Nottingham University Hospitals NHS Trust DRAFT Partnership Plan 2019-2022
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Nottingham University Hospitals NHS Trust
DRAFT Partnership Plan 2019-2022
Executive Summary
Our Trust Strategy describes our vision of being ‘outstanding in health outcomes and patient and
staff experience’. Within our ‘partners’ promise, we make the commitment that ‘we will support
the improvement of the communities we serve through strong system leadership and
innovative partnerships to delivery integrated models of care’.
This short-term partnership plan sets out how key partnerships can help deliver on this
promise. The stakeholder mapping helps to see the breadth and depth of stakeholders whom we
have, and identify high impact partnerships as these are clearly where our efforts should ensure
clear and proactive management.
In this plan we considered and prioritised the key relationships and partnerships we want to
develop (or currently have) that help us achieve our Trust Strategy. We identified the following top
ten partnerships as priorities:
1. Integrated Care System (ICS)
2. Sherwood Forest Hospital (SFH)
3. University Hospitals of Leicester (UHL)
4. University Hospitals of Derby and Burton (UHDB)
5. United Lincolnshire Hospitals (ULH)
6. National Rehabilitation Centre (NRC)
7. Circle
8. University of Nottingham (UoN)
9. Nottingham Trent University (NTU)
10. Charities (including NUH Charity)
These were identified and agreed by the Executive Team based on a criteria (purpose,
sustainability, income generation or qualitative benefits and clear return on investment) as our high
impact stakeholders where there is a priority to develop or maintain that partnership. All of these
are existing partnerships (ICS, SFH, UHL, UoN, NTU, Charities), or strengthening the relationship
further (in the case of NRC, Circle, UHDB, ULH) and require a different focus for support
depending on current state and our strategic intent for the partnership. In addition we are working
with our tertiary partners and specialised service Planning Boards to develop network solutions
and regional models of care.
We have developed strategic intents for each of our priority partnerships, outlining how we
can progress the partnership to realise the benefits of collaborative working. These set a direction
of travel and embed a culture that moves the organisation towards greater collaborative working in
the delivery of integrated care for the population of Nottingham and Nottinghamshire.
Our plan also notes the need for leadership and governance, and each of the priority partnerships
will be owed by the nominated Executive Lead ‘Account Manager’, report into Management Board,
with a review and development approach moving forward.
1Section 1: Our Trust Strategy
1.1 Our Partners Promise and delivering this through our Partnership Plan
Our Trust Strategy describes our vision of being ‘outstanding in health outcomes and patient and
staff experience’. Success for Nottingham University Hospitals (NUH) and the population we serve
is only possible through the collective efforts of many - our staff, partner organisations, patients,
carers, members, volunteers, and other key stakeholders.
We have adopted six strategic objectives knows as ‘Our Promises’ (Table 1) underpinned by
enabling strategies, to the support the delivery of our vision. Within our ‘partners’ promise, we
make the commitment that ‘we will support the improvement of the communities we serve
through strong system leadership and innovative partnerships to delivery integrated
models of care’.
Table 1: Our Promises (Strategic Objectives)
Our Promises (Strategic Objectives)
1. Our Patients We will ensure our patients receive consistently high quality, safe care
with outstanding outcomes and experience
2. Our People We will build on our position as an employer of choice; with an
engaged, developed and empowered team that puts patient care at the
heart of everything it does
3. Our Places We will invest in our estate, equipment and digital infrastructure to
support the delivery of high quality patient care
5. Our We will consistently achieve our performance standards and make the
Performance best use of resources to contribute to an affordable healthcare system
4. Our Partners We will support the improvement of the health of the communities we
serve through strong system leadership and innovative partnerships to
deliver integrated models of care
6. Our Potential We will deliver world-class research and education and transform health
through innovation
Section 2: Developing our Partnership Plan
2.1 Objectives for the Partnership Plan
1. Consider and prioritise the key Relationships and Partnerships we want to develop (or
currently have) that help us achieve our Trust strategy.
2. Agree what are our strategic intents for our key partnerships, and areas we want to
pursue through collaborative working.
3. Set a direction of travel and embed a culture that moves the organisation towards
greater collaborative working in the delivery of integrated care for the population of
Nottingham and Nottinghamshire. Effective stakeholder relationships are a means to
providing accessible and responsive acute care.
Developing a partnership, whether formal or informal, should be a priority for those parties or
2organisations whom it is perceived are integral to achieving a strategic objective, or where the
added value that can be achieved through collaborative working is a significant uplift on what NUH
could achieve alone.
2.2 Different terms for relationships and partnerships
For the purpose of this plan we use the following terminology to describe our interactions with our
stakeholders.
Transactions
A ‘transaction’ is a one-off or series of interactions between stakeholders (individuals,
organisations or groups). There is no commitment to each other’s long-term success. An
example of a transaction is a one of purchase of equipment from a medical supplier e.g. supply of
blood pressure monitors.
Relationships
‘Relationship’ is a term used to describe an ongoing connection between two or more
stakeholders. Often, each stakeholder in the relationship has their own expectations of what that
means, however those expectations are rarely shared. An example of a relationship could be
between a patient and their GP.
Partnerships
A ‘partnership’ is a commitment to an ongoing relationship between stakeholders that is
characterised by mutual cooperation towards the achievement of specific shared goals/objectives.
For example a partnership may occur between neighbouring Trusts to deliver a joint clinical
service, with details outlined in a Service Level Agreement.
Partnership is about moving beyond responsibility for independent results to a relationship that
involves co-creation, shared risks and responsibilities, interdependency and organisational
transformation. True partnership is about identifying shared value and leveraging the combined
strengths of each partner to achieve a level of impact that could not be accomplished
independently.
Partnerships can take many forms, depending on the needs of the strategy and desires of the
partners. Figure 1 illustrates a continuum for collaborative working, with different types of
relationships.
3Figure 1: 5 Level Continuum Model for Collaborative Working
Section 3: Approach to developing a Partnership Plan
3.1 Identifying our key stakeholders
In our Partnership Plan development we have used the ‘NHS Improvement Stakeholder
Analysis’ approach to ensure a comprehensive identification and assessment of NUH’s key
stakeholders. We consulted with key colleagues within the organisation to generate a
comprehensive list of key stakeholders. Figure 2 presents a summary from a more detailed map.
Stakeholders were clustered into groupings by type of stakeholder, and this was sense-checked
and refined with internal colleagues.
Using the NHS Improvement approach, stakeholders were analysed in terms of power and
influence; from those with the greatest need for involvement, through to more peripheral individuals
or groups. The more important the stakeholder is to the success and impact of the strategic
delivery, the more time and resources needed to be devoted to maintaining their involvement and
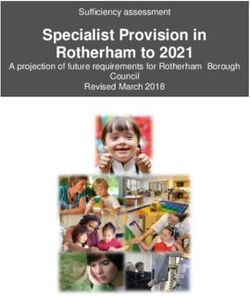
commitment. Figure 3 presents a power-influence analysis for key partnerships, including the ten
priority partnerships agreed by the Executive Team.
4Figure 2: Our 9 stakeholder clusters and summary of key stakeholders (not exhaustive list)
1. Population 2. Health & care commissioners 3. Commercial
Patients Nottingham City Council Other Trusts – local & national
Families & Carers Nottinghamshire County Council East Midlands Shared Service
Members Rushcliffe Clinical Commissioning (Nottingham City Council and
Patient Partnership Group (PPG) Group (CCG) Leicestershire County Council)
Patient Groups Nottingham City CCG Training:
Health & Well Being Boards Nottingham West CCG Nottingham Trent University
Healthwatch Nottingham & Notts. Nottingham North & East CCG University of Nottingham
Bloggers, tweeters & social media Newark & Sherwood CCG Trent Simulation
Voters & Citizens Mansfield & Ashfield CCG Private:
MPs & Local Councillors Associates Connect
Specialist, national and local media NHS England (inc. Specialised In Health
Commissioning) Other industry
4.Staff 5. Community & voluntary sector 6. Regulatory bodies
Salary Sacrifice partners NUH Charity (45 charities on Nottingham City Council
Discount deal partners register – examples below) Nottinghamshire County Council
Clinical & Non-Clinical staff Macmillan cancer support Notts. Fire & Rescue Service
Volunteers Maggie's Nottinghamshire Police
Unions Arthritis Research UK GMC
Recruitment companies Alzheimer's Society Department of Health & Social Care
American Nurses Credentialing Centre Health Foundation NHS England
East Midlands Leadership Academy Cystic Fibrosis Trust NHS Improvement
Nottingham Trent University British Pregnancy Advisory Health Education England
University of Nottingham Anthony Nolan Public Health England
Derby University Bloodwise Human Fertilisation and Embryology
Academy for Healthcare Science Royal Voluntary Service Authority
General Medical Council Nottingham Community Voluntary Care Quality Commission
Royal College of Nursing Services NHS Litigation Authority
Nursing & Midwifery Council League of Friends Crown Prosecution Service
Royal College of Midwives Citizens Advice Bureau Health & Safety Executive
National School of Healthcare Science Residents Forums
7. Procurement 8. Health & care providers 9. Research & Innovation
Suppliers: Integrated Care System Research regulators:
Johnson & Johnson Medical Ltd Greater/Mid Notts. Health Research Authority
Medtronic Ltd Health providers: Medicines & Healthcare products
Globus Medical Spire Regulatory Agency
Zimmer Biomet Circle NHS England
Meltemi Ltd Nottingham Emergency Medical Funders:
Cook Group Service National Institute for Health Research
Procurement partners e.g.: East Midlands Ambulance Service UK Research & Innovation
Supply Chain Co-ordination Ltd Notts. Healthcare Trust Wellcome Trust
Health Trust Europe CityCare Association of Medical Research
Yorkshire Purchasing Organisation GPs Charities/NUH Charity
Crown Commercial Services National Centre for Sport & Exercise Collaborators e.g.:
NHSI Medicine (NCSEM) East Midlands Academic Health
Pathology Network National Rehabilitation Centre Science Network
EMRAD University Hospitals of Derby & Collaboration for Leadership in
Estate & IT: Burton Applied Health Research & Care EM
Century Health University Hospitals of Leicester Clinical Research Network East
Elior United Lincolnshire Hospitals Midlands
Gentian Sherwood Forest hospital Sherwood Forest Hospital
Interserve Birmingham Children's Nottinghamshire Healthcare Trust
Nerve centre Sheffield hospital Clinical Research Network EM
System C/Graphnet Social care e.g.: Industry pharma & technology e.g.:
Dr Doctor Police Parexel, Quotient Sciences, SMEs,
Cisco Prison Service Medicity, Mediline EM, Biocity
GE Healthcare Nottingham City Council Academic e.g.:
Future models of procurement: Nottinghamshire County Council University of Nottingham
Category towers District and Borough Councils Nottingham Trent University
Midlands Health Innovation
53.2 Identifying our partnership priorities
The stakeholder map (Figure 2 summary) populates key stakeholders into nine clusters. Arguably
several stakeholders span the entire map or several clusters. From the stakeholder mapping work
it was identified that NUH has a wide range of relationships and stakeholders:
• Over 175 key stakeholders where identified across the organisation
• Around 30 of these relationships are classed as ‘partnerships’
Given the large number of stakeholders and existing partnerships/relationships there is a need to
prioritise and focus on areas that will have the biggest impact and benefit, and understand the
rationale and strategic intent for the partnership.
Our prioritisation (Table 2) was based on the following criteria:
1. Purpose: must help deliver our Trust strategy (and specific objectives).
2. Sustainability: Address issues i.e. operational, financial, workforce and infrastructure.
Measurable through improvements over time, e.g. new capital, equipment or innovations
resulting in efficiencies or improvements.
3. Meet either:
o a. Income Generation: The partnership secures revenue and increases income
generation, directly measurable through % increase in the value of
services/investment/sponsorship/infrastructure or indirectly through joint funding
awards (e.g. Biomedical Research Centre award).
or
o b. Qualitative Benefits: e.g. improved patient outcomes, pathways, enhanced
training opportunities, enhanced research.
4. Clear Return on Investment: Clear qualitative or quantitative benefits and outcomes
justify the investment of resource over time.
The following ten priority partnerships (Table 2) were identified and agreed by our Executive Team
as the areas for short-term focus, with a nominated Executive Lead identified.
Figure 3 presents a power-influence analysis for the 30 key partnerships identified in the
stakeholder mapping. From this larger list of partnerships, the ten priority partnerships agreed by
the Executive Team are highlighted in the black boxes. This shows the ten priority partnerships are
high in the power-influence analysis: ICS, SFH, UHL, NTU, UoN are within the high impact-high
power cell, and UHDB, ULH, NRC, Charities and Circle in the moderate power-moderate impact
cell.
All of the ten priority partnerships are existing partnerships, although some are more advanced
than others and require a different focus for support depending on current state and our strategic
intent for the partnership. We will follow the ‘seven steps for successful partnerships framework’
(presented in Appendix: Figure 4), which outlines the different stages of partnership development
and areas to consider and implement. The ICS, SFH, UHL, UoN, NTU and work with Charities are
more mature partnerships towards stages 5-7 in the partnership framework. In the case of NRC,
6Circle, UHDB and ULH the focus is around strengthening the relationship further towards a
partnership approach, stages 1-3 of the partnership framework.
Table 2: Priority Partnerships for 2019-20
Cluster/Theme: Partnerships Link to prioritisation Executive Leads
criteria:
1 2 3 4
Health & Care 1. ICS/STP, key areas: Tracy Taylor
providers a. CCGs
ICS b. Mid. Notts./Greater Notts.
c. Local Authorities (LAs)
d. Other providers – health &
social care
Health & Care 2. Sherwood Forest Hospital Keith Girling
providers (SFH)
Acute & other 3. University Hospitals of Alison Wynne
providers Leicester (UHL)
4. University Hospitals of Alison Wynne
Derby & Burton (UHDB)
5. United Lincolnshire Alison Wynne
Hospitals Trust (ULH)
6. National Rehabilitation Alison Wynne &
Centre (NRC) Rupert Egginton
Health & Care 7. Circle (TBC following TC Rupert Egginton
providers - Private procurement)
People (Education) 8. University of Nottingham () Keith Girling
and Research & (UoN)
Innovation 9. Nottingham Trent () Mandie Sunderland
University (NTU) & Nicky Hill
Community & 10. Key Charities (inc. NUH Mandie Sunderland
Voluntary Charity)
A separate internal document presents the Strategic Intent for each of the priority partnerships.
7Figure 3: Impact-Influence Analysis for 30 main partnerships with 10 priorities highlighted
Figure 3 presents a power-influence analysis for the 30 key partnerships identified in the
stakeholder mapping. From this the ten priority partnership areas identified by the Executive Team
(highlighted in the black boxes) fall in the high or moderate power, high or moderate impact cells.
(Note also the ICS partnership includes interactions with CCGs, Greater Notts./Mid Notts. and
Local Authorities – dashed box.)
High Satisfy Manage
power
CCGs ICS
Greater Notts. SFH
Mid Notts. UHL
LAs NTU
NHS England UoN
Moderate
power UHDB
ULH
NRC
Charities
Circle
Health & Social Care
Providers
Notts. Healthcare
PPG
Little or NCSEM
no power EMRAD
Pathology network
In-Health
East Midlands Shared
Service
Procurement partners
e.g. Century Health,
Elior, Gentian, GE
Healthcare
Monitor Research funders
R&I industry –
pharma/technology e.g.
Parexel, Quotient
sciences Inform
R&I networks
Little or no impact Moderate impact High impact
83.3 Regional Collaborative Groups
In addition to the ten partnership priorities, we are working with our tertiary partners and
specialised service Planning Boards to develop network solutions and regional models of care.
There are regional challenges with some tertiary and specialised services, which include
sustainability issues due to workforce shortages. Working with our partners we have established
the East Midlands Acute Providers Collaborative, which brings together NHS hospitals from
Derbyshire, Leicestershire, Lincolnshire, Northamptonshire and Nottinghamshire. The group is
represented by the Medical Director and Director of Strategy from the eight acute Trusts. The
group has identified six priority fragile services for regional focus in 2019-20: Head and Neck,
Radiology, Oncology, Neurology, Neurophysiology and ICU. Head and Neck is the highest priority
regionally.
NHS England are also establishing specialised services Planning Boards, with representation
from acute trusts including Directors of Strategy and Integration. The Planning Board will decide on
the services it will prioritise, but it is likely that they will focus initially on services where there is a
clear overlap with locally-commissioned services. The arrangements overseen by a Planning
Board are likely to encompass existing partnerships at STP or multi-STP level, such as cancer
alliances, transforming care partnerships, or mental health new care models, and may also cover
existing operational delivery networks or clinical senates. There are some pressing issues at the
moment, such as the approach to the development of Operational Delivery Networks (ODNs)
across the East Midlands.
4. Next Steps:
Governance:
• Leadership: Each of the priority partnerships will be owned by the nominated Executive
Lead ‘Account Manager’. This will align to an overarching stakeholder management
approach (developed by Laura Skaife-Knight, Director of Communications & External
Relations).
• Management: These partnerships will be supported by appropriate programme teams or a
nominated programme/relationship manager who will support the co-ordination and delivery
of the partnership.
Reporting:
• Updates and reporting: There will be quarterly updates at Management Board on each
partnership in addition to the regional collaborative groups, and progress updates to
Executive Team Meetings as required.
• Alignment to milestones and annual planning reporting: The agreed partnership
priorities will be incorporated into the refreshed Trust Strategy Year 2 milestones and
deliverables, and reported on via the annual planning reporting process.
Development:
• Alignment with Clinical Service Strategies and other Strategies: Through our Clinical
Service Strategies we will identify the need to work more closely with our partners,
specialities will need to develop their plans in conjunction with the Partnership Plan. The
Partnership Plan will also support (and align to) elements of other strategies and plans e.g.
People Strategy, Research & Innovation Strategy.
9• Annual review and refresh: At the end of the financial year (May) there will be a strategy
session with Management Board where we review what we have achieved, celebrate
successes, and explore where we go next with each of the partnerships. This review will be
key to aligning with the future direction of the ICS, and delivery of integrated care for the
population of Nottingham and Nottinghamshire.
10Appendix: Framework for effective partnerships
In developing our strategic intents for our partnerships, we have drawn on our seven steps for
successful partnerships framework:
Figure 4: 7 steps for successful partnerships framework:
Area of focus & rationale: Prompts:
1. Establish the need for partnership
The decision to partner comes down to • Define the issue the partnership will tackle and what
one key question: Are we better off it is meant to achieve – link it to the Trust’s
together than we are alone? What are objectives.
the benefits? • Determine if partnership is the right choice
• Identify what the partnership needs in order to be
Partnerships are a means to successful, and what partners bring to the
achieving a shared vision that no partnership and the benefits.
one partners could achieve on its • Think about who should make the approach and
own. Setting a clear case for best point of contact.
partnership from the beginning is
critical for future success.
2. Assess the risks and benefits of partnerships
Partners will share both successes • Ask hard questions – understand the deeper issues
and failures so considering the risks is as to why stakeholders should engage with one
an important step amidst the another, devote resources, invest time, and share
enthusiasm for the potential benefits risk.
from the collaboration. Risks include • Consider reputation and current/past performance of
reputational damage, loss of influence, the stakeholder and potential impact.
and heavy investment of resources. • Assess if the benefits outweigh the risks.
3. Build & maintain trust
Trust lays the foundation for open • Have honest conversations, use shared language
and honest conversations, achieves and actively listen to concerns.
partner buy-in, and encourages • Meet regularly – good communication requires more
commitment to the partnership at a than emails and conference calls, and in the early
deeper level. It is critical to sharing dates face to face interaction is key.
knowledge among partners internally • Acknowledge and respect differences (including
and agreeing on how to communicate culture, resources and motivation), these differences
successes and areas for improvement. are just as important as identifying shared values
and a common vision.
114. Set out a clear vision, objectives, understanding of mutual benefit and roles and
responsibilities
Successful partnerships set out clear • Align stakeholder interest and objectives for the
objectives, and a plan for how to partnership, this will reveal common overlap and
achieve them. Stakeholders must priorities.
often justify the investment of • Acknowledge individual benefits, in addition to
resources by demonstrating clear collective impact.
benefits and impact. • Set roles, responsibilities, and expectations at the
beginning and manage throughout.
• Co-create a clear plan and milestones to reach the
objectives.
• Jointly develop a flexible governance structure to
makes decisions and resolve issues.
5. Invest the time, people and resources to manage the relationship
The most successful partnerships • Engage sponsors: Successful partnerships have
are those in which all partners make high level sponsorship. Sponsors enable
the necessary investments both partnerships to secure resources including funding,
within their own organisation and staff time etc.
the partnership itself. Committing the • Empower champions: Champions are individuals
appropriate human, financial and that are deeply committed to the success of the
organisational resource upfront can partnership, leading from conception to
make operating the life of the implementation, helping navigate internal and
partnership more effective. external roadblocks.
• Appoint key relationship managers, providing key
points of contact and navigating bureaucracy.
6. Hold each other accountable, celebrate successes and learn from mistakes
Accountability in partnerships is a key • Regularly assess deliverables, timeframes and
factor. Mechanisms and governance allocated resources.
structures to monitor process, • Celebrate successes and key milestones
evaluate partner actions, and enable • Learn from mistakes, reassess or adjust plans.
accountability help to make sure the
partnership is achieving its
objectives.
7. Have an exit strategy
A successful partnership does not • Go into the partnership knowing it may not be
have to exist in perpetuity. Knowing successful, develop a contingency plan at the start.
when to move on is equally • Exit gracefully, celebrate the successes and key
important as knowing when to press achievements, consider how to apply lessons
on. learned to future partnerships.
12You can also read