COVID-19 Community Sector Forum - dhhs.vic.gov.au/coronavirus - VCOSS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

COVID-19 Community Sector Forum dhhs.vic.gov.au/coronavirus

EMMA KING CEO, Victorian Council of Social Service @EmmaKingVic dhhs.vic.gov.au/coronavirus

Acknowledgement of Country dhhs.vic.gov.au/coronavirus

LUKE DONNELLAN Minister for Child Protection, Disability, Ageing & Carers @LukeDonnellan dhhs.vic.gov.au/coronavirus

ARGIRI ALISANDRATOS Deputy Secretary, DHHS dhhs.vic.gov.au/coronavirus

Implications for Community Service Organisations of COVID-19 Argiri Alisandratos Deputy Secretary Children, Families, Communities and Disability Division Department of Health and Human Services

COVID-19 – What we currently know Highest risk groups • Older Victorians and people with chronic diseases • Early information suggests milder illness in children, particularly those nine years and under. Current focus of health response: • Early identification, contact tracing and isolation to slow community spread Preparation priorities: • Ensuring business continuity plans are current and well understood • Communicating COVID-19 plans and arrangements with staff • Promoting good hygiene, including hand hygiene and respiratory/cough etiquette

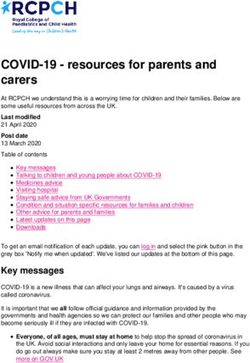
Business continuity planning
BUSINESS
RECOVERY PLAN TESTING &
IMPACT
STRATEGIES DEVELOPMENT EXERCISES
ANALYSIS
During this Identify and Develop the Create a test plan and
phase, document all framework for the subsequent exercises
you will assess resource continuity plan, that can be performed
the factors that requirements based establish and by the business to
could on the BIAs organize the ensure that the
potentially harm completed in the recovery teams, and business continuity plan
your business previous step. develop a plan of (BCP) works
and you will Determine a relocation in the case successfully. Update
create a plausible recovery of disruption or the BCP as needed
business impact strategy based on disaster. Create a based on the tests and
analysis (BIA). the needs of the thorough business exercises.
Review the BIA business and the continuity plan and IT
with senior BIA, and document disaster recovery
management and implement that plan, and document
and key strategy. both in a flexible,
stakeholders to circulating
ensure visibility. document. Gain
upper management
approval upon
completion.Promoting good understanding amongst staff Reference documents • The COVID-19 Pandemic Plan for the Victorian Health Sector • Guidelines for health services and General Practitioners Promoting good hygiene tips • Ten ways to reduce your risk poster • Handwashing, cough and sneezing poster Testing and self-isolation • Self assessment for risk of coronavirus flowchart • National fact sheet on home isolation and care • Travel restrictions Safe workplaces • Worksafe guidance on exposure to coronavirus in the workplace Stay up to date at https://www.dhhs.vic.gov.au/coronavirus
Residential and other facility-based services Development of protocols for • Infection prevention and outbreak identification and management – training and support for staff • Ongoing client care following cases and visitor access • Escalation of care to other settings (hospital etc) • Surge workforce to manage staff reductions and absenteeism (20-30%) • Facility management and cleaning • Finalising arrangements for seasonal flu vaccinations for residents, staff and volunteers • Any health care needs that can be managed now
Support for vulnerable people, including in the community
Identify vulnerable groups and individuals
• for example, isolated older people, people with disability/complex health
needs, families where schools and workplaces are closed
Consider the setting
• Facility based care vs at home in the community
Ways to reach out to vulnerable people, subject to risk level
• Visits, use of technology, social media, regular phone contacts
Forms of support
• Contact to engage/check on welfare, food relief, assistance to access
Commonwealth payments, psychological first aid, care for children and others
Activating community support
• Local social infrastructure (like neighbourhood houses), utilise existing social
connection networks, wider family networksSocial service sector leads
Key contacts for sectors
Children and Families – Beth Allen – Director, Children and Families Policy Branch
Disability – James MacIsaac – Director, Disability
Housing and Homelessness – Sherri Brunihout – Director, Housing Pathways and Outcomes
SRS and other regulated service – Anthony Kolmus – A/Director, Human Services Regulator
Aged Care services and carers– Jackie Kearney – Director, Seniors Aging and Carers
Volunteering and local community services – Phil O’Meara – Director, Disabilities and Community
Branch
HACC – Louise Galloway – Director, Performance and Improvement, Aged and Community Based
Health Care and Cancer Services
Koorie – Paulleen Markwort – Director Aboriginal Strategy and Oversight Branch
Family Violence – Kelly Stanton – Executive Director, Family Safety VictoriaDR BRETT SUTTON Victorian Chief Health Officer @VictorianCHO dhhs.vic.gov.au/coronavirus
COVID-19 in Context The local experience of global threats 12 March 2019 Dr. Annaliese van Diemen Deputy Chief Health Officer, Communicable Disease
Overall current infection rate (11 March)
Internationally:
• 117,000+ confirmed cases
• 4,200 deaths
Of confirmed cases reported globally, the case fatality rate is
approximately 3.6%.
The case fatality rate in countries and regions outside mainland China is
approximately 3.1%.
Australia:
• 112 cases of COVID-19 have been confirmed in Australia (includes 3
deaths)
• 19 confirmed cases in Victoria.
• 4379 people have tested negative in VictoriaCollaboration and communication between countries
Johns Hopkins interactive real-time report
https://www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6Travel history – all people tested Australia (10 March)
• China – 490 (21%) • Italy – 85 (4%)
• Indonesia – 356 (15%) • Malaysia – 68 (3%)
• Japan – 321 (14%) • South Korea – 63 (3%)
• Thailand – 242 (10%) • Philippines – 42 (2%)
• Singapore – 240 (10%) • Cambodia – 28 (1%)
• Hong Kong – 92 (4%) • Iran – 23 (1%)
Denominator is all people tested where travel history is knownHow does COVID-19 compare to other epidemics?
R0
Source: New York TimesEpidemiological characteristics of historic outbreaks
1918 Flu SARS MERS COVID-19
R0 1.4 – 2.8 2.2 2.5% 11% ~45% 2.2 – 4.3%
Incubation 2-7 days 2-7 days 2-14 days 2-14
period
Number of 15 million 774 858 ?
deathsLessons learned from SARS • International travel allows for rapid spread between continents – Restricting movement of citizens (China) – Border restrictions – Quarantine of returned travellers • Importance of nosocomial spread and hospital infection control – Large number of healthcare worker infections, particularly in critical care situations – Aerosol generating procedures
Modelling potential scenarios
Current Victorian response Departmental Incident Management Team formed
Clinical presentation of confirmed cases (10 March)
Infection ranges from asymptomatic or mild through to severe illness and death
Common symptoms: Common clinical signs include the following:
• Fever – 11 (58%) • Pneumonia
• Cough – 12 (68%) • Lymphocytopenia
• Sore throat – 5 (26%) • Prolonged prothrombin time
• Pneumonia – 2 (11%) • CT scans displaying lesions in multiple
• Diarrhoea – 4 (21%) lung lobes and/or ground-glass opacity.Definition COVID 19 – SUSPECTED CASE
A. If the patient satisfies both clinical and epidemiological criteria, they are
classified as a suspected case:
• Clinical criteria: Fever OR Acute respiratory infection (for example,
shortness of breath or cough) with or without fever
AND
• Epidemiological criteria: International travel in the 14 days before the
onset of illness OR Close or casual contact in the 14 days before illness
onset with a confirmed case of COVID-19.
B. If the patient has severe community-acquired pneumonia (critically ill) and
no other cause is identified, with or without recent international travel, they
are classified as a suspect case.
C. If the patient has moderate or severe community-acquired pneumonia
(hospitalised) and is a healthcare worker, with or without international travel,
they are classified as a suspect case.Definition COVID 19 - CONFIRMED CASE A person who tests positive to a validated SARS-CoV-2 nucleic acid test or has the virus identified by electron microscopy or viral culture. Notification Requirements • Proposal that notification to DHHS of suspected cases is not required • Confirmed cases remain notifiable within 24 hours • Further information regarding notification requirements will be provided as they are developed. Decrease the burden on health services, GPs and the department Phone 1300651160, 24 hours a day
Pandemic plan for the Victorian Health Sector
Objectives :
• Reduce the morbidity and mortality
COVID-19 associated with COVID-19.
Pandemic plan for the Victorian • Slow the spread of COVID-19 in Victoria
Health Sector
Version 1.0
through rapid identification, isolation and
10th March 2020 cohorting of risk groups.
• Empower the Victorian community, health
Jenny Mikakos MP
Minister for Health
professionals and the community to ensure a
proportionate and equitable response.
Minister for Ambulance Services
• Support containment strategies through
accurate, timely and coordinated
communication and community support.
• Mitigate and minimise impacts of the
pandemic on the health system and broader
community.
https://www2.health.vic.gov.au/about/publications/ResearchA
ndReports/covid-19-pandemic-plan-for-vicPandemic plan - Victorian response
COVID-19 Hospital Preparedness Assessment /Scenario Testing Tools
• These documents have been developed to support
Victorian hospitals (metropolitan, rural and private) plan
their response to COVID-19
• They should be based on (and read in conjunction with)
business continuity plans and pandemic plans
https://www.dhhs.vic.gov.au/health-services-and-general-practitioners-coronavirus-
disease-covid-19Chief Health Officer alerts
• The CHO will issue a daily Follow the Chief Health Officer
email update from 11 March on Twitter:
twitter.com/VictorianCHO
which will replace Alerts
pertaining to COVID-19.
• A CHO Alert will only be
issued if there is a significant
critical clinical requirement.
• To receive Chief Health Officer
alerts, subscribe
at: https://www2.health.vic.gov
.au/newslettersAdvice for clinicians
• Keep up to date with new
information on the DHHS
website
• Quick reference guide and
checklist
• Guidelines for health services
and general practitioners
• Current case definition
• Chief health officer alerts https://www.dhhs.vic.gov.au/health-services-and-
general-practitioners-coronavirus-disease-covid-19
• Hand hygiene
• Don’t go to work if you’re sickResources DHHS COVID-19 page https://www.dhhs.vic.gov.au/coronavirus - Guideline for Health services - Quick reference guide/Checklist - PPE guidance - Posters - Factsheets for cases and contacts
Unit and organisation level planning Think ahead about • Essential vs non-essential activities • Rostering • When would you activate surge, and what would this mean • How will you manage an outbreak in your unit/organisation? • How will COVID affect your patient population? • How your patient population might change • Where are current or potential blockage points for patient flow? • How to articulate with other health services? How might this change?
JESSE MADDISON Director, Industrial Relations, DHHS dhhs.vic.gov.au/coronavirus
ARGIRI ALISANDRATOS Deputy Secretary, DHHS dhhs.vic.gov.au/coronavirus
dhhs.vic.gov.au/coronavirus vcoss.org.au
You can also read