Nouvelles stratégies médicales dans la prise en charge des IOA en 2022 - Aurélien Dinh
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Nouvelles stratégies médicales dans la
prise en charge des IOA en 2022
Aurélien Dinh
Service des Maladies Infectieuses
Hôpital Raymond-Poincaré, APHP
Université Paris Saclay
23es JNI, Bordeaux du 15 au 17/06/2022
Liens d’intérêt • Ménarini • Shionogi • Pfizer • MSD 23es JNI, Bordeaux du 15 au 17/06/2022
Antibiothérapie probabiliste 23es JNI, Bordeaux du 15 au 17/06/2022
Outcome
Outcome and Predictors of Treatment Failure in and Predictors of Treatment Failure in
Total Hip/Knee Prosthetic Joint InfectionsTotal
Due toHip/Knee Prosthetic Joint Infections Due to
Staphylococcus aureus Staphylococcus aureus
Eric Senneville, Donatienne Joulie, Laurence Legout, Michel Valette, Hervé Dezèque, Eric Beltrand, Bernadette Roselé,
Thibaud d'Escrivan, Caroline Lo!ez, Michèle Caillaux, Yazdan Yazdanpanah, Carlos Maynou, and Henri EricMigaud
Senneville, Donatienne Joulie, Laurence Legout, Michel Valette, Hervé Dezèque, Eric Beltrand, Bernadette Roselé,
Centre National de Référence des Infections Ostéo-Articulaires Nord-Ouest, Roger Salengro Faculty Hospital of Lille, Lille, Thibaud
France d'Escrivan, Caroline Lo!ez, Michèle Caillaux, Yazdan Yazdanpanah, Carlos Maynou, and Henri Migaud
Centre National
Background. Variables associated with the outcome of patients treated for prosthetic joint infections de Référence des Infections Ostéo-Articulaires Nord-Ouest, Roger Salengro Faculty Hospital of Lille, Lille, France
(PJIs) due
to Staphylococcus aureus are not well known.
Background.
Methods. The medical records of patients treated surgically for total hip or knee prosthesis infection due to S. Variables associated with the outcome of patients treated for prosthetic joint infections (PJIs) due
to Staphylococcus
aureus were reviewed. Remission was defined by the absence of local or systemic signs of implant-related infection aureus are not well known.
assessed during the most recent contact with the patient. Methods. The medical records of patients treated surgically for total hip or knee prosthesis infection due to S.
¡ Etude rétrospective 98 patients
Results. After a mean posttreatment follow-up period of 43.6 6 32.1 months, 77 (78.6%) of 98 patients were in
aureus were reviewed. Remission was defined by the absence of local or systemic signs of implant-related infection
remission. Retention of the infected implants was not associated with a worse outcome than was their removal.
Methicillin-resistant S. aureus (MRSA)–related PJIs were not associated with worse outcome, assessed during
compared with the most recent contact with the patient.
¡ Infection prothèse genou et Results.
methicillin-susceptible S. aureus (MSSA)–related PJIs. Pathogens identified during revision for failure no a mean posttreatment follow-up period of 43.6 6 32.1 months, 77 (78.6%) of 98 patients were in
exhibited After
hanche à Staph aureus remission. Retention of the infected implants was not associated with a worse outcome than was their removal.
acquired resistance to antibiotics used as definitive therapy, in particular rifampin. In univariate analysis,
parameters that differed between patients whose treatment did or did not fail were: American Society of
Methicillin-resistant S. aureus (MRSA)–related PJIs were not associated with worse outcome, compared with
Anesthesiologists (ASA) score, prescription of adequate empirical postsurgical antibiotic therapy, and use of
¡ Suivi moyen 4 ans
[OR], 6.87 [95% confidence interval {CI}, 1.45–32.45]; P 5 .04) and rifampin-fluoroquinolone
methicillin-susceptible S. aureus (MSSA)–related PJIs. Pathogens identified during revision for failure exhibited no
rifampin combination therapy upon discharge from hospital. In multivariate analysis, ASA score #2 (odds ratio
acquired resistance to antibiotics used as definitive therapy, in particular rifampin. In univariate analysis,
combination
¡ FDR d’échec (univarié): ATB
therapy (OR, 0.40 [95% CI, 0.17–0.97]; P 5 .01) were 2 independent variables associated with parameters
Conclusions. The results of the present study suggest that the ASA score significantly affects
remission. that differed between patients whose treatment did or did not fail were: American Society of
the outcome of (ASA) score, prescription of adequate empirical postsurgical antibiotic therapy, and use of
Anesthesiologists
post opératoire non adaptée
patients treated for total hip and knee prosthetic infections due to MSSA or MRSA and that rifampin combination
rifampin combination therapy upon discharge from hospital. In multivariate analysis, ASA score #2 (odds ratio
therapy is associated with a better outcome for these patients when compared with other antibiotic regimens.
[OR], 6.87 [95% confidence interval {CI}, 1.45–32.45]; P 5 .04) and rifampin-fluoroquinolone combination
therapy (OR, 0.40 [95% CI, 0.17–0.97]; P 5 .01) were 2 independent variables associated with remission.
Conclusions. The results of the present study suggest that the ASA score significantly affects the outcome of
Prosthetic joint infections (PJIs) represent a growing morbidity, increased medical costs, and reduced quality
public health concern in developed countries as a result
patients treated for total hip and knee prosthetic infections due to MSSA or MRSA and that rifampin combination
of life [3, 4]. General principles of management of PJI
of the increasing number of operations therapy is associated with a better outcome for these patients when compared with other antibiotic regimens.
23es JNI, Bordeaux du 15forautotal joint
17/06/2022 include a multidisciplinary approach at centers with
arthroplasty and a risk of postoperative infection of 1%– expertise in this field. Reliable microbiological diagnosis,
Antibiothérapie post-opératoire immédiate
• Si pas de documentation pré opératoire
• Cibler : Staph doré, strepto, entérocoque,
entérobactérie.
• Tenir compte écologie du service
23es JNI, Bordeaux du 15 au 17/06/2022
HAS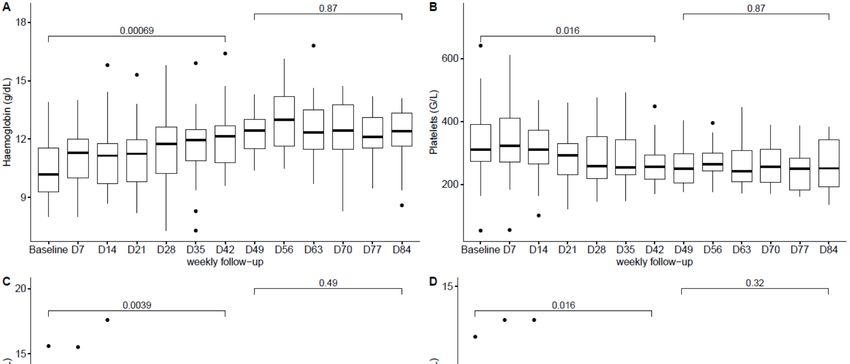
Cohorte PIANO : ATB empirique individualisée • n=783 (27 centres) 23es JNI, Bordeaux du 15 au 17/06/2022 Davis J. et al. Int J Med Int 2022
Durées de traitement 23es JNI, Bordeaux du 15 au 17/06/2022

group). The most frequently used antibiotics were oral Table 1. (Continued.)
Articles
Durées de traitement
fluoroquinolones or rifampicin or a combination of both * Plus–minus values are means ±SD. Stratification variables at randomization included history of prosthetic joint infec-
tion, baseline surgical procedure, and affected joint. IQR denotes interquartile range.
in 253 (72%) patients, followed by oral aminopenicillin † Data on age were available for 203 patients in the 6-week group and 201 patients in the 12-week group.
‡ History of prosthetic joint infection was defined as having had at least one previous episode.
(98 [28%] patients; table 4). Parenteral meticillin § Body-mass index (BMI) is the weight in kilograms divided by the square of the height in meters. Obesity was defined by a
(133 [38%] patients) and aminoglycosides (213 [61%]) BMI greater than 30. Data on BMI were available for 192 patients in the 6-week group and 186 patients in the 12-week group.
¶ An American Society of Anesthesiologists (ASA) score of 1 denotes a normal healthy patient, 2 a patient with mild
were used during the initial intravenous phase of systemic disease, 3 a patient with severe systemic disease, 4 a patient with severe systemic disease that is a constant
Antibiotic
treatment. treatmentof for
The distribution 6 weeks
antibiotics did notversus differ12 weeks in patients
threat to life, 5 a patient in a moribund state, and 6 a patient declared brain-dead.
∥ Data on the time between symptom onset and surgical procedure were available for 198 patients in the 6-week group
with pyogenic
between the two groups vertebral
for any ofosteomyelitis:
the microorganisms an open-label,
and 188 patients in the 12-week group. Among the patients who underwent débridement with implant retention, the
median time between the onset of symptoms and surgical procedure was 5 days (IQR, 3 to 10) among 82 patients in
assessed (appendix). Median duration of intravenous the 6-week group and 5 days (IQR, 3 to 11) among 83 patients in the 12-week group.
non-inferiority,
administration was much randomised,
the same incontrolled both groupstrial
** Data on C-reactive protein (CRP) level were available for 164 patients in the 6-week group and 147 patients in the 12-
week group.
†† Multidrug resistance was defined as an isolate that is not susceptible to at least one agent in at least three antimicro-
(15Louisdays
Bernard, [IQR 7–28]
Aurélien Dinh, in David
Idir Ghout, theSimo,
6-week
Valerie Zeller,group vs 14
Bertrand Issartel, days
Vincent Le Moing, Nadia Belmatoug, Philippe Lesprit, bial classes.
[IQR 6·5–26·5]
Jean-Pierre inDamien
Bru, Audrey Therby, theBouhour,
12-week
Eric Dénes,group).
Alexa Debard,Overall, theKarine Fèvre, Michel Dupon, Philippe Aegerter,
Catherine Chirouze, ‡‡ A total of 68 patients had a polymicrobial infection (37 in the 6-week group and 31 in the 12-week group), so patients
may have had more than one pathogen identified at baseline. A total of 237 pathogens were identified in the 6-week
Denis Mulleman, on behalf of the Duration of Treatment for Spondylodiscitis (DTS) study group*
median duration of intravenous administration was group, and 233 pathogens were identified in the 12-week group.
§§ Other pathogens included anaerobic bacteria, enterococcus, and other gram-positive bacteria.
Summary ¶¶ Data on duration of intravenous route of antibiotic treatment were available for 192 patients in the 6-week group and
Background Duration of treatment for patients with vertebral osteomyelitis is mainly based on expert recommendation 194 385:
Lancet 2015; patients
875–82in the 12-week group.
rather than evidence. We aimed 6-week regimen
to establish 12-week
whether 6 weeksregimen Difftreatment
of antibiotic 95% CI to 12 weeks in
erence in is non-inferior ∥∥ Patients
Published Online may have received more than one oral antibiotic agent.
patients with pyogenic vertebral osteomyelitis. proportion of November 5, 2014
patients* http://dx.doi.org/10.1016/
S0140-6736(14)61233-2
Methods In this open-label, non-inferiority, randomised controlled trial, we enrolled patients aged 18 years or older
Intention-to-treat
with microbiologicallyanalysis, n 176
confirmed 175
pyogenic vertebral osteomyelitis and typical radiological features from 71 medical care
See Comment
Table 2.page 836
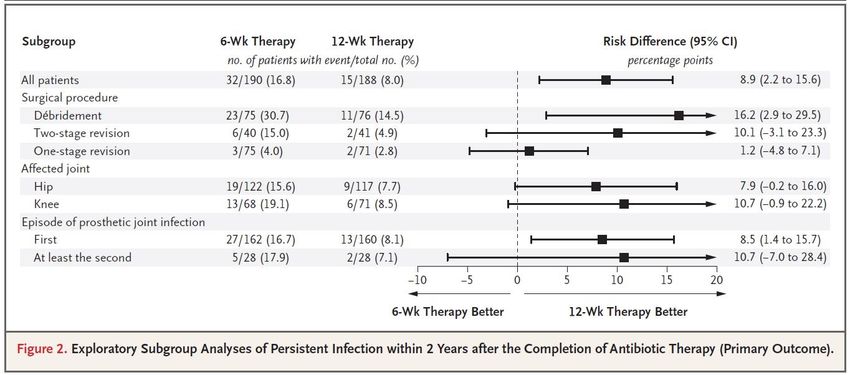
Difference in Risk of Persistent Infection within 2 Years after the Completion of Antibiotic Therapy (Primary Outcome) in the Modified
Intention-to-Treat
*Members listed in appendix and Per-Protocol Analyses.
Cured across France. Patients 160
centres were(90·9%) 159 (90·9%)
randomly assigned +0·1 or 12 weeks–6·2
to either 6 weeks to 6·3
of antibiotic treatment
Division of Infectious Diseases,
(physician’s choice in accordance with French guidelines) by a computer-generated randomisation list of permuted Adjusted Risk
Cured and alive† 156 (88·6%) 150 (85·7%) +2·9 –4·2 to 10·1 University Hospital
blocks, stratified by centre. The primary endpoint was the proportion of patients who were classified as cured at 1 year Analysis
Bretonneau, Tours, France, 6-Wk Therapy 12-Wk Therapy Risk Difference Difference*
Cured
by without
a masked further validation
independent 142committee,
(80·7%) analysed
141 (80·6%) +0·1 Non-inferiority–8·3
by intention to treat. to 8·5
would be declared if the (L Bernard MD); Division of
no. of patients with event/total no. (%) Percentage points (95% CI)
antibiotic treatment‡
proportion of cured patients assigned to 6 weeks of treatment was not less than the proportion of cured patients Infectious Diseases, University
Modified
Hospital Raymond intention-to-treat
Poincaré,
assigned to 12 weeks of treatment, within statistical variability, by an absolute margin of 10%. This trial is registered
Per-protocol analysis, n 146 137 Garches, France (A Dinh MD);
Main analysis in which missing outcomes for patients who 35/193 (18.1) 18/191 (9.4) 8.7 (1.8–15.6) 9.0 (2.3–15.7)
with EudraCT, number 2006-000951-18, and Clinical Trials.gov, number NCT00764114. Clinical Research Unit,
Cured 137 (93·8%) 132 (96·4%) –2·5 –8·2 to 2·9 wereAmbroise
University Hospital lost to follow-up were considered to be per-
Findings Between Nov 15, 2006, and March 15, 2011, 359 patients were randomly assigned, of whom six in the 6-week Paré, Boulogne,sistent
France infections and data from patients who died
Cured and alive† 133 (91·1%) 126 (92·0%) –0·9 –7·7 to 6·0 (I Ghout MSc, Dremoved†
Simo CRA);
group and two in the 12-week group were excluded after randomisation. 176 patients assigned to the 6-week treatment Referral Centre for Bone and in which data from patients who were
Cured without Sensitivity analyses
regimen and 175further NA
to the 12-week treatment regimen were NA analysed by intention
NA to treat. 160 (90·9%)
NA of 176 patients in Joint Infections, Hospital
lost to follow-up or died were removed†
antibiotic
the 6-week treatment‡
group and 159 (90·9%) of 175 of those in the 12-week group met the criteria for clinical cure. The difference Diaconesses Croix Saint-Simon,
between the groups (0·05%, 95% CI –6·2 to 6·3) showed the non-inferiority of the 6-week regimen when compared Analysis
Paris, France (V Zeller in which all persistent infections were counted
MD); 32/190 (16.8) 15/188 (8.0) 8.9 (2.2–15.6) 9.1 (2.6–15.5)
in the Lancet 2015 Unité Mobile des Référents en
with are
Data thenumber,
12-weekorregimen.
number (%)50 unless
patientsotherwise6-week group
specified. and 51 (16
32 patients in the 12-week
in the 6-weekgroup
grouphad andadverse
16 in theevents,
12-week the most Post hoc analysis in which only persistent infections that
Infectiologie, Villeurbanne,
29/187 (15.5) 13/186 (7.0) 8.5 (2.1–15.1) 8.8 (2.5–15.0)
were diagnosed after 6 weeks of antibiotic therapy
common being death (14 [8%] in the 6-week group vs
group) were classified as cases of probable failure of treatment[7%]
12 in independent
by the the 12-week validation
group), antibiotic
committee.intolerance
Of (12 [7%] vs France (B Issartel MD); Maladies
were counted‡
9 [5%]),
68 cardiorespiratory
protocol failure
violations excluded from (7the
[4%] vs 12 [7%]),
per-protocol and neurological
population, 18 cases complications
were classified as(7failure
[4%] vs 3 [2%]).
and 50 as cure in Infectieuses et Tropicales,
University Hospital,
Per-protocol§
the intention-to-treat population. *6-week group minus 12-week group. †Death in cases classified as probable cure by Montpellier, France
Interpretation 6 weeks of antibiotic treatment is not inferior to 12 weeks of antibiotic treatment with respect to the Analysis
MD);in whichofall persistent infections were counted 29/165 (17.6) 11/160 (6.9) 10.7 (3.6–17.9) 10.6 (3.7–17.5)
the independent validation committee were classified as failure. ‡Further antibiotic treatment was regarded as a (V Le Moing Division
proportion of patients with pyogenic vertebral osteomyelitis cured at 1 year, which suggests that the standard antibiotic Internal Medicine, University
treatment failure. NA=not applicable. Post hoc analysis in which only persistent infections that 27/163 (16.6) 11/160 (6.9) 9.7 (2.7–16.8) 9.7 (2.9–16.5)
treatment duration for patients with this disease could be reduced to 6 weeks. Hospital, Beaujon-Clichy,
were diagnosed after 6 weeks of antibiotic therapy
France (N Belmatoug MD);
Table 23 JNI,
2: Primary
es Bordeaux
outcome du 15 au 17/06/2022 were counted¶
ofanalyses
Health. of patients with vertebral osteomyelitis according to duration of NEJM 2021
Mobile Infectious Diseases
Funding French Ministry Unit, University Hospital,
Durées de traitement : individualisation ? 23es JNI, Bordeaux du 15 au 17/06/2022
Relais per os 23es JNI, Bordeaux du 15 au 17/06/2022
23es JNI, Bordeaux du 15 au 17/06/2022
NEJM 2019Un vieil antibiotique 23es JNI, Bordeaux du 15 au 17/06/2022
Rifampin-accompanied antibiotic regimens in the treatment
of prosthetic joint infections: a frequentist and Bayesian
meta-analysis of current evidence
Ozlem Aydın 1 & Pinar Ergen 1 & Burak Ozturan 2 & Korhan Ozkan 2 & Ferhat Arslan 1 & Haluk Vahaboglu 1
Received: 12 September 2020 / Accepted: 22 October 2020
# Springer-Verlag GmbH Germany, part of Springer Nature 2020
Abstract
ompromised
Prosthetic joint infectionsby cause serious morbidity and mortality among joint arthroplasty patients. Rifampin-accompanied
antibiotic regimens are recommended for gram-positive infections. This study aimed to combine current evidence supporting
se theeffects
who did not
rifampin supplement to an effective antibiotic in the treatment of prosthetic joint infections. We conducted a random-
meta-analysis with frequentist and Bayesian approaches. A total of 13 studies, all observational, were included in the
final analysis. The predominant bacteria in eight, two, and three studies were Staphylococcus spp., Propionibacterium spp.,
wereand Streptococcus
mostlyspp.,pa-
2
respectively. We pooled data from 568 patients in the staphylococcus subset (OR, 1.18; 95% CIs,
2
[0.76; 1.82]; I = 23%) and data from 80 patients in the propionibacterium subset (REM OR, 1.61; 95% CIs [0.58; 4.47]; I =
ticularly in the
0%). Both were insignificant with little heterogeneity. We pooled data from 483 patients in the streptococcus subset; the
pooled estimate in this subset favored the use of rifampin supplemented regimens (1.84; [0.90; 3.76]) with moderate to high
unaccounted heterogeneity (I2 = 57%). Bayesian random-effects models produced a posterior probability density indicating
that future studies will not favor rifampin supplementation in Staphylococcus infections (μ, 0.074; τ, 0.570; 89% HPD, [−
0.48; 0.54]). Bayesian posterior distribution in the Streptococcus subset displayed a tendency toward rifampin supplementa-
um subsets, nei-
tion. Studies had a substantial selection bias. Available evidence did not encourage rifampin-accompanied regimens for
staphylococcal infections.
rifampin-based
Keywords Staphylococcus . Propionibacterium . Streptococcus . Rifampin . Arthroplasty
which
Introduction
provide PJIs [3]. Along with an appropriate surgical strategy, a rifam-
malProsthetic
distribution,
joint infections (PJIs) cause a considerable burden
pin combination regimen is the recommended medical treat-
ment for susceptible staphylococcal etiology [4].
ities. Therefore,
in joint plastic surgery [1, 2]. Gram-positive microorganisms,
particularly Staphylococcus spp., are the predominant cause of
Rifampin, a major constituent of tuberculous treatment, has
excellent activity on gram-positive microorganisms. A major
probabilities of
Supplementary Information The online version contains
supplementary material available at https://doi.org/10.1007/s10096-020-
04083-4.
our study, high-
* Haluk Vahaboglu
23 JNI, Bordeaux du 15 au 17/06/2022
Korhan Ozkan
EJCMID
d via Bayesian
es
vahabo@hotmail.com korhanozkan76@gmail.comOpen Forum Infectious Diseases
MAJOR ARTICLE
Predictors of Treatment Success After Periprosthetic Davis J. et al OFID 2022
Joint Infection: 24-Month Follow up From a Multicenter
Prospective Observational Cohort Study of 653 Patients
Joshua S. Davis,1,2,3, Sarah Metcalf,4 Benjamin Clark,5 J. Owen Robinson,6,7 Paul Huggan,8 Chris Luey,9 Stephen McBride,10 Craig Aboltins,10,11
Renjy Nelson,12 David Campbell,13 L. Bogdan Solomon,14 Kellie Schneider,15 Mark R. Loewenthal,2,3 Piers Yates,15,16 Eugene Athan,17 Darcie Cooper,18 Table 5. Factors Associated With Treatment Success in Patients With Periprosthetic Infection Managed With Debridement, Antibiotics and Implant
Babak Rad,17 Tony Allworth,19 Alistair Reid,20 Kerry Read,21 Peter Leung,22 Archana Sud,23 Vana Nagendra,24 Roy Chean,25 Chris Lemoh,26
Nora Mutalima,27 Ton Tran,27 Kate Grimwade,28 Marjoree Sehu,29 David Looke,29 Adrienne Torda,30 Thi Aung,31 Steven Graves,32,33 David L. Paterson,34 and Retention as the Main Management Strategy Within 90 Days of Diagnosis (n = 352)
Laurens Manning5,16, ; on behalf of the Australasian Society for Infectious Diseases Clinical Research Network
Downloaded from https://academic.oup.com/ofid/article/9/3/ofac048/6520536 by guest on 14 June 2022
1
Menzies School of Health Research and Charles Darwin University, Darwin, Northern Territory, Australia, 2Department of Infectious Diseases, John Hunter Hospital, Newcastle, New South Wales,
Australia, 3School of Medicine and Public Health, University of Newcastle, Newcastle, New South Wales, Australia, 4Department of Infectious Diseases, Christchurch Hospital, Christchurch, New
Zealand, 5Department of Infectious Diseases, Fiona Stanley Hospital, Murdoch, Western Australia, Australia, 6Department of Infectious Diseases, Royal Perth Hospital, Perth, Western Australia,
Australia, 7College of Science, Health, Engineering and Education, Discipline of Health, Murdoch University, Perth, Australia, 8Department of Infectious Diseases, Waikato Hospital, Hamilton, New OR Rx Success 95% CI P aOR 95% CI P
Zealand, 9Counties Manukau District Health Board, Auckland, New Zealand, 10Department of Infectious Diseases, Northern Health, Epping, Melbourne, Victoria, Australia, 11Northern Clinical School,
University of Melbourne, Melbourne, Victoria, Australia, 12Department of Infectious Diseases, Royal Adelaide Hospital, Adelaide, South Australia, Australia, 13Department of Orthopaedic Surgery,
Wakefield Orthopaedic Clinic and The University of Adelaide, Adelaide, South Australia, Australia, 14Department of Orthopaedics and Trauma, Royal Adelaide Hospital and The University of Adelaide,
Adelaide, South Australia, Australia, 15Department of Orthopaedic Surgery, Fiona Stanley Hospital, Murdoch, Western Australia, Australia, 16Medical School, University of Western Australia, Perth,
Age 0.988 0.968–1.008 .259
Australia, 17Department of Infectious Diseases, Barwon Health, Deakin University, Geelong, Victoria, Australia, 18Geelong Centre for Emerging Infectious Disease, Deakin University, Geelong, Victoria,
Australia, 19Department of Infectious Diseases, St Vincent’s Private Hospital Northside, Chermside, Queensland, Australia, 20Department of Infectious Diseases, Wollongong Hospital, Wollongong,
New South Wales, Australia, 21Department of Infectious Diseases, North Shore Hospital, Auckland, New Zealand, 22Department of Microbiology and Infectious Diseases, Royal Hobart Hospital,
Presentation type (vs early)
Hobart, Tasmania, Australia, 23Department of Infectious Diseases, Nepean Hospital, Kingswood, New South Wales, Australia, 24Department of Infectious Diseases, Liverpool Hospital, Liverpool, New
South Wales, Australia, 25Department of Infectious Diseases, Latrobe Regional Hospital, Traralgon, Victoria, Australia, 26Department of Infectious Diseases, Dandenong Hospital, Dandenong, Victoria, Late-acute (n = 163) 0.26 0.15–0.46m/cid/article/73/9/1634/6273129 by guest on 09 March 2022
DAIR >4 wks after surgerya 18.6% (73/393) 19.6% (42/214) .75
Clinical Infectious Diseases Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; CRP,
MAJOR ARTICLE C-reactive protein; DAIR, debridement, antibiotics and implant retention; PJI, periprosthetic
joint infections.
a
For early acute (post-operative) PJI.
If, When, and How to Use Rifampin in Acute
Staphylococcal Periprosthetic Joint Infections, a
Multicentre Observational Study
patients who “survived” the intravenous period and were switched
Table 1. Baseline characteristics total cohort (n = 669)
Mark Beldman,1 Claudia Löwik,1 Alex Soriano,2 Laila Albiach,2 Wierd P. Zijlstra,3 Bas A. S. Knobben,4 Paul Jutte,1 Ricardo Sousa,5 André Carvalho,5 Clinical failure as secondary outcome parameter was 10.8%
1
to an oral regimen (n = 598). Treatment failure was(44/407)
Karan Goswami,6 Javad Parvizi,6 Katherine A. Belden,7 and Marjan Wouthuyzen-Bakker8
still signifi-
in the rifampin group, and 32.8% (86/262) in the no
Department of Orthopaedic Surgery, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands; 2Department of Infectious Diseases, University of Barcelona,
Total patient group (n= 669)
cantly lower in the rifampin group compared to therifampin no-rifampin
group (P < .001) (Figure 2B).
IDIBAPS, Hospital Clinic of Barcelona, Barcelona, Spain; 3Department of Orthopaedic Surgery, Medical Center Leeuwarden, Leeuwarden, The Netherlands; 4Department of Orthopaedic Surgery,
Martini Hospital, Groningen, The Netherlands; 5Department of Orthopaedic Surgery, Centro Hospitalar do Porto, Porto, Portugal; 6Department of Orthopaedic Surgery, Rothman Institute at Thomas
Jefferson University Hospital, Philadelphia, Pennsylvania, USA; 7Department of Infectious Diseases, Sydney Kimmel Medical College at Thomas Jefferson University Hospital, Philadelphia,
Downloaded from https://academic.oup.com/cid/article/73/9/1634/6273129 by guest on 09 March 2022
group (31.9% versus 45.4%, Rifampin
(n = 407)
P .001). In addition,
No rifampin
we reduced con-
Pennsylvania, USA; 8Department of Medical Microbiology and Infection Prevention, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands
(n = 262) P value
Background: Rifampin is generally advised in the treatment of acute staphylococcal periprosthetic joint infections (PJI). Outcome Rifampin Based Regimen According to Timing, Dose, and
However, if, when, and how to use rifampin founding
remains a matter
Baseline characteristicsof by
debate. indication
We evaluated the by
outcome subanalyzing
of patients treated with those
and patients who were
Co-Antibiotic
without rifampin, and analyzed the influence of timing, dose and co-antibiotic.
Methods: Acute staphylococcal PJIs treatedMale withnot
sex routinely
surgical debridement treated 43.5%
between 1999 with rifampin
and (177/407)
2017, 43.9%
and a minimal in oneofof the
(115/262)
follow-up .92 participating
A subanalysishos-was performed to determine whether the timing
1 year were evaluated. Treatment failure was defined
>80asyears
the need for any further surgical procedure related to infection, PJI-related
in of
therifampin, the dose and the co-antibiotic administered with
Age 23.4% (95/406) 18.3% (47/257) .12
pitals
death or the need for suppressive antimicrobial treatment.
Results: A total of 669 patients wereBMI >30 Treatment
kg/m
with those patients
2
48.1 % (177/368)
who 55.6% received
with(138/248)
rifampin
.07
hospitals
analyzed. failure was 32.2% (131/407) in patients treated rifampin rifampin were associated with treatment failure.
and 54.2% (142/262) in whom rifampinMedical that
was withheld do
(P
history routinely
< .001). treat
The most prominent with
effect rifampin
of rifampin
knees (treatment failure 28.6% versus 63.9%, respectively, P < .001). The use of rifampin was an independent predictor of
(thus,
was observed in excluding the patients
Diabetes
(OR 0.30, 95% CI 0.20 – 0.45). In the20.6% rifampin(84/407)
group, the use17 .9% (47/262) .39
treatment success in the multi-variate analysis
other than a fluoroquinolone or clindamycin Renal (OR
in10.1,these
failure
hospitals who
95% CI 5.65 – 18.2) and the 6.9%
did
start of (28/407)
not receive
rifampin within
of
5 days(18/262)
6.9%
rifampin
a co-antibiotic
after sur- .99
for i)any reason).
Timing. There was a wide range in the timing when rifampin
COPD Again, treatment failure was still15.6% significantly lower in the wasrifampin
gical debridement (OR 1.96, 95% CI 1.08 – 3.65) were predictors of treatment failure. The dosing of rifampin had no effect
on outcome. 18.4% (75/407) (41/262) .35 started (Figure 3). When rifampin was started within
Conclusions: Our data supports the Liver use of cirrhosis
rifampin in acute staphylococcal PJIs3.7%
group compared
treated(15/407)
with surgical 5.3%
to thebe discouraged,
no-rifampin
debridement, par- 5 days after surgical debridement, treatment failure was ob-
but requiresgroup (32.2% versus 61.3%,
(14/262) .30
ticularly in knees. Immediate start of rifampin after surgical debridement should probably further
investigation. Malignancy 14.3% (58/407) 14.5% (38/262) .93 served in 40.8% (80/196) of cases. Interestingly, treatment
Pstaphylococci;
< .001).
Downloaded from https://academic.oup.com/cid/
Keywords. periprosthetic joint infection; acute;
Rheumatoid arthritisrifampin; failure. 7.4% (30/407) 3.3% (22/262) .63
failure was significantly lower when rifampin was started
Factors
Characteristics implant associated with treatment failure according to the
combination therapy83% for staphylococcal after this time point: 20.9% (28/134) when started between
Acute periprosthetic joint infections (PJIs) Primaryare classically (338/407) PJI, 80.5%and its use has
(206/256) .40
treated with Debridement, Antibiotics, Irrigation and
of the implant (DAIR) [1–3]. AntibioticsCemented
uni- andHowever,
Retention
active against bac-
multivariate
particularly been incorporated
77.3%
despite the
analysis
in many
(310/401)
clear benefit
are
European
64.7%
of rifampin
shown
hospitals
(152/235)
reported
[5].
in the
in Table 2.
.001 dayThe
5 anduse
9, and 21.4 % (17/58) when started after 10 days
teria embedded in biofilm are the mainstay Fracture ofantibiotic
of the as rifampin
indication (OR et15.5%
prosthesis
study of Zimmerli 0.30) and
(63/407)
al., its necessity infected
16.5%
has been [6, 7].primary
(42/254)
questioned .72 (P .001). Subanalyses demonstrated that patients who re-
arthroplasties
Clinical presentationThe final number of patients included in the study of Zimmerli
treatment regimen. Since the randomized controlled trial per-
ceived rifampin within 5 days after surgical debridement had
(ORcom-
formed in the “90 by Zimmerli et al [4], a fluoroquinolone
Serum
0.59) were
et al. was limited independent
(i.e. 12 per treatment arm),variables
and monotherapy associated with treat-
bined with rifampin is considered the most effectiveCRP >115 mg/L
antibiotic 31.1%
with other antibiotics (124/399) has
than ciprofloxacin 34.3%
not been(87/254)
studied. .40 a significantly higher rate of S. aureus infections (74% versus
Serumment Leucocytes success.
Although
>12 Risk
many
cells/µL factors
observational
28.5% studiesfor
(113/396) treatment
do demonstrate
26.9% a higher failure
(60/223) .66 were a serum
failure rate in patients in whom rifampin was not prescribed 51%, P < .001) and mobile components were less often ex-
Late acute PJI 3.2% (13/406) 15.4% (39/253) 115 [8–10],mg/L (OR
these results
Received 29 March 2021; editorial decision 26 April 2021; published online 10 May 2021.
Identified micro-organism
may be 2.31), infections
due to confounding caused by Staphylococcus
by indication changed (32% versus 59%, P < .001) compared to patients in
or survival bias. In addition, lack of efficacy may be due to in-
Correspondence: Dr. M. Wouthuyzen-Bakker, internist-infectiologist, University Medical
aureusaureus (OR
adequate 1.88),
Center Groningen, PO Box 30.001, 9700 RB Groningen, The Netherlands (m.wouthuyzen-
bakker@umcg.nl). Staphylococcus cemented
dosing, inadequate
61.9% protheses
timing, or the56.9%
(252/407) result an interac- (OR
of (149/262) .19 1.69),whom malerifampin
sex was started after this time point. In addition,
tion with the co-antibiotic administered. In this retrospective
Clinical Infectious Diseases® 2021;73(9):1634–41
for early acute (post-surgical) infections, surgical debride-
(OR 1.59),
Polymicrobial
andobservational
multicentre
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases
a 37serum
.8%study, weleucocyte
(154/407) 37.8% (99/262)
aimed to answer the count
fol-
.98
of >12 cells/µL at Figure 1. 4Treatment failure (A) and clinical
ment performed more than weeks after arthroplasty was failure (B) rifampin versus no-rifampin
Society of America. This is an Open Access article distributed under the terms of the Creative
Surgical treatment lowing questions:
presentation (OR 1.55).
Commons Attribution-NonCommercial-NoDerivs licence (http://creativecommons.org/licenses/
by-nc-nd/4.0/), which permits non-commercial reproduction and distribution of the work, in any
Exchange modular components 45.6% (182/399) 45.2% (104/230) .92 according to the type of joint.
23es JNI, Bordeaux du 15 au 17/06/2022
medium, provided the original work is not altered or transformed in any way, and that the work
i) Do patients treated with rifampin have a better clinical out-
is properly cited. For commercial re-use, please contact journals.permissions@oup.com
DOI: 10.1093/cid/ciab426
DAIR >4 wks after surgery come compared18.6% to those(73/393)
a
19.6%is(42/214)
in whom rifampin withheld, .75 Clinical Infectious Diseases, 10 May 2021disappeared in the multivariate analysis (Table 3). We ad-
Clinical Infectious Diseases
ditionally analyzed whether the BMI/mg rifampin ratio T
MAJOR ARTICLE
affected outcome. The mean ratio was 27 (7.5 SD, range re
If, When, and How to Use Rifampin in Acute 12 – 55), but the ratio was not associated with treatment ri
Staphylococcal Periprosthetic Joint Infections, a failure (Table 3). Since rifampin may reduce serum levels of
Multicentre Observational Study pr
Mark Beldman,1 Claudia Löwik,1 Alex Soriano,2 Laila Albiach,2 Wierd P. Zijlstra,3 Bas A. S. Knobben,4 Paul Jutte,1 Ricardo Sousa,5 André Carvalho,5
Karan Goswami,6 Javad Parvizi,6 Katherine A. Belden,7 and Marjan Wouthuyzen-Bakker8 u
1
Department of Orthopaedic Surgery, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands; 2Department of Infectious Diseases, University of Barcelona,
IDIBAPS, Hospital Clinic of Barcelona, Barcelona, Spain; 3Department of Orthopaedic Surgery, Medical Center Leeuwarden, Leeuwarden, The Netherlands; 4Department of Orthopaedic Surgery,
Martini Hospital, Groningen, The Netherlands; 5Department of Orthopaedic Surgery, Centro Hospitalar do Porto, Porto, Portugal; 6Department of Orthopaedic Surgery, Rothman Institute at Thomas
Jefferson University Hospital, Philadelphia, Pennsylvania, USA; 7Department of Infectious Diseases, Sydney Kimmel Medical College at Thomas Jefferson University Hospital, Philadelphia,
multiple antibiotics [13], a subanalysis was performed for 66
Downloaded from https://academic.oup.com/cid/article/73/9/1634/6273129 by guest on 09 March 2022
w
Pennsylvania, USA; 8Department of Medical Microbiology and Infection Prevention, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands
Background: Rifampin is generally advised in the treatment of acute staphylococcal periprosthetic joint infections (PJI).
each oral co-antibiotic used, but in none of the antibiotic
However, if, when, and how to use rifampin remains a matter of debate. We evaluated the outcome of patients treated with and
without rifampin, and analyzed the influence of timing, dose and co-antibiotic. regimens, a higher dose of rifampin was associated with a a
Methods: Acute staphylococcal PJIs treated with surgical debridement between 1999 and 2017, and a minimal follow-up of
higher rate of treatment failure (data not shown).
1 year were evaluated. Treatment failure was defined as the need for any further surgical procedure related to infection, PJI-related
death or the need for suppressive antimicrobial treatment. so
Results: A total of 669 patients were analyzed. Treatment failure was 32.2% (131/407) in patients treated with rifampin iii) Co-antibiotic. Fluoroquinolones were prescribed as
and 54.2% (142/262) in whom rifampin was withheld (P < .001). The most prominent effect of rifampin was observed in
knees (treatment failure 28.6% versus 63.9%, respectively, P < .001). The use of rifampin was an independent predictor of co-antibiotic of rifampin in 46.9% (191/407) of cases, of
treatment success in the multi-variate analysis (OR 0.30, 95% CI 0.20 – 0.45). In the rifampin group, the use of a co-antibiotic
other than a fluoroquinolone or clindamycin (OR 10.1, 95% CI 5.65 – 18.2) and the start of rifampin within 5 days after sur-
gical debridement (OR 1.96, 95% CI 1.08 – 3.65) were predictors of treatment failure. The dosing of rifampin had no effect these included: levofloxacin (47.1%), ciprofloxacin (29.3%) 5
ou
on outcome.
Conclusions: Our data supports the use of rifampin in acute staphylococcal PJIs treated with surgical debridement, par- and moxifloxacin (20.4%). In 3.1% of cases multiple
ticularly in knees. Immediate start of rifampin after surgical debridement should probably be discouraged, but requires further
investigation. fluoroquinolones were used, most likely due to an antibiotic qu
Keywords. periprosthetic joint infection; acute; staphylococci; rifampin; failure.
switch during therapy. Treatment failure did not differ be-
a
Acute periprosthetic joint infections (PJIs) are classically
treated with Debridement, Antibiotics, Irrigation and Retention
combination therapy for staphylococcal PJI, and its use has
particularly been incorporated in many European hospitals [5]. tween the types of fluoroquinolones used, but a trend was
of the implant (DAIR) [1–3]. Antibiotics active against bac-
teria embedded in biofilm are the mainstay of the antibiotic
However, despite the clear benefit of rifampin reported in the
study of Zimmerli et al., its necessity has been questioned [6, 7]. observed in favour of levofloxacin and moxifloxacin (Figure n
treatment regimen. Since the randomized controlled trial per-
formed in the “90 by Zimmerli et al [4], a fluoroquinolone com-
The final number of patients included in the study of Zimmerli
et al. was limited (i.e. 12 per treatment arm), and monotherapy 4). Other oral antibiotics combined with rifampin were m
bined with rifampin is considered the most effective antibiotic with other antibiotics than ciprofloxacin has not been studied.
β-lactams (13.1%), linezolid (11.3%), clindamycin (9.6%),
Downloaded from https
Although many observational studies do demonstrate a higher
failure rate in patients in whom rifampin was not prescribed
Received 29 March 2021; editorial decision 26 April 2021; published online 10 May 2021. [8–10], these results may be due to confounding by indication cotrimoxazole (6.6%) and minocyclin (5.7%). When ex- i)
Correspondence: Dr. M. Wouthuyzen-Bakker, internist-infectiologist, University Medical or survival bias. In addition, lack of efficacy may be due to in-
Center Groningen, PO Box 30.001, 9700 RB Groningen, The Netherlands (m.wouthuyzen-
bakker@umcg.nl). adequate dosing, inadequate timing, or the result of an interac- cluding patients treated with triple therapy, the co-antibiotic
Clinical Infectious Diseases® 2021;73(9):1634–41
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases
tion with the co-antibiotic administered. In this retrospective
multicentre observational study, we aimed to answer the fol-
Figureof 3. Timingassociated
rifampin of rifampinwith
afterthe
surgical
highestdebridement.
treatment failure was
Society of America. This is an Open Access article distributed under the terms of the Creative
Commons Attribution-NonCommercial-NoDerivs licence (http://creativecommons.org/licenses/ lowing questions:
by-nc-nd/4.0/), which permits non-commercial reproduction and distribution of the work, in any
medium, provided the original work is not altered or transformed in any way, and that the work
cotrimoxazole (38%), and the co-antibiotic with the lowest
23Figure 2. Survival curve rifampin
i) Do patients treated with rifampin have a better clinical out-
versus no-rifampin. Survival curve rifampin
is properly cited. For commercial re-use, please contact journals.permissions@oup.com
DOI: 10.1093/cid/ciab426 JNI, Bordeaux
es du 15 au 17/06/2022 come compared to those in whom rifampin is withheld, treatment failure clindamycin (14%) (Figure 3). Infectious Diseases, 10 May 2021
Clinical
(n = 407) versus no-rifampin (n = 262) depicted according to treatment failure (A) Acute StaphylococcaRifabutin versus rifampicin bactericidal and antibiofilm activities
against clinical strains of Staphylococcus spp. isolated from bone and
joint infections
Pauline Thill 1*, Olivier Robineau 1,2, Gabrielle Roosen3, Pierre Patoz3, Benoit Gachet1,2,
Downloaded from https://academic.oup.com/jac/article/77/4/1036/6506691 by University of Lille user on 12 June 2022
Rifabutin and rifampicin antibiofilm ac t
Barthélémy Lafon-Desmurs1, Macha Tetart1, Safia Nadji3, Eric Senneville1,2 and Nicolas Blondiaux3,4
Median
1
Department of Infectious Diseases, Hospital of Tourcoing, Tourcoing, France; 2EA2694, Univ Lille, Centre Hospitalier de Tourcoing,
b
c
Antibotic/strain 0. 04 0. 08 0. 16 0. 32 0. 64 0.125 0.25 0.5 1 2 4 .4 MBEC
S.epidermids 3(6.4%) 1 (23.4%) 3(6.4%) 5(10.6%) 5(10.6%) 6(12.8%) 8(17%) 5(10.6%) 1(2.1%) 0 0 0 0. 64
CoNS 2(6.4%) 6(19.4%) 3(9.7%) 2(6.5%) 5(16.1%) 7(2 .6%) 3(9.7%) 1(3.2%) 1(3.2%) 1(3.2%) 0 0 0. 64
c
a
CoNS 1(3.2%) 1(3.2%) 1(3.2%) 1(3.2%) 9(29%) 2(6.5%) 2(6.5%) 2(6.5%) 4(12.9%) 7(2 .6%) 1(3.2%) 0 0.25
a
b
S.aureus 0 0 1(2%) 0 0 0 1(2%) 3(6%) 12(24%) 12(24%) 8(16%) 13(26%) 2
S.epidermids 1(2.1%) 1(2.1%) 0 2(4.2%) 6(12.8%) 2(4.2%) 6(12.8%) 6(12.8%) 14(29.8%) 8(17%) 0 1(2.1%) 0.5
S.aureus 0 3(6%) 1(2%) 1(2%) 4(8%) 3(6%) 9(18%) 17(34%) 6(12%) 3(6%) 0 3(6%) 0.5
Tourcoing, France; 3Department of Bacteriology, Hospital of Tourcoing, Tourcoing, France; 4Univ. Lille, CNRS, Inserm, Institut Pasteur de
Lille, U1019 - UMR9017 Center for Infection and Immunity of Lille, Lille, France
*Corresponding author. E-mail: pauline.thill@gmail.com
Received 2 September 2021; accepted 8 December 2021
Background: Staphylococci account for approximately 60% of periprosthetic joint infections (PJIs). Rifampicin
(RMP) combination therapy is generally considered to be the treatment of choice for staphylococcal PJIs but
carries an important risk of adverse events and drug–drug interactions. Rifabutin (RFB) shares many of the
properties of rifampicin but causes fewer adverse events.
MBEC(mg/L)
Objectives: To compare the minimal inhibitory concentration (MIC), the minimum bactericidal concentrations
(MBC), and the minimum biofilm eradication concentrations (MBEC) of rifabutin and rifampicin for staphylococ-
cal clinical strains isolated from PJIs.
Methods: 132 clinical strains of rifampicin-susceptible staphylococci [51 Staphylococcus aureus (SA), 48
Table3. DistributionofStaphyloc cus p .(numberofstrains)ac ordingtoMBEC
Staphylococcus epidermidis (SE) and 33 other coagulase-negative staphylococci (CoNS)] were studied. The
MBC and the MBEC were determined using the MBEC® Assay for rifabutin and rifampicin and were compared.
Results: When compared with the rifampicin MIC median value, the rifabutin MIC median value was signifi-
cantly higher for SA (P , 0.05), but there was no statistically significant difference for SE (P = 0.25) and CoNS
(P = 0.29). The rifabutin MBC median value was significantly higher than that of rifampicin for SA (P = 0.003)
and was lower for SE (P = 0.003) and CoNS (P = 0.03). Rifabutin MBEC median value was statistically lower
than that of rifampicin for all strains tested.
Conclusions: Using the determination of MBEC values, our study suggests that rifabutin is more effective than
rifampicin against clinical strains of Staphylococcus spp. obtained from PJIs. Using MBECs instead of MICs seems
to be of interest when considering biofilms. In vivo higher efficacy of rifabutin when compared with rifampicin
needs to be confirmed.
Rifampicn
Rifabutin
Introduction concentration but a larger volume of distribution, a longer term-
inal half-life, and higher tissue-to-plasma drug concentration
Staphylococci account for approximately 60% of periprosthetic ratio.10 Both in vitro and clinical studies show that rifabutin is
joint infections (PJIs).1,2 Biofilm formation contributes to the
23es JNI, Bordeaux du 15 au 17/06/2022 pathogenesis of staphylococcal PJIs and influences treatment
as efficient as rifampicin for the treatment of mycobacterial in-
fections.8 Only two studies have evaluated in vitro activity of ri- JAC 2022
outcomes.3,4 Rifampicin (RMP) combination therapy is generally fabutin against Staphylococcus spp. and concluded that theNouveaux antibiotiques 23es JNI, Bordeaux du 15 au 17/06/2022
with prosthesis retention (debridement, antibiotics, and implant retention—DAIR), attempt
Review eradication and cure with prosthesis removal (followed by prosthesis
Dalbavancin treatment for prostheticreimplantation in
joint infections in real-life: a
Dalbavancin for the Treatment of Prosthetic Joint Infections: national cohort study and literature review
eitherReview
A Narrative a one- or two-stage exchange procedure, or else a joint arthrodesis), or prosthesis a a b c d
Morgan Matt , Clara Duran , Johan Courjon , Romain Lotte , Vincent Le Moing ,
retention, abandoning the attempt to eradicate the Borisinfection inPavese
Monnin , Patricia favor ofChavanet
, Pascal
Luis Buzón-Martín 1,2, * , Ines Zollner-Schwetz 3 , Selma Tobudic 4 , Emilia Cercenado 5,6,7 and chronic , Lydiesuppressive
Khatchatourian , Pierre Tattevin , d
i
e
j
f
k
g
k
h
Jaime Lora-Tamayo 2,8,9 Vincent Cattoir , Catherine Lechiche , Gabriella Illes , Flore Lacassin-Beller ,
antimicrobial therapy [53]. Bearing this in mind,
1
a given
Eric Senneville , Aurélienantibiotic
Dinh , on behalf can perform
of the Dalbavancin very
French Study Group
Department of Internal Medicine, Infectious Diseases Division, Hospital Universitario de Burgos,
l a,∗
Antibiotics 2021
differently depending on which surgical strategy has been chosen.
a
09006 Burgos, Spain Infectious Disease Unit, Raymond-Poincaré University Hospital, AP-HP Paris Saclay University, Garches, France
b
2 Bone and Joint Infection Study Group of the Spanish Society of Infectious Diseases and Clinical Infectious Disease Unit, University Hospital of Nice, Nice, France
3
Microbiology (GEIO-SEIMC), 28003 Madrid, Spain; sirsilverdelea@yahoo.com
Section of Infectious Diseases and Tropical Medicine, Department of Internal Medicine, Medical University
c
d
e
Microbiology Laboratory, University Hospital of Nice, Nice, France
Infectious Disease Department, University Hospital of Montpellier, Montpellier, France JGAR 2021
Infectious Disease Unit, University Hospital of Grenoble, Grenoble, France
of Graz, 8036 Graz, Austria; ines.schwetz@medunigraz.at f
4 Infectious Disease Department, University Hospital of Dijon, Dijon, France
Department of Medicine I, Division of Infectious Diseases and Tropical Medicine, Medical University g
Infectious Disease Unit, Cornouaille Hospital, Quimper, France
Table 2. Clinical series published on the experience with DAL, including cases of bone and joint
5
of Vienna, 1090 Wien, Austria; selma.tobudic@meduniwien.ac.at
Servicio de Microbiología y Enfermedades Infecciosas, Hospital General Universitario Gregorio Marañón,
28007 Madrid, Spain; emilia.cercenado@salud.madrid.org
h
i
Infectious Disease Unit, Pontchaillou University Hospital, Rennes, France
Microbiology Laboratory, Pontchaillou University Hospital, Rennes, France
j
Infectious Disease Unit, Carémeau University Hospital, Nîmes, France
infection and prosthetic joint infection.
6 CIBER Enfermedades Respiratorias-CIBERES (CB06/06/0058), 28029 Madrid, Spain k
7 Infectious Disease Unit, Hospital of Mont-de-Marsan, Mont-de-Marsan, France
Medicine Department, School of Medicine, Universidad Complutense de Madrid, 28040 Madrid, Spain l
8 Infectious Disease Unit, Hospital of Tourcoing, Tourcoing, France
Department of Internal Medicine, Hospital Universitario 12 de Octubre, Instituto de Investigación Hospital 12
de Octubre i + 12, 28041 Madrid, Spain
9 Red Española de Investigación en Patología Infecciosa (REIPI), 28029 Madrid, Spain
* Correspondence: luisbuzonmartin78@gmail.com
n Bone & Joint Infection
a r t i c l e i n f o a b s t r a c t PJI Outcome
!"#!$%&'(!
!"#$%&' Reference (Other than PJI)
Abstract: Dalbavancin (DAL) is a lipoglycopeptide with bactericidal activity against a very wide Article history:
Episodes of PJI (Success, %)
Objectives: Dalbavancin is a long-lasting lipoglycopeptide active against Gram-positive ba
range of Gram-positive microorganisms. It also has unique pharmacokinetic properties, namely a Received 2 November 2020 methicillin-resistant staphylococci. Few data are available on dalbavancin use for treatm
Citation: Buzón-Martín, L.;
prolonged half-life (around 181 h), which allows a convenient weekly dosing regimen, and good Revised 15 March 2021
joint infections (PJIs). We describe a cohort of patients treated for PJI with dalbavancin
Bouza et al., 2017 [51] 69 13 20 80%
Zollner-Schwetz, I.; Tobudic, S.;
Accepted 27 March 2021
Cercenado, E.; Lora-Tamayo, J. diffusion in bone tissue. These features have led to off-label use of dalbavancin in the setting of bone literature regarding this condition.
Available online 4 May 2021
and joint infection, including prosthetic joint infections (PJI). In this narrative review, we go over
Morata et al., 2019 [50] 64 NP 26 NP
Dalbavancin for the Treatment of Methods: All adult patients with PJI from the French dalbavancin national cohort from
Prosthetic Joint Infections: A the pharmacokinetic and pharmacodynamic characteristics of DAL, along with published in vitro Editor: S. Stefani
1 January 2019 were included. We collected clinical and microbiological characterist
72 20 8 75%
and in vivo experimental models evaluating its activity against biofilm-embedded bacteria. We also
Tobudic et al., 2019 [45]
Narrative Review. Antibiotics 2021, 10, Keywords: through a standardised questionnaire. Clinical cure was defined as absence of clinical sig
656. https://doi.org/10.3390/ examine published experience of osteoarticular infection with special attention to DAL and PJI. Dalbavancin last visit. Failure was a composite criterion defined by persistence or reappearance of s
Wunsch et al., 2019 [49] 101 30 32 94%
antibiotics10060656 Prosthetic joint infection
and/or switch to suppressive antibiotic treatment and/or death from infection. The litera
PJI
Keywords: dalbavancin; prosthetic joint infection; gram-positive performed using PubMed.
Staphylococci
Martín et al., 2019 [48] 16 0 16 88%
Academic Editor: Jaime Esteban
Results: Seventeen patients were included. Bacteria were identified in 16 cases: Staph
(n = 10), including methicillin-resistant S. aureus (n = 1); and coagulase-negative staphy
Dinh1.et al., 2019 [52] 75 48 NP NP
Received: 20 April 2021
Accepted: 26 May 2021
including methicillin-resistant Staphylococcus epidermidis (n = 4). Sixteen patients (94.1
Introduction antibiotic therapy prior to dalbavancin use (mean of 2.2 ± 1.3 lines). Clinical cure was
Published: 31 May 2021
Total joint arthroplasties are common worldwide, and the incidence of this surgery patients after a median follow-up of 299.0 (IQR 97.0–476.0) days. We reviewed all cas
NP: not provided.
Publisher’s Note: MDPI stays neutral
PJI:
is expected to increase prosthetic
steadily joint
in the coming years infection.
as the population ages [1]. The most with dalbavancin available in the literature and the overall clinical cure was estimated a
with regard to jurisdictional claims in
feared complication is infection, which is not associated with high mortality rates, but does Conclusion: Our study and literature data suggest that use of dalbavancin in PJI could be
published maps and institutional affil-carry substantial morbidity, may require many surgeries, and the final results in terms as salvage therapy. Dalbavancin appears to be a safe and easy treatment for patients wi
iations. of limb functionality and pain resolution are not always satisfactory. At the same time, PJIs.
prosthetic joint infections (PJI) represent a massive economic burden for healthcare systems
An additional limitation of these studies is the wide heterogeneity in the use of DAL,
that continues to rise, and is expected to be around $1.62 billion in USA by 2030 [2].
PJIs are complex infections, in which the formation of biofilm, enabling bacteria to
© 2021 The Authors. Published by Elsevier Ltd on behalf of International Society
This is an open access article under the CC BY license (http://creativecommons.org
even within the same institutions. Loading doses on day 1 ranged from 1000 mg to 1500 mg,
Copyright: © 2021 by the authors.
Licensee MDPI, Basel, Switzerland.
evade the host immune system, is crucial. Biofilm-embedded bacteria can also develop
phenotypic changes that ultimately lead to antimicrobial tolerance and infection persistence.
Not all antimicrobials perform equally in this scenario, and not all antibiotics are ideal for
and following doses at day 7 ranged from 500 to 1500 mg. The number of doses was also
This article is an open access article
distributed23 es JNI,
the Bordeaux the treatment of PJI. In this context, the arrival of new antimicrobials is very welcome [3].
under terms and du 15 au 17/06/2022
DAL is a lipoglycopeptide (Xydalba; https://www.ema.europa.eu (accessed on 27
conditions of the Creative Commons
May 2021)) that is almost universally active against Gram-positive bacteria, which are byAny ≥1combination
adverse eventtherapy 20 (60.6) 0.8
- Yescombination
Any (n = 18) therapy 11 (61.1)
- - No(n(n
Yes = 15)
= 18) 9 (60)
11 (61.1) 0.8
antibiotics - Rifampicin
No (n = 15) combination therapy
-Rifampicin
Yes (ncombination
= 16) therapy
9 (60)
0.9
9 (56.3)
- - YesNo(n(n = 17)
= 16) 9 (56.3)
11 (64.7) 0.9
- No (n = 17) of treatment 6 weeks
Duration 11 (64.7)
Article Duration of =treatment ≤6 weeks 0.8
- Yes (n 13)
Tolerance of Prolonged Oral Tedizolid for Prosthetic Joint - - Yes (n = 13)
No (n = 20)
7 (53.8)
7 (53.8)
13 (65)
0.8
Infections: Results of a Multicentre Prospective Study - No (n = 20) 13 (65)
The follow-up
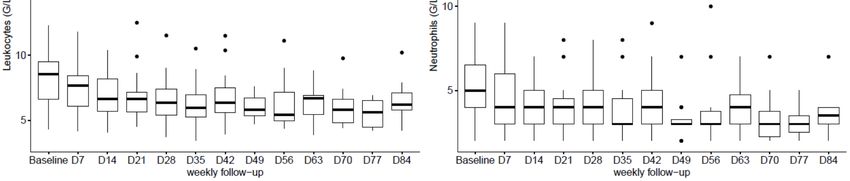
The follow-upofofthethehaematological
haematological parameters
parameters showed
showed a significant
a significant increase
increase of
of hae-
Eric Senneville 1,2,3, *,
Aurélien Dinh 4,5 , Tristan Ferry 6,7 , Eric Beltrand 3,8 , Nicolas Blondiaux 3,9 haemoglobin
moglobin blood
blood levels
levels between
between baseline
baseline andand
weekweek 6 followed
6 followed by by stabilisation,
stabilisation, as as well
well as
and Olivier Robineau 1,2,3 aassignificant
a significant decrease
decrease ininplatelets,
platelets,leukocytes
leukocytesandandneutrophils
neutrophils counts
counts between
between baseline
baseline
and week
and week 66 followed
followed by
by stabilisation
stabilisation until
until the
the end
end of
of the
the treatment
treatment (Figure
(Figure 1A–D).
1A–D).
Etude prospective multicentrique
1 Infectious Diseases Department, Gustave Dron Hospital, 59000 Lille, France; orobineau@ch-tourcoing.fr
2 Faculty of Medicine Henri Warembourg, Lille University, 59000 Lille, France
3 French National Referent Centre for Complex Bone and Joint Infections, CRIOAC Lille-Tourcoing,
33 patients infection prothèse ostéo articulaires :
4
59000 Lille, France; ebeltrand@ch-tourcoing.fr (E.B.); nblondiaux@ch-tourcoing.fr (N.B.)
Infectious Diseases Department, Ambroise Paré Hospital, 92100 Boulogne-Billancourt, France;
hanche (n = 19), genou (n = 13) et épaule (n = 1)
5
aurelien.dinh@aphp.fr
French National Referent Centre for Complex Bone and Joint Infections, CRIOAC Paris-Ambroise,
DAIR (33.3%), changement en 1 et 2 temps 17/56
75000 Paré, France
Infectious Diseases Department, Croix-Rousse Hospital, 69004 Lyon, France; tristan.ferry@univ-lyon1.fr
(51.5%/15.2%),
7 French National Referent Centre for Complex Bone and Joint Infections, CRIOAC Lyon, 69000 Lyon, France
8 Orthopaedic Surgery Department, G. Dron Hospital Tourcoing, 59200 Tourcoing, France
9
Bactéries : Staphylococci et enterococci
Microbiology Laboratory, G. Dron Hospital Tourcoing, 59200 Tourcoing, France
* Correspondence: esenneville@ch-tourcoing.fr; Tel.: +33-0-32694848; Fax: +33-0-32694496
Durée moyenne deAbstract:
ttt 8.0 ± 3.27
Objectives: Data onsemaines(6–12).
clinical and biological tolerance of tedizolid (TZD) prolonged therapy
Arrêt prématuré chez 6 patients
joint infections(18.2%)
are lacking. Methods: We conducted a prospective multicentre study including patients with
prosthetic (PJIs) who were treated for at least 6 weeks but not more than 12 weeks.
Intolerance au TZDknee(n(n== 2),
Results: Thirty-three adult patients of mean age 73.3 ± 10.5 years, with PJI including hip (n = 19),
13) and shoulder (n = 1) were included. All patients were operated, with retention
2 cas d’anémie (hémorragie)
!"#!$%&'(!
of the infected implants and one/two stage-replacements in 11 (33.3%) and 17/5 (51.5%/15.2%),
respectively. Staphylococci and enterococci were the most prevalent bacteria identified. The mean
2 échecs septiquesduration
!"#$%&'
of TZD therapy was 8.0 ± 3.27 weeks (6–12). TZD was associated with another antibiotic
in 18 patients (54.5%), including rifampicin in 16 cases (48.5). Six patients (18.2%) had to stop
Citation: Senneville, E.; Dinh, A.; Ferry,
T.; Beltrand, E.; Blondiaux, N.; Robineau, TZD therapy prematurely because of intolerance which was potentially attributable to TZD (n = 2),
O. Tolerance of Prolonged Oral Tedizolid early failure of PJI treatment (n = 2) or severe anaemia due to bleeding (n = 2). Regarding compliance
for Prosthetic Joint Infections: Results of
with TZD therapy, no cases of two or more omissions of medication intake were recorded during
a Multicentre Prospective Study.
the whole TZD treatment duration. Conclusions: These results suggestFigure Figure 1. Boxplot
1. Boxplot of
good compliance the
theahaematological
ofand haematological parameters
parameters ((A):
((A): Haemoglobin,
Haemoglobin, (B):
(B): Platelets,
Platelets, (C):
(C): Leukocytes, (D): Neutrophils)
Leukocytes, (D): Neutrophils)
Antibiotics 2021, 10, 4. https://dx.doi.org/
23 JNI, Bordeaux du 15 au 17/06/2022
es
10.3390antibiotics10010004
favourable safety profile of TZD, providing evidence of the potential during
during
benefit of Tedizolid
Tedizolid
the use of therapy.
therapy.
this agent Each
Each box
box represents
representsmedian,
median,interquartile
interquartilerange,
range,largest,
largest, Antibiotics 2020
smallest
smallestand
andoutside
outside(point)
(point)values.
values.
for the antibiotic treatment of PJIs.You can also read

















































