Nierenersatztherapie beim akuten Nierenversagen - Univ.- Prof. Dr. Michael Joannidis - Nephrologisches Seminar Heidelberg
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Nierenersatztherapie beim akuten Nierenversagen
Univ.- Prof. Dr. Michael Joannidis
Internistische Intensiv- und Notfallmedizin
Department Innere Medizin
Medizinische Universität Innsbruck
Potentielle Interessenskonflikte Sprecher Konsulent • Fresenius • Baxter • Baxter • Fresenius • Braun • Sandoz • CLS Behring • AmPharma

Inhalt Update NET auf der Intensivstation: 1. Epidemiologie 2. „Optimaler“ Beginn der Nierenersatztherapie 3. Behandlungsdosis 4. Antikoagulation
1032 ICU patients out of 1802 had AKI [57.3%; 95% CI 55.0-59.6]
25% of AKI patients required RRT
Maximum AKI stages
600
30 %
500
400
18,4%
300
AKI RRT 15%
200 8,9%
100
0
AKI stage 1 AKI stage 2 AKI stage 3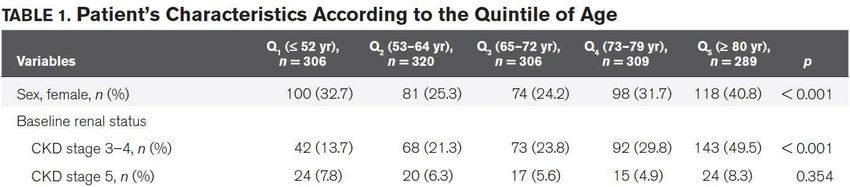
Etiology
Ravindra L Mehta et al, Lancet 2015
A worldwide multicentre evaluation of the influence of deterioration or improvement of acute kidney
injury on clinical outcome in critically ill patients with and without sepsis at ICU admission: results from
The Intensive Care Over Nations audit.
N=7970 Sepsis No sepsis
(N=1946) (n=6024)
AKI 68% 57%
AKI stage 3 40% 24%
RRT 20% 5%
Improvement to AKI
Mortality of AKI-RRT
Trial N †
Metnitz 2002 17.126 62.8%
BEST KIDNEY 2005 29.269 60.3%
ATN 2008 1.124 53.6%
RENAL 2009 1.508 44.7%
Multi-centre
AKIKI 2016 620 48.5% RCTs
(n>400)
IDEAL-ICU 2018 488 56.0%
STARRT-AKI 2020 2927 43.8%
Metnitz PGH et al. Crit Care Med 2002
Uchino S et al. JAMA 2005
RENAL, N Engl J Med 2009;361:1627-1638
VA/NIH ATN, N Engl J Med 2008;359:7-20
Gaudry S et al. N Engl J Med 2016;375:122-133
Barbar SD et al., N Engl J Med 2016;379:1431-42
STARRT-AKI Investigators. N Engl J Med 2020;383:240-251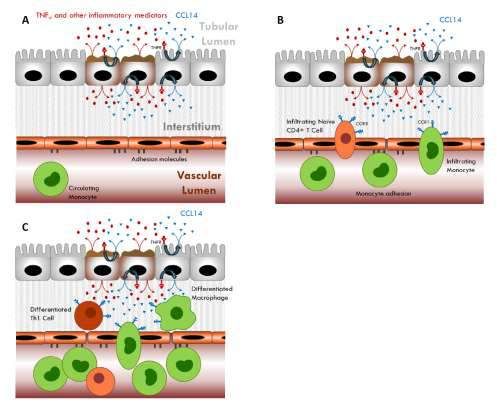
ICU Patients Requiring Renal Replacement
Therapy Initiation: Fewer Survivors and More
Dialysis Dependents From 80 Years Old
Prospektiv gesammelte Daten von 1,530 (2 französische Intensivstationen)
Outcome-Analyse kohortiert nach Alter (Quintile), 289 Patienten > 80 Jahre
Commereuc M et al, Crit Care Med. 2017 Aug;45(8):e772-e781
Der „optimale“ Beginn mit der
Nierenersatztherapie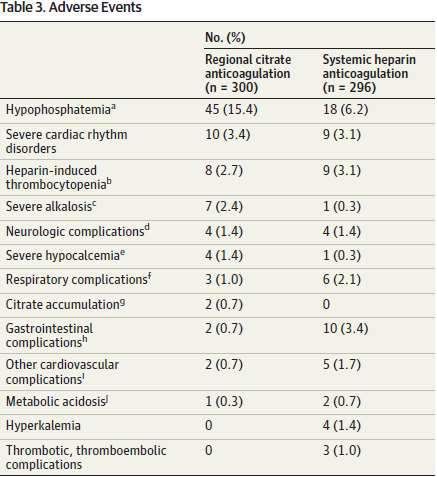
Effect of Early vs Delayed Initiation of Renal
Initiation Strategies for Renal-Replacement Timing of Renal-Replacement Therapy in
Replacement Therapy on Mortality in
Therapy in the Intensive Care Unit Patients with Acute Kidney Injury and
Critically Ill Patients With Acute Kidney
(AKIKI trial) Sepsis (IDEAL-ICU)
Injury: The ELAIN Randomized Clinical Trial
KDIGO 3 vs. absolute criteria RIFLE F vs. RIFLE F + 48h max
KDIGO 2 vs. KDIGO 3
49% (AKIKI) and 38% (IDEAL-ICU) did
not require RRT in the delayed arm
17% emergent indications in
the delayed arm
Zarbock A et al, JAMA. 2016;315(20):2190-2199 Gaudry S et al. N Engl J Med 2016;375:122-133 Barbar SD et al. N Engl J Med 2018;379:1431-1442
Single Centre Multicentre Multicentre
N= 231 N= 619 N= 488
95% surgical 80% medical/(75% Sepsis) 100% early septic shock
100% CVVHDF 55% IHD (!) 55% IHD (!)
Time difference: 21.5h Time difference: 57h Time difference: 44h
Fragility index = 3 Terminated for futilityTiming of Renal-Replacement Therapy in Patients with Acute Kidney
Injury and Sepsis (IDEAL-ICU)
Early Delayed
Patients who received RRT — no. (%) 239 (97%) 149 (62%)Timing of Initiation of Renal-Replacement Therapy in Acute
Kidney Injury (STARRT-AKI trial)
Randomised controlled trial
15 countries, 168 centres, 3019 patients
~ KDIGO 2
Accelerated strategy: Standard strategy:
RRT < 12 hours after RRT discouraged unless
meeting eligibilty criteria • K>6 mmol/l,
• pH < 7.2
• HCO3 < 12 mmol/l
• paO2/FiO2 < 200
• volume overload
• persistent AKI > 72h
Primary outcome: all cause mortality at 90 days
The STARRT-AKI Investigators. N Engl J Med 2020;383:240-251.Timing of Initiation of Renal-Replacement Therapy in Acute
Kidney Injury (STARRT-AKI trial)
Patient characteristics:
CKD 44% (1284)
Surgical patients 33% ( 965)
Medical patients 67% (1962)
Sepsis 58% (1689)
Septic shock 44% (1284)
Modality:
CRRT 70% (1590)
IHD 26% (606)
SLED 4% (101)
The STARRT-AKI Investigators. N Engl J Med 2020;383:240-251.Timing of Initiation of Renal-Replacement Therapy in Acute
Kidney Injury (STARRT-AKI trial)
Kaplan–Meier Estimates of Survival at 90 Days Subgroup Analyses
Time from eligibility to RRT Initiation 6.1h (IQR 3.9-8.6) vs. 31.1h (IQR 19.0-71.8). Median time difference 25h.
The STARRT-AKI Investigators. N Engl J Med 2020;383:240-251.Timing of Initiation of Renal-Replacement Therapy in Acute
Kidney Injury (STARRT-AKI trial)
96.8%
61.8%
Adverse events occurred in 346 of 1503 patients (23.0%) in the accelerated-strategy group and in 245 of 1489 patients
(16.5%) in the standard strategy group (risk ratio, 1.40; 95% CI, 1.21 to 1.62; PHypothesis: early renal replacement therapy increases mortality
in critically ill patients with acute on chronic renal failure.
A post hoc analysis of the AKIKI trial
60 of 619 with CKD (GFR 30-60 ml/min)
Gaudry S et al, Intensive Care Med (2018) 44:1360–1361Overview on timing studies in critically ill patients
ELAIN AKIKI IDEAL ICU STARRT-AKI
Number of centres 1 (Germany) 31 (France) 29 (France) 168 (15 countries)
Number of patients 231 620 488 3019
AKI Stage 2 AKI stage 3
AKI stage 3
Main inclusion criteria + ↑ NGAL + sepsis, vasopressors, + mechanical ventilation and/or AKI Stage 2 and clinical equipoise
+ early septic shock
fluid overload or ↑ SOFA vasopressors
Criteria for early RRT initiation 8 hr of AKI stage 2 6 hr of AKI stage 3 12 hr of RIFLE Failure 12 hrs of AKI stage 2
Criteria for delayed RRT initiation 12 hr of AKI stage 3 AKI complications Absolute indication Absolute indication
Mean SOFA score at RRT initiation 15.8 +/- 2.3 10.8 +/- 3.2 12 +/- 3 11.7 +/- 3.6
Cumulative fluid balance at
~ +6.5L N/A + 3.2L +2.7L
randomization
Proportion of patients in delayed arm
91% 71% 51% 61.8%
who received RRT
IHD 56% CRRT 56% CRRT 68%
Initial modality CVVHDF 100%
CRRT 44% IHD 44% IHD 26%
Primary outcome (early vs. delayed 90-day mortality 60-day mortality 90-day mortality 90-day mortality
initiation) 39.3% vs. 54.7% 48.5% vs. 49.7% 58% vs. 54% 43.9% vs. 43.6%
RRT associated complications (early overall no difference overall no difference Metabolic acidosis (9% vs 17%) 23.0% vs. 16.5%
versus delayed initiation) (hypocalcaemia 66.9% vs. 75.7%) (hypophosphatemia 22% vs. 15%) Hyperkalemia (0% vs. 10%) (hypotension, hypophosphatemia)Kriterien für den Beginn der Nierenersatztherapie
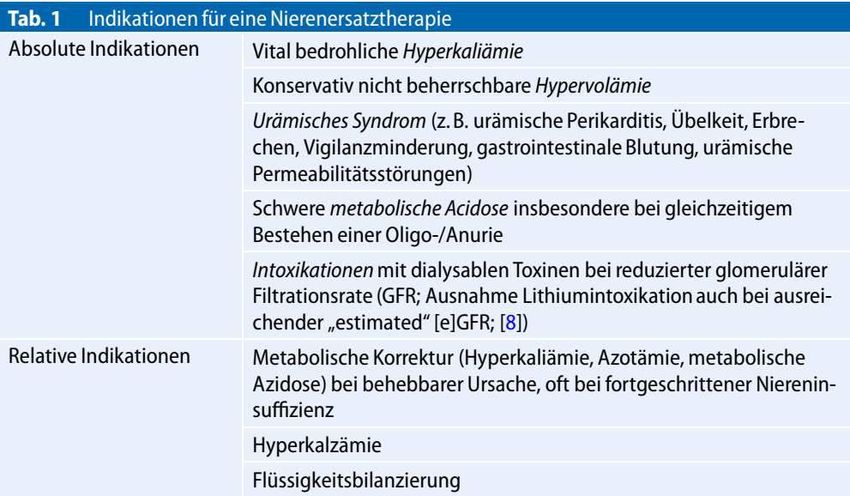
• Notwendigkeit für eine Nierenersatztherapie (NET) kann nicht
anhand eines einzelnen Parameters festgelegt werden.
• Die absolute Indikationsstellung anhand der Kriterien schwere
Hyperkaliämie, Azidose, Urämie und Hypervolämie ist für
kritisch kranke Patienten nicht ausreichend.
• Zu beachten ist die Diskrepanz zwischen Beeinträchtigung
der exkretorischen Kapazität der Niere und der Belastung
durch Komorbiditäten, Schweregrad der Akuterkrankung und
der Flüssigkeitsüberladung (kumulative Flüssigkeitsbilanz)
• Die Rolle von Biomarkern der Nierenschädigung oder
Furosemid Stress-Test für die Indikationsstellung einer NET
ist noch zu evaluieren.
• Die Entscheidung zum Beginn einer NET muss immer auch das
zu erwartende Outcome berücksichtigen
• Die Indikationsstellung hat somit auf individualisierter Basis
zu erfolgen
Schwenger et al, Med Klin Intensivmed Notfmed 2018 · 113:370–376Was spricht gegen eine „wait and watch“
Strategie?Sodium bicarbonate therapy for patients with severe metabolic acidaemia in the intensive care
unit (BICAR-ICU): a multicentre, open-label, randomised controlled, phase 3 trial
26 French ICUs, 389 patients w. metabolic acidosis, (ph < 7. 2, s-bicarb. < 20 mmol/l)
4.2% sodium bicarbonate to achieve pH >7.3, 125 -250 ml/30 min, max 1L/d vs. no sodium bicarbonate
Cumulative fluid balance within first 24h: 3500 ml (co) vs. 3350 ml (Nabic), p=0.835
Average amount of NaBic within first 24: 500 ml (250-750)
Overall cohort AKI stages 2-3 (pre-specified)
Saber J. et al, Lancet 2018; 392: 31–40Fluid Overload Associates With Major Adverse Kidney Events in Critically Ill Patients
With Acute Kidney Injury Requiring Continuous Renal Replacement Therapy
Woodward C et al, Critical Care Medicine47(9):e753-e760, September 2019Können uns “neue” Biomarker bei der
Entscheidung weiterhelfen?Biomarkers predicting RRT in AKI?
(systematic review and meta-analysis)
63 studies comprising 15,928 critically ill patients (median per study 122.5 [31–1439]) met eligibility.
41 studies evaluating 13 different biomarkers included
Blood/serum/plasma Number Number of RRT AUC 95% CI
biomarker of patients
studies
Cystatin C 7 1079 18% 0.768 0.729–0.807
Creatinine 15 2969 9% 0.764 0.732–0.796
NGAL 22 4391 8.9% 0.755 0.706–0.803
Urinary biomarker Number Number of RRT AUC 95% CI
of patients
studies
TIMP-2 × IGFBP-7 4 280 5.2% 0.857 0.789–0.925
Cystatin C (normalised) 4 1232 8.9% 0.790 0.645–0.934
NGAL 12 3412 10.4% 0.727 0.678–0.776
Urinary Output 2 604 50% 0.614 0.389–0.840
Klein S et al, Intensive Care Med (2018) 44:323–336Cell Cycle Biomarkers and Soluble Urokinase-Type Plasminogen Activator
Receptor for the Prediction of Sepsis-Induced Acute Kidney Injury Requiring
Renal Replacement Therapy: A Prospective, Exploratory Study
100 critically ill patients with positive Sepsis-3 criteria, 2 ICUs, 19 patients required RRT
Nusshag C et al, Crit Care Med 2019; 47:e999–e1007Can we detect persistent AKI?
Prediction of persistent AKI stage 3
• ICU patients enrolled with 36h of AKI stage 2+
• Primary outcome
• AKI stage 3 of >72h
• dialysis
• death following KDIGO stage 3 AKI
E. Hoste et al, Intensive Care Med (2020) 46:943–953Urinary C-C motif chemokine ligand 14 (CCL14)
• CCL14 is a member of the chemokine family of C-C motif chemokine ligand 14 (CCL14)
small molecules that were initially recognized for and renal fibrosis
roles in leukocyte chemotaxis and are implicated
in tissue injury and repair processes
• CCL14 binds with high affinity to the chemokine
receptors
• CCL14 has been shown to be an important
chemokine for monocyte/macrophage
recruitment and is associated with pro-
inflammatory chemotaxis in a variety of diseases
including rheumatoid arthritis, multiple sclerosis,
and lupusPatients with Persistent Stage 3 AKI Had Worse Outcomes
Log rank test; Persistence must start within 48 hours of enrollment;
93 (28%) of patients received RRT within 90 days
90-Day Mortality Major Adverse Kidney Events (MAKE)
90%
90%
80% pEarly versus standard initiation of renal replacement therapy in furosemide stress test non-responsive
acute kidney injury patients
(the FST trial)
FST non resp
Early FST non resp FST resp
98% RRT Standard 14% RRT
75% RRT
Lumlertgul et al. Critical Care (2018) 22:101Furosemide stress test as a predictive marker of acute kidney
injury progression or renal replacement therapy: a systemic
review and meta-analysis
11 trials / 1366 patients:
AKI stage progression reported in 517 patients, renal replacement therapy reported in1017 patients
Chen et al. Critical Care (2020) 24:202Proposed algorithm for initiation renal replacement
therapy (RRT) in critically ill patients with acute kidney
injury (AKI).
Biomarkers ?
Furosemide stress test ?
Bicarbonate administration
Bagshaw S & Wald R.
Kidney International (2017) 91, 1022–1032Nierenersatztherapie - Dosis • Empfohlene Mindestdosis (nach KDIGO 2012): CRRT: 20–25 ml/kg/h IHD: Kt/V 1.3, wöchentliches Kt/V 3.9 • Initiale Dosis zur Kompensation von Stehzeiten etc. gegebenenfalls höher ansetzen (25-30 ml/kg/h) • Anpassung der Dosis an die individuelle Situation (Metabolismus, Harnstoffwerte). Kidney Int 2012, Suppl. 2012, 2: 1-138 Bagshaw S et al, Blood Purif. 2016 Schwenger V. et al, Med Klin Intensivmed Notfmed 2018, 113:370–376
Renal replacement therapy intensity for acute kidney injury and recovery to dialysis
independence: a systematic review and individual patient data meta-analysis
Probability of being RRT dependent
High Intensity
Standard Intensity
Y. Wang et al, Nephrol Dial Transplant (2017) 1–8KDIGO
CHAPTER 5.3: Anticoagulation
Systemic anticoagulation RRT:
required /coagulation disorder no anticoagulation
Not increased bleeding IHD: heparins (1C)
risk
CRRT: citrate>heparins (2B)
Increased bleeding IHD: no AC
risk
CRRT: citrate (2C)
HIT Direct thrombin inhibitors>F-X inhibitors (1A/2C)
Kidney Int 2012, Suppl. 2012, 2: 1-138Regionale Zitratantikoagulation
Gattas et al. trial CASH trial Stucker et al. trial RICH trial
212 patients 139 patients 103 patients 596 patients
Device: 5 Prismaflex (CVVHDF) Device: Dirinco (CVVH) Device: Prismaflex(CVVHDF) Device: CRRT (various)
2 Aquarius
Solutions : Prismocitrate 10/2 Solutions : HFCitPre Solutions : Prismocitrate 18/2 Solutions : various
Hemosol HF32bic Prsimocal B22
Primasol
Heparin-Protamine / Citrate Heparin / Citrate Heparin / Citrate Heparin / Citrate
Citrate
Citrate Citrate
Citrate
Heparin
Heparin Heparin
Heparin
39 h vs 23 h 46 h vs 32 h 49 h vs 23 h 45 h vs 33 h
Gattas et al. Critical Care Med 2015, 43:1622–1629 Schilder et al. Critical Care 2014, 18:472 Strucker et al. Critical Care 2015, 19:91 Zarbock et al JAMA 2020, 324:1629Effect of Regional Citrate Anticoagulation vs Systemic Heparin Anticoagulation During
Continuous Kidney Replacement Therapy on Dialysis Filter Life Span and Mortality Among
Critically Ill Patients With Acute Kidney Injury (RICH) - A Randomized Clinical Trial
A parallel-group, randomized multicenter clinical trial in 26 centers across Germany (March 2016 and December 2018),
terminated early after 596 patients. Coprimary outcomes were filter life span and 90-day mortality
90 day overall mortality Secondary Outcomes
Zarbock A et al, JAMA. 2020;324(16):1629-1639Effect of Regional Citrate Anticoagulation vs Systemic Heparin Anticoagulation During
Continuous Kidney Replacement Therapy on Dialysis Filter Life Span and Mortality Among
Critically Ill Patients With Acute Kidney Injury A Randomized Clinical Trial
Filter lifespan (adjusted for the factors anticoagulation strategy, study
center, cardio-vascular SOFA score, presence or absence of oliguria, sex,
pre/post amendment 1, CKRT modality)
Zarbock A et al, JAMA. 2020;324(16):1629-1639NET beim akuten Nierenversagen 2021
Zusammenfassung
• Eine NET ist in 5-20% der Intensivpatienten erforderlich, die Sterblichkeit
liegt immer noch um 40-60%.
• Indikationsstellung hat sich von früh auf abwartend verändert.
• Zu frühe NET führt zu unnotwendiger Therapie mit vermehrten
Nebenwirkung und beeinträchtigt die Erholung Nierenfunktion.
• „Neue Biomarker“ für AKI bislang wenig hilfreich für Indikationsstellung.
Biomarker für persistente AKI vielversprechend. Funktionelle Tests
(Furosemid-Stresstest) möglicherweise am aussagkräftigsten
• Dosis unverändert 25-30 ml/kg/h, mit individueller Anpassung an
metabolischen Bedarf
• Bevorzugte Antikoagulation bei CRRT ist die regionale Zitratantikoagulation
(überlegenene Filterlaufzeit und verringerte Blutungskomplikationen)Michael.joanndis@i-med.ac.at
You can also read

















































