No. 35 July 2016 - Special Feature Desirable Healthcare System Reform: How Hospitals Should Handle System Reform Tsuneo Sakai - 日本病院会
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

July 2016
No. 35 July 2016
Special Feature
Desirable Healthcare System Reform:
How Hospitals Should Handle System Reform
Tsuneo Sakai
Serial Number 35
No. 35 July 2016
JAPAN
HOSPITALS
The Journal of Japan Hospital Association
Contents
Foreword
Tsuneo Sakai 1
Special Feature
Desirable Healthcare System Reform:
How Hospitals Should Handle System Reform
Tsuneo Sakai 3
Submitted Article
Making Guarantees in Healthcare — Why Not?
John C. Wocher 17
In Healthcare —
When Is Good Enough, Good Enough?
John C. Wocher 21
Estimating the Impact of the New Income Deduction
System for Over-the-Counter Drug Expenses
Koichi Kawabuchi, Yusuke Kabeya 27
Development of Case Mix Based Evaluation
System in Japan
Shinya Matsuda 35
Hospitals and Big Data: Use of Case Mix and
E-claim Data in Japan
Shinya Matsuda 45
Financial Burden and Employment Support for
Patients with Cancer in Japan: A Review
Kiichiro Onishi 53Japan Hospital Association is committed to
contributing to society by enhancing hospital services
in Japan.
This journal introduces the activities of the
Association and healthcare in Japan to the world.
Enquiries regarding the Association and its services
should be addressed to:
Japan Hospital Association
9-15 Sanbancho, Chiyoda-ku, Tokyo 102-8414, Japan
Tel: 03-3265-0077 Fax: 03-3230-2898
Email: info@hospital.or.jp
Editorial Board
Journal and Newsletter Editorial Committee of the
Japan Hospital Association
Dr. Hiroshi Sakihara
Editorial Cooperation
faro inc.
6-15-1-5F Kasai bld., Hon-komagome, Bunkyo-ku,
Tokyo 113-0021, Japan
Tel: 03-6380-4888 Fax: 03-6380-5121
http://www.faroinc.com
Copyright © 2016 Japan Hospital AssociationForeword
Tsuneo Sakai
President, Japan Hospital Association
The 2016 JHA project plan was approved at the March 2016 Govering Council Meeting. I would like to explain the
important points contained in the plan.
Our goals in (1) “Promotion of Transparency” include “the promotion of information gathering, analysis, and sharing”
and “the establishment of a medical care support system.” These are linked with “the development of a think-tank function”
found in (2) Development of a Base to Facilitate the Operation of the JHA as a General Incorporated Association, and we
are planning to begin utilizing the Japan Hospital Association Strategy Tactics Information System (JHAstis). This system
was established to utilize electronic medical treatment prescription data to visualize and support the management of small
and medium-sized JHA member hospitals that do not adopt the DPC inpatient hospital payment system. We would also
make policy proposals by analyzing the data.
This system was established to help small- and medium-sized JHA member hospitals that have decided not
adopt the diagnostic procedure combination (DPC) inpatient hospital payment system through the visualization
of management status, the provision of support for management, and policy proposals based on the analysis of
accumulated electronic medical treatment prescription data from individual hospitals. We have been discussing this
system for several years, and it is a pleasure to see its implementation for member hospitals. Currently, 102 hospitals
are using the system, and we are continuing to improve it in regard to the management status visualization project
in cooperation with external organizations.
In (3) “Promotion of Future Hospital Care,” we set the goal of promoting an integrated community care system to
deepen our examination of suitable medical and nursing care collaboration for each region. The JHA has been focused
primarily on medical rather than nursing care. From this point on, we need to make nursing care a more active part of the
conversation. Considering the creation of the 7th medical care plan & the 7th long-term nursing care insurance project plan
that will be necessary after creation of the community care plan, we would like to take all possible measures to improve
nursing care.
In (4) Cultivation of Hospital Employees, we will work together on the implementation of the new medical specialist
system that is scheduled to start in 2017. Currently, this medical specialist system is being discussed by the Council on
Healthcare Provider Supply and Demand. There are potential problems in this new system which may lead to the increasingly
uneven distribution of doctors and the inevitable collapse of the medical care system. The medical specialist system faces
a wide range of challenges such as the need to maintain professional autonomy, the cultivation of high-quality human
resources, and the need to address the distribution of doctors. In addition, the many stakeholders in the system makes
reaching agreement on clear directions difficult; and addressing individual issues has been further complicated with the
establishment of a special committee under the Social Security Council Committee on Health Insurance and individual local
government councils to examine the uneven distribution of doctors both regionally and nationwide. This is the second venue
for discussion established by the Ministry of Health, Labour and Welfare (MHLW) following the council for the creation of
community care plans. If these function well, there is no problem. However, I have to say that there is the risk of widening
gaps among prefectures because a wide range of roles has been transferred to the regional level.
It is our hope that the Japanese Medical Specialty Board, the Board Certification Committee, and the Council share
information and that the MHLW serves as an effective coordinator among them. Hospitals have put significant effort
Japan Hospitals No. 35 / July 2016 1into senior resident education and training. We hope that all stakeholders fully understand that hospitals are willing to
contribute to the new medical specialist system more than ever.
An increase in the consumption tax to 10% in April 2017 has been voted into law. If this increase were to be postponed,
the government would need to look at alternative ways of securing the revenue required to for social security. Capital
investment into facilities and systems, and the purchase of major medical devices would be greatly hindered without the
appropriate resources. We will, however, continue working toward solutions to these issues by contributing our strengths
as an industry.
The medical accident investigation system will be reviewed in June 2016. The JHA continues providing wide
ranging support for the third-party Japan Medical Safety Research Organization. In terms of the issues related to
Article 21 of the Medical Practitioners’ Act, the JHA has been working on solutions in cooperation with the Japan
Medical Association (JMA).
This concludes my outline of the 2016 plans. I look forward to your continuing understanding and support as we enter
this new fiscal year.
2 Japan Hospitals No. 35 / July 2016Special Feature
June 2015 in Nagano
The 65th Japan Hospital Association (JHA) Congress 2015 Karuizawa
Desirable Healthcare System Reform:
How Hospitals Should Handle System Reform
Tsuneo Sakai
President, Japan Hospital Association
Chairman (Aizawa): It is both an honor and a
pleasure to present JHA President, Tsuneo Sakai, our Outline of Today’s Presentation
featured speaker. Well-known to everyone here, he needs
Introduction
no introduction; however, we have included his profile on • Changing environment surrounding the
pg. 88 of the Congress Guide for those who are interested healthcare system
The road to healthcare provision system reform:
in the specifics of his background. The title of his talk Desirable healthcare system
today is, “Desirable Healthcare System Reform: How • Community Care Vision
• Medical service fee optimization plan
Hospitals Should Handle System Reform.” Artificial intelligence
Now, without further ado, please welcome Dr. Sakai. New hospital management
• Further paradigm shift in healthcare
Sakai: Thank you. (Slide 1) In today’s presentation, I Conclusion
will talk about the “changing environment surrounding • “Proactively understanding patient needs”
and“seeking desirable healthcare”
the healthcare system,” “the path to healthcare provision
system reform,” “new attempts with artificial intelligence,”
Slide 1
and “new hospital management.”
National Council on Healthcare System Reform that
n Introduction – The changing was released in August 2013 has had a great impact on
environment surrounding the policies. I believe that things have already been decided
healthcare system for us.
I often use Slide 2; however, I have added some (Slide 3) I attended hearings conducted by the
new information on “policy decision maker” for this National Council on Healthcare System Reform
presentation. In the five columns bottom left, you see as a representative of the Council of Four Hospital
“reporting hospital bed functions,” “community care Organizations and submitted proposals, three of which
vision,” “Japanese Medical Specialty Board,” “Japan were included in the report.
Medical Safety Research Organization,” and “financial First of all, I explained that the medical service fee
stringency.” The Japanese government places the highest system had reached its limit. I then stated that we needed
priority on finance reform, which has resulted in the to have a better system, a system based on both the
Cabinet Office and Ministry of Finance placing significant Medical Service Act and the medical service fee system
pressure on the medical industry to stem increasing because it is impossible to solve the current problems
healthcare costs. In addition to this, the Report from the through economic inducements alone, and that appropriate
evaluations were essential. I also said it was necessary to
Takao Aizawa
President, The 65th JHA Congress 2015 Karuizawa
establish a system of healthcare provision that matches
Chairman & Director, Aizawa Hospital the needs of individual regions rather than to establish a
Japan Hospitals No. 35 / July 2016 3Changing Environment Surrounding the Healthcare System
Changes in the Healthcare and Response by the National and
Issues
Social Environment Local Governments
Rapid aging of society Combination of healthcare needs/
Changes in the proportion of disease Changes in healthcare
✓ Progress of artificial intelligence Alternative to healthcare providers?
Insufficiency of care providers and Maintenance and improvement of
o Establishment of a sustainable system
uneven distribution healthcare quality
by 2025
Gaps generated in the content and o Report from the National Council on
Progress of medical technology
quality of healthcare Social Security System Reform
(August 6, 2013)
Hospital bed functions that are hard for
Functionalization of hospital beds
users to understand
Functionalization of hospital beds and
✓ Reporting hospital bed functions o 2014 Revision of Medical Fee Service
community care vision
System (February 12, 2014)
Shift from hospital-oriented care to o Medical and Long-term Care Promotion
community-oriented care Act (June 18, 2014)
✓ Community care vision
Increasing involvement of local o Lower house election
governments/ Regional gaps (December 14, 2014)
Maintaining the quality of healthcare/ o Requests from the national government
✓ Japanese Medical Specialty Board o Future path has been determined.
Autonomy in healthcare ✓
Maintaining healthcare safety/
✓ Medical accident investigation system
Responsibilities of administrators
Prioritizing fiscal consolidation
✓ Financial stringency
Reduction of healthcare costs
Users/ Society Healthcare Providers Policy Decision Makers
Slide 2
JHA Involvement in the National Council on Social Security System Reform
- Major Flows of System Reform
The following three items were included in the report as the opinion of the Four Hospital Organizations.
(Hearing on March 27, 2013)
1. Limits of medical service fee system alone
• Need to have a system based on both the Medical Service Act and the medical service fee system
• Difficult to solve problems through economic inducements alone
• Appropriate evaluations
• Need to promote the establishment of a system of healthcare provision that matches the needs of individual regions rather
than a nationally unified system
2. Making a request to implement the plan earlier than scheduled
• Cannot wait another five years to set policy for the next term
3. Making a request to visualize data for the medical industry
• Development and disclosure of data
• Demand in regional healthcare/Need to have micro data that shows supply and demand
“Path to healthcare provision system reform that matches the long-term care needs of the nation”
National Council on Social Security System Reform by PhD. Yoshikazu Kenjoh (April 19, 2013)
Opinions that lead to the flow of current community care vision
Slide 3
4 Japan Hospitals No. 35 / July 2016nationally unified system. n Path to healthcare provision
Second, I asked the Council not to wait another five system reform: Desirable
years to set policy for the next term because the community healthcare system
care plan had already been implemented. (Slide 5) Some paths have already been determined.
Third, I asked the Council to promote data system One is the community care vision, and another one is
development and disclose data, including micro data that the adjustment of healthcare costs. These are already
would show supply and demand in regional healthcare. scheduled and must be completed by 2018. We do not
These requests were included in the report that formed have any more time to waste.
the basis of the community care vision.
Slide 4 shows the flow of the current reform. I also l Community care vision
use this slide often. Details of the healthcare system (Slide 6) The Community Care Vision Coordination
are usually based on the medical service fee system Council is to be established in the community care vision
and Medical Service Act. Currently, however, the to discuss bed functions to be handled by hospitals and
government has control over decision making and asks clinics with beds in the regions, the sharing of information
the medical industry to respond to proposals such as fiscal through the system of medical bed function reporting,
consolidation, the reduction of healthcare costs, and the projects to be included in the prefectural plans (annual
establishment of non-profit organizations. project plans for funds for community nursing care), and
Finally, the government wants to establish a other measures designed to facilitate achievement the
comprehensive community care system. However, I am community care vision.
worried because the system seems to focus on nursing Each hospital organization has contributed its
rather than healthcare. opinions to these discussions. The JHA considers the
active involvement of hospital organizations essential in
community care. Prefectural branch offices of the JHA
and prefectural hospital associations should take the
initiative in leading these discussions.
Three Flows that Determine the Path to System Reform
Medical and Long-term
Medical Service Fee System Care Promotion Act Reform led by the Cabinet Office
Reduction of 7:1 hospital beds Medical bed function reporting Fiscal soundness
Comprehensive community Reduction of social security costs
care beds Community care vision
Corporation system that
Comprehensive Community Care System promotes community care
Healthcare Nursing care
Hospitals:
Acute phase
Recovery phase
Chronic phase
Medical care requested by patients
Comprehensive Visiting hospitals &
community support day care facilities Implementation of a fixed cost for visits
Primary care
center/ doctors to large hospitals without a referral
Care manager
Medical service costs
Conducting Home/ Housings optimization plan
consultation and for the elderly with Home-
coordinating nursing care
Individual visit nursing
services Life support & nursing care
homes
care prevention
Comprehensive community
care system is planned for
junior high school districts with
populations of 10,000 or more Senior citizen’s club/ Residents’ association/
Nursing care prevention/ Life support, etc.
Slide 4
Japan Hospitals No. 35 / July 2016 5Path to Healthcare Provision System Reform
1. Community care vision
Content of community care vision guidelines
• Medical care demand reflecting the current status
• Desirable healthcare provision system considering the desirable number of hospital beds and average number of days of
hospitalization
• Desirable healthcare provision system that prevents regional gaps (e.g. rate of medical treatment received)
• Clear positioning of desirable healthcare provision system
2. Medical service fee optimization plan
Clear positioning of goals regarding the level of medical care service costs and average number of days of hospitalization
Need to review by the end of 2016 (by the end of 2017 if not sooner)
3. Path and time schedule have been determined.
Review Plan
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023
5 years 6 years
Healthcare
plan Establishment of community care vision
Current plan (5 years)
Interim Results
Medical evaluations evaluations
service costs New plan (6 years)
optimization Provisional
plan *Estalishing evaluations
community
care vision Implementation of the progress Reflecting to
earlier than management for each year the next-term plan
the schedule
Source: The Ministry of Finance Material documents issued on October 8, 2014
Slide 5
Community Care Vision Coordination Council (for Discussion)
Contents of Discussion
• Bed functions to be borne by regional hospitals and medical clinics with beds
• Sharing information through the System of Medical Bed Function Reporting
• Projects included in the plans of local governments (Annual plans of funds for long-term community nursing care)
• Other measures to achieve community care vision
JHA Concepts
• Necessary to have the active involvement of hospitals
• Prefectural branch offices of the JHA and prefectural hospital associations should take the initiative in leading discussions.
• Agreed that the chairman should be selected from a medical associations, but fairness should be ensured.
• It is desirable to realize effective collaboration among hospitals, clinics, and regions.
• Roles of hospitals and primary care doctors are important.
• It is desirable to establish team medicine focusing on users.
Slide 6
There are many opinions about who should serve as services can be provided. In order to initiate such services,
the chairman of the council. The JHA agreed that the hospital staff and staff in the regions must work together.
chairman should be selected from one of the medical (Slide 7) What is necessary for realization of
associations. What we must ensure is fairness. Fairness the community care vision is the optimization of
would enable us to realize effective collaboration among hospitals and regions. Specifically, it is necessary for
hospitals, clinics and regions. As Congress Chairman each hospital to understand its actual position in the
Aizawa mentioned in his address, it is extremely important community care vision.
to that roles are shared between hospitals and primary It is also important to visualize the state of community
care physicians, role sharing such as Aizawa Hospital has care and hospitals. It is necessary to objectively understand
implemented. Based on such a system, team healthcare the state of the entire region based on the actual data. This will
6 Japan Hospitals No. 35 / July 2016To Realize the Community Care Vision - Shift from Optimization of Hospitals to Regions
Understand the actual state of each hospital in the community care vision
Visualization of hospitals and community care data
• Understanding of supply and demand: Objectively understand the overall state of each region based on data
• Fair evaluations of hospitals: Quality of medical care and management
• Future goals of hospitals and regions
Points to be considered
• Improvement of incentives for employees
• Economic incentives at hospitals
Need to establish alliance which is more gentle than the Corporation System and that promotes community care
• Role sharing among facilities in individual regions
• Cooperation suitable for supply and demand in each region
• Cooperation focusing on human resources, products, finance, and information
Promote the optimization of hospitals and regions from the above-mentioned viewpoints
Slide 7
clarify the state of individual hospitals in the region, which on the assumption that the current system of healthcare
facilitates the evaluation of hospital management. However, provision will continue. Not all hospital beds are going
we must also evaluate the quality of the medical care at each to be occupied; therefore, the number of required hospital
hospital. Visualization of all of these elements can help us to beds is usually based on estimated supply and occupancy
create future plans for each hospital and region. rates. The MHLW sets the occupancy rate for highly-
What we need to consider as hospitals is the acute phase care beds at 75%, acute phase care beds at
improvement of incentives for employees. Hospitals have 78%, recovery phase care beds at 90%, and chronic phase
been influenced by economic incentives based on the care beds at 92%.
medical care service fee system. The figure shown in the lower right on Slide 8 shows
One example is the shift to 7:1 hospitals. I understand a comparison between the hospital bed functions in
that newly established comprehensive community care accordance with the System of Medical Bed Function
wards are not very popular, which I suspect is because Reporting and the actual status of hospitalized patients.
incentives for employees have decreased. You can see beds with different functions overlap
Furthermore, a corporation system that promotes significantly. We need to reduce this by 2025. However,
community healthcare, what is called the non-profit we are still not sure of the degree to which we will be able
holding company system, may be effective. If it is not a to accomplish this.
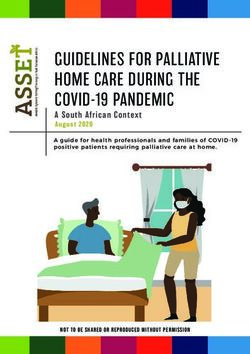
constrictive system, but a loose alliance, it will function The lower graphs in Slide 9 show the estimated
well. Such a system allows role sharing in the regions, number of hospital beds as of 2025, which was released
and cooperation that is suitable for regional supply and two days ago. The upper graphs show the numbers of
demand. Cooperation should be focused on people, hospital beds reported by the system, which reveals a
goods, money, and information. If we can achieve the significantly larger number of acute phase care beds.
above-mentioned, we will see a natural optimization of As Mr. Aizawa mentioned, it is a real possibility that
hospitals and regions. the Matsumoto Secondary Medical Service Area will
have a greater than 70% level of 7:1 hospital beds.
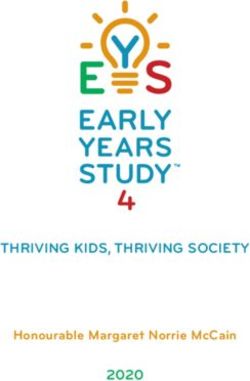
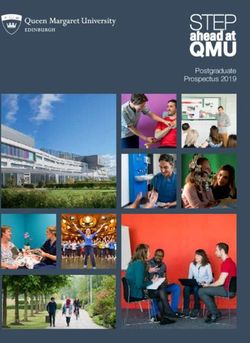
l Estimated number of beds (Slide 10) Is, as reported by the media, the number of
(Slide 8) The estimated number of required hospital beds, hospital beds excessive? They say, for example, that we
which has been discussed here and there, is arrived at by will exceed the required number of highly-acute and acute
comparing the estimated demand in regional healthcare phase care beds by 240,000 beds, that the required number
based on demographics with estimated supply based of recovery phase care beds will be short by 265,000
Japan Hospitals No. 35 / July 2016 7Estimate of Number of Required Beds
Comparison of estimated demand in regional healthcare based on demographics with estimated supply based on the the
assumption that the current system of healthcare provision will continue
Number of required beds is calculated with estimated supply and occupancy rates.
Number of required beds = Estimated number of supply ÷ Bed occupancy rate
Bed occupancy rates
Hospital bed functions selected by each hospital
• Highly-acute phase 75% in accordance with the reporting system
• Acute phase 78% Highly-acute Acute phase Recovery phase Chronic phase
phase
• Recovery phase 90%
• Chronic phase 92% Highly-acute
Actually hospitalized patients
phase
Need to assign patients in accordance with
hospital bed functions on each ward Acute phase
Hospitals naturally need to provide mixed care.
Recovery phase
Chronic phase
Hospital wards before the implementation Hospital wards after the implementation
of the reptorting system of the reptorting system (2025)
Slide 8
Estimated Number of Beds by Function
Long-term care beds General beds
Highly-acute phase (2014) 19.1
Acute phase (2014) 57.9
N=1,233,929 beds
Recovery phase (2014) 5.0 6.0
Chronic phase (2014) 26.6 8.6
Highly-acute phase (2025) 13.0
Acute phase (2025) 40.1
N=1,150,000–1,190,000 beds
Recovery phase (2025) 37.5
Chronic phase (2025) 24.2 – 28.5
0 10 20 30 40 50 60 (Unit: 10,000 beds)
Blue graph (upper): Reported medical bed functions (Vol.3) As of March 2, 2015; 6,996 hospitals (94.5%), 5,996 medical clinics with beds (78.6%)
Green graph (lower): Estimated number of beds as of 2025 (June 15, 2015 by MHLW)
Slide 9
beds, and that the number of chronic phase care beds and rehabilitation phase care beds.
will be 60,000 to 110,000 more than needed. However, There are many problems to be solved. The number of
these estimates are inaccurate. These estimates are, as recovery phase care beds will need to increase by 265,000,
you know, acquired from medical resource investment in which is equivalent to the excess number of highly-acute
DPC scores; however, as you know from routine medical and acute phase care beds. It is also, however, difficult to
consultations, hospital functions cannot be evaluated by understand the functions of recovery phase care beds.
scores alone. There is always debate over how to quantify Specifically, the number of required beds differs
such hard-to-evaluate functions. In addition, we also need depending on the positioning of comprehensive
to think about how we evaluate the functions of chronic community care wards, whose establishment is based on
8 Japan Hospitals No. 35 / July 2016Examination of Estimated Numbers of Hospital Beds
Is the number of hospital beds excessive?
• Highly-acute phase + Acute phase Excessive by 240,000 beds
• Recovery phase Insufficient by 265,000 beds
• Chronic phase Excessive by 60,000 to 110,000 beds
Problems
• Estimates acquired from medical resource investment
• Hospital functions cannot be evaluated by scores alone.
• Need to consider how to evaluate the functions of chronic phase care beds
Tasks
• Excessive amount of highly-acute and acute phase care beds used for recovery phase care.
• Recovery phase care bed function is not clarified.
• Number of required beds changes depending on the positioning of comprehensive community care wards.:Acute phase
or recovery phase?
• Need to confirm consistency of hospital bed function classification and medical service fees
• Overall hospital beds are not always excessive, but need to change hospital bed functions.
• Need to consider how hospitals promote user understanding
Slide 10
the medical service fee system, not on Medical Service Four Hospital Organizations were included in the policies
Act. Comprehensive community care beds will handle and reflected the adoption of the Medical Service Act.
patients that have been cared for by 7:1 hospitals, or who However, whether or not we will be able to achieve the
have been cared for at home or nursing facilities. The goals remains unknown.
comprehensive community care beds are for both patients In creating the community care vision, the national
from 7:1 hospitals and patients whose conditions have government is shifting control to local governments.
taken a sudden turn for the worse. The number of required However, we still do not know who will fulfill the think-
beds will change depending on whether comprehensive tank function. I think there will be gaps among prefectures.
community care beds are considered for acute phase or I also wonder how we should coordinate to facilitate
recovery phase. Simply showing figures does not help us realization of the comprehensive community care provision
to make decisions, and does cause misunderstanding. system. It depends on how well the Community Care
It is also essential to confirm the consistency of Vision Coordination Council functions. It is also necessary
hospital bed function classification and medical service to optimize individual hospitals and regions. For example,
fees. The overall number of hospital beds is not excessive, in the secondary medical care areas, public health centers
but it is necessary to change the hospital bed functions. are trying hard now. What roles the public health centers
It is always true that we need to consider medical care will play and how they will perform them in accordance
from the patient perspective. However, this is not always with the new vision remains unclear. I personally believe
clear cut, making it difficult to base decisions on patient that each prefecture should create university departments
perspective alone. that teach medical care management if they have not
already done so. These universities should then analyze
l Evaluation of and problems in the medical care and the system data, which we can all share
community care vision to improve the system.
(Slide 11) Functionalization of general hospital beds Another important issue is financial resources. In order
and the creation of community care vision are highly to ensure a smooth shift from, for example, acute phase
regarded. This is because general hospital bed functions care beds to recovery phase care beds, it is necessary to
that were previously related to the medical service have a firm system of financial support utilizing medical
fee system are clearly defined in accordance with the service fees and funds for community nursing care.
Medical Service Act. In addition to the functionalization of hospital beds,
As JMA President Yoshitake Yokokura stated at the another essential element is the expansion of the primary
opening ceremony, the proposals made by the JMA and care physician system in each region.
Japan Hospitals No. 35 / July 2016 9Evaluation of and Problems in the Community Care Vision
Functionalization of general hospital beds and the creation of community care vision are highly regarded.
• Functionalization of hospital beds that were previously related to the medical service fee system was promoted to be
clearly defined in accordance with the Medical Service Act.
• Conduct the above-mentioned functionalization from the viewpoint of regions
How to create the community care vision
• Who will fulfill the think-tank function that supports the creation?
How to prepare to realize future healthcare provision system in accordance with the vision
• Need to clarify the function of the Community Care Vision Coordination Council
• How to optimize individual hospitals and regions
• What is the role of public health centers?
• It is desirable to have the involvement of universities
Need to confirm that the community care vision will be beneficial for hospital management
• Effective utilization of financial resources from medical service fees and funds for long-term community nursing care
Essential to conduct functionalization of hospital beds and improvement of roles of primary care physicians
Slide 11
n Medical service fee outrageous opinion. He insisted on reducing the subsidies
optimization plan and funds to areas that were slow to optimize medical
(Slide 12) Let’s take a look at the medical service fee service costs. I don’t think such an absurd thing can be
optimization plan. done. Visualization of data and correction of the gaps in
This was established to set goals regarding the level medical service fees among regions is necessary; however,
of medical service fees and the effective provision of he said that evaluations of approaches to the plan by each
services in accordance with the community care vision, local government should be reflected to the subsidies
to perform factor analysis to check achievements, and to and funds by the national government. This is wrong.
initiate necessary measures. He does not understand the functions and efforts of the
At a meeting of the Council on Economic and Central Social Insurance Medical Council. I am always
Fiscal Policy, a member of the private-sector voiced an disappointed to hear such opinions. Such people focus
Medical Service Fee Optimization Plan
Set goals regarding the level of medical service fees and the effective provision of services in accordance with the
community care vision
If the achievements are far from the goals, it is necessary to perform factor analysis to initiate necessary measures.
Proposals made by a private-sector member at a meeting of the Council on Economic and Fiscal Policy held on
May 19, 2015
“Need to reduce medical service fees in the areas that are slow to optimize medical service costs”
• Need to promote visualization of gaps in healthcare provision system by prefectures
• Ask local governments to correct gaps of healthcare costs per person.
• Ask national government to evaluate approaches of local governments as of 2018 and reflect the results to subsidies
and funds.
• The outrageous opinion of a person who does not understand the functions of and efforts by the Central Social Insurance
Medical Council.
• Only focusing on the financial issues without considering the quality of medical services
Slide 12
10 Japan Hospitals No. 35 / July 2016on the financial issues without considering the quality of The Weekly Social Security magazine published an
medical services. article stating that a shift to the medical service fee system
by hospitals, regardless of whether they provide acute or
l Essential elements for success recovery phase care, would lead to stable management.
(Slide 13) An extremely important key to the success of At the Council on Economic and Fiscal Policy
this new system is incentives for medical care providers. meeting held on June 10, a private-sector member
As I mentioned before, the comprehensive community expressed the opinion that revising the medical service
care bed concept has been difficult to implement because fee system to clarify bed function and evaluation would
of undeveloped incentives. Medical service fees and facilitate reform. In response, the MHLW Minister said
subsidies provide inadequate compensation, making it that the Central Social Insurance Medical Council would
essential that we identify a more effective system. be discussing the clarification and evaluation of acute and
In addition, it is a challenge for nurses working at 7:1 chronic phase bed functions for the 2016 revision.
hospitals to make the change to 10:1 hospitals because Unfortunately, this were reported by the Health Policy
of the increased workload. It is also hard for physicians Bureau so that I am not sure to what degree the Health
to reassign acute phase care patients to recovery phase Policy Bureau and the Health Insurance Bureau will
care. What is important, then, is the sense of mission and cooperate; however, they have to cooperate to some extent.
accomplishment, purpose and pride that employees have.
These are non-economic incentives, however, whose n Artificial intelligence
effectiveness are difficult to evaluate. It is, therefore, (Slide 15) Artificial intelligence has become a part of the
desirable that these be covered by the medical care system world of medicine. Global trends have been changing
and medical service fee system. drastically, and our response to progress in artificial
(Slide 14) Another important element is linkage and intelligence has become a significant issue.
collaboration between the community care vision and The “da Vinci” robotic surgery system is an example
medical service fee system. JMA Deputy-President, of this. As its use has spread, some doctors are unwilling
Dr. Toshio Nakagawa, for example, stated that the purpose to perform surgery without it. Another example is the
of the vision is not to reduce hospital beds and medical Denou Sen Shogi Tournament, in which a computer shogi
service costs, but to assign hospital bed functions, and program successfully defeated professional players.
that for this reason the vision should not be linked with The March 30 edition of the Nikkei Business featured
medical service fee system revision. I agree with this. an article entitled “Amazing Artificial Intelligence.” The
Essential Elements for Success — Incentives for Medical Care Providers
Examples of comprehensive community care wards: Medical service fee system revision in 2014
• Implemented as a hospital function shifting from 7:1 hospital system
• Few implemented
• Registered comprehensive community care hospitals:
Number of beds corresponding to 7:1 hospital beds reduced by 11,600 beds
• Insufficient appropriate incentives
Economic incentives No. of facility No. of bed
• Medical service fees As of October 2014 920 24,600
• Subsidies, etc. As of April 2015 1,170 31,700
• Easy to understand, but none have succeeded
Non-economic incentives
• Sense of mission and accomplishment
• Purpose of work
• Pride
• Difficult to see effects, but extremely important
It is desirable that these be covered by the medical care and medical service fee system.
Slide 13
Japan Hospitals No. 35 / July 2016 11Linkage and Collaboration between the Community Care Vision and the Medical Service Fee System
The vision is not to reduce hospital beds and medical service costs, but to assign hospital functions, and for this reason the
vision should not be linked with medical service fee revision.
(Toshio Nakagawa, JMA Deputy-President, March 13, 2015)
A shift to the medical service fee system by hospitals, regardless of whether they provide acute or recovery phase care,
would lead to stable management. (Weekly Social Security, March 23, 2015)
MHLW statement (Council on Economic and Fiscal Policy, June 10, 2015)
• A private-sector member
“Revising the medical service fee system to promote the reform of hospital bed functions from 2016”
• MHLW
“Central Social Insurance Medical Council would be discussing the clarification and evaluation from acute to chronic
phase bed functions for 2016 revision”
Slide 14
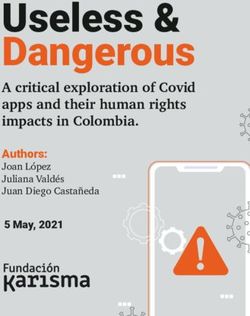
author discussed what is known in the world of robotics Oxford University. Some jobs will be highly automated in
as the Year 2045 Problem, when robots will be capable of the future. The jobs of librarians, telephone operators, and
having offspring with humans and other robots. I cannot orthoptists will all be handled by artificial intelligence,
imagine robot babies. Fortunately, I will not survive to while psychiatric social workers, audiologists, and oral
2045, so I won’t be around for it. There are two outcomes surgeons are not likely to be replaced by robots.
possible with artificial intelligence, friendly and hostile. We should not be pessimistic.
(Slide 16) Watson at IBM is very friendly. It collects We need to examine the content of each job. We need
information on diseases and effective treatments for to find added value in each job, and seek differentiation
individual patients from a tremendous amount of from artificial intelligence. It is an important problem that
documents and records. we will encounter sooner or later.
Slide 17 shows a quote from a shocking thesis about
future jobs in relation to artificial intelligence released by
Artificial Intelligence
— Need to Catch up with the Changing Technology
Global trends have been changing drastically.
How to respond to changes and progress of artificial intelligence
Two types of artificial intelligence; one is friendly and the other is hostile.
“da Vinci” robotic surgery system
Robots will be capable of having offspring
with humans and other robots by 2045.
Nikkei Business March 30, 2015
Denou Sen Shogi Tournament - FINAL
Slide 15
12 Japan Hospitals No. 35 / July 2016The Friendly IBM Robot, “Watson”
Collects information on disease and effective treatments for individual patients from a tremendous amount
of documents and records.
Different from the development of AI, whose functions are superior to humans, Watson was developed to
expand the ability of humans.
Humans are capable of
accumulating more than 1 million
GB of health information
(equivalent to the information in
more than 300 million books).
IBH Watson Health Cloud is capable of providing
tremendous amounts of personal information,
information on the environment, health, and
Source: https://www.flickr.com/photos/ibm_media/sets/ research to perform highly-advanced analysis
72157651509573960 and acquire necessary answers.
Slide 16
n Further paradigm shift in provision of high-quality, safe, and secure healthcare
healthcare – Hospital Measures based on clearly defined functions. Hospital should be
(Slide 18) I also often use Slide 18. This shows the need classified in patterns. In order to maintain sound hospital
for further paradigm shift. management, we need to have strong leadership, role
Hospitals must change if they hope to find solutions sharing and cooperation among mid-level employees
to the wide range of problems they will face. What do we in administration. We need to engage in future-oriented
need in the new paradigm? selection and decision making. We need human resources,
What we are trying to achieve is effective and efficient products, funds, and information.
Amazing Artificial Intelligence - Future Employment
Jobs that are likely to be automated Jobs that are not likely to be automated
Librarians 99% Psychiatric social workers 0.31%
Telephone operators 97% Audiologists 0.33%
Orthoptists 97% Occupation therapists 0.35%
Dental hygienist 97% Social workers 0.35%
Receptionists 96% Oral surgeons 0.36%
Source: “The Future of Employment” Carl Benedikt Frey, et al., University of Oxford, September 17, 2013
We should not be pessimistic.
Need to examine job contents
Need to find added value in each job
Seek the differentiation from artificial intelligence
Slide 17
Japan Hospitals No. 35 / July 2016 13Desirable Healthcare System Reform — Further Paradigm Shift
Old Paradigm New Paradigm
• Not clear
• Specialized care centering on acute • High quality, safe and secure healthcare
Goal phase patients • Healthcare based on clearly defined functions
• Quality of either healthcare or • Quality of both healthcare and hospital management
management
Leadership • Administration • Community residents: Cooperation in the regions
Center of discussions • Theoretical: macro data • On-site state state: micro data (accessible)
Classification of hospitals • Hierarchy • Functionalization
• Medical Care Act: Community care vision
Incentives • Medical service fees
• Satisfaction in working
• Strong leadership
• Unclear
• Roles and cooperation among mid-level employees
• Compartmentalized structure
Hospital management in management
• Continuation of management
• Future-oriented: Selection and decisions
• Human resources, products, and funds
• Human resources, products, funds, and information
• Healthcare provider-oriented • User-oriented
Concept of healthcare provid • Specialty-oriented • Team medicine
• Prioritizing on continuation • Changes/ Future-oriented
Slide 18
(Slide 19) High-quality medical care requires the l Establishment of the medical accident
establishment of a cooperative system between general investigation system
practitioners and primary care physicians. The role of Slide 20 gives the background of the establishment of
general practitioners at hospitals is, for example, patient the medical accident investigation system. This system
triage and initial treatment. Acute-phase care wards will be implemented in October 2015. It was created to
can provide postoperative care. Physicians working ensure safety in healthcare, to prevent the recurrence of
on recovery and chronic-phase care wards can serve medical accidents, and ensure the reporting of stillbirths
as hospitalists. Comprehensive hospitals can provide and unexpected patient deaths. The significance of roles
combined care to satisfy a wide range of patient needs and responsibilities of administrators will increase. The
from the perspective of community-oriented care. Japan Medical Safety Research Organization and other
The proposals made by the JMA and Four Hospital support organizations will be required to play extremely
Organizations included primary care physician functions. significant roles as a third party.
We view primary care physicians as doctors that patients We also need to address issues related to Article 21 of
can consult with about anything that concerns them, who the Medical Practitioners’ Act.
are familiar with the most advanced medical care, who
can refer patients to specialists and special hospitals, and n Conclusion — Proactively
who have the comprehensive ability to deliver health and understanding patient needs and
welfare for the community. seeking desirable healthcare
What we may need to consider increasingly in the near (Slide 21) When I was Director of Seirei Hamamatsu
future is differentiation between general practitioners and General Hospital, I asked all our staff to proactively
primary care physicians, and the system of cooperative seek to understand patient needs and pursue desirable
between them. healthcare. Although a significant challenge, I still believe
it to be of great importance.
The changing healthcare environment has had a
significant impact on measures. The path to the new
14 Japan Hospitals No. 35 / July 2016Seek High Quality Healthcare
- General Practitioners & Primary Care Physicians
General Practitioners
Roles at hospitals
• ER: Patient triage and initial treatment, etc.
• Acute phase care wards: Postoperative care, etc.
• Recovery and chronic phase wards: Serve as hospitalists (Respond to combined medical care needs)
Roles in the regions
• Serve as gatekeepers
• Respond to combined medical care needs
• Perspective of physicians who take care of the overall community
Primary Care Physicians
(August 8, 2013, Proposals for healthcare provision system made by the JMA and Four Hospital Organizations)
• Those who patients can consult with about anything that concerns them
• Those who are familiar with the most advanced medical care
• Those who can refer patients to specialists and special hospitals
• Those who have the comprehensive ability to deliver health and welfare for the community
How to differentiate general practitioners and primary care physicians
Slide 19
Seek Safe and Secure Healthcare
- Medical Accident Investigation System
Background
• May 2013: Summary of the Committee on the Investigation System for Medical Accidents
• June 2014: Establishment of Revised Medical Service Act including the Medical Accident Investigation System
• March 2015: Summary of the Committee on the Enforcement of the Medical Accident Investigation System
• May 2015: Promulgation of a partial revision of the Ordinance for Enforcement of the Medical Service Act (about the
Medical Accident Investigation System)
• October 2015: Enforcement of the Medical Accident Investigation System
System of investigations regarding medical accidents
• To ensure safety in healthcare and to prevent the recurrence of medical accidents
• To report stillbirths and unexpected patient deaths suspected or confirmed to have resulted from medical treatment
Explanation of investigation results to bereaved families by medical institutions
• To be explained appropriately in writing, in person, or both.
• Need to place efforts into explaining the purposes and results of the investigations in the way that the bereaved families choose
Future tasks
• Roles and responsibilities of administrators
• Roles of the Japan Medical Safety Research Organization and other support organizations
• Issues related to Article 21 of the Medical Practitioners’ Act
Slide 20
medical care provision system has already been decided. and achieve desirable healthcare.
We cannot change this easily, and we cannot be selfish in As Mr. Aizawa said, we need to act with self-initiative
seeking to create a system based on what benefits us alone. rather than under duress. Only when the entire staff at a
We need to optimize individual hospitals and regions hospital works together to achieve our goals will we be
from the patient’s perspective as we move toward the able to reform the system.
realization of the community care vision, the optimization I quote Charles Darwin: It is not the strongest of
of medical service costs, and increased healthcare quality. the species that survives, nor the most intelligent that
When considering these issues, we can see how hospital survives. It is the one that is most adaptable to change.
and healthcare system reform should be pursued. We need Thank you for listening.
to proactively understand patient needs. This is it. If we Chairman (Aizawa): Thank you, Mr. Sakai for your
focus on patient needs, it will be possible for us to pursue interesting and informative presentation. You provided us
Japan Hospitals No. 35 / July 2016 15Conclusion
- Proactively Understanding Patient Needs and Seeking Desirable Healthcare
The changing healthcare environment has had a significant impact on measures.
In order to respond to this, the path to the new medical care provision system has already been decided.
We cannot be selfish in seeking to create a system based on what benefits us alone.
We need to optimize individual hospitals and regions from the patient’s perspective as we move toward the realization of
the community care vision and the optimization of medical service costs from the users’ viewpoint considering the quality
of healthcare.
When considering these issues, we can see how hospital and healthcare system reform should be pursued.
This equals understanding patient needs.
If we focus on patient needs, it will be possible for us to pursue and achieve desirable healthcare.
It is not the strongest of the species that survives, nor the most intelligent that survives.
It is the one that is most adaptable to change.
(Charles Darwin)
Slide 21
with many suggestions about current state and problems
in healthcare and what we need to do from now. We have
hard work ahead of us.
16 Japan Hospitals No. 35 / July 2016Submitted Article
Making Guarantees in Healthcare — Why Not?
John C. Wocher
Executive Vice President, Kameda Medical Center;
Director, International Patient Services, Kameda Medical Center;
Consultant, Joint Commission International
Healthcare may be the only service industry that does INFORMATION
not come with a warranty or a guarantee. It strikes me REGARDING YOUR RIGHTS,
as somewhat odd that there is no fine print to read about RESPONSIBILITIES,
what is covered or not covered, and what rights one has OUR LIMITED GUARANTEE
if the service is found to be ineffective or is otherwise AND INFORMED CONSENT
dissatisfied with the service. However, I fully understand
that, because of the complexity, variability, and unique FICTITOUS GENERAL HOSPITAL
individual characteristics of each patient, it is often
difficult or impossible to predict outcomes. However, I It is important for you to read and understand this
think there are aspects of healthcare services that can be document, which is intended to inform you of your rights
guaranteed. If we desire to reassure patients that we have and responsibilities as a patient in this hospital or clinic
taken steps to ensure that we provide care under the safest as well as our informed consent process and our limited
conditions possible, and that we have gone above and guarantee to you of safe medical care. We consider
beyond the minimum requirements to put systems in place ourselves as partners in your healthcare experience with
that will give them confidence when they put their lives us, and we believe in transparency. You will be given a copy
in our hands, I think we should consider guarantees. I of this document on admission and at your first outpatient
understand this is controversial, and if we make promises, visit. Additional copies are available upon request. The
we have to keep them. I am proposing that hospitals point of contact at this hospital for inquiries or questions
consider adding some guarantees to the information we about the information on this form is: Xxxxxx X. Xxxxxx
typically provide to patients to instill that confidence. at 1234-46-7890.
The below form, combines the typical patient rights and
responsibilities, and suggested statements regarding the n Your Rights
informed consent process and adds an example listing 1. You and your family have the right to participate in
of guarantees. It is a work in progress, and this article is our care processes.
intended to provoke a discussion about whether we should 2. You have the right to be respected in a safe and caring
add guarantees to this information. Maybe the time has environment.
come to consider this. I think so. 3. You have the right to seek a second opinion within this
hospital or externally without fear of compromise, and
we can assist you with this if requested
4. You have a right to be informed of your medical
condition and diagnosis as well as the name of your
attending physician.
5. You have the right to proper evaluation and treatment.
Japan Hospitals No. 35 / July 2016 176. You have the right to assessment and management n Our Guarantee
of pain. 1. We guarantee that we have verified all physician and
7. You have the right to be protected from abuse. nurse licenses from the issuing authority, the Ministry
8. You have the right to spiritual services, and assistance of Health, Labour and Welfare.
will be provided upon request. 2. We guarantee that we have verified that all physicians
9. You have the right to refuse or discontinue treatment, have successfully graduated from from medical
and we will inform you of the probable consequences college by directly confirming with the diploma
of that decision. issuing authority. We have verified all nurses have
10. You have the right to refuse participation in research graduated by confirming directly with the nursing
studies college diploma issuing authority. All other licensed
11. You have the right to voice complaints, conflicts and healthcare providers have had their licenses and
differences of opinion for resolution. Our staff can tell education primary source verified.
you how to accomplish this and assist you. 3. We guarantee that we have verified all physicians’
12. You have the right to designate others to make specialty training directly from the specialty training
decisions for you. organizations.
13. You have the right to privacy and the confidentiality of 4. We guarantee that the vast majority (>90%) of our
your medical information in accordance with existing physicians, nurses, and other direct care providers
laws and regulations. have completed a course in basic life support (or
14. You have the right to see your medical record and be advance life support if required) and have a valid,
given a copy, in accordance with existing laws and unexpired certificate.
regulations. 5. We guarantee that your physicians’ credentials have
15. You have the right to be informed of the cost of been primary source verified and serve as the basis
treatment. for privileging, and that your physician is qualified
and privileged for the treatment he or she may render
n Your Responsibilities to you.
1. It is your responsibility to give correct and complete 6. We guarantee that your physician has an annual
information about your health status and health performance evaluation that is metric based and that
history. any substandard performance or concerns (if any)
2. You have the responsibility to ask questions if you do have been documented and corrected. Competency
not understand any information or instructions. assessments are done for all staff.
3. You are responsible for informing caregivers if you do 7. We guarantee that a Universal Protocol will be
not or cannot follow your treatment plan. followed prior to any surgery in order to ensure correct
4. You are responsible for the consequences, after you patient, correct procedure and correct site surgery.
are informed of them should you refuse treatment or 8. We guarantee that every prescription medication
to participate in your treatment plan. ordered will undergo an appropriateness review, prior to
5. You are responsible to cooperate with your caregivers. dispensing, to prevent any medication dispensing error.
6. You must respect the rights and property of others. 9. We guarantee that the building meets or exceeds the
7. You must tell your caregivers of any medications you National Fire Code and safety requirements and that
brought from home and/or are taking. Fictitious Hospital is in full compliance with existing
8. You must report any changes in your health status. laws and regulations.
9. You must not smoke in any building or on the grounds
of this hospital.
10. You are responsible for payment for the care provided
to you.
18 Japan Hospitals No. 35 / July 2016You can also read