New Therapeutic Strategies in the Management of Systemic Lupus Erythematosus 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
New Therapeutic Strategies in the Management of Systemic Lupus Erythematosus – 2021
Diagnosis Classification vs. Diagnostic Criteria
New EULAR/ACR SLE Classification Criteria Criteria and weighting • 23 international SLE centers Patients classified as SLE if ANA ≥1:80 and have ≥10 points • Diagnoses verified for 1193 SLE and 1059 non-SLE patients Manifestation Points Points Points Class 3/4 Class 2/5 Proteinuria – Derivation cohort: 500 random SLE Renal nephritis 10 nephritis 8 ≥0.5 g/d 4 and non-SLE patients Anti-Sm or Specific antibodies 6 – – – – – Validation cohort: rest of SLE Anti-dsDNA and non-SLE patients Alopecia or Mucocutaneous ACLE 6 SCLE or DLE 4 2 oral ulcers ACR SLICC New criteria Serosa Pericarditis 6 Effusion 5 – – Derivation Musculoskeletal Arthritis 6 – – – – Sensitivity 85 97 98 CNS Seizures 5 Psychosis 3 Delirium 2 Specificity 95 90 96 Blood AIHA/ATP 4 Leukopenia 3 – – Validation Complement Low C3 and C4 4 Low C3 or C4 3 – – Sensitivity 83 97 96 Antiphospholipid Abs Any one 2 – – – – Specificity 93 84 93 Constitutional Fever 2 – – – – • New SLE classification criteria have better sensitivity and specificity than previous criteria AIHA/ATP, autoimmune hemolytic anemia/thrombocytopenia; A/SCLE, acute/subacute cutaneous lupus; DLE, discoid lupus; anti-Sm, anti-Smith. Aringer M et al. ARD. 2019;0:1151–1159. doi:10.1136/annrheumdis-2018-214819; ibid: A+R. 2019;1–13 DOI 10.1002/art.40930.
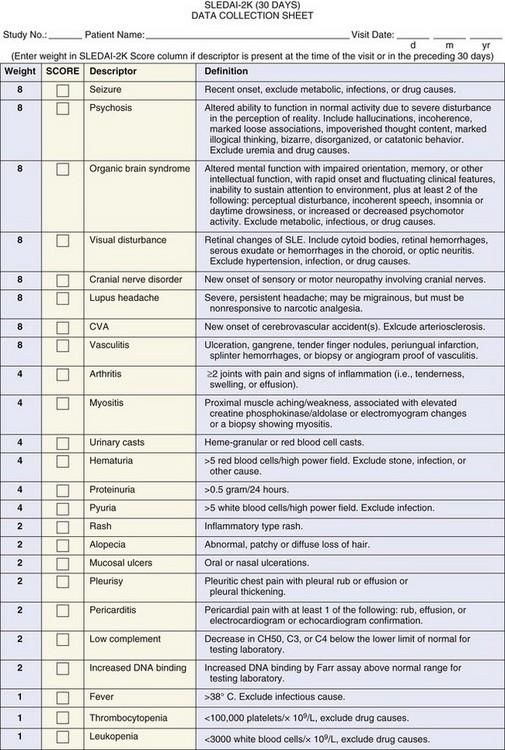
Disease Activity: SLEDAI-2K • Components – Clinical: 16 – Laboratory: 8 • Scores – Score range: 0-105 – Activity • Score ≥ 6 = active needing Rx • Score ≥ 12 = highly active • Score ≥ 20 is rare – Change • Increase ≥ 4: meaningful worsening • Decrease ≥ 4: meaningful improvement – Modifications • S2K-RI50: scores partial, ≥ 50% improvement2 • SLEDAI-2KG: accounts for GC use3 1. Gladman DD et al. J Rheum. 2002; 29:288; 2. Touma Z et al. Rheum. 2012; doi:10.1093/rheumatology/kes146; 3. Touma Z et al. Rheum. 2018;57:1370-1376.
Prognosis Morbidity (Damage) vs. Mortality
Prognosis • Overall mortality • Hospitalizations – 5 Yrs: 95% – 20-25% hospitalized annually – 10 Yrs: 89-93% • Causes of death – 15 Yrs: 76-82% – Infection: 25% – 2-3x ↑ over age-matched population – Active SLE (first 1-5 yrs): 35% • Poor prognostic factors – Cardiovascular Disease (after 5 yrs): – Af-Am race; males 30-40% – Malignancy: 5-10% – Age of onset 50 years – Disease manifestations • Renal/ESRD, CNS, GI • Vasculitis, cardiopulmonary Fors Nieves CR et al. Curr Rheumatol Rep. 2016; 18:21; Tektonidou MG et al. ARD. 2017; Garris C et al. J Med Econ. 2013; 16:667
Comorbidities • Overall: fatigue, depression, underemployment • Premature atherosclerosis: overall CV events 12x RR compared with general population – SLE CV risk is 2x calculated Framingham risk score; MI: 2.5x RR; CHF: 3.24x RR – CVA: 2.53x RR; PAD: 9.0x RR • Renal: ESRD in up to 30% (HR 44x) who develop lupus nephritis • Neurologic deficits – CVA; Migraine; “Lupus headache” – Dementia: especially in patients with APS and/or prior NPSLE • Disfiguring skin lesions • Medication adverse effects: AVN, osteoporotic fxs, infection, malignancy, infertility, obesity • Malignancy – Viral (HPV)-related malignancy (SIR 5) – Hematologic malignancies (SIR 2.75); Lymphoma increased 5x (SIR 3.64) • Pregnancy comorbidities: 20% have adverse outcomes (fetal death, IUGR, prematurity) Dregan A et al. Heart. 2017; O’Sullivan M et al. Best Prac Res Clin Rheumatol. 2016; 30:81; Lin Y-R et al. AC&R. 2016; 68:1774; Buyon JP et al. AIM. 2015; 163:153.
Predictors of Organ Damage • Hopkins Lupus cohort: – 2054 SLE patients (92% female, 56% white, 37% AA) – SLICC/ACR Damage Index score increased at a rate of 0.13/year Petri M. Arthritis Rheum. 2012;64(12):4021-8.
Predictors of Organ Damage • Hopkins Lupus cohort: – 2054 SLE patients (92% female, 56% white, 37% AA) Petri M. Arthritis Rheum. 2012;64(12):4021-8.
Mortality in SLE • Lumina cohort: – Age (p=0.0041), disease activity score (p
Predictors of Organ Damage and Death • Hopkins Lupus Cohort, published 2021 – 1168 patients w/ ≥24 mos Follow-up; assessed quarterly by SELENA SLEDAI and SDI – Background: 12 month period after entry; Observation: 2nd 12 mos: Longer Term F/U; until damage, death or end of data; AUC/time interval for SLEDAI and SDI in pts w/ SDI=0 BL • Median 7 years F/U: 39% accrued new damage (CV: 7%;renal: 3%); 8% died • Each 1 unit increase adjusted mean SLEDAI score during 12 mo observation period assoc w/: [multivariable analysis] – Death HR 1.22 (1.13 to 1.32) * * p7.5 mg QD: Death HR 1.54 (0.88-2.71); damage: HR 1.85 (1.40-2.44) * ⎻ NSAID use: CV damage: HR 1.66 (1.04-2.63) * Petri M. Lupus S&M 2021: 8:e000446. doi:10.1136/lupus-2020-000446
Treatment Evidence-Based vs. Eminence-Based
Goals of Treatment: T2T With the Least Immunosuppression Remission Low disease activity (LLDAS) • Can be on antimalarials • Can be on antimalarials • SLEDAI-2K = 0 on no prednisone or • Clinical SLEDAI-2K ≤4 with no major organ immunosuppressive (7%) involvement, +/- active serology on prednisone ≤7.5 mg/d and • Clinical SLEDAI-2K = 0, +/- active immunosuppressives serology on prednisone (1-5 mg/day) and immunosuppressives (30%) • If LLDAS maintained 50% of time, damage accrual reduced 50% • If remission maintained for 2 years, damage accrual reduced • If LLDAS maintained for 2 yrs, damage accrual reduced >70% • Median time of most remissions: 3 months ARD. 2017. 76:547; ARD. 2017. 76:562
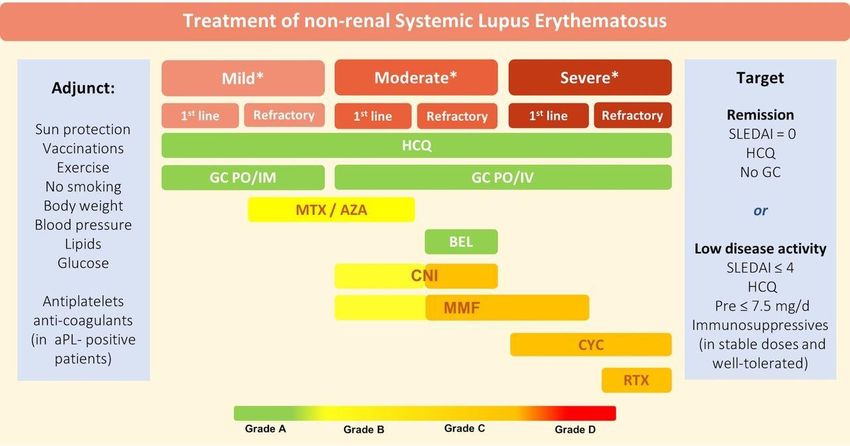
Mild: constitutional symptoms/mild arthritis/rash ≤9% BSA/PLTs 50-100 x 103/mm3; SLEDAI≤6; BILAG C or ≤1 BILAG B manifestation. Moderate: RA-like arthritis/rash 9-18% BSA/cutaneous vasculitis ≤18% BSA; PLTs 20-50x103/mm3/serositis; SLEDAI 7-12; ≥2 BILAG B manifestations. Severe: major organ threatening disease (nephritis, cerebritis, myelitis, pneumonitis, mesenteric vasculitis; thrombocytopenia with platelets 12; ≥1 BILAG A manifestations. Fanouriakis A et al. ARD. 2019;78:736-45.
Definitions of Low Disease Activity/Remission • Post hoc analysis of HDA patients receiving Correlation of disease activity measures, Atacicept in ADDRESS II RCT Week 48 (LTE; n=158)* • SRI-6: improved SELENA-SLEDAI ≥6 points, no new flares by BILAG, no worsening in PtGA SRI-6 52.5% • LDA: clinical SLEDAI-2K ≤2; no meds other than antimalarials 1 LDA (n=83) 26.6% • LLDAS: SLEDAI-2K ≤4 without major organ activity, (n=42) LLDAS no new disease activity vs previous visit, MDGA ≤1, 19% prednisone equivalent ≤7.5 mg QD, and stable immunosuppressants 2,3 (n=30) Confirmed in Anifrolumab and IFN kinoid Ph 2 RCTs 4,5 • Remission: clinical SLEDAI-2K = 0, MDGA
FDA Approved Therapies for Treatment of SLE • Glucocorticoids • Hydroxychloroquine • Belimumab, now for LN • Voclosporin Under FDA Review: • Anifrolumab www.fda.gov.
Medications • Glucocorticoids – Dosing: pulse (1 gram QD) in exceptional cases, high-dose (>30 mg QD), lower doses for non-life threatening manifestations; goal: ≤7.5 mg QD – Doses > 5-7.5 mg QD associated with organ damage (HR 1.7); >10 mg QD with CVD – Avascular necrosis increased (10-40%) in SLE pts: active disease, APS, Cushingoid appearance, obesity; mean daily GC doses / cumulative doses are risk factors – Osteoporotic fractures can occur with relatively normal T scores – PJP prophylaxis if on prednisone >15-20mg QD: SMX-TMP; as well as dapsone, atovaquone, inhaled pentamidine Gatto M et al. Nat Rev Rheum. 2019;15:30.
Pneumocystis Jiroveci Pneumonia (PJP) Prophylaxis Pneumocystis occurs in ~10% of vasculitis/SLE patients on prednisone + another immunosuppressive and prophylaxis should be administered • Prophylaxis if prednisone >15-20mg QD • Additional risk factors: ≥4 weeks – Elderly • Recommendations for stopping prophylaxis: – If no additional risk factors, stop prophylaxis – Underlying lung disease (esp. GPA, MMF/MPA, after 3 weeks IF prednisone ≤15mg QD DM/antisynthetase syndrome, DAH) – If ≥ 2 additional risk factors; continue PJP – Initial prednisone dose >60mg QD prophylaxis even w/ prednisone
Medications • Hydroxychloroquine (HCQ) – Anchor drug for all SLE pts; reduces/prevents flares; improves long term outcomes – Increases survival, decreases renal damage, safe during pregnancy: decreases neonatal Lupus; reduces recurrance congenital heart block 1; favorable lipid/glucose lowering effects; prevention thrombotic events – ACR, AAD, RDS, and AAO 2020 Joint Statement on HCQ Use with respect to retinal toxicity: Dose: ≤5 mg/kg actual BW 2; Risk of retinal toxicity 60 yrs, male, Hx renal ds, concomitant retinal ds, tamoxifen use, HCQ use >15 yrs. – Following baseline exam, annual screening should begin after 5 years of use 2 Optical coherence tomography (OCT) is optimum test for yearly monitoring. Need retinal expert interpretations; tests frequently abnormal due to other causes. – Risk of cardiomyopathy 3 (esp if renal insufficiency) Other adverse effects: dizziness, headaches, nausea; may be ameliorated by splitting dose – Utility of measuring drug levels (therapeutic >500 ng/ml) 4 – Can combine HCQ with quinacrine for refractory skin ds without increased risk of retinopathy. 1. Izmirly P et al: JACC 2020: 76:292-302; 2. Rosenbaum JT et al: A+R 2021: doi:10.1002/ART.41683; 3. Tselios K et al: J Rheumatol 2019;46;391-396; 4. Petri MA et al A+R 2019; doi: 10.1002/ART.41121; 5. Gatto M et al. Nat Rev Rheum. 2019;15:30
Monitoring Hydroxychloroquine Retinal Toxicity Following baseline exam, annual screening should begin after 5 years of use. Screening should include dilated eye examination, an automated white target 10-2 visual field and OCT. Screening tests should examine beyond the macula in Asian patients. A. Fundus photographs B. Fundus autofluorescence C. Fluorescein angiography D. Optical coherence tomography (OCT) Rosenbaum JT et al. A+R. 2016; 68:1805-9; letter to Editor. A+R. 2019; DOI: 10.1002/art.39703.
Belimumab • Approved by FDA 3/8/11 to reduce disease activity in adult SLE patients with autoAb positive active SLE receiving standard of care therapy; RCTs for FDA approval did not include severe active LN or CNS lupus • Human IgG1 Ab binds to soluble B-lymphocyte stimulator (BLyS) important in B cell survival • Most effective in serologically active SLE pts w/ hypocomplementemia; Reduces flares and steroid-sparing • Subgroup analysis: African Americans had lower responses – Not evident in Phase 2 RCT – Not confirmed in subsequent trials (Lupus Sci Med. 3:e000118, 2016) or recent LN RCT • No increase in SAEs compared with PBO; 2 cases of PML subsequently reported • SQ belimumab 200mg q week equally effective as 10 mg/kg IV weeks 0, 2, 4, then q 4weeks • Ph 3 104-wk RCT in LN positive: BEL+SOC vs PBO+SOC: 1◦ efficacy renal response: 1.3x RR w/ BEL – Again most effective w/ background MMF vs CTX -> AZA • Average price for therapy: $42,000/year • Pregnancy category C Lancet. 2011; 377:721-31; A+R. 2009; 61:1168-78; Gatto M et al. Nat Rev Rheum. 2019;15:30; Furie R et al. NEJM. 2020; 383:1117-28.
Greater Benefit in SLE Patients With High Serological Activity in BLISS RCTs Placebo plus SOC Belimumab 10 mg/kg 100 * * p
Early Clinical Responses in BLISS RCTs: SRI-4 Responses Over 52 Weeks Pooled BLISS-52 and -76 data 1,2 60 Responders (%) + + # + # # # # 50.6% 50 * 40 38.8% 30 *P
Responder vs Non-Responder Analysis of BLISS RCTs: Improvements in Patient Reported Outcomes PF * 90 80 BLISS 52+76 BL2 70 * * MH RP 12 BLISS 52+76 A/G Norms2 60 SRI Non-responders 50 SRI Responders BLISS 52+76 Non-Responders 10 40 10.4 (n=923)3 MCID Mean Change from BL 30 BLISS 52+76 Responders 8 20 (n=761)3 10 * BP 6 6.5 * RE 0 5.2 4 2 3.0 0 FACIT Fatigue SF-36 Vitality * SF GH * *p < 0.001 VT * 1. Strand V et al. ARD. 2014;73:838–44; 2. Furie R, Strand V et al. Lupus S&M. 2014;1:e000031. doi:10.1136/lupus-2014-000031; 3. www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/DrugArthritisAdvisoryCommittee/UCM233581.pdf.
SLE – New and Promising Therapies
SLE: New and Promising Therapies • NEW Therapies: Approved and Expected: – Belimumab in Lupus Nephritis ⎼ Approved; Addition to Label: December 2020 – Voclosporin in Lupus Nephritis ⎼ Approved: Jan 22, 2021 – Anifrolumab for Treatment of SLE ⎼ ? 2021 ? • Promising Therapies Targeting Type I IFN; pDCs: – BIIB059: Targeting BDCA2 on pDCs in CLE and DLE – Iberdomide: High affinity cereblon ligand • Promising Therapies: – Obinituzumab: Type II aCD20 mAb for Lupus Nephritis
Lupus Nephritis • Approximately 50% SLE patients develop significant LN – 50 – 80% respond to standard treatment within 12 months: partial/complete response 1,2 • Poor prognostic factors – Young (age < 26 years) and African-American – Elevated creatinine (> 30% over baseline) and/or nephrotic range proteinuria (> 3 gm/day) – Renal Biopsy: • Crescents, fibrinoid necrosis (> 25% of glomeruli), and microvascular clots • Class III or IV with significant activity (index > 10) and/or chronicity (index > 3-4) – Poor response to initial therapy or renal relapse – Noncompliance with medications • Recently, First Approved Therapies: ⎻ Belumimab ⎻ Voclosporin , 1. Ginzler et al. NEJM. 2005;335:2219; 2. Houssiau et al. Arthritis Rheum. 2002;46:2121.
2012 ACR Lupus Nephritis Guidelines ISN/RPS Classification of LN Class I Minimal mesangial LN Don’t TREAT Class II Mesangial proliferative LN Don’t TREAT Class III Focal LN (50% glomeruli) TREAT S= segmental, D=diffuse A= active C= chronic A/C = active/chronic Class V Membranous TREAT Class VI Advanced sclerosis LN (>90% globally) Don’t TREAT Bertsias GK et al. ARD. 2012; 71:1771; Hahn BA et al. AC&R. 2012; 64:797.
Belimumab Phase 3 RCT in LN • Phase 3 104-wk RCT in Bx proven LN: 448 pts: duration: 0.2 yr – 1:1: IV BEL+SOC vs PBO+SOC, per investigator – 1◦ EP: 1◦ efficacy renal response (PERR): U pro/Cr ≤0.7; eGFR 60 ml/min/ 1.73 m2 – 2◦ EP: complete renal response (CRR): U pro/Cr
Belimumab in Lupus Nephritis – Conclusions • Well tolerated • Patients w/ relatively early LN: Median 0.2 yrs duration; range 0.1 ⎼ 3.3 years; Classes III +/⎼ V; IV +/⎼ V; and V • Effective by renal response and complete renal response (U pro/Cr AZA • Responses as early as week 12 • Higher urinary protein, lower eGFR, lower complement levels, longer disease duration, and greater exposure to previous treatment for LN in CTX/AZA group • Af-Am patients more likely to respond although numbers were small • Greater reductions in adsDNA and C1q Abs and increases in C3 and C4 w/ BEL • Risk of renal-related AEs during RCT was ≅ 50% lower w/ BEL
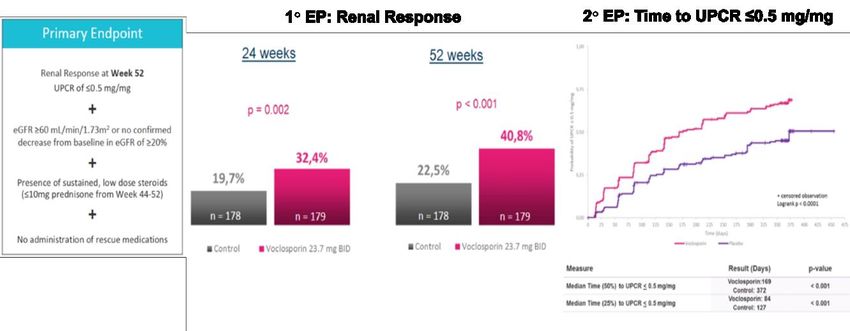
Voclosporin: Phase 2 and 3 RCTs in Lupus Nephritis Arriens C et al. EULAR. 2020: Abstract OP0277.
Voclosporin: AURORA: Phase 3 RCT in Lupus Nephritis COMBINED ANALYSIS: Ph 2 & 3 RCTs: Safety VOC Control SAEs 37 38 • Odds renal response: 2.76% greater SIEs 18 20 while maintaining GC dose ≤2.5mg QD Deaths 1 5 Disease related SAEs 18 16 • 50% ↓ UPCr: 93.7% v 75.2% PBO Disease related AEs 96 87 Arriens C, et al. EULAR. 2020. OP0277; Ginzler E et al: ACR. 2020. 1843.
Voclosporin in Lupus Nephritis: Conclusions • Phase 2 RCT: AURA: high vs low dose (23.7mg) VOCLO+MMF: 24 wks: CRR (U pro/Cr ≤0.5) 1 – But 10 deaths in low dose group due to infections vs 2 in high dose and 1 in MMF SOC • Phase 3 RCT: AURORA: 23.7mg VOCLO+MMF v MMF: 52 wks: 40.8 v 22.5% CRR – No such safety signal; AEs, SAEs, SIEs balanced; deaths 1 v 5 • Only studied w/ background MMF as SOC • Higher portion CRR at 24 weeks compared to SoC; 50% reduction in UPCR 2x faster than SOC • With rapid protocol-defined steroid taper: ≤10 mg prednisone QD weeks 44 ⎼ 52 • Improved responses in all parameters across Classes III +/⎼ V; IV +/⎼ V; and V of LN • VOCLO is a calcineurin inhibitor; cyclosporin analog: known AEs associated w/ CsA include: decreased GFR, HTN, infections, tremor, diabetes, leukopenia 2 • Most common AEs (>3%) included decreased GFR and HTN 1. Rovin B et al. Kidney Intl. 2019; 95, 219–31; 2. Gatto M et al. Nat Rev Rheum. 2019;15:30; Fanouriakis A et al. ARD 2019;78:736-45
Promising Therapies
Obinituzumab: Humanized Type II Anti-CD20 mAb • Obinutuzumab is approved for combination treatment of CLL and follicular lymphoma 1 • Compared to rituximab and ofatumumab, administration results in: – 100-fold greater antibody-dependent cytotoxicity due to a glycoengineered Fc 2,3 – Greater direct cell death, reduced internalization, less reliance on complement- dependent cytotoxicity because of its type II binding conformation 2,3 • Results in greater B-cell depletion than rituximab in tissue3 and SLE patient samples 4 • Superior to rituximab in head-to-head RCTs in B-cell malignancies 5,6 1. Obinutuzumab USPI; 2. Herter. Mol Cancer Ther. 2013; 3. Mossner. Blood. 2010; 4. Reddy. Rheumatology. (Oxford). 2017; 5. Goede. NEJM. 2014; 6. Marcus. NEJM. 2017; Furie R et al. ACR. 2020: 0988;
Obinituzumab: Phase 2 NOBILITY RCT in LN 104-week double-blind period Obinutuzumab 1000 mg + MMF (n = 63) 1:1 All patients received MMF, 1000-3000 mg IV methylprednisolone, and a prednisone taper* Placebo + MMF (n = 62) OBI or PBO 0 2 4 8 12 24 26 36 52 76 Week 104 infusions *MMF target dose 2-2.5g, oral prednisone 0.5 mg/kg/day tapered to 7.5 mg/day by Week 12 and held until Week 52. Furie R et al. ACR. 2020: 0988; Vital EM. ibid: 0859
Obinituzumab: Pharmacodynamics and Biomarkers Conventional flow cytometry (≤ 5 cells/microL) Changes in C3, C4, anti-ds DNA Abs and eGFR Patients with depletion (%) 100% 98% 96% 96% 93% 94% 80% 60% 40% 16% 20% 12% 2% 4% 5% 4% 2% 0% 2 4 12 24 52 104 Week Last Obi Dose Obinutuzumab + MMF Placebo + MMF Furie R et al. ACR. 2020: 0988; Vital EM et al. ibid: 0859. Week Week
Obinituzumab: Renal Response Endpoints Obinutuzumab PRR Placebo PRR Overall renal response (CRR or PRR) Obinutuzumab CRR Placebo CRR Δ25%, P = 0.005 Patients with a response (%) Δ20%, P = 0.025 Δ20%, P = 0.024 60% 60% 60% 21% 13% 40% 40% 11% 40% 38% 41% 35% 13% 11% 6% 20% 20% 20% 23% 23% 18% 0% 0% 0% OBI + MMF PBO + MMF OBI + MMF PBO + MMF OBI + MMF PBO + MMF (n = 63)Week 52 (n = 62) (n = 63) Week 76 (n = 62) (n = 63)Week 104 (n = 62) CRR required all of: PRR required all of: • UPCR < 0.5 • UPCR ≥ 50% reduction to
Obinituzumab: Safety Through Week 104 Obinutuzumab + MMF Placebo + MMF (n = 64) (n = 61) Any adverse event 58 (91%) 54 (89%) Deaths (cause) 4 (7%) 1 (2%) GI bleed, SLE, PML, GI perforation Respiratory infection Serious adverse events 16 (25%) 18 (30%) Serious infection events 5 (8%) 11 (18%) Infection adverse event 48 (75%) 38 (62%) Adverse event leading to discontinuation from blinded 1 (2%) 3 (5%) infusions Infusion-related reaction 10 (16%) 6 (10%) Infusion-related reaction (7), headache, tachycardia, Infusion-related reaction (6), insomnia hypertension, nausea Serious infusion-related reaction 0 0 Progressive multifocal leukoencephalopathy 0 1 (2%) One patient randomized to placebo inadvertently received active obinutuzumab during the first cycle and included in obinutuzumab group for safety. Phase 3 REGENCY RCT underway. Furie R et al. ACR. 2020: 0988; Vital EM et al. ibid: 0859.
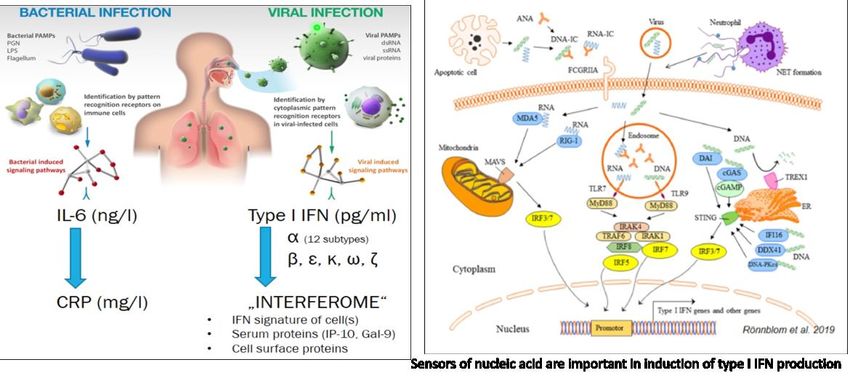
The Interferon System in SLE Rönnblom L, Leonard D. Lupus S&M. 2019;6:e000270. doi:10.1136/lupus-2018-000270.
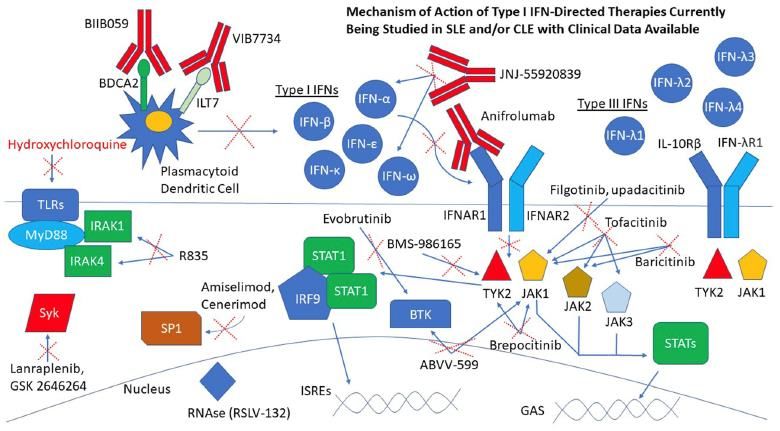
Therapies Directed Against IFNs in SLE Chaichian Y & Strand V. Clin Rheum. 2021: https://doi.org/10.1007/s10067-020-05526-1.
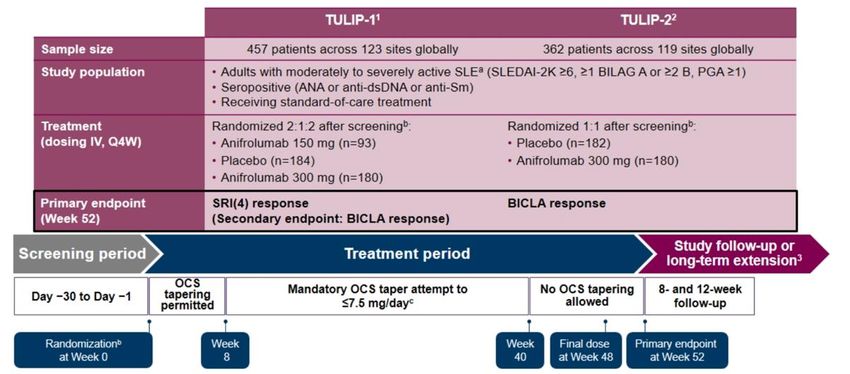
Anifrolumab in SLE: TULIP-1 and -2 Phase 3 RCTs Morand E et al. EULAR. 2020: Abstract OP0003.
Anifrolumab in SLE: Time to Onset BICLA Responses to Wk 52 • BICLA response is defined as all of the following1,2: − Reduction of baseline BILAG-2004 A and B domain scores to B/C/D and C/D, respectively, and no worsening in other BILAG-2004 organ systems − No increase in SLEDAI-2K (from baseline) or PGA score (≥0.3 points from baseline) − No study treatment discontinuation − No use of restricted medications beyond protocol-allowed thresholds Morand E et al. EULAR. 2020: Abstract OP0003.
Anifrolumab: What does It Mean to Be a BICLA Responder? Patients with ≥1 flare Patients w/ ≥1 Flare Sustained Sustained oral Reductions: GC dosage reductionGCs to ≤7.5≤7.5 mg/daymg QD a 100 Difference –23.9% (95% CI –30.4% to –17.5%), 100 BICLA Responders have: 80 nominal P
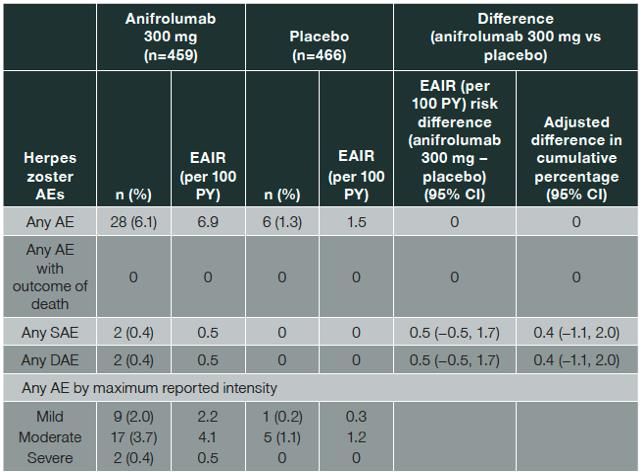
Herpes Zoster With Anifrolumab: Phase 2 and 3 RCTs H Zoster more frequent w/ Anifrolumab • Most single dermatome; few SAEs or D/Cs • More frequent in Asians; with IS use Furie R et al. ACR. 2020: 0849.
Anifrolumab in SLE: TULIP-1 and -2 Phase 3 RCTs: Conclusions • Robust BICLA responses at Week 52 with anifrolumab in TULIP-1, TULIP-2, and pooled data – No substantive impact on effect size by demographics, BL disease activity, or BL GC doses • Baseline type I IFNGS test status: – Responses to anifrolumab similar in IFNGS test– high and – low – Numerically higher placebo responses in IFNGS low, thus lower BICLA effect size • Clinical meaningfulness of “BICLA Responders” – Fewer SLE Flares – Clinically meaningful reductions in GC doses – Improved PROs: SF-36, LupusQOL and FACIT-F all statistically greater in responders vs non-responders in TULIP-1, -2 and combined analyses – Lower medical resource use • Well tolerated; expected increase in HZ infections; majority not serious or requiring D/C Morand E et al. EULAR. 2020: Abstract OP0003 and OP0049; Furie. ACR. 2020: #850.
Future Therapies The Pipeline
Promising SLE Therapies BIIB059: Targeting BDCA2 on pDCs in CLE and DLE
BIIB059: hu mAb Targeting BDCA2 on pDCs: Ph 2 LILAC RCTs Type 1 interferons (IFN-Is) are implicated in SLE pathogenesis, and plasmacytoid dendritic cells (pDCs) produce large amounts of IFN-I in SLE1 • In patients with SLE: – Serum levels of IFN- are often elevated1 – Expression of IFN-regulated genes is increased in the majority1,2,3 – IFN-I receptor blockade has been shown to reduce SLE disease activity4 • pDCs accumulate in the skin and other tissues of SLE patients such as kidneys and secondary lymphoid organs5,6 • BDCA2 receptors are uniquely expressed on the surface of pDCs7 Furie R et al. ACR. 2020: Abstract 0935; Werth V, et al. ACR. 2020: Abstract 0986.
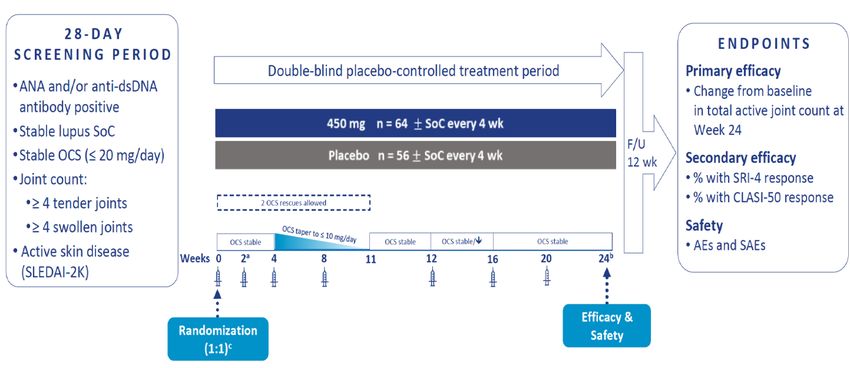
BIIB059: Phase 2 LILAC Part A in Active SLE Furie R et al. ACR. 2020: 0935.
BIIB059: Phase 2 LILAC Part A in Active SLE: Endpoints Week 24 1◦ EP: Change in Active Joint Count 2◦ EP: SRI-4 Responses Furie R et al. ACR. 2020: 0935.
BIIB059: hu mAb Targeting BDCA2 on pDCs: Phase 2 LILAC Werth V et al. EULAR. 2020: Abstract OP0193; ACR. 2020: Abstract 0986.
BIIB059: hu mAb Targeting BDCA2 on pDCs: Phase 2 LILAC • BIIB059 at doses of 50, 150, and 450 mg SC Q4W for 12 weeks significantly reduced CLASI-A score (% from baseline) at Week 16 • A significant dose-response relationship was demonstrated • A higher % of participants achieved CLASI-50 and ≥ 7-point reduction in CLASI-A score from baseline with BIIB059 vs. placebo at Week 16 • Majority of AEs were mild or moderate • Incidence of SAEs was similar in pooled BIIB059 and placebo Werth V et al. EULAR. 2020: Abstract OP0193; ACR. 2020: Abstract 0986.
Promising SLE Therapies Iberdomide: High Affinity Cereblon Ligand
Iberdomide: High Affinity Cereblon Ligand • Transcription factors Ikaros (IKZF1) and Aiolos (IKZF3) involved in immune cell development and homeostasis • Gene polymorphisms of IKZF1 and IKZF3 overexpressed in cells of SLE patients and associated with risk of disease development • Iberdomide is a high affinity cerblon ligand that promotes ubiquination and proteasomal degradation of Ikaros and Aiolos -> ↓ B cells and autoAbs; ↓ pDCs & IFNa and ↑ Tregs & IL-2 • Phase 2 RCT: – 3 doses: 2:2:2:1: 0.15, 0.3, 0.45mg QD v PBO; re-randomization of PBO at wk 24; LTE to wks 52; 104 – 1◦ EP: SRI-4 at wk 24 – Mean ds duration: 7.7 ⎼ 10.4 yrs; SLEDAI: 9.5 ⎼ 9.8; CLASI: 6.3 ⎼ 7.2; SJC: 5.5 ⎼ 7.2; TJC: 8.2 ⎼ 9.8 – Ikaros high: 65 ⎼ 79%; Aiolos high: 33 ⎼ 44%; Type I IFN high: 58 ⎼ 70%; adsDNA Ab+: 28 Lipsky PE et al. ACR. 2020: 851; Mettill J et al. ibid: 0987.
Iberdomide: Phase 2 RCT Responses by Aiolos and Type I IFN Signature at BL • SRI-4 response at week 24 achieved by 54.3% patients receiving 0.45mg QDay vs 34.9% PBO (stratified difference, 19.4%; 95% CI: 4.12, 33.42, p = 0.011) • Iberdomide significantly reduced activity of Type I IFN and B cell pathways – Dose dependent manner • 0.45mg dose led to: – ↓ B cells expressing gene for BLyS R – ↓ pDCs – ↑ % Tregs, CD8+ CTLs & TFH cells – ↑ IL-10 and IL-2 levels – ↓ adsDNA-Abs • ? Broad rebalance of immune regulation via ↑ IL-2 and Tregs Lipsky PE et al. ACR. 2020: 851; Mettill J et al. ibid: 0987.
Promising SLE Therapies Baricitinib
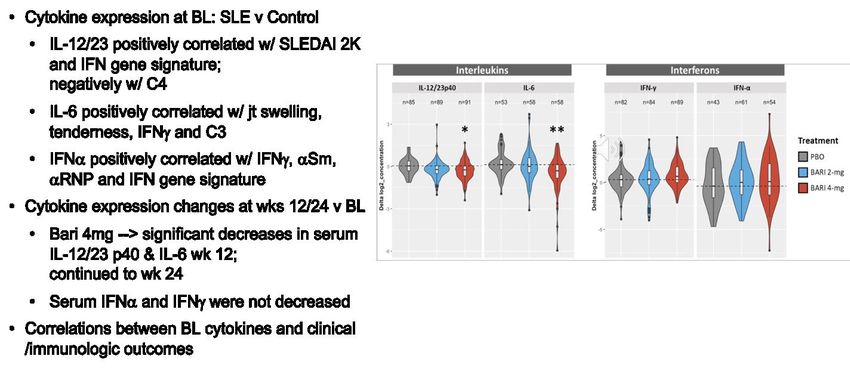
Baricitinib: 24 week Phase 2 RCT in SLE: JAHH 1. Wallace DJ et al. EULAR. 2018: OP0019; ibid: Lancet. 2018: 392:222-31; 2. Doerner T et al. ACR. 2018: #1894; 3. Doerner T et al: EULAR. 2020: OP0045.
Baricitinib: 24 week Phase 2 RCT in SLE: JAHH Wallace DJ, et al. EULAR 2018: OP0019: ibid: Lancet 2018: 392:222-31; Doerner T et al: ACR 2018: #1894; Doerner T et al: EULAR 2020: OP0045.
Other Promising SLE Therapies Entering Phase 2 RCTs VIB7734: humanized, afucosylated IgG1 mAb vs ILT7 on surface of pDCs, triggers ADCC JNJ-839: mAb to IFNw and IFNa subtypes NKTR 358: Pegylated IL-2: expansion and activation of Tregs AMG-592: IL-2 mutein Rozibafusp alfa: Bispecific Ab peptide conjugate vs BAFF and ICOSL; Ph 1 RCT in RA PRV-3279: Novel Bispecific DART vs CD32B (FcgRIIB) and CD79B BcR subunit Werth V et al. ACR. 2020: L10; Orillion A et al. Ibid: 1834; Fanton C et al. ibid: 1824; Abuqayyas L et al. ibid: 0235; Dunford P et al. ibid: 0860.
SLE Pathophysiology and Potential Therapeutic Targets BDCA2 Rituximab JAKi CD28 CD74 CD80/86 Obinutuzumab MHC-II TCR B cell CD20 T cell Dendritic cell CD80/86 CD28 CD22 Hydroxychloroquine CLTA4-B7 CD40L CD40 Belimumab Abatacept Dapirolizumab Blys APRIL IFNα Anifrolumab Low-dose IL-2 Atacicept Methotrexate Azathioprine Cell proliferation Mycophenolate mofetil Leflunomide Cytotoxics mTOR inhibitors Cyclosporine Voclosporin Cyclophosphamide Plasma cell Proteasome Immune complexes Autoantibodies Bortezomib KZR-616 Selected agents approved for/commonly used in SLE management Selected agents in trials for SLE management
Target Agent Therapeutics in T cells Anti-CD40L Fab-PEG (dapirolizumab) Rigerimod (P140 peptide) (lupuzor) Phase 2/3 RCTs Low dose IL-2 (NKTR-358) IL-2 mutein (AMG-592) Autologous TREGs B cells BTK inhibitors (evobrutinib, AC0058TA, M2951, GDC0853) Anti-CD19/FcγRIIb (obexelimab) Anti-CD20 (SBI-087, obinutuzumab) Anti-CD38 on plasma cells (TAK-079) Anti-CD40 (BI 655064) Anti-BAFF/April (telitacicept, atacicept) Anti-ICOS/anti-BAFF (Rozibafusp alfa) pDC Anti-BDCA2 (BIIB059) blood dendritic cell Ag 2 Complement Anti-MASP-2 (OMS721) Cytokines Anifrolumab Interferon alpha kinoid vaccine Anti-IL-21 (BOS-161721) Anti-IL-12/23: Ustekinumab: failed Anti-TWEAK (BIIB023) JAK-STAT Tofacitinib, Baricitinib, Upadacitinib, Filgotinib Tyk-2 (BMS-986165) Other Cereblon modulator (iberdomide) Human RNAase (RSLV-132) Mesenchymal stem cell infusion Chemokine inhibitor (PF-06835375) Felten R et al. Autoimmun Rev. 2018; 17: 781; Immunoproteasome-LMP2/7 unit (KZR-616) updated. Cenerimod (S1P1 R modulator)
Summary • Prognosis is improving yet morbidity and mortality pose significant risk • Large impact of disease on patient reported fatigue and HRQOL • New SLE classification criteria facilitate earlier identification of SLE • Guidelines: PJP prophylaxis, HCQ dosing and retinal toxicity monitoring • Tapering and use of lowest effective GC doses imperative • Newly approved therapies offer promise!! – Expect 3 approvals within the year!! – Indicate better understanding of trial designs and outcome measures • Hope for the future with many new targets; improved understanding of the underlying disease
You can also read

















































