another 7 years and a third respiratory
disease appears on the scene COVID-19
• First case date of onset:
Dec. 1, 2019
• First international notice
Dec. 31, 2019
• ~ 12,000 cases as of
Feb. 1, 2020
• Associated with wet market
• Physician who raises concern
is censored; later dies from
the disease.Clinical Features of Initial 41
Patients infected with COVID-19
⚫ Dyspnea and low systolic
⚫ 41 patients admitted in pressures were the only clinical
Wuhan: 27/41 (66%) features with statistical
exposed to Huanan significance:
seafood market ⚫ 12/13 (92%)-vs- 10/27 (37%) in
non-ICU (p = 0.002)
⚫ Study compared ICU-vs- ⚫ Lower systolic pressure in ICU
non-ICU cases for cases (p = 0.018)
differences by X2 test, ⚫ Most severe cases had
lymphopenia, low Procalcitonin,
Fisher’s Exact Test, or and all cases had bilateral
Mann-Whitney U test involvement on Chest X-rays
Huang C, et al. The Lancet. Jan 24, 2020 ⚫ ARDS in 12/41; Anemia in 6/41;
6/41 (15%) died, and 5/13 ICU
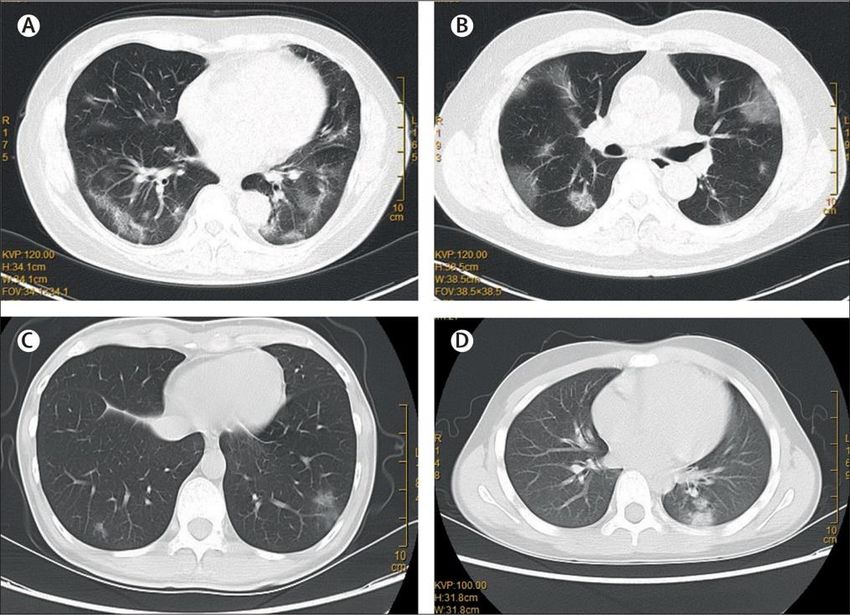
(32%) died.Figure 3
Chest Radiographs and CT Scans
of Initial Cases of COVID-19
⚫ Zhu N, et al. NEJM.2020 Chan J F-W, et al. The Lancet Jan 24, 2020
The Lancet DOI: (10.1016/S0140-6736(20)30183-5)COVID-19 in Cell Culture and EM
2019-n-CoV CPE EM in Lung Tissue
Zhu N, et al. NEJM.2020Comparison of Recent Severe
Coronavirus Infections
Coronavirus Attack Rate Case-Fatality Comment
(% exposed who Rate
become infected)
SARS 50% 10% Higher in those
over 65 yrs, co-
morbidities
MERS 8% 20-25%
2019-nCoV ?? ~ 2%* Higher in those
over 65 yrs of
age, co-
morbidities
* As of 1-28-2020Basic Reproduction number: R0
⚫ R0, or R nought, of an
infection is the number
of cases that one case
generates on average
over time in an
uninfected population.
Zhao S, et al. bioRxiv
2020:01.23.916395COVID-19 Sequenced
Zhou P, Yang X-L, Wang S-G, et al. bioRxiv. 20202019-n-CoV Genetics and Possible
Source(s)
Dr. Ji and colleagues
sequenced the 2019-nCoV
and noticed some overlaps
with both bat and snake
coronaviruses; thus, as
snakes hunt bats, they
theorize that the spike
glycoprotein may have
recombined in the bat, and
now can infect humans
Ji W, Wang W, Shao X, et al. J Med Virology. 22 Jan 2020Is the Pangolin the source?
How deadly is the virus? It’s hard to know yet. But the fatality rate is probably less than 3 percent, much less than SARS.
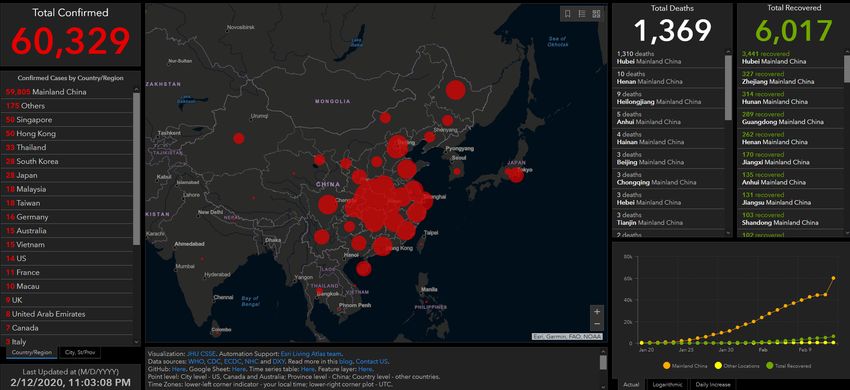
How much have infected people traveled? The virus spread quickly because it started in a transportation hub.
Mortality Rate = 2.27% Wuhan population = 8,364,977;
Attack Rate = ??? (remember, over 50,000,000 people live density = 3,108/sq. mile
in the immediate area) Roanoke City population = 96,714
density = 2,300/sq. mile
Roanoke County population = 93,730
density = 144/sq. mileDaily New Cases Primarily Mainland China
16000
15100
14000
12000
10000
8000
6000
4000
4000 3700 3500
3100 2900 3200 3000
2500 2700 2500
2000 2000
2000 1700 1600 1700 1500
1084
700
322 221 277 400
4 92
014 cases in USA as of Feb. 12,2020. All connected with Wuhan.
Watch what you drink!!
You can also read