NATIONAL ASTHMA STRATEGY 2018 - National Asthma Council Australia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

NATIONAL ASTHMA STRATEGY 2018

© Commonwealth of Australia as represented by the Department of Health 2017
Title: National Asthma Strategy 2018
ISBN: 978-1-76007-338-1
Online ISBN: 978-1-76007-337-4
Publications Number: 11983
Creative Commons Licence
This publication is licensed under the Creative Commons Attribution 4.0 International Public License available from
https://creativecommons.org/licenses/by/4.0/legalcode (“Licence”). You must read and understand the Licence before
using any material from this publication.
Restrictions
The Licence may not give you all the permissions necessary for your intended use. For example, other rights (such as
publicity, privacy and moral rights) may limit how you use the material found in this publication.
The Licence does not cover, and there is no permission given for, use of any of the following material found in this
publication:
the Commonwealth Coat of Arms. (by way of information, the terms under which the Coat of Arms may be used
can be found on the Department of Prime Minister and Cabinet website http://www.dpmc.gov.au/government/
commonwealth-coat-arms);
any logos and trademarks;
any photographs and images;
any signatures; and
any material belonging to third parties. The third party elements must be included here or have a footnote reference
throughout the document showing where they are
Attribution
Without limiting your obligations under the Licence, the Department of Health requests that you attribute this publication
in your work. Any reasonable form of words may be used provided that you:
include a reference to this publication and where, practicable, the relevant page numbers;
make it clear that you have permission to use the material under the Creative Commons Attribution 4.0 International
Public License;
make it clear whether or not you have changed the material used from this publication;
include a copyright notice in relation to the material used. In the case of no change to the material, the words “©
Commonwealth of Australia (Department of Health) 2018” may be used. In the case where the material has been
changed or adapted, the words: “Based on Commonwealth of Australia (Department of Health) material” may be
used; and
do not suggest that the Department of Health endorses you or your use of the material.
Enquiries
Enquiries regarding any other use of this publication should be addressed to the Branch Manager, Communication
Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to copyright@health.gov.au
NATIONAL ASTHMA STRATEGY 2018 Development of the National Asthma Strategy 2018 was led by the National Asthma Council Australia, in partnership with Asthma Australia and with funding from the Australian Government Department of Health.
Contents
Foreword.............................................................................................. 1 Objective 5:
Promote research, evidence and data.................................. 16
Executive Summary.......................................................................... 2
Monitoring progress..................................................................... 17
Introduction......................................................................................... 3
Acknowledgements....................................................................... 18
The approach...................................................................................... 4
Appendix 1:
Asthma policy context................................................................. 20
The challenge of asthma................................................................ 6
Appendix 2:
Objective 1:
Health, social and economic impacts of asthma.............. 22
Support effective self-management practices.................. 10
Appendix 3:
Objective 2:
Key challenges facing asthma.................................................. 27
Develop the health professional workforce........................ 11
References........................................................................................ 30
Objective 3:
Enhance asthma care and management.............................. 13
Objective 4:
Create supportive community environments.................... 14NATIONAL ASTHMA STRATEGY 2018
Foreword
The National Asthma Strategy 2018 (the Strategy) improving patient quality of life, and reducing asthma
builds on the considerable progress made in asthma over morbidity and its associated costs.
the past three decades and leverages our strengths as a
Development of the Strategy is also occurring at a
nation to continue to address the impact which asthma
time of other significant reforms taking place within
– one of Australia’s most widespread chronic health
the Australian health care system. The results of these
conditions – is having on the community.
reforms are likely to affect any future roll-out of activity
Aligned with the National Strategic Framework for associated with the Strategy.
Chronic Conditions, and the Implementation Plan for
The Strategy is underpinned by a whole-of-system
the National Aboriginal and Torres Strait Islander Health
approach that has the person with asthma and their
Plan 2013-2023, the Strategy outlines a targeted and
caregivers at the centre.
comprehensive approach to optimise asthma diagnosis
and management. With an emphasis on Aboriginal Support for research into the causes of asthma and
and Torres Strait Islander people and other priority finding a cure is an integral component of the Strategy.
populations, the Strategy focuses on areas where the
The Strategy aims to significantly reduce the impact of
biggest gaps between evidence and practice lie, and
asthma and other chronic conditions on individuals, the
where the potential for impact is greatest. Increasing the
community and the economy, and take Australia to the
uptake of asthma action plans for adults and children
next stage of improvement in asthma outcomes.
is a focus, as we strive to achieve the biggest gains in
Dr Jonathan Burdon AM Dr Simon Bowler
Chairman Chairman, Medical and Scientific Advisory
National Asthma Council Australia Committee
Asthma Australia
nationalasthma.org.au/strategy 1NATIONAL ASTHMA STRATEGY 2018
Executive Summary
The National Asthma Strategy 2018 (the Strategy) aims The objectives fall under a number of guiding principles
to outline Australia’s national response to asthma and which will help to align and focus effort. These guiding
inform how existing limited health care resources can principles need to be incorporated into any future action
be better coordinated and targeted across all levels of to address asthma.
government. This Strategy identifies the most effective
Enabling factors which influence the ability to achieve
and appropriate interventions to reduce the impact
the objectives include governance and leadership, health
of asthma in the community and continue to be an
workforce, health literacy, research, data and information,
international leader in asthma prevention, management
technology and resources.
and research.
This Strategy responds to the unique challenges of
Overcoming the many barriers to improving asthma
asthma in Australia. Asthma is one of the most common
diagnosis and management requires a multi-sectoral
chronic conditions in Australia, with prevalence and
response that has the person with asthma and their
mortality rates that are high by international comparison.
caregivers at the centre. This Strategy provides guidance
Asthma remains a significant cause of ill health,
for collaborative efforts by governments and other parts
disability and poor quality of life in Australia. As is the
of the community, including people with asthma, health
case with many chronic conditions, asthma is markedly
care professionals, non-government organisations,
overrepresented in the Aboriginal and Torres Strait
researchers, families, carers, communities and industry,
Islander population.
to improve asthma control and patient quality of life and
reduce asthma morbidity and its associated costs and Australia is a world leader in the asthma field and an
further reduce asthma mortality. active member of the global asthma community. This
Strategy builds on the considerable progress that
The goal of the Strategy is to reduce the health, social
Australia has made in asthma over recent decades and
and economic impacts of asthma with a targeted and
builds on our strengths as a nation in order to realise
comprehensive approach to optimise asthma diagnosis
further improvements in asthma outcomes.
and management, including within the Aboriginal and
Torres Strait Islander population and other priority The National Asthma Council Australia led the
populations. To achieve this, the Strategy outlines five development of this Strategy, in partnership with
high-level objectives with potential areas for action. While Asthma Australia, and with funding from the Australian
the Strategy is not an action plan and does not mandate Government Department of Health. This Strategy has
any specific activities, it does include potential initiatives been informed by the expert advice of the National
that may be considered by governments and health Asthma Strategy Advisory Group and consultations with
organisations in planning any future action relating to key stakeholders and the community.
asthma and other chronic respiratory conditions.
This Strategy was developed in consultation with state
and territory jurisdictions via the Community Care and
The five objectives of this Strategy are: Population Health Principal Committee, the National
Aboriginal and Torres Strait Islander Health Standing
1. Support effective self-management practices Committee, the Australian Health Ministers’ Advisory
2. Develop the health professional workforce Council) and the Council of Australian Governments.
3. Enhance asthma care and management Future action to address asthma will involve collaboration
4. Create supportive community environments with stakeholders across all levels of governments, the
5. Promote research, evidence and data. health sector and relevant organisations.
2 nationalasthma.org.au/strategyNATIONAL ASTHMA STRATEGY 2018
Introduction
The National Asthma Strategy 2018 (the Strategy) is an asthma and the conditions that exist alongside asthma
opportunity to articulate a shared goal for reducing the and which can affect it.
impact of asthma on the community; identify effective,
Further, this Strategy also aligns with the Implementation
evidence-based priority areas for action; and maximise
Plan for the National Aboriginal and Torres Strait Islander
the efficient use of health care resources. This Strategy
Health Plan 2013-2023 – Domain One: Health System
aims to better coordinate health resources across all
Effectiveness (3), and international policies including
levels of government and to focus these resources where
the Global Action Plan for the Prevention and Control
they are needed most.
of Noncommunicable Diseases developed by the World
There is currently no cure for asthma. However, good Health Organization in 2013 (4), and the Global Strategy
management can control the disease and prevent for Asthma Management and Prevention developed
symptoms from occurring or worsening (1). by the Global Initiative for Asthma in 2016 (5). See
Appendix 1 for more information on the asthma policy
This Strategy focuses on improving asthma control in
context.
people with asthma, as this is where the biggest gap
between evidence and practice lies, and where the The health care system is subject to ongoing national
potential for reducing the impact of asthma is greatest. reform, such as the establishment of Primary Health
Best practice asthma care is both effective and efficient. Networks, redevelopment of the My Health Record,
By optimising asthma diagnosis and management, and the Healthier Medicare Initiative. Future action to
significant gains can be achieved in patient quality of address asthma will be informed by this work.
life and substantial reductions in asthma morbidity and
The Strategy is not an action plan. The Strategy does
associated costs.
incorporate examples of initiatives that could be
In terms of prevention, the emphasis of the Strategy is undertaken in order to drive improvements in the
on the reduction of asthma risk across the life course, treatment and management of persons affected by
and timely and appropriate asthma diagnosis and asthma, however, the introduction of any of these
management (secondary and tertiary prevention only). measures is not mandated and would require the support
The Strategy aims to strengthen the evidence base and agreement of jurisdictions to implement.
for asthma prevention as there is currently no reliable
evidence for effective interventions to prevent the onset
of asthma (primary prevention) (1). In accordance with Purpose
this focus on secondary and tertiary prevention, the
Strategy often refers to people with asthma as patients. This Strategy supersedes previous national asthma
strategies (6-8) as the overarching strategy to reduce
Asthma affects all Australians, but some populations are the impact of asthma in Australia. The Strategy 2018
disproportionally affected. The Strategy includes a strong sets out the strategic directions and key actions for a
emphasis on improving asthma control in the Aboriginal coordinated national response to asthma diagnosis and
and Torres Strait Islander population and other priority management. As a national strategy for a specific chronic
populations. condition, the Strategy has been designed to align with,
This Strategy is also an opportunity to align with policies and support, the policy directions in the Framework (2),
at the jurisdictional, national and international levels. which provides the overarching national policy for the
It is expected that jurisdictional and regional health prevention and management of chronic conditions in
policies to address asthma will evidence links between Australia.
local policy, priorities and outcomes and this national
Strategy.
Audience
At a national level there is considerable focus on the
prevention and management of chronic conditions. This Strategy has been developed for policy makers at
This Strategy has been designed to align with, and all levels of government, non-government organisations
support, the policy directions in the National Strategic such as national peak bodies, stakeholder organisations,
Framework for Chronic Conditions (the Framework) (2), researchers and health professionals who advocate for
which provides the overarching national policy for the and provide asthma care.
prevention and management of chronic conditions in
Australia. Asthma often occurs alongside (and shares
risk factors with) other chronic conditions. Potential
initiatives in this Strategy aim to improve outcomes for
nationalasthma.org.au/strategy 3NATIONAL ASTHMA STRATEGY 2018
The approach
The Strategy articulates a goal supported by five high- Enablers
level objectives. Each objective contains potential areas
for action informed by the expert advice of the National In line with the Framework (2), this Strategy draws on
Asthma Strategy Advisory Group and consultations with seven enablers that will assist in achieving the goal of
key stakeholders and the community. this Strategy:
This Strategy includes principles to guide action within Governance and leadership – supports evidence-
the objectives and common enablers to achieve them. based shared decision-making and encourages
The enablers represent cross-cutting themes that will collaboration to enhance health system performance.
strengthen efforts across each of the objectives. Health workforce – a suitably trained, resourced and
distributed workforce is supported to work to its full
scope of practice and is responsive to change.
Goal Health literacy – people are supported to understand
To reduce the health, social and economic impacts of information about health and health care, to apply
asthma with a targeted and comprehensive approach to that information to their lives and to use it to make
optimise asthma diagnosis and management. decisions and take actions relating to their health.
Research – quality health research accompanied
by the translation of research into practice and
Principles knowledge exchange strengthens the evidence base
In line with the Framework (2), this Strategy is and improves health outcomes.
underpinned by eight guiding principles. These principles Data and information – the use of consistent, quality
are expected to guide future action to address asthma data and real-time data sharing enables monitoring
and other chronic respiratory conditions. and quality improvement to achieve better health
Equity – all Australians, including Aboriginal and outcomes.
Torres Strait Islander people and other priority Technology – supports more effective and accessible
populations, receive culturally safe and appropriate, prevention and management strategies and offers
high quality health care. avenues for new and improved technologically driven
Collaboration and partnerships – identify linkages initiatives.
and act upon opportunities to cooperate and partner
Resources – adequate allocation, appropriate
responsibly to achieve greater impacts than can occur
distribution and efficient use of resources, including
in isolation.
funding, to address identified health needs over the
Access – high standard, appropriate support and long-term (2).
services are available, accessible and affordable for all
Australians. The table below lists the components of this Strategy.
Evidence-based – rigorous, relevant and current
evidence informs best practice and strengthens the
knowledge base to effectively prevent and manage
asthma and other chronic conditions.
Person-centred approaches – the health system
is shaped to recognise and value the needs of
individuals, their carers and their families, to provide
holistic care and support.
Sustainability – strategic planning and responsible
management of resources delivers long-term
improved health outcomes.
Accountability and transparency – decisions and
responsibilities are clear and accountable, and achieve
best value with public resources.
Shared responsibility – all parties understand, accept
and fulfil their roles and responsibilities to ensure
enhanced health outcomes for all Australians (2).
4 nationalasthma.org.au/strategyNATIONAL ASTHMA STRATEGY 2018
Table 1: Components of the Australian National Asthma Strategy 2018
Goal
To reduce the health, social and economic impacts of asthma with a targeted and comprehensive approach to optimise
asthma diagnosis and management.
Principles
Equity for all Australians – including Aboriginal and Torres Strait Islander people
Collaboration and partnerships
Access
Evidence-based
Person-centred approaches
Sustainability
Accountability and transparency
Shared responsibility
Objectives
1. To support effective self-management practices through increasing patient knowledge, confidence and skills
2. To ensure consistent, best practice asthma care through improving health professional adherence to treatment
guidelines for asthma diagnosis and management
3. To enhance asthma care and management by creating an integrated, equitable and accessible health care system
4. To promote health and reduce asthma risk through supportive community environments
5. To improve asthma prevention, diagnosis and management through increased support for research, evidence and
data
Enablers
Factors which influence the ability to achieve success such as governance and leadership, health workforce, health
literacy, research, data and information, technology and resources.
nationalasthma.org.au/strategy 5NATIONAL ASTHMA STRATEGY 2018
The challenge of asthma
Asthma defined Additional chronic conditions that are commonly found
in people with asthma, and that can impact on asthma,
Asthma is a common, chronic respiratory disease. include allergic rhinitis, obesity, obstructive sleep
People with asthma experience episodes of wheezing, apnoea, nasal polyps (soft, painless, non-cancerous
breathlessness and chest tightness due to widespread growths) and gastro-oesophageal reflux disease (10).
narrowing of the airways.
Asthma affects people of all ages; however, many of the
The symptoms of asthma are usually reversible, either people with asthma and comorbid conditions are older
spontaneously or with treatment, and may sometimes be Australians, reflecting the fact that chronic conditions are
absent for weeks or months at a time. On the other hand, more prevalent in older age groups (10). Older people
asthma can have a severe adverse impact on quality with asthma often suffer from more than one chronic
of life, and patients can experience episodic flare-ups respiratory condition as well as experiencing acute
(exacerbations) of asthma that may be life-threatening respiratory conditions.
(5, 9).
Approximately 15–20% of people with a diagnosis of
The underlying causes of asthma are still not asthma or COPD have both conditions (11). People with
well understood, although there is evidence that both asthma and COPD experience significantly worse
environmental and lifestyle factors, as well as genetic health outcomes than those with asthma or COPD alone
factors such as an allergic tendency, increase the risk of (12).
developing asthma (9).
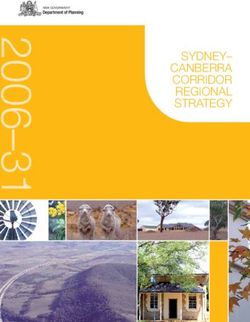
The conditions that may affect asthma are presented in
There is currently no reliable evidence for effective Figure 1 (1).
interventions to prevent the onset of asthma, and no cure
for asthma (1). However, good management can control Asthma shares a number of risk factors with other
the disease and prevent symptoms from occurring or chronic conditions. Modifiable risk factors for asthma
worsening. include tobacco use, exposure to environmental hazards,
being overweight and/or obese and a sedentary lifestyle
Asthma is one of several chronic conditions that are (9, 13). Evidence is emerging that thunderstorms may
prevalent in Australia but, unlike most other chronic trigger asthma in people who have never experienced
conditions such as arthritis or cardiovascular disease, it asthma before, particularly among people with a history
is not progressive – that is, it does not typically worsen of hay fever and rye grass allergy (14-17).
with increasing age (9).
The impact of asthma
Comorbid conditions
Asthma is one of the most common chronic conditions
Asthma commonly coexists with other chronic in Australia, with prevalence rates that are high by
conditions. According to the Australian Health Survey international comparison (9). In 2016, it was estimated
2011–12, 57.5% of people with asthma had another that 10.8% of the population had asthma – that is,
chronic condition, and nearly 30% had two or more around one in ten Australians (10).
chronic conditions (10).
Despite asthma affecting around 2.5 million Australians,
The presence of one or more comorbid conditions in there is a widespread misperception that it is no longer
people with asthma is likely to compromise their quality a problem in Australia, especially following the marked
of life and may complicate the management of asthma. decrease in asthma mortality from its peak in the late
People with asthma have a higher prevalence of: 1980s (18).
Arthritis The Australian Burden of Disease Study 2011 (19),
Back problems however, illustrates that improvements are still needed
Cancer in order to ensure improved health outcomes for
Cardiovascular disease/diseases of the circulatory Australians affected by asthma. In 2011, asthma was
system (CVD) the 11th largest cause of disability adjusted life years
(DALYs) and the 5th leading cause of non-fatal disease
Chronic obstructive pulmonary disease (COPD)
burden, being responsible for around 100,000 years
Diabetes lived with a disability (YLDs) (19).
Mental health problems (10).
6 nationalasthma.org.au/strategyNATIONAL ASTHMA STRATEGY 2018
Figure 1: Conditions that may affect asthma symptom control, risk or management (25)
Rhinitis
(allergic and non-allergic)
Upper airway dysfunction
Chronic sinusitis
Hyperventilation
GORD Mental illness
Obesity ASTHMA Smoking GORD: gastro-oesophageal reflux disease;
Nicotine OSA: obstructive sleep apnoea;
OSA dependence COPD: chronic obstructive pulmonary disease
Hormonal changes COPD
Other allergic conditions Respiratory
infections
Other respiratory
conditions
outcomes based on its past progress and current
Asthma remains a significant cause of ill health, strengths which include:
disability and poor quality of life in Australia.
World-leading treatment guidelines – Australian
Around 2.5 million Australians have asthma, and
Asthma Handbook (1)
poor control of this chronic condition is common.
Availability of effective therapies and adoption of
different management strategies
In 2015, there were 421 deaths due to asthma, which is Government commitment and ongoing funding since
high by international standards (9, 20). 2001
People with chronic conditions, such as asthma, World-leading asthma researchers and health
experience a significant burden associated with the professionals
treatment of their condition and are also affected by Strong stakeholder coordination and collaboration
psychosocial issues (21). Asthma has a long-term impact
Strong research and data collection activities,
on quality of life, and people with asthma may live for a
including by AIHW’s National Centre for Monitoring
long period of time with its associated disability (22).
Asthma and Other Chronic Respiratory Conditions and
It is difficult to estimate the total economic and social the Australian Centre for Airways disease Monitoring
impact of asthma. The total annual costs of asthma, A rigorously developed set of 10 national asthma
including indirect costs such as lost productivity, indicators that are feasible for population-level
were calculated in a recent report by Deloitte Access monitoring
Economics as $27.9 billion (23).
Comprehensive, evidence-based strategies to
More information on the health, social and economic coordinate national action on asthma since 1999
impacts of asthma is presented in Appendix 2. (6-8)
Models of asthma care and asthma action plan
ownership
Australia’s strengths and key challenges Innovations in digital health technology
Australia is a world leader in the asthma field and an Education programs for health professionals and
active member of the global asthma community. Asthma people with asthma
management in Australia has made considerable Community-based support services for people with
progress over recent decades, most notably the marked asthma
decrease in asthma mortality. Australia is in a strong
position to realise further improvements in asthma Universal health insurance through Medicare.
nationalasthma.org.au/strategy 7NATIONAL ASTHMA STRATEGY 2018
While there is currently no cure for asthma, there are guidelines, the Australian Asthma Handbook, despite high
effective management strategies available to control the awareness of the guidelines (9, 24-29).
disease and prevent the worsening of asthma symptoms,
More information on the key challenges facing asthma
such as uptake of asthma action plans (1). However,
in Australia, and the broader international context, is
uptake of effective self-management practices is seldom
presented in Appendix 3.
reported by patients and there is evidence of health
professional non-adherence to best practice treatment
guidelines (9, 18, 24-29).
Aboriginal and Torres Strait Islander
Most asthma is mild, and can be well-controlled people and other priority populations
with regular low dose preventer (anti-inflammatory)
treatment, but many people with asthma do not take Asthma affects all Australians, but some populations are
this, or do not take it regularly (9, 24, 30). Uncontrolled disproportionally affected. These populations experience
asthma carries the risk of permanent loss of lung a higher prevalence of asthma and a greater burden of
function, persistent symptoms and acute attacks or flare- disease, resulting in inequitable health outcomes. Due
ups (9). to the disparity in health outcomes, equal focus is not
sufficient: greater investment and sustained efforts are
People with asthma often treat their asthma as an required to positively advantage priority populations and
acute condition rather than a chronic condition, using overcome current inequalities in asthma outcomes (2).
medication to relieve symptoms with a short-acting
reliever rather than to avoid symptoms occurring The Strategy focuses on improving asthma control in
with a preventer (31). Suboptimal asthma control people with asthma (secondary and tertiary prevention),
is a critical issue in Australia. Poor asthma control as this is where the biggest gap between evidence
(frequent symptoms and/or flare-ups) is common in both and practice lies, and where the potential for impact is
adults and children: for half of the people with asthma, greatest. The Strategy includes a strong emphasis on
there is a gap between the potential control of their improving asthma control in high risk and vulnerable
asthma symptoms and the level of symptoms currently populations, while maintaining good practice in other
experienced (18). population groups.
Overall, levels of asthma symptoms and frequency Aboriginal and Torres Strait Islander people
of dispensing reliever medication in the Australian
community are higher than is consistent with good As is the case with many chronic conditions, asthma
asthma control (31). is markedly overrepresented in the Aboriginal and
Torres Strait Islander population. In 2012-13, 18% of
There is great opportunity to realise effective change Aboriginal and Torres Strait Islander Australians had
for asthma, as it is a common chronic condition with asthma (an estimated 111,900 people), meaning that
clearly defined interventions that can reduce its impact prevalence of the condition was almost twice as high as
on individuals and the community (9). Evidence-based for the non-Indigenous population (34).
effective strategies are available to address patient
factors such as medication adherence, correct inhaler Asthma was 33% more common among 0-14 year olds
technique, use of asthma action plans and understanding and 58% more common among 15-24 year olds in the
asthma triggers. Similarly, health professionals need Aboriginal and Torres Strait Islander population, as it
to work in partnership with patients to conduct regular was among the general Australian population. Identifying
reviews, prescribe appropriate medications, update and effectively addressing asthma among Aboriginal and
asthma action plans, and assist patients to use their Torres Strait Islander children carries extra importance,
inhalers correctly (1). as health inequalities in the Indigenous population begin
prior to birth, and continue through early childhood,
Innovation in digital health technology and more significantly increasing the prospects of illness, poor
integrated health care systems are likely to transform health and premature death for this population compared
asthma care and ease pressure on the healthcare system with the non-Indigenous population (35).
by reducing routine GP appointments and enabling
people to manage their own condition (32). The disparity in prevalence rates is even more stark
when older age cohorts are compared, with Aboriginal
However, a proactive approach towards asthma self- and Torres Strait Islander people aged 45 years and over
management is seldom reported by patients, with experiencing rates of asthma that were approximately
many experiencing daily symptoms, struggling with double the rate experienced by this age cohort in the
medication use and adherence, and feeling ill-informed general population (34, 35).
and disempowered about their condition (18, 31,
33). Similarly, there is evidence of health professional Continuing this theme, asthma mortality rates are
non-adherence to Australia’s best practice treatment substantially higher among Aboriginal and Torres Strait
8 nationalasthma.org.au/strategyNATIONAL ASTHMA STRATEGY 2018
Islander Australians compared with non-Indigenous Awareness that disease co-morbidity is commonly
Australians. During the period from 2007 to 2011, experienced by Aboriginal and Torres Strait Islander
the mortality rate for asthma among Aboriginal and people, which increases the need for, and likely
Torres Strait Islander Australians was 4.0 per 100,000 effectiveness of, cross-disease approaches to
population, which was 2.3 times that of non-Indigenous treatment and management, where appropriate.
Australians (1.7 per 100,000) (36).
Other groups disproportionally affected by asthma
The Aboriginal and Torres Strait Islander Burden of Disease
Study, provides further evidence of the impact being Amongst people who have asthma, some populations
wrought upon the Indigenous population by asthma. In are at greater risk of poor outcomes. Children are much
2011, asthma was the 8th largest cause of disability more likely than adults to be hospitalised for asthma.
adjusted life years (DALYs) and the 5th leading cause of Over the last few decades, asthma management in
non-fatal disease burden, being responsible for around younger age groups has improved greatly so there are
5,802 years lived with a disability (YLDs) (37). now few deaths. Conversely, older people with asthma
are at higher risk of dying from asthma than younger
Addressing asthma in the Aboriginal and Torres Strait people, and often have comorbidities (9).
Islander population
In 2014-15, asthma was more common among people
While Aboriginal and Torres Strait Islander people are living in areas of lower socioeconomic status (13%)
a priority population due to their overrepresentation in compared with those in areas of higher socioeconomic
the asthma data, it is expected that – given the broad status (10%) (38).
national nature of the Strategy – issues relating to this
There is evidence of a widening gap in the prevalence
population cohort will be addressed, where possible, in
of asthma across socioeconomic groups, suggesting
any actions undertaken for each of the five priority areas
that asthma is shifting from a condition more prevalent
outlined in the Strategy. This mirrors the approach taken
among the higher socioeconomic group to one more
by the Framework, which presents Aboriginal and Torres
strongly associated with socioeconomic disadvantage
Strait Islander people as a target priority population,
(9).
noting that extra consideration need be provided to this
group on account of the ‘disproportionate burden of People with asthma who have special considerations
chronic conditions’ it experiences (2). for diagnosis and management:
Any Aboriginal and Torres Strait Islander health specific Children and their parents/carers
action for asthma will need to take into account the range Adolescents and young adults
of mitigating factors that inhibit effective health service Pregnant women
provision to, and reinforce health inequalities for, this
Older Australians
disadvantaged population group. Prominent among these
People with asthma who face specific challenges with
mitigating factors are:
their condition and where the potential to improve
Understanding that Aboriginal and Torres Strait health outcomes and reduce costs is greatest:
Islander people will be more likely to frequent services
Are newly diagnosed
where Aboriginal and Torres Strait Islander workers
Have severe or poorly controlled asthma
are on staff.
Have complex and comorbid chronic conditions
Acknowledging that this population is more likely
to access care where provided locally and where Are frequent users of medical and health services.
provided in a culturally appropriate manner by In order to prevent asthma from developing in people
culturally aware staff, but such services are commonly who do not already have a diagnosis of asthma (primary
not available in rural and remote areas. prevention of asthma), a number of additional priority
Recognising that socioeconomic disadvantage populations exist. These include people without asthma
hinders access to required health services among the who may be at increased risk due to the presence of risk
general population, and that this disadvantage is more factors for asthma and other chronic conditions:
commonly experienced by Indigenous Australians. Smokers and people exposed to cigarette smoke,
Noting that Aboriginal and Torres Strait Islander including children and pregnant women
people are commonly adversely affected by social People exposed to environmental hazards and
determinants (e.g. healthy housing, employment, events (e.g. poor air quality/air pollution, bushfires,
education, food security, sanitation, etc.), which thunderstorms)
impact their capacity to access required services People who are overweight/obese
and treatment, and to maintain effective treatment
People who are sedentary
regimes.
People with allergic rhinitis.
nationalasthma.org.au/strategy 9NATIONAL ASTHMA STRATEGY 2018
Objective 1:
Support effective self-management practices
Effective self-management practices to control evaluation and improvement to be established to ensure
asthma symptoms and prevent flare-ups are known. awareness campaigns have a measurable impact.
These strategies include regular treatment with anti-
inflammatory medication, regular medical review, and 1.3 Provide information and support services
provision of support for people with asthma to self-
Continue to provide information and support services
regulate their asthma treatment and health related
for people with asthma, their carers and families, with a
behaviours. Effective self-management practices
focus on priority populations. Information and support
include self-monitoring of asthma symptoms and/or
services to be provided via accessible channels, with
lung function, presenting for regular medical review,
a nationally consistent approach tailored for the local
medication adherence, correct inhaler technique, uptake
situation.
of asthma action plans and understanding asthma
triggers.
1.4 Enhance asthma health literacy
The uptake of these strategies is not optimal among
Employ innovative approaches to enhance asthma health
people who could benefit greatly, in terms of reducing the
literacy, and support people with asthma, their carers
impact of asthma on both themselves and the community
and families to understand information about asthma, to
(9, 24, 30-31, 33). Supporting people with asthma to
apply that information to their lives and to use it to make
increase knowledge, confidence and skills for effective
decisions and take actions relating to their health.
self-management practices will empower them to play an
active role in their own health care, better control their Consider ways that people with asthma participate in
condition and lead full and active lives. Support should health care and employ approaches that build their
be tailored to the person with asthma and appropriate capacity to navigate the health care system and make
for their treatment regimen, asthma severity, culture, informed decisions about their asthma care, with a focus
language, literacy level and ability to self-manage (1). on priority populations.
Ongoing support of evidence-based patient interventions
that enhance self-management practices is critical. 1.5 Promote, provide and implement asthma
action plans
Actions Increase uptake of asthma action plans along with
1.1 Deliver education programs and skills training effective delivery which involves education in self-
monitoring, review of medicines and assessment of
Continue to deliver education programs that target severity. Explore approaches to maximise uptake of
people with asthma and their caregivers in order to written asthma action plans in different settings (e.g.
increase knowledge, confidence and skills, and drive schools) and through partnerships (e.g. health insurance
health behaviours that optimise asthma control and industry). Investigate actual use of asthma action plans
active engagement in health care and shared decision- including e-health adaptations.
making processes. Education programs to focus on
medication adherence, inhaler technique, risk reduction, 1.6 Promote, provide and implement asthma and
understanding asthma triggers and managing asthma anaphylaxis first aid protocols
alongside other conditions. Mechanisms for regular
evaluation and improvement to be established to ensure Increase awareness and use of asthma and anaphylaxis
education programs and skills training have a measurable first aid protocols. Explore approaches to maximise
impact. uptake of consistent, standard first aid protocols in
educational and other settings.
1.2 Deliver awareness campaigns
1.7 Explore innovative new adherence strategies
Deliver awareness campaigns that target people with
asthma and their caregivers to increase understanding of Explore new and emerging strategies and digital
asthma preventer medicines including costs. Awareness technologies to support self-management and active
campaigns would aim to increase the uptake of asthma engagement, with a focus on understanding and
action plans, enhance asthma health literacy and improving medication adherence and improving inhaler
address myths and misperceptions around appropriate technique. Investigate and adopt, at scale, the effective
self-management practices. Mechanisms for regular and validated use of technologies, such as telehealth and
medication reminder strategies.
10 nationalasthma.org.au/strategyNATIONAL ASTHMA STRATEGY 2018
Objective 2:
Develop the health professional workforce
Asthma care is provided by a number of different health priority population groups that are disproportionally
professionals within the health care system. This impacted by asthma, such as Aboriginal health
includes those working in primary health care (e.g. GPs, professionals and non-health professionals in Aboriginal
primary health care nurses, nurse practitioners, asthma community controlled organisations.
and respiratory educators, Aboriginal health workers,
pharmacists, and physiotherapists) and secondary care Actions
(e.g. hospital staff including emergency department staff,
generalist physicians and nurses, and specialists such as 2.1 Develop and implement a health workforce
respiratory physicians and allergists). plan to ensure people with asthma receive
patient-centred, multidisciplinary care
It is critical that a suitably trained, resourced and
distributed health workforce is supported to work Develop and implement a national health workforce plan
to its full scope of practice and is responsive to to ensure people with asthma receive person-centred,
change. Asthma is predominantly managed in primary multidisciplinary care that is delivered at the right time
health care by GPs, however there is potential for and meets the needs of all Australians, including priority
increased participation by primary health care nurses populations. The plan will explore innovative and cost
and pharmacists. Pharmacists, particularly through effective workforce strategies to ensure the health
community pharmacy, play an important role in providing workforce is suitably trained, resourced and distributed,
advice and support for self-management practices. and is working to its full scope of practice. This includes
Similarly, primary health care nurses have an important investigating obtaining Medical Provider status for
role in this area that is likely to increase as their scope specifically trained asthma educators, and enabling
of practice expands over time. The role of respiratory appropriately trained health care professionals such
specialists remains vital, particularly for patients with as practice nurses to prepare asthma action plans (i.e.
poorly controlled and severe asthma. A number of communicate/explain the plan and discuss options with
professionals working outside the health care system the patient). Preparation of asthma action plans would be
are also involved in asthma care. This includes early undertaken in partnership with the prescriber, usually the
childhood educators and teachers, sports coaches GP who is currently legally required to sign off the plans.
and Home and Community Care workers. Asthma care The health workforce plan will include a review of existing
involves a multidisciplinary and holistic approach, and training (Vocational, Undergraduate and Post-Graduate)
initiatives to develop the workforce should include inter- to identify how future education and training can improve
professional and inter-disciplinary training opportunities asthma outcomes and meet the evolving needs of people
where appropriate. with asthma.
Australia has world-leading, evidence-based treatment
guidelines – the Australian Asthma Handbook – to guide 2.2 Ongoing revision, dissemination and
primary care health professionals in the diagnosis implementation of the best practice
and management of asthma. Proven strategies for treatment guidelines for asthma diagnosis
health professionals who provide asthma care include and management
the imperative to conduct regular reviews, prescribe Continue to disseminate and implement the best
appropriate medications, provide and update asthma practice treatment guidelines for asthma diagnosis and
action plans, and support the patient to develop effective management in primary care – the Australian Asthma
self-management practices so as to control their asthma Handbook – including regular updates in response to
(e.g. correct use of inhalers) (1). emerging issues and new evidence, to ensure clinical
There is evidence of health professional non-adherence care reflects evidence-based best practice guidelines.
to Australia’s best practice guidelines (9, 24-29). For example, revise current asthma treatment guidelines
Supporting health professionals to realise their full scope to address issues associated with asthma management
of practice and deliver consistent, best practice asthma in those with psychosocial problems, including drug and
care based on the asthma treatment guidelines will close alcohol addiction, given that both are problematic and
the gap between evidence and practice, and improve widespread.
patient quality of life and reduce asthma morbidity and
its associated costs. Greater investment and sustained
effort is required to support professionals working with
nationalasthma.org.au/strategy 11NATIONAL ASTHMA STRATEGY 2018
2.3 Deliver education, training and support for 2.4 Support the development of communication
health professionals and counselling techniques
Continue face-to-face and online education, training and Support the development of effective and culturally
support of health professionals to develop the workforce safe and appropriate communication and counselling
and its capacity to provide consistent, best practice techniques to improve the cultural competence of the
asthma care. Education, training and support to focus on: health workforce. A culturally competent workforce
Detecting and diagnosing asthma and other acute communicates respectfully and is able to establish good
and chronic respiratory conditions in a timely and relationships in order to support people with asthma
appropriate manner and their caregivers to understand information about
asthma and health care, to apply that information to their
Supporting patient self-management practices
lives and to use it to navigate the health care system
(particularly for newly diagnosed) and assisting
and make decisions about their asthma care. Culturally
patient behaviour change, with a focus on addressing
safe and appropriate communication and counselling
incorrect inhaler technique, poor adherence, patient
techniques will improve asthma outcomes for Aboriginal
preferences and practical issues
and Torres Strait Islander people and other priority
Managing asthma alongside comorbid conditions populations.
Enhancing asthma health literacy and evidence-based
2.5 Develop quality use of medicine initiatives for
shared decision making
prescribing preventer medicines
Appropriate prescribing of preventer medicine
Develop initiatives to improve health professional
Delivery of asthma action plans combined with patient
understanding of the efficacy and cost-effectiveness of
education in self-monitoring, review of medicines and
ICS only preventer medicines compared to combination
assessment of severity
(ICS/LABA) preventer medicines, with treatment
Annual review of asthma patients targeted to individual patient needs. Support patients to
Work-related asthma including importance of make informed decisions about their asthma medication
eliminating exposures at work that take into account medication expenses and their
Management strategies in school and childcare capacity to fund treatment.
services
2.6 Deliver training and support for non-health
Mental health impact of asthma on patients.
professionals
Continue delivery of evidence-based workshops on
Deliver training and provide support to professionals
asthma management and lung function testing to GPs,
working outside the health care system, including
primary health care nurses, pharmacists, asthma and
community environments where people live, learn,
respiratory educators, generalist physicians and nurses,
work and play, e.g. Aboriginal community controlled
and Aboriginal health workers and practitioners in
organisations, early childhood educators and teachers,
remote, regional and urban Australia.
sports coaches and Home and Community Care workers.
Education, training and support for health professionals Professionals in different sectors and settings have
providing services to Aboriginal and Torres Strait an important role to play in asthma care, including
Islander people to include cultural awareness training to responding to emergency situations and promoting
ensure culturally safe and appropriate asthma care. health and reducing asthma risk across the life course.
12 nationalasthma.org.au/strategyNATIONAL ASTHMA STRATEGY 2018
Objective 3:
Enhance asthma care and management
Australia’s health care system is a complex and multi- such as increasing the number of Aboriginal and Torres
faceted web of public and private providers, patients, Strait Islander people in the workforce and enhancing
settings and supporting mechanisms. Health providers the focus on culture within health care education.
deliver a plethora of services across many levels, from Responsible partnerships and an inclusive and locally
public health and preventive services in the community, responsive approach is required.
to primary health care, emergency health services,
hospital-based treatment, and rehabilitation and 3.2 Develop and implement nationally consistent
palliative care. It can be difficult for people to navigate hospital discharge protocols for asthma
their way through the ‘maze’ of health service providers
Effective discharge pathways between health services,
and receive integrated, ‘joined-up’ care (39, 40).
particularly between the acute and primary care
Strong governance and leadership that supports settings, are essential to providing coordinated asthma
evidence-based shared decision-making and encourages care across multiple health settings and services. In
collaboration to enhance health system performance is collaboration with stakeholders across all levels of
required. Powerful approaches can be adopted within governments, develop and adopt national hospital
the health care system to facilitate the efforts of people and emergency department discharge and outpatient
with asthma, their caregivers and health professionals to follow-up protocols/guidelines, with a focus on priority
work together to enhance asthma care and management. population groups such as Aboriginal and Torres Strait
This includes multidisciplinary, collaborative care models Islander people. This would include the use of technology
to ensure the different levels of care are linked. Links to identify patients who are frequent users of emergency
between different sectors and settings – such as a GP departments.
and nurse working in primary care, a secondary care
hospital emergency department, ambulance services, 3.3 Contribute to health system reforms and
pharmacist advice and a school in the community – reviews
enables appropriate management and systematic
Contribute to health system reforms and reviews in order
follow-up. Removing system barriers to optimal care and
to improve asthma outcomes and meet the evolving
creating an integrated, equitable and accessible system
needs of people with asthma.
for all stages of asthma care will ensure health services
are accessible to priority populations such as Aboriginal Contribute to PBS reviews and continue to provide
and Torres Strait Islander people, and deliver better advice to the Pharmaceutical Benefits Advisory
health, social and economic outcomes for all Australians. Committee.
Contribute to the Australian Government Healthier
Actions Medicare Initiative to explore opportunities for the MBS
3.1 Explore initiatives that positively advantage to recognise and encourage best practice and quality
Aboriginal and Torres Strait Islander people improvement in asthma diagnosis and management. The
and other priority populations to overcome initiative’s MBS and/or Primary Health Care reviews to
current inequities in asthma outcomes include an economic modelling and investment review of
all asthma-related Medicare Provider Numbers and PIP
Explore initiatives that positively advantage Aboriginal payments provided to health professionals, and make
and Torres Strait Islander people and other priority recommendations on an integrated model of care which
populations to overcome current inequities in asthma may include, but is not limited to:
outcomes. Accessible health services that are culturally
safe and appropriate, effective, high quality, affordable The effectiveness of the Asthma Cycle of Care
and flexible are critical to address the disproportionate Program, GP Management Plans, Team Care
burden of asthma experienced by priority populations Arrangements
and ensure the health system at all levels is responsive The adequacy of PIPs for lung function testing and the
to the specific needs of priority populations. need to update the wording of these PIPs to reflect
current medicines
The concept of health for Aboriginal and Torres Strait
Islander people is holistic, with culture, land and Consideration of health professionals who do not have
spirituality playing a key role (3). Explore initiatives to a provider number, such as nurse practitioners.
enhance the cultural competency of the health workforce
nationalasthma.org.au/strategy 13NATIONAL ASTHMA STRATEGY 2018
3.4 Identify and use new and emerging 3.5 Explore innovative strategies to support
technologies and strategies in asthma cost-effective prescribing of asthma
interventions medications to improve access to affordable
medication
Monitor, identify and utilise, as appropriate, new and
emerging technologies, digital tools and platforms to Explore innovative strategies to support cost-effective
support people with asthma and health professionals. prescribing of asthma medications to improve access to
Technology supports more effective and accessible effective affordable medication.
prevention and management strategies by empowering
people with asthma to engage in effective self- 3.6 Optimally implement and disseminate new
management practices (e.g. supports medication evidence-based asthma treatments
adherence) and supporting health professionals to
Optimally implement and disseminate effective and
provide best practice asthma care (e.g. asthma action
efficient treatments for asthma, ensuring affordability,
plans and decision support tools in medical software and
accessibility and appropriate targeting of therapy.
other digital platforms).
Continue to work in a coordinated and collaborative way
Consider innovative and flexible service provision options to introduce novel therapies into the Australian market
such as e-health technologies, as a means of delivering using a sustainable and cost-effective approach. Ensure
information and services (e.g. telehealth), particularly new evidence-based treatments are disseminated
for those in rural and remote areas where access is through treatment guidelines and other forms, and
problematic. integrated into clinical practice.
Explore the opportunity to pilot the use of personal
e-health records using asthma as a chronic condition test
case, with asthma action plans a key component.
Objective 4:
Create supportive community environments
The environments where Australians live, learn, work and chronic conditions and may improve outcomes for other
play are important settings in which to promote health chronic conditions that commonly coexist with and can
and reduce asthma risk. affect asthma.
There is currently no reliable evidence for effective International and national experience shows that a multi-
interventions to prevent the onset of asthma (primary sectoral approach is most effective at improving asthma
prevention), however risk factors may increase the care and patient outcomes. Different sectors and settings
chance of a person developing asthma in the first – such as workplaces, schools and communities – have
place, or may increase the chance that a person with an important role in promoting health and reducing
asthma will develop additional health problems. Actions asthma risk across the life course.
to create supportive community environments will
promote health and reduce asthma risk, with a focus Actions
on minimising or preventing asthma from worsening
(secondary prevention) and reducing the risk of people 4.1 Explore innovative strategies to reduce
with asthma developing additional chronic conditions, modifiable risk factors for asthma and
complications and/or associated disabilities (tertiary strengthen asthma prevention
prevention). Explore innovative strategies to reduce modifiable risk
Asthma shares a number of risk factors with other factors in the general population and strengthen asthma
chronic conditions. The Australian Burden of Disease prevention. Drive change to support the development
Study in 2011 (19) identified that almost one-third of of health-promoting community environments that
the burden of disease in Australia in 2011 could be encourage people to increase levels of physical activity,
prevented by eliminating exposure to risk factors such reduce sedentary behaviour and tobacco use, and
as tobacco use, overweight and obesity, and sedentary improve healthy eating. Address maternal, family and
lifestyle/physical inactivity. Hence, actions to improve child health, enhancing early life and growth patterns.
asthma outcomes are applicable for a broad range of
14 nationalasthma.org.au/strategyYou can also read