NatioNal Drug Strategy 2010-2015 - Ministerial Council on Drug Strategy - A framework for action on alcohol, tobacco and other drugs
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Ministerial Council on Drug Strategy NatioNal Drug Strategy 2010–2015 A framework for action on alcohol, tobacco and other drugs
This document was approved by the
Ministerial Council on Drug Strategy
at its meeting held in Perth on
25 February 2011.
ISBN: 978-1-74241-406-5
Online ISBN: 978-1-74241-407-2
Publications Number: D0224
Paper-based publications internet sites
© Commonwealth of Australia 2011. © Commonwealth of Australia 2011.
This work is copyright. You may This work is copyright. You may
reproduce the whole or part of this work download, display, print and reproduce
in unaltered form for your own personal the whole or part of this work in unaltered
use or, if you are part of an organisation, form for your own personal use or, if you
for internal use within your organisation, are part of an organisation, for internal
but only if you or your organisation do not use within your organisation, but only
use the reproduction for any commercial if you or your organisation do not use
purpose and retain this copyright notice the reproduction for any commercial
and all disclaimer notices as part of that purpose and retain this copyright notice
reproduction. Apart from rights to use and all disclaimer notices as part of that
as permitted by the Copyright Act 1968 reproduction. Apart from rights to use
or allowed by this copyright notice, all as permitted by the Copyright Act 1968
other rights are reserved and you are not or allowed by this copyright notice, all
allowed to reproduce the whole or any other rights are reserved and you are not
part of this work in any way (electronic allowed to reproduce the whole or any
or otherwise) without first being given part of this work in any way (electronic
the specific written permission from the or otherwise) without first being given
Commonwealth to do so. Requests the specific written permission from the
and inquiries concerning reproduction Commonwealth to do so. Requests
and rights are to be sent to the and inquiries concerning reproduction
Communications Branch, Department and rights are to be sent to the
of Health and Ageing, GPO Box 9848, Communications Branch, Department
Canberra ACT 2601, or via email to of Health and Ageing, GPO Box 9848,
copyright@health.gov.au. Canberra ACT 2601, or via email to
copyright@health.gov.au.Contents Executive summary ii 1. About the National Drug Strategy 1 2. The Pillars 9 Pillar 1: Demand reduction 9 Pillar 2: Supply reduction 13 Pillar 3: Harm reduction 16 3. Supporting approaches 20 Workforce 20 Evidence base 21 Performance measures 22 Governance 24 Appendix A 26 NATIONAL DRUG STRATEGY 2010–2015 i
Executive summary
The aim of the The harms to individuals, families,
communities and Australian society as a
In the National Drug Strategy 2010–
2015, the three pillars are underpinned
National Drug whole from alcohol, tobacco and other by strong commitments to:
drugs are well known. For example, the • building workforce capacity
Strategy 2010–2015 cost to Australian society of alcohol, • evidence-based and evidence-
is to build safe and tobacco and other drug misuse1 in the
financial year 2004–05 was estimated at
informed practice, innovation and
evaluation
healthy communities $56.1 billion, including costs to the health • performance measurement
and hospitals system, lost workplace • building partnerships across sectors.
by minimising productivity, road accidents and crime.
Specific objectives have been identified
alcohol, tobacco and The overarching approach of harm under each pillar as follows:
other drug-related minimisation, which has guided the
National Drug Strategy since its inception
Demand reduction
health, social and in 1985, will continue through 2010–2015.
• prevent uptake and delay onset of
drug use
This encompasses the three pillars of:
economic harms • demand reduction to prevent the
• reduce use of drugs in the community
• support people to recover from
among individuals, uptake and/or delay the onset of use
of alcohol, tobacco and other drugs;
dependence and reconnect with the
families and reduce the misuse of alcohol and the
community
• support efforts to promote social
communities. use of tobacco and other drugs in
the community; and support people
inclusion and resilient individuals,
families and communities.
to recover from dependence and
reintegrate with the community Supply reduction
• supply reduction to prevent, stop, • reduce the supply of illegal drugs
disrupt or otherwise reduce the (both current and emerging)
production and supply of illegal drugs; • control and manage the supply of
and control, manage and/or regulate alcohol, tobacco and other legal
the availability of legal drugs drugs.
• harm reduction to reduce the
Harm reduction
adverse health, social and economic
• reduce harms to community safety
consequences of the use of alcohol,
and amenity
tobacco and other drugs.
• reduce harms to families
The three pillars apply across all drug • reduce harms to individuals.
types but in different ways, for example,
Part 1 of the National Drug Strategy
depending on whether the drugs being
2010–2015 provides background and
used are legal or illegal. The approaches
explains the conceptual framework
in the three pillars will be applied with
of the strategy.
sensitivity to age and stage of life,
disadvantaged populations, and settings Part 2 details specific objectives and
of use and intervention. suggested actions under each pillar.
Part 3 discusses the supporting
approaches of workforce, evidence,
performance monitoring and governance.
1. Collins, D and Lapsley, H 2008, The Costs
of Tobacco, Alcohol and Illicit Drug Abuse
to Australian Society in 2004/05, National
Drug Strategy Monograph Series No. 64.
ii NATIONAL DRUG STRATEGY 2010–20151. About the National
Drug Strategy
The National Drug At the heart of the framework are the
three pillars of demand reduction, supply
Mission:
Strategy provides a reduction and harm reduction, which To build safe and
are applied together to minimise harm.
national framework Prevention is an integral theme across healthy communities
for action to minimise the pillars. by minimising alcohol,
the harms to The 2010–2015 framework builds on
longstanding partnerships between the
tobacco and other
individuals, families health and law enforcement sectors and drug-related health,
seeks to engage all levels and parts of
and communities government, the non-government sector social and economic
from alcohol, and the community.
harms among
tobacco and other Australia has had a coordinated national
policy for addressing alcohol, tobacco
individuals, families
drugs. and other drugs since 1985 when and communities.
the National Campaign Against Drug
Abuse was developed. In 1993 it was
renamed the National Drug Strategy. This
2010–2015 iteration is the sixth time the
strategy has been updated to ensure
it remains current and relevant to the
contemporary Australian environment.
Throughout this strategy, these terms are used:
Drug
The term ‘drug’ includes alcohol, tobacco, illegal (also known as ‘illicit’) drugs,
pharmaceuticals and other substances that alter brain function, resulting in changes
in perception, mood, consciousness, cognition and behaviour.
Illegal drug
A drug that is prohibited from manufacture, sale or possession—for example
cannabis, cocaine, heroin and amphetamine type stimulants (ecstasy,
methamphetamines).
Pharmaceuticals
A drug that is available from a pharmacy, over-the-counter or by prescription, which
may be subject to misuse—for example opioid-based pain relief medications, opioid
substitution therapies, benzodiazepines, over-the-counter codeine and steroids.
Other substances
Other psychoactive substances, legal or illegal, potentially used in a harmful way—
for example kava, or inhalants such as petrol, paint or glue.
NATIONAL DRUG STRATEGY 2010–2015 1The harms from • Other drugs and substances that are Harm minimisation
legally available can cause serious
drug use harm. The harmful use of inhalants,
Since the National Drug Strategy
began in 1985, harm minimisation has
The harms to individuals, families, like petrol, paint and glue, can cause
been its overarching approach. This
communities and Australian society as a brain damage and death. The misuse
encompasses the three equally important
whole from alcohol, tobacco and other of pharmaceutical drugs can have
pillars of demand reduction, supply
drugs is well known. serious health impacts and their
reduction and harm reduction being
trafficking contributes to illegal drug-
• The cost to Australian society of applied together in a balanced way.
related crime.
alcohol, tobacco and other drug • Demand reduction means strategies
• Alcohol, tobacco and other drug
misuse2 in 2004–05 was estimated and actions which prevent the uptake
use can contribute to and reinforce
at $56.1 billion, including costs to and/or delay the onset of use of
social disadvantage experienced by
the health and hospitals system, alcohol, tobacco and other drugs;
individuals, families and communities.
lost workplace productivity, road reduce the misuse of alcohol and the
Children living in households where
accidents and crime. Of this, tobacco use of tobacco and other drugs in
parents misuse drugs are more likely
accounted for $31.5 billion (56.2 per the community; and support people
to develop behavioural and emotional
cent), alcohol accounted for to recover from dependence and
problems, tend to perform more
$15.3 billion (27.3 per cent) and illegal reintegrate with the community.
poorly in school and are more likely to
drugs $8.2 billion (14.6 per cent). • Supply reduction means strategies
be the victims of child maltreatment.
• The excessive consumption of alcohol and actions which prevent, stop,
Children with parents who drink
is a major cause of health and social disrupt or otherwise reduce the
heavily, smoke or take drugs are more
harms. Short episodes of heavy production and supply of illegal drugs;
likely to do so themselves—leading to
alcohol consumption are a major and control, manage and/or regulate
intergenerational patterns of misuse
cause of road and other accidents, the availability of legal drugs.
and harms. Family breakdown and
domestic and public violence, and • Harm reduction means strategies
job loss is also associated with
crime. Long-term heavy drinking and actions that primarily reduce the
problematic drug use.
is a major risk factor for chronic adverse health, social and economic
• Disadvantaged populations are at
disease, including liver disease and consequences of the use of drugs.
greater risk of harms from alcohol,
brain damage, and contributes
tobacco and other drug misuse. The National Drug Strategy 2010–2015
to family breakdown and broader
For example, Aboriginal and Torres seeks to build on this multi-faceted
social dysfunction. Drinking during
Strait Islander peoples experience a approach which is recognised
pregnancy can cause birth defects
disproportionate amount of harms internationally as playing a critical role
and disability, and there is increasing
from alcohol, tobacco and other in Australia’s success in addressing
evidence that early onset of drinking
drug use. Drug-related problems drug use.
during childhood and the teenage
play a significant role in disparities in
years can interrupt the normal
health and life expectancy between
development of the brain.
Indigenous and non-Indigenous
• Tobacco smoking is one of the
Australians. Indigenous Australians are
top risk factors for chronic disease
more likely to die of smoking-related
including many types of cancer,
illnesses, such as diseases of the
respiratory disease and heart disease.
respiratory system and cancers, than
• Illegal drugs not only have dangerous
other Australians.
health impacts but they are a significant
contributor to crime. They are a major
activity and income source for organised
crime groups. Like alcohol, illegal
drugs can contribute to road accidents
and violent incidents, and to family
breakdown and social dysfunction.
Unsafe injecting drug use is also a major
driver of blood-borne virus infections like
hepatitis C and HIV/AIDS. 2. Collins, D and Lapsley, H 2008, The Costs
of Tobacco, Alcohol and Illicit Drug Abuse
to Australian Society in 2004/05.
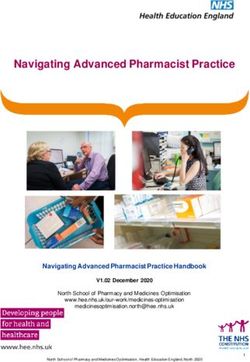
2 NATIONAL DRUG STRATEGY 2010–2015Figure 1: Harm minimisation approach
Disadvantaged
Alcohol Harm minimisation
populations
Tobacco Age/stage of life
Demand Supply
reduction reduction
Illegal drugs Settings
Pharmaceuticals Harm Partnerships
reduction
Other substances Other frameworks
Workforce
Evidence base
Performance measures
Governance
(including partnerships and consumer participation)
Figure 1 illustrates the approach that drugs at transition points such • The three pillars will be underpinned
will be taken to implement the harm as moving from school to work. by commitments to:
minimisation framework under the The workplace, schools, licensed – partnerships across sectors
National Drug Strategy 2010–2015: premises and communities need to – consumer participation in
• The three pillars apply across all be considered as settings for possible governance
drug types but in different ways. For interventions. The potential of new – building the evidence base,
example, supply reduction of legal media, such as social networking sites evidence-informed practice and
drugs refers to regulation of supply, on the internet, to deliver interventions innovation
but for illegal drugs means disruption also needs to be considered. – monitoring performance against
of supply. This is covered in more Integrated cross-sectoral approaches the strategy and its objectives
detail against each pillar. may be needed for disadvantaged – developing a skilled workforce
• The approaches within the three populations such as people with co- that can deliver on the strategy.
pillars need to be sensitive to age occurring mental health and alcohol
These supporting approaches are
and stage of life, disadvantaged and other drug-related problems.
covered in Part 3 of the strategy.
populations and settings of use and These are explained in more detail
intervention. People may be more below and against each pillar.
vulnerable to experimenting with
NATIONAL DRUG STRATEGY 2010–2015 3Successes of the • Harms associated with injecting Challenges for 2010–2015
drug use have also been reduced.
National Drug Strategy It is estimated that from 2000–2009
Many challenges still remain. The
following have been identified as drug-
Since the inception of the National needle and syringe programs, which
specific priorities for 2010–2015:
Campaign Against Drug Abuse in 1985, ensure the safe supply and disposal of
• Risky drinking, drinking to intoxication
Australia has had major successes in syringes to injecting drug users, have
and alcohol-related disease, injury
reducing the prevalence of, and harms directly averted over 32 000 new HIV
and violence continue to cause
from, drug use. infections and nearly 97 000 hepatitis
significant harms in the community.
C infections.
• Far fewer Australians are smoking An estimated 813 072 Australians
• Since its introduction in September
and being exposed to second-hand aged 15 years and older were
2005 non-sniffable Opal fuel has
smoke as a result of comprehensive hospitalised for alcohol-attributable
contributed to a 70 per cent reduction
public health approaches, including injury and disease over the 10-year
in petrol sniffing across 20 regional
bans on advertising, bans on period 1995–96 to 2004–05. Rates
and remote communities in Western
smoking in enclosed public spaces of alcohol-attributable hospitalisations
Australia, South Australia, the
and significant investments in public increased in all states and territories.
Northern Territory and Queensland.
education and media campaigns. The Alcohol remains a leading cause of
• Early intervention and diversion
daily smoking rate among Australians Australian road deaths, particularly
programs, which help prevent young
aged 14 years and over has fallen among young people.
people and adults apprehended for
from 30.5 per cent in 1988 to • Smoking rates continue to be
drug use from getting caught up in
16.6 per cent in 2007. unacceptably high in the general
the criminal justice cycle by diverting
• Far fewer people are using illegal population—16.6 per cent smoked
them to treatment interventions,
drugs. The 2007 National Drug daily in 2007—and particularly among
have become an established
Strategy Household Survey shows the Aboriginal and Torres Strait Islander
and successful part of the harm
proportion of people reporting recent people, of whom around 45 per cent
minimisation approach.
use of illegal drugs fell from 22 per smoked daily in 2008. The Council
• Drink driving has become largely
cent in 1998 to 13.4 per cent in 2007. of Australian Governments (COAG)
unacceptable within the general
The recent use of cannabis—the most has agreed in the National Healthcare
Australian population. There was a
commonly used illegal drug—fell from Agreement 2008 to targets of
substantial reduction in alcohol-related
17.9 per cent in 1998 to 9.1 per cent reducing the prevalence of smoking
road deaths between the mid 1970s
in 2007. in the Australian population to
and the early 1990s through mass
• Law enforcement agencies have 10 per cent by 2018 and to halving
breath testing of drivers, lower and
continued to be effective in detecting the smoking rate among Aboriginal
nationally consistent driver blood
and seizing illegal drugs to disrupt and Torres Strait Islander peoples.
alcohol content limits, zero limits for
supply. The number of illegal drug • Changing patterns of use of, and
special driver groups, a system of
seizures increased by almost 70 harms from, illegal drugs need to be
penalties, mass public education and
per cent between 1999–2000 and continually monitored and responded
media campaigns and other road
2008–09, and the collective weight to. At the time of writing in 2010,
safety initiatives.
of seizures increased by about emerging trends included:
• Far more is known about what works
116 per cent.
in the treatment of alcohol and other
• The heroin shortage that began in
drug dependence, including through
2000 has been sustained, with heroin
brief interventions, detoxification,
use remaining at low levels since then.
pharmacological and psychosocial
treatment approaches.
4 NATIONAL DRUG STRATEGY 2010–2015– increasing harms from – while rates of heroin and other There are a number of structural priorities
cannabis. The number of older injecting drug use have stabilised for 2010–2015:
users presenting to hospital with at low levels, harms from ongoing • The internet poses both challenges
dependence and other cannabis- heroin and other injecting drug and opportunities for the National
related problems increased use persist, particularly in relation Drug Strategy. It is an efficient
markedly between 2002–07 and to blood-borne virus infections and channel for information on illegal drug
nearly doubled among users aged overdose. manufacture and use, and a difficult
30–39. Hospital presentations for – new ‘analogue’ drugs—derivatives to regulate advertising medium for
cannabis-induced psychosis were or substances similar in chemical alcohol and tobacco. However, it also
highest among users aged 20–29. structure to illegal drugs—are provides opportunities for providing
The number of hospital outpatient emerging, particularly in sales information, and potentially treatment,
treatment episodes for cannabis- over the internet. Many of these to audiences who may not be reached
related problems increased by substances have not yet been through other media.
30 per cent. Cannabis cultivation captured under the drug law • Planning and quality frameworks
continues to be an activity of schedules which govern their legal for treatment services need to
interest for organised crime. status. incorporate evidence into successful
– continuing high demand for • The harms from drug use are drug treatments.
ecstasy and domestic production potentially amplified by the increasing • Continued work is needed with the
of amphetamine type stimulants pattern of poly-drug use—the mental health sector to improve
(ATS). Self-reported recent use of concurrent use of more than one drug. links and coordination between the
ecstasy increased from 2.4 per Alcohol is the drug most commonly two sectors to support individuals
cent in 1998 to 3.5 per cent in used in this way. For example, it is with co-occurring mental illness and
2007 with particularly concerning often used with legal drugs resulting alcohol and other drug use, and their
increases among young women. in unpredictable consequences. More families.
ATS arrests more than doubled recently it is increasingly mixed with • Data collection and management
between 1999–2000 and highly-caffeinated products/other is vital to the delivery and evaluation
2008–09. Manifestations of stimulants (‘energy drinks’). Mixing of of services and broader policy
extreme behaviour in ATS users, drugs can multiply the effects of each development. Enhancing the data that
including violence, increases risks drug, increase adverse reactions and is available and how it is used will help
for police, ambulance, and hospital the unpredictability of the reactions inform efforts under the National Drug
emergency department workers, as and even increase the risk Strategy.
well as users and the community. of overdose.
Organised crime involvement in • Pharmaceutical drug misuse. Age and stage of life
manufacturing and trafficking ATS The most commonly misused
It is well recognised that people are
is also a concern. pharmaceuticals include opioids,
at greater risk of harm from drugs at
– an expansion of the cocaine benzodiazepines, codeine, the
points of life transition. These include
market is reflected in recent stimulants methylphenidate
transitioning from primary to high school,
increases in cocaine arrests, (Ritalin) and dexamphetamine and
from high school to tertiary education or
seizures and reported use. Two performance-enhancing drugs such
the workforce, leaving home and retiring.
distinct user groups have been as steroids. Diversion and misuse
identified. The first is employed, of opioid drugs is widespread and • Drinking alcohol in adolescence can
well-educated and socially prevalent where heroin is not readily be harmful to young people’s physical
integrated individuals and the available. Misuse also occurs among and psychosocial development.
second injecting drug users. poly-drug users and those with Alcohol-related damage to the brain
chronic pain. An extra challenge is can be responsible for memory
balancing the legitimate use of, and problems, an inability to learn,
access to, pharmaceuticals with the problems with verbal skills, alcohol
need to prevent harms caused by dependence and depression.
misuse.
NATIONAL DRUG STRATEGY 2010–2015 5• The Australian Secondary School Disadvantage and • Smoking is the primary cause of
Students Alcohol and Drug Survey chronic disease among Aboriginal
has consistently shown that fewer social isolation and Torres Strait Islander peoples.
students are smoking overall. Drug use can have a significant In 2003 smoking was responsible for
However, the secondary school years impact on disadvantaged groups and one-fifth of deaths and accounted
remain a key risk period for the uptake lead to intergenerational patterns of for 12 per cent of the total burden of
of smoking, with higher rates in each disadvantage. disease among Aboriginal and Torres
age group from 12 years onwards • There is strong evidence Strait Islander peoples. In 2004–05,
through adolescence. of an association between 55 per cent of Aboriginal and Torres
• The adolescent drive to take risks social determinants—such as Strait Islander peoples aged 18 years
and the need for coping mechanisms unemployment, homelessness, and over reported drinking at short-
during adolescence can be major poverty, and family breakdown— term risky or high risk levels on at
influences on the uptake of illegal and drug use. Socio-economic status least one occasion in the previous
drugs by teenagers. has been associated with drug- 12 months.
• Young people are more at risk of related harms such as foetal alcohol • Despite a sustained decline in the
motor vehicle accidents, injuries, syndrome, alcohol and other drug prevalence of smoking among
accidental death and suicide whilst disorders, hospital admissions due people in major cities, the decline has
under the influence of alcohol and to diagnoses related to alcoholism, been slower among people living in
drugs. They are also highly susceptible lung cancer, drug overdoses and regional and remote areas. Men
to being victims of crime. alcohol-related assault. In the 2007 in these areas were significantly
National Drug Strategy Household more likely than those in major cities
The National Drug Strategy 2010–2015 Survey the highest prevalence of to report risky or high-risk alcohol
recognises the challenge of long-term recent illegal drug use was reported consumption.
drug use and misuse among adults by unemployed people—23.3 per • Thirty-five per cent of people who
and the new challenges that an ageing cent compared with 13.4 per cent use drugs also have a co-occurring
population may pose. of the general population. Alcohol, mental illness. Although people with
• Daily cannabis use is most common tobacco and other drug use among mental illness benefit from alcohol,
amongst 40–49 year olds. This age homeless people is common. One tobacco and other drug treatment,
group is nearly twice as likely as study estimated the overall 12-month they have poorer physical and mental
14–19 year olds to report daily use. prevalence of harmful alcohol use for health and poorer social functioning
This is despite an overall decline in the homeless people in Sydney at 41 per following treatment than other people.
proportion of the population reporting cent and the prevalence of drug use at • People in prison have underlying high
recent use of cannabis. 36 per cent. Family factors—including rates of drug use. In 2009, 81 per
• The proportion of Australians aged poor parent–child relationships, family cent of prison entrants were current
65 years or older is expected to disorganisation, chaos and stress and smokers and 74 per cent smoked
increase from 12.1 per cent currently family conflict and marital discord with daily, 52 per cent of prison entrants
to 24.2 per cent by 2051. Older verbal, physical or sexual abuse—also reported drinking alcohol at levels
people face particular issues with have a strong association with drug that placed them at risk of alcohol-
drug misuse including interactions use. There are a number of strong related harm and 71 per cent of prison
with prescribed medications, under- protective factors that guard against entrants had used illegal drugs in
recognition and treatment of alcohol problematic alcohol and other drug the 12 months prior to their current
and drug problems, unintentional use. These include having a job, a incarceration. Injecting drug use and
injury and social isolation. Alcohol can stable family life and stable housing. the associated risk of blood-borne
increase the risk of falls, motor vehicle These factors can be important in virus infection is a particular issue for
accidents and suicide in older people. preventing or overcoming drug-related prison populations. Among prison
problems. entrants, 35 per cent tested positive
for hepatitis C.
6 NATIONAL DRUG STRATEGY 2010–2015• Some culturally and linguistically More attention is needed to address Strong partnerships and integrated
diverse (CALD) populations may drug use among prison populations. service approaches with alcohol and
have higher rates of, or are at higher This includes addressing supply other drug treatment, social welfare,
risk of, drug use. For example, some reduction in the prison environment, income support and job services,
members of new migrant populations reducing demand through education and housing and homelessness services,
from countries where alcohol is not treatment and approaches for reducing mental health care providers and
commonly used may be at greater harm. Attention is also needed to help correctional services are needed if
risk when they come into contact prevent drug use from continuing or people with multiple and complex needs
with Australia’s more liberal drinking recurring when people leave prison. are to be assisted to stabilise their lives,
culture. Some types of drugs specific reintegrate with the community and
More focus will also be placed on the
to cultural groups, such as kava and recover from alcohol and other drug-
internet as an important emerging
khat, can also contribute to problems related problems.
medium for prevention and treatment
in the Australian setting.
approaches and as a potentially effective Closer integration with child and family
• People from disadvantaged or
tool for reaching new or hard to reach services is needed to more effectively
marginalised groups, such as gay,
settings. recognise and manage the impacts of
lesbian, bisexual, transgender
drug use on families and children.
and intersex populations, may also
experience more difficulty in accessing Partnerships Ongoing partnerships with Aboriginal
drug treatment and achieving Since its inception the National Drug and Torres Strait Islander
successful outcomes from that Strategy has been underpinned by strong communities are also needed to help
treatment unless it is appropriate for partnerships, particularly across the reduce the causes, prevalence and
their particular needs. Those who are health and law enforcement sectors, harms of alcohol misuse and tobacco
most at risk are people with multiple between the government and non- and other drug use among Aboriginal
and complex needs. This may government sectors, and among policy- and Torres Strait Islander peoples.
involve a combination of drug use, makers, service providers and experts.
Finally, Australia needs to engage
mental illness, disability and injury,
For 2010–2015 the health–law in international partnerships to
family breakdown, unemployment,
enforcement partnership will remain maximise the effectiveness of law
homelessness and/or having spent
at the centre of the strategy. However, enforcement efforts, to learn and share
time in prison.
this partnership will be extended best practice demand, supply and
Under the National Drug Strategy to other sectors as appropriate, harm reduction approaches and to
2010–2015, socially inclusive including education, particularly to help enhance our regional neighbours’
strategies and actions are needed that help tackle the more complex causes efforts to respond to the problem of
recognise the particular vulnerabilities of, and harms from, drug use in the drug use. Under the National Drug
and needs of these disadvantaged present environment (see Supporting Strategy 2010–2015, Australia will
groups. approaches: Governance). continue to actively engage in multilateral
forums for international cooperation
In relation to alcohol, partnerships
Settings continue to be needed with liquor
on alcohol, tobacco and other drug
issues, including the World Health
Settings-based approaches are also a licensing authorities, local
Organization and its implementation of
key feature of the National Drug Strategy governments including town planners
the Global Alcohol Strategy, the United
2010–2015. and transport authorities and local
Nations Office on Drugs and Crime,
communities to help reduce potential
Priority settings for possible preventive the Conference of the Parties to the
harms. Collaborative partnerships with
interventions on alcohol, tobacco World Health Organization Framework
business also need to be maintained
and other drugs will include families, Convention on Tobacco Control and
both for regulatory issues and
educational settings, workplaces, the United Nations Commission on
preventative approaches in workplaces.
licensed premises and communities. Narcotic Drugs. The Australian Federal
Police and the Australian Customs and
NATIONAL DRUG STRATEGY 2010–2015 7Border Protection Service will continue During the life of the National Drug
to cooperate with their international Strategy 2010–2015, seven sub-
counterparts on drug investigations. strategies will be updated or developed
Australian health and law enforcement to address specific priorities:
agencies and non-government • National Aboriginal and Torres Strait
organisations will also continue to engage Islander Peoples Drug Strategy
with developing countries, particularly • National Alcohol Strategy
in the Asia-Pacific region, to provide • National Tobacco Strategy
assistance on drug-related problems • National Illicit Drugs Strategy
where such assistance is needed. • National Pharmaceutical Drug Misuse
Strategy
Sub-strategies • National Workforce Development
Strategy
A number of sub-strategies sit under the
• National Drug Research and Data
umbrella of the National Drug Strategy
Strategy.
2010–2015. These sub-strategies
provide direction and context for specific Standing committees and working
issues, while maintaining the consistent groups of the Intergovernmental
and coordinated approach to addressing Committee on Drugs (see Supporting
drug use, as set out in this strategy. In approaches: Governance) will be
particular, the National Drug Strategy responsible for the development of these
Aboriginal and Torres Strait Islander sub-strategies. Best efforts will be made
Peoples Complementary Action Plan was to synchronise the timing of these sub-
developed to provide national direction strategies.
on drug-related problems that concern
There are also national strategies and
Aboriginal and Torres Strait Islander
frameworks in other sectors relevant to
peoples.
the work of the National Drug Strategy
2010–2015, where efforts are needed to
integrate and leverage complementary
approaches. These frameworks are listed
in Appendix A.
8 NATIONAL DRUG STRATEGY 2010–20152. The Pillars
This part of the The objectives and actions listed under
each pillar are not exhaustive but provide
The appropriate mix of educational and
social marketing approaches will vary by
National Drug a general explanation of what is involved. drug type. Whole-of-population strategies
may be more appropriate for alcohol
Strategy sets out The approach and the actions specified
and tobacco and for those illegal drugs
take into consideration differences across
the objectives drug type, disadvantaged populations,
that are widely used, while approaches
targeted to users and at-risk groups may
of, and actions age and stage of life and settings.
be more appropriate for those drugs
only used by a small percentage of the
against, each of Pillar 1: Demand population.
the three pillars reduction Settings-based approaches will be
of the Australian Demand reduction includes strategies to
an important feature of the National
Drug Strategy 2010–2015. The COAG
harm minimisation prevent the uptake of drug use, delay the Preventive Health National Partnership
first use of drugs, and reduce the misuse Agreement includes a focus on
approach—demand of alcohol, and the use of tobacco and prevention activities for alcohol and
reduction, supply other drugs. This includes providing
information and education, for example
tobacco in communities, childcare and
school settings and workplaces. Other
reduction and harm through school-based programs or settings such as prisons also require
public-awareness campaigns. Evidence-
reduction. Each of based early intervention programs,
planned and comprehensive demand-
reduction strategies.
the pillars is equally diversion, counselling, treatment,
rehabilitation, relapse prevention, No one strategy on its own can prevent
important to the aftercare and social integration can and reduce the demand for drugs.
Rather, broad-based, multidisciplinary
help drug users reduce or cease their
success of the drug use. The demand for drugs can and flexible strategies are needed to
meet the varied needs of individuals and
strategy. also be affected by their availability and
affordability which can, depending on communities.
the drug, be influenced through supply Demand reduction requires the
control, regulation and taxation. cooperation, collaboration and
People use drugs for a range of reasons participation of a diverse range of
including as an integral part of social sectors. It is important to recognise the
behaviour, to experiment, because range of sectors that can influence drug
of peer pressure, to escape or cope demand and to develop closer links with
with stress or difficult life situations or them.
to intensify feelings and behaviours.
Drug use is influenced by a complex
interaction of physical, social and
economic factors. Disadvantaged
populations are at heightened risk of drug
misuse and its associated harms. People
can also be at risk of different patterns
of use at different ages. For example,
younger people may be more at risk of
short-term harms from alcohol use while
older people may be more at risk from
chronic alcohol misuse.
NATIONAL DRUG STRATEGY 2010–2015 9Objective 1: Actions Objective 2:
Prevent uptake and delay onset • Explore and implement strategies Reduce use of drugs
of drug use that contribute to the development in the community
Preventing drug use can be more of a culture that promotes healthy The effects of the use of drugs go
cost-effective than treating established lifestyles. beyond injury and illness or disease
drug-related problems. Prevention • Develop and implement treatment to a range of social and economic
efforts can help reduce personal, family and family-support strategies that consequences. People experiencing
and community harms, allow better use can prevent and break patterns of problems with drugs can find it difficult
of health system resources, generate drug use, including intergenerational to form or maintain relationships, may
substantial economic benefits and patterns. have their educational and vocational
produce a healthier workforce. • Work collaboratively with other paths disrupted and their general social
national policies to reduce risk factors development hampered. To reduce the
A key step in preventing the uptake of and build protective factors, while occurrence and cost of such problems,
drugs is changing the culture so that recognising the diverse range of interventions need to be implemented
drug misuse is no longer seen as a influences on drug use. early, preferably before problems emerge.
cultural norm. This involves improving • Continue to implement and support For dependent users, reducing and/
community understanding and well-planned social marketing or ceasing the use of drugs can help
awareness of the drugs being used, campaigns that address the risks them to lead more stable, healthy and
their effects, the harms associated of alcohol, tobacco and other drug productive lives.
with their misuse and the choice of use, the risks of specific drug use
effective interventions and treatment. practices (such as injecting) and Successfully reducing the misuse
For some drugs, such as tobacco, promote healthy lifestyles and safer of alcohol, and the use of tobacco
cultural acceptance by a large portion drinking cultures, including targeted and other drugs requires a range of
of the population has been successfully approaches and local complementary approaches across the continuum of use,
challenged, contributing to a significant initiatives for different population from experimental to dependent use. It
reduction in use over many years. groups. is important to ensure that appropriate
Harmful alcohol consumption, on the • Use the internet and other media to treatment is available and accessible.
other hand, still remains a challenge. sustain and strengthen the provision Engaging the support of family and
of credible and accurate information friends for those seeking treatment is an
There is an increased risk of harms
about alcohol, tobacco and other important part of helping people reduce
associated with the early uptake of
drugs to target particular population their drug use.
drugs. The earlier a person commences
use, especially heavy use, the greater groups. Brief interventions can also be very
their risk of harm in the short and longer • Limit or prevent exposure to alcohol effective. Brief interventions aim to
term (such as mental and physical health and tobacco advertising, promotion identify current or potential problems
problems) and the greater their risk of and sponsorship through regulation with drug use and motivate those at
continued drug use. and, where appropriate, voluntary risk to change their behaviour. They can
and collaborative approaches with range from five minutes of brief advice
business. to 30 minutes of brief counselling. Brief
• Explore ways of influencing interventions are commonly delivered
responsible media reporting and by general practitioners and alcohol and
portrayal of alcohol, tobacco and other drug workers, but can also be used
other drug use. by other service providers, police officers,
• Support community-based initiatives, mental health workers, nurses or family
including in Indigenous communities, members.
to change the culture of smoking,
harmful alcohol use and other drug
use.
• Improve the application of evidence-
based whole-of-school drug
education policies and programs.
10 NATIONAL DRUG STRATEGY 2010–2015In instances of dependence, it is Actions Objective 3:
important for people to have access • Build on efforts to increase the range Support people to recover from
to effective and affordable treatment of, access to and links between dependence and reconnect with
services and where needed, support for evidence-based treatment and other the community
rebuilding their lives and reconnecting support services. Recovering from drug dependence
with the community. Evidence • Sustain efforts to increase access to can be a long-term process in
supports the effectiveness of a range a greater range of culturally-sensitive which individuals need support and
of appropriately targeted treatment services. empowerment to achieve independence,
approaches. However, people can find it • Improve access to screening and a healthy self-esteem and a meaningful
difficult to locate and access the service targeted interventions for at-risk life in the community. Successful support
that meets their needs and people with groups such as young people, people for longer-term recovery after treatment
multiple and complex needs have the living in rural and remote communities, requires strategies that are focused on
added difficulty of finding a number of pregnant women and Aboriginal and the whole individual and look across the
different, sometimes unrelated, services Torres Strait Islander peoples. life span.
in a timely way. • Increase the community’s
understanding of effective drug While different people will have different
A range of appropriate, specialised routes to recovery, support for recovery
interventions by providing factual,
services should be available to anyone is most effective when the individual’s
credible information.
with a drug-related problem, irrespective needs are placed at the centre of their
• Continue efforts in diverting people
of personal history, circumstances or care and treatment. Treatment service
from traditional criminal justice
socioeconomic status. A ‘no wrong door’ providers can help individuals recover
pathways by providing information
approach should be adopted so that from drug dependence, help the
and/or referring them to assessment
people are provided with, or are guided individual access the internal resources
and treatment.
to, appropriate services regardless of they need (such as resilience, coping
• Increase awareness, availability and
where they enter the system of care. skills and physical health) and ensure
appropriateness of evidence-based
Generalist health care and social welfare telephone and internet counselling referral and links to a range of external
services should also notice, assess and and information services. services and support (such as stable
respond to people with alcohol, tobacco • Strengthen the capacity of the accommodation, education, vocational
and other drug-related problems. primary healthcare system to manage and employment support and social
There is a range of brief interventions, prevention, early intervention and connections).
for example, that can be delivered by treatment of tobacco use and harmful In maintaining and strengthening the
generalist services or over the internet. alcohol use. current system of treatment and other
These could refer people to specialised • Develop planning models for treatment support services across jurisdictions,
services where necessary or provide services that anticipate needs. the following principles will be continued
support before harms and long-term • Develop and implement quality under the National Drug Strategy:
dependence occur. frameworks for treatment services. • In designing treatment services, it
• Create incentives for people who is important to recognise that drug
misuse drugs or are dependent to users are not a homogenous group.
access effective treatment and to Treatment services should incorporate
make healthier choices. a principle of consumer involvement
• Encourage family members to access in planning and operations. Treatment
and make use of support services to interventions should also be tailored
help improve treatment outcomes for to the varying needs of individuals
clients. (including the potential for access to
• Explore and develop opportunities in substance-specific treatment and
the criminal justice system, including services).
correctional services, to assist drug
users through education, treatment
and rehabilitation services.
NATIONAL DRUG STRATEGY 2010–2015 11• In designing and coordinating referral Actions • Identify and link the necessary
pathways, it is important to recognise • Develop new evidence-based national services to provide those affected by
that trigger points for entry into planning tools to help jurisdictions drug use and dependence, such as
treatment come from a broad range better estimate the need and demand family members, children and friends,
of sources which should be reflected for alcohol and other drug health with ongoing support including links to
in those pathways. These include services across Australia. This should child welfare and protection services.
through alcohol and other drug include the full spectrum of services • Move towards a nationally consistent
diversion programs and links with from prevention and early intervention approach for non-government
primary health care. to the most intensive forms of care, treatment services including
• In designing and coordinating support and a range of services across the quality frameworks and reporting
after treatment to help individuals life span. requirements.
rebuild their lives and reconnect • Develop a set of national clinical • Develop a sustained and
with the community, it is important standards for alcohol and other drug comprehensive stigma reduction
to recognise that individuals often treatment services. strategy to improve community and
become marginalised or socially • Improve the links and coordination service understanding and attitudes
isolated as a result of their drug use, between primary health care and towards drug dependence, help
losing touch with their families and specialist alcohol and other drug seeking and the related problems
friends as well as opportunities for treatment services to enhance the of individuals.
education, vocational, employment, capacity to deal with all health needs • Improve links and coordination
housing and other areas of social and to facilitate the earlier identification between health, education,
participation. Furthermore, all services of health problems and access to employment, housing and other
need to work together to reduce treatment. sectors to expand the capacity
stigma attached to seeking treatment. • Improve the communication and flow to effectively link individuals from
Drug treatment alone cannot solve of information between primary care treatment to the support required
these problems which, if not dealt and specialist providers, and between for them to reconnect with the
with, can place an individual at risk clinical and community support community.
of relapsing to drug use and related services to promote continuity of care
issues. Consequently, it is important and the development of cooperative
that treatment services are linked service models.
to a broader range of services able • Investigate appropriate structures that
to provide these supports and the could be developed to help engage
necessary relationships and processes families and other carers in treatment
developed to better ensure these links pathways and ensure that information
are effective. about the pathways is readily
accessible and culturally relevant.
12 NATIONAL DRUG STRATEGY 2010–2015Objective 4: Actions
• Support whole-of-government and
Pillar 2: Supply
Support efforts to promote social
inclusion and resilient individuals, whole-of-community efforts to build reduction
families and communities parenting and family capacity, creating
communities that support the positive Supply-reduction strategies are directed
Socially inclusive communities and toward enforcing the prohibition of illegal
resilient individuals and families are development of children. This may
include evidence-based approaches drugs and regulating and enforcing
less likely to engage in harmful drug access to legal drugs, including alcohol,
use. Resilient individuals can adapt to to drug prevention in schools.
• Continue to implement skills training tobacco, pharmaceuticals and other
changes and negative events more easily drugs. In the case of illegal drugs,
and reduce the impacts that stressors to provide individuals with coping skills
to face situations that can lead to risky supply-reduction activities, including both
have on their lives—and are less likely border and domestic policing, extend to
to use drugs. behaviour including harmful drug use.
• Implement preventive support controlling the availability of precursor
Resilient and inclusive communities are programs targeting life transition chemicals and equipment used for
characterised by strong social networks points—primary to secondary manufacturing drugs. It also extends to
and work together to support individuals school, secondary school to tertiary compliance with Australia’s obligations
who need assistance. They also promote education, school to work and prison under international drug control treaties.
safe and healthy lifestyles. Supportive to community—to help individuals Reducing the supply of drugs requires
and informed families and communities develop the skills to manage the the collaborative participation of all levels
can prevent the uptake of drug use, next stage of life. of government including law enforcement
identify drug use in its early stages and • Support efforts to encourage and the health sector (public and private),
help individuals access and maintain participation of at-risk groups in industry and regulatory authorities.
treatment. A resilient community will community life including recreational,
support people to avoid relapse and help sporting and cultural activities. It also requires engaging the Australian
them reconnect with the community. • Provide support services to parents community and their support for these
in recovery to ensure the needs of strategies. The message must be clear
Responsibility for building resilient that the supply and use of illegal drugs
communities lies at all levels—from dependent children are met.
and the illegal supply and misuse of
governments, to communities, non- tobacco, alcohol, pharmaceuticals and
government organisations, families other legal drugs is not acceptable.
and individuals.
For alcohol, tobacco, pharmaceuticals
and other legal drugs, government
authorities, and community and business
organisations need to collaborate to
regulate access to these drugs based
on community expectations and
standards, and the costs and benefits
of their use. For alcohol, this means that
liquor licensing, planning authorities,
local government, licensed venues and
retailers need to be involved. Parents and
families also have a role in reducing the
supply of alcohol to minors. A wide range
of businesses and retailers need to be
involved in regulatory and collaborative
approaches to reducing harms from
alcohol.
NATIONAL DRUG STRATEGY 2010–2015 13For tobacco, the involvement of Objective 1: Actions
retailers is essential. For pharmaceutical Reduce the supply of illegal drugs • Prevent the importation of illegal drugs
drugs, doctors and pharmacists (both current and emerging) and control the legitimate trade of
need to be consulted and involved in Reducing the supply of illegal drugs equipment and chemicals used in their
supply-reduction strategies to reduce requires activity at Australia’s borders manufacture.
pharmaceutical misuse. Retailers of to prevent and disrupt importations of • Increase and improve enforcement
other substances (such as inhalants) are illegal drugs and their precursors and targeting cultivation, manufacture and
essential partners in the regulation and within Australia to prevent cultivation, trafficking of illegal drugs, including the
enforcement of supply. manufacture and distribution of illegal financial proceeds arising from these
drugs. Legislative frameworks exist and activities.
For illegal drugs, law enforcement
require constant enforcement to ensure a • Improve powers of detection through
strategies are needed which target all
reduction in the supply of illegal drugs. supportive technology (and systems),
parts of the supply chain from actions
access to relevant information and
aimed at preventing importation across These frameworks need to be supported workforce development.
the border to those that target the point by demand-reduction strategies which • Strengthen collaboration between law
of supply to consumers. The increasing engage the health sector and community enforcement, industry and relevant
prevalence in the use of the internet and raise awareness of the harms and agencies to prevent the diversion
to facilitate the global supply of illegal consequences arising from illegal drug of precursor chemicals into the
drugs—particularly those marked as use. manufacture of illegal drugs.
‘party pills’ and ‘legal highs’—also needs
Border activities are crucial in controlling • Improve cooperation and collaboration
to be considered in these strategies.
the importation of illegal drugs and between law enforcement agencies,
Communities—not only in metropolitan
Australia must continue to develop especially with respect to information
areas but also in rural and remote areas
strong international partnerships and and intelligence access and exchange.
and Aboriginal and Torres Strait Islander
help strengthen the capability of our • Develop closer relationships with
communities—have an important role to
international partners, particularly in international partner agencies and
play in not tolerating illegal drug supply
the Asia-Pacific region, to manage bodies and enhance Australia’s
and helping law enforcement to combat
borders. It is important too that Australia national approach to implementing its
this.
continues to participate in international obligations under international drug
There is a strong connection between law enforcement activities, such as those control treaties.
the supply of illegal drugs and the illegal coordinated by the United Nations Office • Build on Australia’s capacity to use
supply of legal drugs because of the on Drugs and Crime. the border as a significant choke point
financial proceeds that arise from such for the supply of illegal drugs into
activities. Therefore the disruption of The illicit drug market is not only Australia through promoting nationally
organised crime and money laundering constrained by international borders. consistent drug control laws, which
is an important component of any drug Information sharing and coordinated would also limit the opportunity for
supply-reduction strategy. The disruption approaches are needed to stem the organised crime to exploit legislative
and dismantling of organised crime supply of illicit drugs at all stages from inconsistencies.
is a high priority for governments as the supply chain from overseas suppliers, • Ensure the ongoing and timely review
reflected in the Australian Government’s interception at the border (jurisdictional of legislation and regulation to reflect
Commonwealth Organised Crime and international) and investigation and the dynamic nature of illegal drug
Strategic Framework. prosecution of domestic producers, markets and manufacture.
manufacturers and suppliers. • Research, investigate and gather
information on all aspects of drug
supply markets including identifying
emerging drugs and manufacturing
techniques to properly inform law
enforcement responses.
• Foster research and development in
technological innovation to provide
investigative tools for use in the
disruption of the supply markets.
14 NATIONAL DRUG STRATEGY 2010–2015You can also read