CHILD BEHAVIORAL ASSESSMENT & MANAGEMENT IN PRIMARY CARE - WILLIAM B. CAREY, M.D. SEAN C. MCDEVITT, PH.D.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Child Behavioral
Assessment
& Management in
Primary Care
William B. Carey, M.D.
Sean C. McDevitt, Ph.D.


Table of Contents Introduction 6 Chapter 1: The Dilemma of the Primary Care Practitioner Today 8 Chapter 2: Obstacles to the Provision of Good Care 11 Chapter 3: What are the Problems? A Clinician’s Perspective on Behavioral Issues Presented in Primary Care 18 Chapter 4: Improving Assessment of Child Behavior in Primary Care 35 Chapter 5: Better Management in Primary Care. 48 Chapter 6: Prospects for Improvement in What We Understand and Can Do Clinically 61 Chapter 7: Conclusions 65 References 68 Appendix: Forms for Use in Primary Care 72 Tables and Figures Table 3.1: The BASICS Profile of Behavioral Adjustment 20 Table 3.2: Comprehensive Profile of Behavioral and Emotional Adjustment 22 Table 3.3: Basics Behavioral Profile- Ages 0-4 and 4-14 Years 24 - 25 Table 3.4: The Nine NYLS Dimensions of Temperament 27 Table 3.5: Clinician’s Impressions of Child’s Temperament 29 - 31 Figure 4.1: Algorithm for Management of Parental Concerns about Child’s Behavior 37 Table 4.1: Comprehensive Formulation of Assessment 41 - 44 Table 5.1: Management of Temperament Differences 53 - 54 Appendix: Forms for Use in Primary Care 72-80 1. Comprehensive Profile of Behavioral and Emotional Adjustment 73 - 74 2. Clinician’s Impressions of Child’s Temperament 75 - 76 3. Comprehensive Formulation of Assessment 77 - 78 4. Management of Temperament Differences 79 - 80

Child Behavioral Assessment & Management in Primary Care Second Edition
Introduction
Professionals who work with children in primary care 4. It encourages health care and educational
medical, psychological, and social settings are most professionals to feel more responsive to patients
likely to be oriented toward finding and diagnosing and students and be more effective in dealing
abnormal conditions requiring expert involvement. with their needs; and
Yet, the great majority of concerns expressed by
5. It avoids labeling children with psychiatric
caregivers about their children’s behavior are of mild
diagnoses when they really do not meet the
or moderate severity, not meeting any definition of a
criteria for them. It supports the use of
DSM-V disorder or requiring referral to a specialist.
environmental change rather than a reliance on
This book, written by two clinicians who have
medication.
worked for many years in primary care, rejects the
notion that behavioral issues should be simply Primary care providers, as defined in this book,
classified as normal or abnormal. Rather, the include pediatricians, family care physicians,
authors suggest that primary care professionals general nurses, pediatric nurse practitioners,
should view children’s behavior on a spectrum community and school psychologists, physician
where annoying normal variations may shade into assistants and others in general health service. They
problems and then to disordered behavior requiring may also include social workers, teachers, other
specialized care. This perspective is preferable to educators, and childcare providers who work directly
the limited approach of simply making categorical with children in an educational or care-giving setting.
judgments about whether or not the concerns being Utilizing theory, research, and clinical experience
presented by the caregiver are severe enough to gained over the last 50 years in the child
diagnose and treat as an abnormal condition or development field, the authors present a framework
declare that there is no real problem. There are for dealing with normal temperament and patterns of
several good reasons to conceive of behavior along mild to moderate reactive behavioral issues that
the broader spectrum: frequently confront professionals in primary care.
Suggestions are offered for direct assessment and
1. It recognizes and considers the many levels of
management of child behavior as well as indications
concern that caregivers have about their
of which problems will likely require referral
children; elsewhere for specialized services.
2. It allows for prevention and early intervention The perspective outlined here should prove valuable
with minor problems that are in a beginning or in educating new professionals in these several
developing stage; disciplines as well as assisting more seasoned ones
3. It educates primary caregivers and to refine and improve their approaches to these
empowers them to help resolve mild to moderate important issues in infancy and childhood.
behavioral conflicts with their children; With the first edition of this book having been issued
6
Child Behavioral Assessment & Management in Primary Care Second Edition
as recently as 2012, one might wonder why a
revision is being offered so soon. There is nothing to
correct in the earlier version. In fact, the two book
reviews in pediatric journals have been highly
complimentary (Almas R, 2015; Narayan A, 2012).
The difference here lies in an enhancement of the
earlier text by the introduction of further helpful
materials in most areas of the discussion of
assessment and management. This includes in
particular an expanded report of other views of
temperament beside the one we have found most
useful and a wider range of areas of application of
temperament counseling, A new chapter deals with
the problems with the confusion of terminology that
has crept into this field in recent years.
Acknowledgements
The authors are grateful for the support of three
colleagues who reviewed the original manuscript of this
book and offered helpful comments and suggestions:
Linda Caterino, PhD; Gerald M. Fendrick, MD; and Sarah
Macdonald, MD. Many thanks are due for their
assistance, though all problems and limitations in this
revised work remain the responsibility of the authors.
Heartfelt thanks are also owed to our wives, Ann Carey
and Suzi McDevitt,
7
Child Behavioral Assessment & Management in Primary Care Second Edition
The Dilemma of the Primary Care
Practitioner Today
Despite enormous scientific and technological children in their care. Sometimes clinicians are able
advances in many areas of healthcare in our times, to provide accurate and valuable counseling about
most primary practitioners dealing with children’s behavior, but far too often what they have to offer is
mental health today face a troubling gap in their not sufficient or really useful. Professional groups
preparation. Too often they have been given such as the American Academy of Pediatrics urge
insufficient training in the science and the practical members to provide exemplary care for their
skills needed to understand and manage the patients. They make recommendations that
wide variety of behavioral concerns that are sometimes helpful, but often supply
young people and their caregivers present to insufficient or incomplete knowledge to
them. Unfortunately, only being support the process. Pediatricians have been
taught about informed that in the next decade behavioral
abnormal concerns may occupy 30% of their time.
behavior
Yet, the two most recent
requiring referral
official advice papers
elsewhere does not prepare primary
from the Academy
practitioners to understand and deal
have been more
with the many varieties of normal
descriptive of the problems, screening, and
behavioral variations and conflict seen
parent education than promoting of solutions
daily while caring for children in a
by practitioners in individual interactive
clinical setting. Learning to identify
primary care settings (AAP, 2014; AAP, 2015).
“disease” does not make one
Neither mentions the existence or
competent to deal with lesser levels of
management of significant aversive but
discomfort or maladjustment. Most
normal temperament differences, nor are
sensitive professionals eventually realize
there comments on the availability and
that labeling a behavioral concern as
usefulness of the several established
“normal” and reassuring the caregiver that
comprehensive pediatric textbooks in the
the child will “grow out of it” does not help
field since 1983. The Institute of Medicine
the problem get resolved, and may be
(now the National Academy of Medicine)
misleading, inaccurate or even harmful.
(2015) has offered a similar general
Practitioners are expected to be competent overview of various points of view on
experts who can deal capably with “Opportunities to Promote Children’s
irregularities in the performance of infants and Behavioral Health; Health Care Reform and
8
Child Behavioral Assessment & Management in Primary Care Second Edition
Beyond. Workshop Summary.” It can be expected coaxed to take in comparable amounts and variety
that professionals in other primary child care and of foods. Her clinic nurse has been advising her
health related areas will be similarly challenged with mother on ways to increase Takesha’s intake by
behavioral matters in their areas of practice. various strategies such as putting cereal in the bottle
and urging her to keep taking another mouthful in
To illustrate the plight of the primary care
order to gain some reward. Vegetables must be
professional, we authors provide here some
consumed no matter what. However, since Takesha
examples of this confusion of concepts, diagnosis,
is growing and developing normally and eating a
and management strategies:
sufficient variety of foods, this bribery and coercion
Baby Frank (known to his mother as Frank the is inappropriate and may lead to overweight. Picky
Crank) is two months old and cries a great deal. The eating in this period is normal.
average baby at this age is crying not more than
Toddler Jill (known to her mother as Jill the Pill) is not
three hours a day, but this little boy is fussing or
the mild, obedient little girl her parents had expected
yelling for at least six hours a day in spite of good
but is highly persistent and very hard to redirect from
health and a vigorous appetite. The doctor has
forbidden activities. Her parents are frustrated by her
suggested two formula changes without success
opposition to them. They have been screaming at
and has finally told Frank’s desperate mother not to
her with increasing volume and have started to
spank her for her noncompliance. Not understanding
about the temperamental qualities of persistence
and low adaptability, the pediatrician has advised the
parents to “show her who is boss” and insist on
prompt cooperation. This misreading and
pathologizing of her temperament has led to
increased stress and greater rebellion. Jill just needs
time to adjust to new situations.
Three-year-old Harry is just starting day care. He
has trouble separating from his parents and is slow
worry because “it is only colic” and will be gone in to join in the play activities, just sitting on the edge
another month or two. The doctor has failed to watching. His inexperienced teacher reports to his
understand that the solution lies in helping the parents that Harry is “emotionally insecure.” His
mother now to understand the reaction pattern of competent parents are reassured by Harry’s doctor
this particular child and to respond to it more of what they already know, that he is just a shy but
appropriately, which will lead to a reduction in the normal child about whom there is no reason for
overstimulation and crying within days but will not, of concern.
course, alter his temperament.
Just turning five, Steve is finishing a preschool
Takesha is a healthy little girl of 18 months, but her program and about to enter kindergarten. His
mother is alarmed by her reduced appetite. She daycare teacher tells his mother on the last day
used to eat everything offered. Now she has to be there that Steve has ADHD and should be taking a
9
Child Behavioral Assessment & Management in Primary Care Second Edition
All of these vignettes have something in common.
They all involve a concern about a child’s behavior,
and unfortunately in each case the physician, nurse,
or teacher misunderstood the nature of the situation
and provided poor advice to the child’s family. An
opportunity to be helpful was lost and possible harm
was done.
These examples are the types of missteps that could
be corrected if the professionals involved had a solid
conceptual framework to use when dealing with
concerns about behavior. The authors will present
such an approach in the contents of this book. The
framework is intended for professionals in primary
care: medicine, nursing, education, child care, and
psychological counseling. It is not principally for
specialty referral personnel, though these
professionals may recognize the extension of their
main concerns into more general care. The
perspective presented here includes an analysis and
recommendations designed to cover concerns
stimulant such as methylphenidate. His parents are expressed in the three general areas of caregiver
angry that such a person should make this worry: truly dysfunctional behavior, aversive
neurological diagnosis and a recommendation for temperamental “fit,” and caregiver misperceptions of
therapy. After a more professional assessment it problems. It includes all levels of behavioral,
becomes clear that Steve is not overactive, not emotional, and functional performance from superior
inattentive, and not dysfunctional. He is simply a to average to perplexing normal variations to various
somewhat inflexible and negative child, whose dysfunctions and psychopathology. Thus, the
temperamental traits the parents were aware of and approach is concerned here with strengths as well
were handling well. The teacher had noted as weaknesses. This discussion does not attempt to
something different about Steve but had the poor cover physical problems or developmental issues,
judgment of labeling an annoying normal variation which are extensively discussed elsewhere (for
as a defect in brain function. example, Carey, Crocker, et al., 2009). By focusing
Charlie is not doing well in first grade. He says he directly on the elements of behavioral concerns the
does not like the work. His teacher tells the parents authors hope to define, and refine, the primary care
that this bright little boy is intelligent enough but is clinician’s view of the considerable ground between
just lazy. The school has not yet considered the normal child behavior and significant
possibility that he has a subtle learning difference or psychopathology.
disability.
10
Child Behavioral Assessment & Management in Primary Care Second Edition
Obstacles to the Provision of Good Care
In the previous chapter the need for improved developmental or behavioral problems. Defining
diagnosis and management by professional the role of the clinician as someone who only looks
persons was stressed. These providers are for diseases to diagnose and treat or refer ignores
responsible for delivering competent mental health a plethora of concerns that caregivers present to
services to children and caregivers in primary care. their health care professionals in the normal course
Several examples illustrated the variety of missteps of a youngster’s development. Furthermore, not
that occur today from the misuse of techniques now preparing professionals to respond appropriately to
commonly available. Before proceeding to the main caregiver concerns and limiting their view of their
content of the book—that is, to suggestions for expected role may result in a lessened interest and
improving behavioral assessment and treatment— level of competence in their subsequent practices.
it would be appropriate to review in greater detail A lack of training in dealing with behavioral
some of the current barriers to optimal professional concerns also provides the new practitioner with a
performance. This review will specifically clarify diminished source of intellectual stimulation, a
some of the areas in which changes proposed in lowered sense of job satisfaction, and greater
this book could correct many of the cited overall frustration.
deficiencies. There are currently three main areas
Clinical encounters provide an opportunity to
of weakness: 1) professional education, 2)
promote wellness in addition to curing diseases.
theoretical or technical problems, and 3) logistical
Many caregivers arrive at the office with minor
or practical limitations.
physical concerns but significant behavioral issues
with their child. An unresponsive clinician can
Professional Education actually intensify the caregiver’s worries by
Insufficient emphasis on behavioral care during the ignoring or discounting them. Communicating to
training of many primary care professionals with caregivers that their behavioral concerns are not
regard to information now available is undeniably a important if a physical illness is not discovered may
problem. For example, during the three years of only make matters worse. Frequently the
pediatric residency training even at the best nonphysical concerns that prompt a visit to a health
academic centers, a disproportionately large care professional indicate a pressing need for
amount of time is spent learning about the care of caregiver support. Instead primary caregivers
seriously ill children, with whom the trainees will should be able to deal with these concerns, taking
have minimal subsequent contact, and relatively the appropriate steps to assess, evaluate and
little learning about the vast majority who are intervene in an effective manner.
physically well or those troubled with the common The topography of normal behavior has been
11Child Behavioral Assessment & Management in Primary Care Second Edition
established by the last 50 or more years of 1. A Clear Definition of What is “Normal”
research in child development. Some improvement
There is little if any generally accepted definition of
in training has occurred over these years, but it is
the nature and full range of normal behavior.
nowhere near enough to meet the challenges of
Behavior is presumed to be normal if it doesn’t
today. Unfortunately this knowledge is transmitted
meet the criteria for what is defined as abnormal.
adequately to far too few professionals during their
However, there are many children whose behavior
training. A major enhancement of education is thus
is clearly problematic but who do not fit into any
needed. Primary care professionals need to be
diagnostic category. Thus, teaching new
taught to understand and respond to behavioral
professionals in their training to appreciate an
issues in the normal ranges of behavior, as well as
unclearly defined version of normal behavior is
to refer moderate to severe cases to providers who
problematic. Normal could be more accurately
specialize in treating them clinically.
described in an affirmative way, not just as an
Coincident with some small improvements in absence of abnormality. Two major consequences
education, there has also been a major shift in the of the normal/abnormal conundrum are: a) that
prevailing beliefs about where behavior problems ubiquitous temperament and adjustment variations
come from. A half century ago, human nature, both seen clinically may not be recognized as normal
normal and abnormal, was seen as being almost behavior, nor appreciated by clinicians in primary
entirely a reflection of the impact of the care as the assets they usually are; and b) that
environment. In the interim the consensus has bothersome or unusual but normal variations of
swung to the opposite extreme, that human adjustment are too often misunderstood and
diversity and mental status are largely determined identified as abnormalities. For example, a major
by intrinsic brain function with only a minimal role defect of the DSM system of the American
for the environment. Somewhere along the way, Psychiatric Association (2013) is that it does not
awareness of the basic concept of nature-nurture encompass recognition of normal variations in
interactions got lost, along with an appreciation of behavior. A child who is inattentive or overactive
largely innate temperamental variations as but who does not meet criteria for ADHD (Attention
mediators and moderators between the two. There Deficit/Hyperactivity Disorder) is eligible to be
has been a swing from an outlook of given the pathological label of ADHD- NOS (Not
“psychobabble” to one of “neurobabble” (Carey, Otherwise Specified) but not to be viewed more
2011b). accurately as “disorder free”—as possibly
challenging, but normal. Also, normal shyness
Theoretical and Technical appears to be frequently labeled as Social Anxiety
Deficiencies Disorder if it is bothersome to the caregiver. The
desire to provide help may prompt professionals to
Professionals in primary care face an urgent need diagnose cases that do not really meet the
for an improved diagnostic system and more diagnostic criteria. Professionals concerned with
practical management methods in dealing with behavioral health need a clearer definition of the
child behavior. Some specific areas for boundaries of normal so that both normal and
improvement are mentioned here:
12Child Behavioral Assessment & Management in Primary Care Second Edition
abnormal phenomena may be more clearly acceptable are generally not a part of the
understood, and normal behavior to be treated as evaluation process. They should be considered.
such.
Thus, current thinking about behavior in childhood
2. Clarity on what Constitutes a is based upon a rigid, categorical system for
Behavioral Problem defining abnormality when what is needed is one
that is developmental, adaptational, contextual and
At present the official catalogues of behavioral
interactional.
problems, such as the DSM-V and the ICD-10
(WHO 1992) offer to professionals lists of Just published in 2011 in a leading psychiatric
categorical pathological disorders, the criteria for journal was a collection of articles about what
which the child either does or does not meet. should be done to improve the existing mental
However, the current definitions of behavioral health diagnosis schemes. It was edited by the
disorders do not make clear the differences distinguished British psychiatrist, Sir Michael
between annoying variants of normal, which may Rutter (2011), and included five other international
superficially resemble the diagnosis but which do experts. They reached several important
not qualify, and levels of true dysfunction. For conclusions about revisions. Also, there was
example, exhibiting a pattern of low adaptability is general agreement on the “need to develop a
not the same as exhibiting an established, primary care classification for causes of referral to
consistent pattern of opposition to the requirements both medical and non-medical primary care.“
of the caregivers. However, their clinical Some of us in primary care have been working on
presentation can be quite similar in some this for a while and this book attempts to fill that
instances. (Francis A, 2013) need.
3. Resolution of Diagnostic Complexities 4. Methods for Evaluating Child Behavior
The current diagnostic schemes also do little to A number of clinical tools currently employed by
provide allowances for frequently observed practitioners have been developed to evaluate
changes occurring with development and various dimensions of behavior. However, most
maturation with advancing age. When the appear to be much less precise and more
diagnosis of a chronic disorder such as ADHD is inefficient than they ought to be, since they are
made in early childhood, the youngster may have based on the same classification system that
few or no signs of the disorder a few years later. So generates categorical diagnoses. The process of
much for chronicity! Important interactions within evaluating child behavior requires: a) accurate,
the context of the child’s environment are practical methods for collecting pertinent
responsible for much of what clinicians see in child information; and b) a realistic conceptual
behavior, but not acknowledged in diagnostic framework in which to organize the data
classifications as being in any way responsible, assembled for a diagnostic impression. Most
since the “disorder” is presumed to be all in the available measurement techniques have
child. Social and cultural differences in perceptions substantial limitations when compared with these
of the types of behavioral patterns considered standards.
13Child Behavioral Assessment & Management in Primary Care Second Edition
5. Methods for Obtaining Pertinent Questionnaire (SDQ) (Goodman & Goodman,
Information 2009); and the Parents’ Evaluation of
Developmental Status (PEDS) (Glascoe, 1979).
The general methods used in obtaining the
These tend to be too brief and impressionistic to
behavioral information necessary to establish a
allow an accurate picture of the child with sufficient
diagnosis are familiar to all clinicians: interviewing,
detail. Consequently, additional time interviewing is
observations, and questionnaires. However,
needed to supplement the information obtained
professional training in interviewing and making
from them.
observations of behavior is typically very minimal.
Beyond that, obtaining sufficient information to Some of the longer instruments are: The Child
provide assessment and guidance frequently Behavior Checklist (Achenbach & Edelbrock,
requires the use of standardized questionnaires 1983); Behavior Assessment System for Children
developed to measure behavioral status. The (BASC) (Reynolds & Kamphaus, 1992); Brief
advantages of these behavioral scales are: 1) they Infant-Toddler Social and Emotional Scale
gather information from the persons best (BITSEA) (Briggs-Gowen et al, 2004); Ages and
acquainted with the child; 2) they include some Stages Questionnaire: Social Emotional (ASQ:SE)
behavior not observable in the clinical situation, (Squires et al, 2002); Devereux Early Childhood
such as sleep or eating; 3) they are inexpensive Assessment Program (DECA) (LeBuffe & Naglieri,
and quick; 4) some have norms that tentatively help 1999); and Vineland Socio-Emotional Early
identify deviations; and 5) they provide quantitative Childhood Scale (Sparrow et al, 1998). Information
assessments concerning qualitative aspects of received from these tools seems to provide more
behavior. adequate data, at least about the child’s side of the
behavioral interaction.
Questionnaires available for use in primary care
today vary widely in their value to the practitioner. Undoubtedly the completion of an informative
Some direct response tools such as the HEADSS questionnaire has the tangible value of facilitating
(Home Education/Employment Activities Drugs communication between the clinician and the
Sexuality Suicide) seem to work for eliciting from parent or teacher. However, there are still problems
adolescents discussions of important areas of limiting their usefulness at the primary care level:
stress and conflict. Clinicians attempting to find out 1. The data provided may suggest which
about comparable strengths and concerns in youngsters need a referral to a specialist but do
prepubertal children or their parents frequently use not assist the primary care clinician in dealing
some sort of caregiver report instrument. Some with a present problem that does not require a
brief screening checklists provided mainly by referral;
psychiatrists and psychologists are: The Pediatric
Symptom Checklist (Jellinek et al. 1986); The 2. There is no evidence supporting the
Eyberg Child Behavior Inventory (Eyberg & Ross, contention that behavioral rating scales are any
more efficient than brief, well directed
1978); The Conners Parent Rating Scale (Goyette interviewing;
et al, 1978); The Strengths and Difficulties
3. With rare exceptions assessment instruments
14Child Behavioral Assessment & Management in Primary Care Second Edition
rate only abnormalities and not positive normal children but have not been verified clinically
behavior; or shown to have value in clinical studies or
practice. We clinicians are asked to provide help
4. Most scales utilize behavioral items that are
with present concerns, not to make predictions.
highly impressionistic. For example, what does
“often talks excessively” mean?; 6. A Realistic Behavioral or Mental
5. Many do not separate out the less from the
Status Diagnostic Profile
more serious problems; for example, nose Once data are gathered, the dilemma is how to
picking from fire setting; classify the information obtained. No existing
system appears to have an entirely satisfactory
6. Questionnaires do little to reveal the extent of
method for utilizing the data in primary care. The
the issue or its impact since most rate frequency
DSM-V, (2013), the most widely known one, is
rather than the effects of issues being rated;
primarily intended for adults, uses the categorical
and
“medical model,” and does not recognize or
7. With rare exceptions they neglect information describe normal variations.
on caregiver-child interactions, which will almost
The DSM-PC of the American Academy of
always be the focus of parent counseling. (see
Pediatrics (1996) aimed to overcome all of these
Carey, 2009).
limitations, but, despite its valuable offering of three
And yet, use of these questionnaires is what is levels of concern, it failed, among other
generally promoted in pediatric texts for behavioral shortcomings, to acknowledge physical health,
screening and evaluation, rather than more temperament, developmental status, and parent-
sensitive, individualized interviewing. These child interactions as major contributors to
suggested scales are usually offered by persons behavioral outcome. The ICD-10 of the World
with little or no primary care experience. Health Organization (1992) also deals only with
As for the evaluation of normal temperament disorders and essentially does the same job as the
characteristics, a division of opinion has occurred DSM. The DC: 0-3 (2005)... describes itself as “a
in how to do this. Clinicians have generally found systematic, developmentally based approach to the
that the nine traits originally established in the classification of mental health and developmental
1950s by Thomas, Chess, and Birch (1968) are the disorders in the first four years of life.” Its more
best to use because of their clinical derivation and comprehensive approach is promising but it fails to
established practical usefulness. However, include normal temperament in any appropriate
academic developmental psychology researchers way. The International Classification of
have followed the path of submitting observed and Functioning, Disability and Health for Children and
reported data to factor analysis in order to arrive at Youth (ICFCY), also from the WHO (2001), is
packages of specific behaviors that serve better for remarkably comprehensive but it is regarded as too
the purpose of making predictions about later concerned only with impairments of function. The
personality. These computer generated dimensions Big Five (Eysenck, 1994) have gained in favor
apparently work well for studies of behavior in among colleagues in developmental psychology.
However, the five adult characteristics of
15Child Behavioral Assessment & Management in Primary Care Second Edition
extraversion, conscientiousness, agreeableness, not always the preferred one. (I [WBC] can recall a
emotional stability, and openness to experience do young pediatric trainee several years ago who
not fit with well with the chief clinical concerns of advised a parent that the best way to stop a child
parents about their children like social competence, from waking up at night was to put him in time out
task performance, and eating and sleep problems. when he did it!) Too many clinicians fail to
(For a more extensive evaluation of these scales individualize the parent counseling to the specific
see Carey, 2009). situation and to deal with problems in the particular
interaction apparently responsible for the trouble.
7. Tools for Managing Behavioral Issues
Meanwhile, reliance on drugs has reached an
in Primary Care
alarming extent. (Grundmeier R, Fiks A, Liu W, et
For the professional person in children’s primary al, 2015)
care, recommendations for how to manage a
To replace the common inadequate alternative
problem that has been diagnosed usually follows
strategies of Dodge, Quick Fix, or Immediate
the “medical model,” which proposes that for each
Referral, this book will encourage a framework for
condition there is a specific preferred, evidence-
selecting interventions that offers an individualized
based plan of treatment. Unfortunately for
and comprehensive approach that is more likely to
clinicians, particular behavioral interventions with
be successful.
children and caregivers do not work so
conveniently. Giving standardized advice is usually
effective for only a small percentage of cases and Logistical Problems
may make others worse instead of better. For Besides the issues of educating trainees and the
example, there is generally thought to be an theoretical and technical barriers described above,
there are some practical obstacles that should be
mentioned here. One major problem is the
availability of professional time to deal with
caregiver concerns that do not align with a
traditional medical diagnosis. In many health
delivery systems there is an emphasis on
delivering services that generate revenue, rather
than on prevention and early intervention activities
that may promote behavioral health and avoid
problems in the future. Although some of the
solutions to logistical issues may be beyond the
scope of this book, the problem of finding enough
established method for handling noncompliance or time and sufficient compensation to deal
aggressiveness. Sometimes these methods are conscientiously with matters of child behavior does
appropriate, but too often such remedies are deserve prompt resolution.
generalities, such as “Don’t spank. Use time out.”
While time out is a valuable disciplinary tool, it is In brief, most of the limitations identified in this
16Child Behavioral Assessment & Management in Primary Care Second Edition
chapter emanate from their emphasis on fitting into
a system that views behavior as a categorical
entity, normal or abnormal, or in assuming that the
impact of intervention will be the same for all
children. Professional education currently
concentrates on the extremes of behavior, the
diagnostic categories of DSM disorder that the vast
majority of children do not have. Assessment tools
may help clinicians appreciate the specific
behaviors exhibited by the youngster but do not
lead to a formulation of what to do about them,
other than make a diagnosis. Behavioral programs
usually help a certain percentage of youngsters,
but may not help, or may even harm children for
whom they are not suited.
Professionals in primary care operate in an
environment where many different levels of
behavior (situational, transitory and contextual as
well as permanent) and many different techniques
(specific to the child’s problems and patterns of
reaction) may be brought to bear to assist in
dealing with caregiver concerns about behavior.
The authors’ formulation of what this environment
is and how it operates are delineated in the next
few chapters about behavioral assessment and
management.
17Child Behavioral Assessment & Management in Primary Care Second Edition
What are the Problems? A Clinician’s
Perspective on Behavioral Issues
Presented in Primary Care
Even when bringing a child to the office for a well any primary care physician, nurse, counselor, or
check or common physical problems, caregivers teacher. In fact, some allied health and education
often present additional concerns about their practitioners are able to pursue these inquiries with
children to primary care professionals. Some of equal or greater skill than many of their physician
these concerns are behavior- or development- associates.
related questions, which most well-trained
professionals are expected to be prepared to I. Behavioral Adjustment and
handle as part of their daily routine. Some are more
Maladjustment
challenging ones, which can range in severity. Of
course, most behavioral complaints are minor, as Maladjustment suggests that behavioral issues
seen from their transient and/or situational nature, tend to be severe, obvious, and easily classified
and may require only a brief investigation and into a known category of “psychiatric illness.” In
suggestions or counsel to simply watch and wait. primary care this is not usually the case, especially
Others are much more complex and these tend to when the concerns are routine rather than urgent.
require special assessment and disposition. Based The largest percentage of cases presented by
on research and clinical experience dealing with parents are issues seen in children who do not
the full range of issues that caregivers present, the meet the criteria for any psychiatric diagnosis. They
authors describe here a framework for represent behavioral dysfunctions that fall into the
conceptualizing behavioral components and mild to moderate range of severity. Some
outcomes spanning the normal range, up to and practitioners dismiss these problems on the
including the DSM disorders. presumption that they need no attention if they do
This framework suggests that there are three broad not represent a diagnosable “illness.” Those
categories of issues or conditions that are professionals who do choose to assist caregivers
presented: 1) behavioral maladjustment (including with these concerns, however, recognize that
but not limited to the DSM-V disorders), 2) aversive dealing with these problems requires that they
temperament leading to a poor “fit,” and 3) parental perform at least some assessment, and not simply
misperception or misinterpretation of normal child dispense standard advice or refer every problem
behavior due to parental inexperience or their own on to a mental health specialist. Some of the most
problems. The present chapter will describe in common behavioral problems seen in
some detail these three possible situations. It preadolescent children include such conditions as
should be stressed that this view can be utilized by mild to moderate aggression, anxiety,
18Child Behavioral Assessment & Management in Primary Care Second Edition
noncompliance, sleep problems, wetting and emotions, or function.
soiling, and problems with siblings. Before one can describe any behavior as
In considering the concept of adjustment, the focal abnormal, the clinician needs to have a clear idea
point is the content of the child’s behavior rather of what is normal. Unfortunately such a definition is
than its style, especially in relationships—or, simply hard to find. It is usually assumed to be an absence
put, what he or she actually does and why in the of abnormality, but one needs a more specific
particular environmental circumstances. Behavioral positive description. One of the few clear
adjustment may interact with, and be to some statements of behavioral adjustment to be offered
extent derived from, his or her physical and by the experts came over 25 years ago from
developmental status and temperament, but it is psychiatrist Stella Chess (personal communication,
conceptually distinct from these other aspects of 1989):
the child’s functioning. A word of caution about “As a working concept, keeping in mind its
terminology. The DSM diagnostic system (APA subjective nature, one may identify the
2013) was primarily designed by psychiatrists who
following broad characteristics of normal children:
wanted to standardize mental disorder terminology
They get along reasonably well with parents, sibs,
for the purpose of meaningful intra-professional
and friends; have few overt manifestations of
clinical communication. It does not include theories
behavior disturbance; use their apparent
of causation. Many other medical, psychological,
intellectual potential to appropriate capacity; are
educational, and social organizations in the United
interested in accomplishing developmentally
States and abroad have adopted this terminology
appropriate tasks; and are contented a reasonable
because they lack diagnostic systems of their own, proportion of the time. This description covers a
even though the scheme is not developmental, wide range of temperamental and personality
contextual, or adaptational and was not designed patterns. One should not arbitrarily consider certain
well for children. Also, the term “psychiatric children to be abnormal because their conduct is
disorders” requires further definition. It implies that identified with types of behavior that do not
the behavioral status is of such a nature and conform to an abstraction.”
severity as to require the expert services of a
Thus, she recommends thinking of positive
psychiatrist (or perhaps a skilled clinical
adjustment primarily in terms of the individual’s
psychologist). Therefore, although included in the
relationships with other people, with tasks, and with
DSM manual, the term should not be used to
oneself.
describe learning differences and disabilities,
motor skills disorders, communication disorders, The need for an adequate descriptive diagnostic
pervasive developmental disorders, cognitive scheme that is comprehensive, developmental,
deficits, aversive temperaments, attention deficits, contextual, and adaptational led us, the authors, to
enuresis, and other conditions not clearly and devise an entirely new designation of adjustment
uniquely the province of mental health starting with these criteria for children ages 4-14
professionals. DSM categories are more years. The new plan recognizes strengths as well
appropriate for major disturbances of behavior, as weaknesses. And there is a useful mnemonic
19Child Behavioral Assessment & Management in Primary Care Second Edition
that helps the user to recall the six parts: BASICS, from outstandingly good, to better than average, to
which stands for Behavior in social relationships, average, to less than average, to poor.
Achievements, Self-relations, Internal status, The BASICS Behavioral Adjustment Scale (BBAS)
Coping, and Symptoms of physical functioning. The (Carey & McDevitt, 2004) was derived from this
process involved in this construction is described in view of adjustment. This relatively new scale is
a textbook chapter by Carey (2009). Inspection of comprehensive (covering all six of these areas),
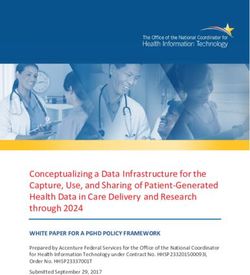
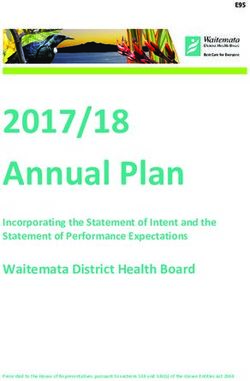
the table of definitions (Table 3-1) shows the dimensional (positive, average or intermediate, and
behaviors at the two poles of each of the six areas. negative), descriptive (of actual behavior at each
Table 3-2 demonstrates the variations within each level), and useful for clinical practice. It was
Table 3.1: The BASICS Profile of Behavioral Adjustment
Areas of Behavioral Adjustment Concerns: Behaviour, Emotions, Functions
Behavior competence in social relationships. Undersocialization- Aggression, opposition,
Skills, success, caring, cooperation, withdrawal.
involvement, reliance. Parents, sibs, peers,
teachers, other adults.
Achievements- task performance and mastery Poor achievement or failure. Excessive
in school, home, community. High or sufficient preoccupation with work or play
achievement, effort, motivation, satisfaction
Self-relations - self assurance.
Self esteem about academics, social worth, Poor self- esteem. Poor body image.
appearance, physical abilities.
Self-care, good health and safety attitudes, Self-neglect, risk taking. Overconcern for
practices, handling personal stress. oneself
Self-control or regulation- actions-feelings Over-control- inhibition or under control-impulsivity.
Internal status- feeling and thinking-. Anxiety. Depression. Thought disturbance (e.g.
Reasonable contentment. Thought clarity. obsessions)
Coping or problem solving patterns: direct and Ineffective, maladaptive problem solving with
appropriate engagement Identifies problems; excessive use of denial, avoidance or
plans solutions; works on solutions; persists at repression.
solutions; revises solutions; gets help for
solutions.
Symptoms of physical function.- Moderate to severe symptoms in eating, sleep,
Comfortable function elimination, gender, unexplained physical
complaints, repetitive behaviors.
(From Carey, 2009)
20Child Behavioral Assessment & Management in Primary Care Second Edition
standardized on a sample of more than 400 Its aim is to yield a description, not a score.
children seen in several general pediatric practices Clinicians can use these ratings as a starting point
in the greater Philadelphia area. The printed to focus further interviewing and observations.
questionnaire can be completed by a parent in Table 3-2 contains an approximation of the content
about 15 minutes and scored by a secretarial of the BBAS. It also does not lead to a score but to
helper in 2 to 4 minutes. An online version can be a description of the child.
completed in the same time and scored instantly.
The BASICS model has been proposed but not
The BBAS has good psychometric qualities of
extensively researched. However, it represents an
internal consistency, retest reliability, and
initial step forward in defining the parameters of
discriminant validity. We see its main use not for
primary screening but as an additional assessment normal behavioral adjustment, suggesting
of adjustment when the clinician has discovered gradations between happy and healthy vs.
some complex degree of parental concern about symptomatic and maladjusted. Refinement and
the child and desires an efficient way to obtain a validation of the intermediate steps is important if
broader inventory. the gap between normal and abnormal in everyday
21Child Behavioral Assessment & Management in Primary Care Second Edition
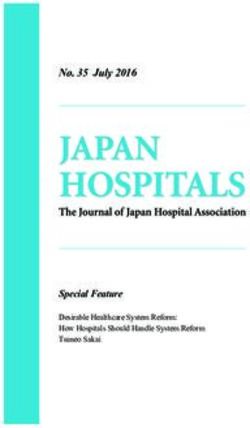
Table 3.2: Comprehensive Profile of Behavioral and Emotional Adjustment
Areas of Adjustment - Definations Ratings & Comments
Behavior, social competence- a) Highly competent, pleasant, likeable
Relationships with people: How well does b) More pleasing, likeable than average
child get along with people? c) Gets along moderately well. Average.
l High social skills vs. deficit d) Some significant relationship problems,
l Caring vs. hostile, aggressive, destructive. not major. Conflict with parents, sibs,
l Cooperation vs. opposition, defiance,
teachers or peers.
manipulation. e) Generally unpopular, often rejected.
l Involvement vs. withdrawal.
Frequent severe incidents, real or
l Autonomy vs. dependence, overconformity
threatened exclusion from relationships.
Comments:
Achievements a) Excellent achievement
Task performance- school, home, other. b) Good achievement.
How well does child do tasks and play? c) Average, satisfactory achievement.
l Extent of achievement d) Underachievement, not failing.
l Skill development, utilization.
Excessive striving
l Motivation, effort, interest, responsibility.
e) Poor achievement, failing. Truancy.
l Satisfaction, pride in accomplishment
Comments:
Self relations a) Excellent self-esteem, care and
Self-assurance and management. How regulation.
does child feel about and manage self? b) Good status in these areas.
l Self-esteem- mental and physical
c) Variable, average status
abilities, appearance, social worth.
d) Below average in some of these
l Self-care vs. neglect, abuse, risks,
matters.
overconcern
e) Poor. Problems in some or all these
l Self-regulation- appropriate vs. over or
under regulation areas.
Comments:
22Child Behavioral Assessment & Management in Primary Care Second Edition
Table 3.2 (Continued): Comprehensive Profile of Behavioral and Emotional Adjustment
Areas of Adjustment - Definations Ratings & Comments
Internal status- a) High but reasonable contentment.
General contentment vs. disturbance in b) Comfortable feelings and thinking.
feelings or thinking. How does child feel and c) Average mixture of concerns.
think? d) Unsatisfactory. Disturbing but not crippling
l Feelings- degree of comfort or discomfort.
feelings of fear, anxiety, depression, anger,
l Thinking- clarity and reality vs. distortion.
guilt; or reality distortions, phobias,
obsessions, compulsions, delusions. PTSD.
e) Poor- major disturbance of feelings or
thinking.
Comments:
Coping. a) Highly effective coping.
Problem solving. How well does child identify
b) Generally effective coping.
and solve problems?
c) Satisfactory. Average. Variable.
l Identify problems vs. denial.
l Plan solution vs. avoidance d) Unsatisfactory coping.
l Work on solution vs. passivity. e) Poor problem solving. Excessive use of
l Persist at solution vs. give up
defensive strategies---denial, giving up, etc
l Makes needed revisions vs. perseveration.
Comments:
l Seek appropriate help vs. not.
Symptoms of body function. a) Comfortable in all areas.
General comfort of body functions vs b) Generally good function. Only minimal
discomfort or dysfunction.
concern.
l Eating
l Sleeping
c) Some concern. Within normal range.
l Elimination d) Significant concern. Not severe.
l Gender e) Major concern.
l Pains
Comments:
l Repetitive behavior
General assessment
Main service needs
(From Carey, 2009)
23Child Behavioral Assessment & Management in Primary Care Second Edition
life is to be understood and utilized to promote behavioral adjustment problems do not meet the
behavioral and emotional well-being. criteria for any DSM-V disorder. Thus, the
descriptive approach to adjustment difficulties can
At what point can the term “psychopathology” be
be useful in determining the type of problem and
applied? Perhaps that is best thought of as the
indicate the direction needed for resolution.
situation when the extent of the undesirable or
Primary care professionals will nearly always refer
unacceptable behavior is so great and
most severe problems to a behavioral specialist,
internalized that it takes more than brief
though a few primary care physicians do feel
counseling for a restitution of healthy interactions
comfortable and competent in prescribing
with the environment to cause it to moderate to a
medications or counseling for common
more acceptable level. It is a behavioral variation
“psychiatric” conditions in childhood.
that is in some way harmful. The DSM-V
categories certainly define the criteria for The authors at this time present a tentative outline
psychopathology for specialty providers, such as for recognizing and rating behavioral adjustment
psychiatrists, psychologists, therapists and for children under the age of four years, a time
others. Implicitly, all psychopathology includes when “abnormal” is even harder to distinguish from
significant problems in behavioral adjustment, but acceptable, and the danger of overdiagnosis is
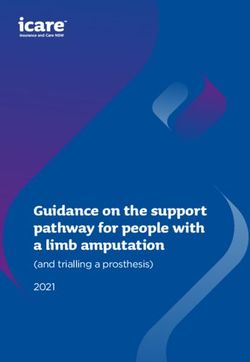
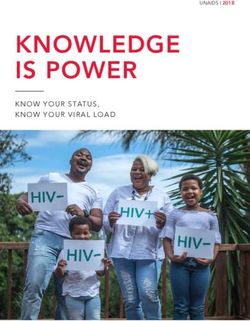
the reverse is not true. Many children with especially great. (See Table 3-3 below).
Table 3.3: BASICS Behavioral Profile- Ages 0-4 and 4-14 Years
BEHAVIORAL Concerns: 0-11 months Concerns: 12-47 months Adjustment Concerns-
ADJUSTMENT (other than “difficult” (other than “difficult” 4-14 years:
The quality of child’s temperament: especially temperament: especially behavioral, emotional,
psychosocial functioning in active, unpredictable, inflexible, active, unpredictable, functional.
BASICS areas. (not inhibited, intense, negative, inflexible, inhibited, intense,
including physical status, Inattentive/inappropriate negative, inattentive/
neurological, cognitive persistence, low soothability, inappropriate persistence,
functions or temperament.) sensitive.) distractible, sensitive.)
Behavioral competence in Deficient positive relations: Excessive negative or Undersocialization- Poor
social relationships: How attachment, closeness, insufficient positive social quality of interpersonal
well is he/she getting along reciprocal engagement, caring, adjustment: Noncompliance, relationships. Aggression,
with people? affection, smiling, enjoyment Aggression: kicks, hits, Opposition.
Skills, success, caring, from being held, eye Opposition. Tantrums. Withdrawal
cooperation, involvement, contact.Excessive negative Withdrawal. Detachment. Avoidance.
reliance. Parents, sibs, social adjustment: withdrawal, Inconsiderate of others Detachment.
peers, teachers, other adults. detachment; Clinging, excess Conduct issues- steals, lies,
crying when left alone. bullies
Achievements: How well is Inappropriate play- solo or with Insufficient achievement in Poor achievement or failure
he/she performing, others; either ignores toys, tasks at home, with others of engagement in tasks and
considering his/her abilities? stimuli or overly occupied with and at school: clean up, play -in home or school
Task engagement and repetitive activities, helping, other chores, etc. despite adequate instruction.
achievement in school, nonproductive use. Inappropriate solo or group Refusal/avoidance of
home, community. High or play: selfish, non- homework, chores, family
sufficient effort, motivation, cooperative, poor care of duties, etc.
satisfaction. toys, destructive, etc.
24Child Behavioral Assessment & Management in Primary Care Second Edition
Table 3.3: (Continued): BASICS Behavioral Profile- Ages 0-4 and 4-14 Years
Self-relations-How well
does he/she do viewing &
managing self.
--Self–esteem- about (May be hard to determine Little self-confidence. Over- Poor self- esteem. Poor
academics, social worth, this early) dependent. body image.
appearance, physical Clingy.
abilities
--Self-care- good health Inadequate self-soothing. Careless about danger. Self-neglect, risk taking.
and safety attitudes, Excessive crying when left Excessive lag in self-care- Overly concerned about
practices, handling personal alone. toilet, dressing, eating. Poor self. Preoccupied.
stress. self-soothing.
--Self-control or regulation- Failure to achieve regulation Inadequate self-control. Impulsive. Over-control- inhibition;or
of actions, feelings; “effortful of physical functions. Disruptive. Excessively inhibited under-control- impulsivity.
control” Excessive crying- colic. or detached.
Internal Status: Little expression of contentment Anxious, Fearful. Few signs of contentment.
How content or troubled with care. Absence of Phobias. Angry. Expression of discontent with
internally in feeling and regard/smiling. Excessive Depressed. surroundings
thinking? Reasonable distress: negative, crying- “colic” Obsessions. Anxiety. Depression. Fearful.
contentment. Thought Excess fear with non-primary Angry.Thought disturbance-
clarity. caregivers. obsessions, other distortions.
Coping: Hard to estimate in this Insufficient appropriate coping Ineffective, maladaptive
Problem solving patterns. How period. skills and accommodation. problem solving with
effective is he/she at solving Excessive avoidance, Excessive ineffective coping excessive use of
personal problems?
nonresponsive etc. skills: avoidance or denial, ignoring, repression,
Direct and appropriate
Frequent tantrums or crying shuts down, etc. avoidance. , etc.
engagement. Identifies problems;
plans solutions; works on when delayed or restrained. Frequent (daily or more)
solutions; persists at solutions; Shuts down or disengages tantrums when presented with
revises solutions; gets help. obstacles
Symptoms of physical Little expression of contentment Enuresis. Encopresis. Moderate to severe
function: How comfortable with body functions: eating, Constipation. symptoms or disruptions
sleep, etc.
are his/ her body functions? Sleep disorders. Self- in eating, sleep,
Apparently excessive body
discomfort, malfunction stimulation -rocking, twirling. elimination, gender.
symptoms: night waking, food Gender confusion. Unexplained pains.
rejections. Food fads. Pica. Repetitive behaviors
WBC 11/27/13 Revised SMcD 9/21/15
25Child Behavioral Assessment & Management in Primary Care Second Edition
The DC: 0-3R Manual (2005) offers suggestions for could be an aversive, normal temperament or a
some categorical labels for use up to age four years caregiver misperception of abnormality due to
but tends to pathologize some normal behavioral either insufficient information or caregiver
patterns. For disruptive behaviors Wakschlag et al. psychosocial problems distorting their view of the
(2007) have proposed a still-undeveloped system child.
focusing on noncompliance, temper loss, and
aggression. To these symptoms can be added some Aversive Temperament
other worrisome ones such as lack of personal
feeling for people. The DSM-PC (DSM for Primary Stresses from dissonant reactions between a child’s
Care, Child and Adolescent Version) of the American normal temperament
Academy of Pediatrics (1996) was an extensive but and the values and
unsuccessful attempt to adjust the DSM scheme to expectations of the
the primary care medical setting. parents or other
caregivers are a
Not discussed here are screening techniques for major source of
detecting autism, ADHD, or other syndromes, which caregivers’
are controversial and not generally recommended. complaints to
In particular, the criteria for ADHD are greatly in clinicians, but these
need of refinement (Carey, 2002) and are presently situations are
in a slow stage of reappraisal and revision (Furman, commonly not
2005; Thapar & Lewis, 2009). The problem of the recognized for what
overlap of ADHD symptoms with normal they are. The extensive descriptions of temperament in
temperament traits has yet to be adequately clinical settings available in other sources (Carey, 2009,
resolved (Foley, McClowry, Castellanos, 2008). It 2011a; Carey & McDevitt, 1995; Chess & Thomas, 1986,
seems likely that the present overdiagnosis of ADHD 1999; Thomas & Chess, 1977; Thomas, Chess, Birch
may in part be due to the lack of recognition by many Hertzig & Korn, 1968) should make necessary only a brief
clinicians of temperament variations which are summary here.
annoying to caregivers but still inherently normal.
Detecting and managing autism is not a primary The best simple definition of temperament is the behavioral
concern of this book but the responsible clinician style of the individual, the characteristic pattern of
should be screening for it when it is suspected by experiencing and reacting to the external and internal
using informed clinical observations and approved environment. It is the ”how” of behavior rather than the
questionnaires (http://www.cdc.gov/ncbddd/autism/). “what” or “why.” Because at least for young children we
cannot know for sure what they are feeling, we rate the
behavior observed by the caregivers when doing the
II. When No Behavioral evaluations rather than guessing what the child is feeling.
Dysfunction Is Detected At first, clinicians sometimes have a problem distinguishing
If there is parental or other caregiver concern and between temperament and behavioral adjustment.
the criteria for behavioral dysfunction have not Temperament is the normal, early-appearing, largely
been met, then evaluation of the child’s status genetically determined, somewhat stable set of stylistic
shifts to the possibility that the source of the worry differences in reactions to the environment. Behavioral
26You can also read