N The Leeds Teaching Hospitals NHS Trust - Quality Improvement Strategy 2017-2020 - Leeds Teaching ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

n
The Leeds
Teaching Hospitals
NHS Trust
Quality Improvement
Strategy 2017-2020
1
3 Foreword 24 Examples of local Quality
Contents
Improvement
4 Quality Improvement in LTHT
26 Complementary strategies
6 Our methodology and tools
27 Our future priorities
10 LTHT Quality Improvement
framework 28 How to get involved
12 Examples of our improvement 29 Resources
programmes:
- Leeds Improvement Method 30 Meet the steering team
Value Streams
- Falls
- Deteriorating Patient
- Safety Huddles
- Acute Kidney Injury
- Pressure Ulcers
- Sepsis
- Parkinson’s Disease
- Integrated Care with Partners
- Transforming End of Life Care
- Patient Experience ‘Always
Events’
At Leeds Teaching Hospitals NHS Trust, we are This strategy is shaped by:
Foreword
committed to improving the quality of care
• working with our staff and patient representatives
we provide to our patients and their carers.
at our Quality Ambitions workshop
This requires everybody to be involved in
improvement, as individuals, as teams, and as a • our current work with the Virginia Mason
whole organisation. Institute and partner organisations
We published our first Quality Improvement • our collaborative Quality Improvement
Strategy in 2014, and in less than three years work, supported by partners including the
we have taken huge steps in improving the Improvement Academy.
quality of care we provide to our patients. We
are proud of the ambitions we set, the amazing It describes our organisational approach to
achievements our staff have made so far, but improvement: The Leeds Improvement Method.
now we wish to set out our commitment that Everyone working at LTHT has a role in the work
together we can go even further. they do, and also in improving the work they do.
In this 2017 Quality Improvement Strategy we Yvette Oade,
reflect on the progress we have made, and set Chief Medical Officer
our ambitions for the next three years; including
areas we wish to improve even further, as well Suzanne Hinchliffe,
as setting new priority areas. Chief Nurse and Deputy Chief Executive
3
Quality Improvement at LTHT • Lots of smaller improvement work within and
Quality Improvement at LTHT
across our departments, bringing about real
This document aims to improvements for our patients
1. Outline our quality improvement ambitions • Our Leeds Way values.
for the organisation in the future
2. Tell you about information about our The Trust signed up to the
approach to quality improvement in the Trust national Sign Up to Safety
3. Bring together our existing quality Campaign in August 2014
improvement approach with the Leeds pledging to put safety first
Improvement Method to form the Trust’s and reduce avoidable harm.
approach to quality improvement
Our Quality Ambitions workshop in April
4. Showcase our quality improvement successes
2016 helped us to build on our learning
to date at Leeds Teaching Hospitals, which
to date, and shaped our core principles for
we are proud of
enabling continuous quality Improvement
5. Show how you can get involved throughout the Trust. These principles are:
Our ambition for the future Leadership at all levels to engage and sustain
our improvement culture
Our ambition is for Leeds Teaching Hospitals
to build a culture of continuous improvement Engagement and Support to partner with
across the organisation. patients and their families for the safest
care, and for all our staff to be involved in
We will treat every patient as an individual, deliver improvements as part of the work they do.
the best outcomes, the best possible experience,
Communication to support continual learning
and one which is free from avoidable harm.
and improvement from senior leaders to frontline
staff, from ward to the Board and throughout
How we will achieve our ambition
the organisation
Building on solid foundations
Empowerment to create a shared purpose and
We have some great foundations which will understanding of quality improvement
help us achieve our ambitions: Infrastructure training and capability for all
• Out partnership work with Virginia Mason, staff in quality improvement
and the success of the first Leeds Improvement
Method value streams in Elective Orthopaedics The Quality Ambitions workshop helped us
consider our approach to improving care not
• Our Trust-wide quality improvement within our own organisation and across health
programmes as outlined on pages 12-22, and social care with a focus on Older People,
which have helped spread the knowledge and Children and integrated care for all (both Trust
learning from quality improvement methods wide and locally within CSUs and specialties.
4
Our strategy is to continually develop and deliver improvement programmes using
a range of Quality Improvement Tools. We will share and celebrate learning, and
continue to develop and deliver training to as many staff as possible.
5
Our Methodology and tools
Methodology and tools
Leeds Teaching Hospitals NHS Trust promotes Both methods also recognise that improvement
the use of both the Leeds Improvement Method works best when people at the point of
and the Model for Improvement as methods for care, those engaged directly in the work,
quality improvement. are empowered to test changes and use
local feedback data to make improvements.
There are many similarities between the
You shouldn’t assume that what works well
approaches and their underlying philosophies,
in one place is going to work everywhere:
and they complement each other well. The Leeds
improvements might need additional
Improvement Method uses Lean methodology
adaptation and testing in a different location.
which has strong and well-defined approaches
that can help identify system-level issues for Again and again we’ve seen out in the field
improvement. The Model for Improvement that it’s not as important to choose one method
often uses similar tools as those used in Lean to or the other, it’s most important to empower
understand the local system. Both approaches people at the point of care to make changes.
concentrate on the patients as the focus of the
outcomes to be improved.
6
Leeds Improvement Method
LTHT is one of only five Trusts in the UK to be
working with the prestigious Virginia Mason
Institute on a programme known at the Trust as
the Leeds Improvement Method. The method
focusses on improving the efficiency and flow of
our services, with patient and staff experience
embedded at the centre of this work.
Creating the Infrastructure:
• The Trust Guiding Team includes the: Chief
Executive, Executive Team, Kaizan Promotion
Office Lead, and NHSI Partner
• A Kaizen Promotion Office (KPO) has been
established to drive the improvement work in
the organisation, including the KPO Lead and
three KPO Specialists.
• The following training programmes have been
established in the method: Lean for Leaders
Programme, one hour introduction sessions,
and a one day leadership orientation.
The Leeds Improvement Method:
• Is patient focused
• Is the application of observation and data
analysis tools, to describe how patients
experience our services
• Supports staff to systematically remove waste
• Promotes zero defects and zero harm for patients
• Uses a disciplined time frame
• Encourages participation and respect for each
other as equals.
It brings together a representative cross section
of staff, with a range of skills and experience, to
review and improve how they work in order to
improve patients’ experience of our care.
7
There are three key concepts at the heart of the Leeds Improvement Method. They are:
Methodology and tools
1. Value 2. Waste 3. Respect for people
• Value is defined by our • Waste is anything that does • Respectful behaviour is the
patients not add value from the common denominator under-
perspective of our patients pinning our Leeds Way Values
• The patient is at the top
of our strategic plan as we • Some of our activities • We must not judge those
aspire to ensure that our may not add value for our doing the work and work
patients voice is embedded in patients but are required - hard to understand how
our improvement activities we call this Type 1 Waste they have learned to do it, or
been taught to do it, in our
• In order to achieve our • Some of our activities
organisation
aspiration it is important we may not add value for our
have one chosen method patients, or our staff, and • Respect for the patient
for running our services and can be stopped immediately journey will require us to
improving our services - The without any detrimental challenge our thinking in the
Leeds Improvement Method impact on our services - way we work together
we call this Type 2 Waste
• In the early phases of
implementation we are keen
to remove Type 2 waste first
• There are seven categories
of core waste in The Leeds
Improvement Method
7 categories
of waste
Processing Time Overproduction
Unnecessary processes Waiting for people or Producing something
and operating traditionally services to be delivered (time at the wrong time or in
accepted as necessary when people, process or unnecessary amounts
equipment are idle)
Defects Inventory Transportation Motion
Waste related to costs for Excessive supplies, materials Conveying, transferring, Unnecessary movement
inspection of defects in materials or info for any length of time picking up, setting down, that does not add value
and processes, customer (having more on hand than piling up and otherwise (movement that is done too
complaints and repairs what’s needed moving unnecessay items quickly or slowly)
8
Model for Improvement Breakthrough
Over recent years at LTHT we have successfully used Series Model
The Model for Improvement, from the Institute for
Healthcare Improvement, to improve our processes
and outcomes. It is a simple yet powerful tool for
accelerating improvement and complements our
approach with Virginia Mason to reduce variation
and waste to continuously improve.
What are
Set out your ambition with
we trying to
specific aims
accomplish? Driver Diagram
A Driver Diagram helps you set out you aim and
How will we know Determine how you are going
that a change is to measure your outcomes
identify the components you need to improve
an improvement? and processes
What change can we The Plan-Do-Study-Act (PDSA)
make that will result cycle is for testing a change
in improvement? in the real work setting — by
planning it, trying it, observing
the results, and acting on
what is learned. After testing a
change on a small scale, learning
Act Plan
from each test, and refining the
change through several PDSA
Study Do cycles, the team embeds the
change, and by working as part
of a collaborative can spread
the changes to other parts of
the Trust.
Measurement - SPC charts
A Statistical Process Control chart helps you
to plot variation and see where change may
Key Tools represent a significant improvement
Breakthrough Series Collaborative
This is a structure for medium scale improvement
where a faculty supports several areas working
together to test changes linked to secondary drivers,
and find out which bring about real improvements.
9
LTHT Quality Improvement
Quality Improvement framework
framework
Our Strategy to continually learn and improve in Our current improvement programmes are
every aspect of our work, focuses on four main described on the following pages, showing our
areas, with patient experience at the heart. journey, successes and future ambitions
Harm free care
Developing a world-class culture of
‘first do no harm’ to deliver the safest
healthcare in the UK. This will focus on
harm free care in our wards
Patient Safety
(harm free care)
The Leeds
Integrated care Improvement
t Experie
Improvement Method
ien nc
with partners at Method
across the health
economy (LIQH)
Integrated care
P
value streams
e
Working with partners in LTHT is one of only five
Trusts in the UK to work
Leeds
health and social care to
develop improvements with the prestigious
in care for the whole of Virginia Mason Institute
the pathway of care for on a programme known
at the Trust as the Leeds
P
e
at
patients with specific ien nc
conditions
t Experie Improvement Method
Local
Improvement
Local small scale quality
improvements
Where everybody can improve the services
and care they provide
1011
Leeds Improvement Method
Improvement programmes
Value Streams
In October 2015 four work areas, known Successes:
as Value Streams, were chosen for initially • For elective orthopaedics, total hip and knee
developing the Leeds Improvement Method: replacement, patients now typically receive
• Elective Orthopaedics (total hip and knee their appointments six weeks in advance of
replacement - admission to recovery) surgery. It used to be three weeks notice
• Urology (transurethral resection of the • As a result no-one listed for surgery has
prostate – recovery to discharge) cancelled their appointment meaning better
theatre utilisation
• Critical Care (patient flow to neurosurgery
wards) • The scheduling team now spend only 10%
of their time rescheduling cancelled
• Outpatients (patient journey and experience appointments, compared with 80% previously
in their Ophthalmology appointment)
• There has been a 37% reduction in
Two sponsor development sessions have been sterilisation costs by reducing the number
held to develop the value streams. of theatre trays required and number of tools
on each tray
Five 5-day Rapid Process Improvement
workshops have already been held, and eight • There has been an 80% reduction in
more are planned each year. theatre tray set up time, down from 49
minutes to just 9 minutes
Around 200 staff have been directly involved in
improvement activity to date. • We have actively involved a patient in
our elective orthopaedic pre-assessment
work and will build on this as we start other
workstreams.
OUR AMBITION is to scale up the
implementation of the Leeds Improvement
Method to ensure that by 2020 all our
workforce have experienced the method,
either through direct training and
education or from being involved in an
improvement event.
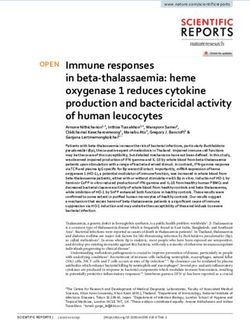
12Falls
The most common patient safety incident Successes:
causing harm reported by NHS Trusts relates to May 2016 saw pilot wards reach their aim of
patients who fall whilst in hospital care. 50% falls reduction. The intervention bundle is
already scaled up across four clinical service units.
AIM: to reduce inpatient falls by 50% on Falls per 1,000 bed days - Pilot Wards
16
pilot wards
14 Ward Walks 50% Reduction Achieved
Collaborative Start Bundle Launch
12
In July 2014, we started a breakthrough 10
Number of Falls
series collaborative improvement programme 8
with 14 pilot wards. The wards trialled small 6
tests of change, and measured the results
4
using PDSA cycles to assess whether they
were an improvement. Successful changes 2
were then tested across all pilot wards. These 0
Nov-13
May-14
Nov-14
May-15
Nov-15
May-16
Mar-14
Aug-14
Mar-15
Aug-15
Mar-16
Oct-13
Oct-14
Oct-15
Jun-14
Jun-15
Jun-16
Dec-13
Jan-14
Feb-14
Sep-14
Dec-14
Jan-15
Feb-15
Sep-15
Dec-15
Jan-16
Feb-16
Jul-14
Jul-15
Jul-16
Apr-14
Apr-15
Apr-16
interventions, shown to make a difference,
went on to form the Falls Intervention Bundle. Falls per 1000 Bed Days Baseline Target Mean
The Intervention Bundle consists of;
• Safety huddles OUR AMBITION is to scale up the
• Toileting implementation of the intervention bundle
across all wards in the Trust and achieve
• Good footwear
and sustain a 50% reduction Trust-wide.
• Post falls review
• Cohorting of
patients at risk
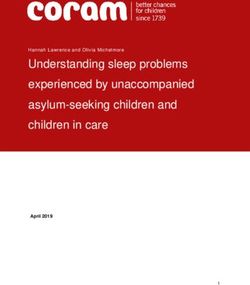
13Deteriorating Patients
Improvement programmes
We want to continually improve the treatment Successes:
and care of our patients when they deteriorate In July 2016 the pilot wards achieved their aim
on our wards, to ensure they receive safe, of a 50% reduction in cardiac arrest calls
timely and effective treatment and care, and
better end of life care. The scale up of the intervention bundle is now
being tested in two full CSUs (Acute Medicine
and Abdominal Medicine and Surgery) and will
then be finalised for scale up across all wards in
AIM: to reduce avoidable deterioration by the Trust.
50% on pilot wards
Cardiac Arrest Calls - Pilot Wards
Cardiac Arrest Calls - Pilot Wards
12
In July 2014 we started a breakthrough series 10
collaborative improvement programme with
14 pilot wards. Our aim was to reduce 8
avoidable deterioration by 50% on pilot
6
Calls
wards. The wards trialling small scale tests of
change, to reduce avoidable deterioration. 4
Our “Deteriorating Patient Intervention Bundle” 2
was launched in June 2015 incorporating
the interventions which the pilot wards had 0
Jul-14
Oct-14
Dec-14
Jul-15
Oct-15
Dec-15
Jul-16
Oct-16
Feb-14
Sep-14
Feb-15
Sep-15
Feb-16
Sep-16
Jun-14
Jun-15
Jun-16
Jan-14
May-14
Jan-15
May-15
Jan-16
May-16
Mar-14
Apr-14
Nov-14
Mar-15
Apr-15
Nov-15
Mar-16
Apr-16
Nov-16
Aug-14
Aug-15
Aug-16
identified as being successful:
Month
• Safety Huddles,
• 1:1 NEWS Training
and Observations OUR AMBITION is to scale up the
Made Easy implementation of the intervention bundle
• NEWS sticker across all wards in the Trust and achieve
and sustain a 50% reduction Trust-wide.
• Escalation of Care
sticker
• Post 2222
call review.
14Safety Huddles
Ward led Safety Huddles were first tested on Successes:
four wards at LTHT in 2013, with evidence So far, Huddles have been adapted and
of reduction in patient harm and improved embedded to more than 50 wards at LTHT. This
teamwork and safety culture. Other wards has been associated with reductions in harm
adapted huddles to their areas, and the Trust including falls, pressure ulcers, cardiac arrests
were awarded a ‘Scaling Up Improvement’ and improvements in safety culture. As a result
Grant from the Health Foundation in 2014. many other organisations nationally are taking
an interest in our learning and improvement.
AIMS: Implement patient safety huddles
on all our wards to deliver:
- improvements in ward-level patient
safety culture
- significant reductions in patient harm
- learning about the implementation
that is valuable across the NHS
The huddle follows some general principles; Safety Huddles are focused on one or
more agreed patient harms (identified
staff review how many days it is since the last by the team) such as falls, pressure
fall, cardiac arrest (or other agreed harm); look ulcers, or avoidable deterioration.
at who may be at risk of the harm today; and
Safety Huddles are a short (5-10 min),
what actions need to be implemented by the daily, MDT ward patient safety meeting
team to reduce the risk. involving all members of the team.
Patient and public engagement events
have been held where safety huddles are
demonstrated. Suggestions from attendees OUR AMBITION is to embed safety
as to how the patients and carer views and Huddles on all our wards by the end of
concerns can brought into the daily huddle, are 2017.
currently being tested on several wards
15Acute Kidney Injury (AKI)
Improvement programmes
Acute Kidney Injury (AKI) is a major cause of Successes:
harm, with half a million people sustaining AKI • AKI electronic alert and care bundle is in use
in England every year. It has a major impact on in 8 wards across the Trust
patients, including increased length of stay, the
risk of progression into chronic kidney disease, • Changes to the Trust observation charts to
and an increased risk of dying. It is estimates that improve awareness around AKI
AKI could be preventable in 20-30% of cases. • Targeted AKI education sessions for medical
and nursing teams
• Embedding the STOP acronym throughout
AIM: to apply evidence based interventions the Trust as an aid to manage AKI
to improve:
• Sharing learning with other organisations in
- prevention
the project through peer assist events
- detection
• Increased knowledge and awareness around
- management
AKI
- safe discharge
• Improved speed of diagnosis
- follow-up
- rehabilitation
of patients with AKI OUR AMBITION is to continue to spread
the package of AKI interventions across all
wards in the Trust.
The tackling Acute Kidney Injury (AKI) project
was launched in April 2016 as part of a Health
Foundation project across five NHS Trusts.
Improvements will be achieved through
awareness, education, an electronic alert, and
use of the STOP AKI care bundle.
16Pressure Ulcer Prevention
Pressure ulcers can be painful, affecting quality Successes:
of life, lengthen hospital stay and may even be • Following successful testing within a number
life threatening. It is estimated the overall cost of CSUs, Trust wide scale up started in 2016,
of treating pressure ulcers is between £21.4- supported by the Tissue Viability Team and a
£2.1 billion per year in the UK; around 4% of Clinical Leadership fellow for Nursing.
the annual NHS expenditure. It is estimated that
80-95% of all pressure ulcers are avoidable. • There has been a reduction in the number of
category 3 pressure ulcers, and a period of 74
days between April and July 2016 without a
hospital acquired Category 3 pressure ulcer.
AIM: through a collaborative team
approach, we aim to reduce the number
of patients who develop avoidable
pressure ulcers through implementation of OUR AMBITION is by the end of 2017, to
the SSKIN intervention bundle. have achieved zero avoidable category 4
pressure ulcers developed in our hospitals,
and reduce category 3 pressure ulcers
by 50%, through scale up of the SSKIN
Our QI programme was launched in November
interventions across the Trust.
2015 based around the ‘stop the pressure’
initiative from Midlands & East Region. We are Our longer term ambition is to have
testing a range of interventions that sit under a no category 3 or 4 avoidable hospital
SSKIN acronym: acquired pressure ulcers and to have no
more than 3 hospital acquired category 2
Skin Inspection
pressure ulcers per month, per CSU.
Surface - appropriate mattress/cushion
Keep Moving
Incontinence/Moisture
Nutrition/Hydration
This framework has been
widely tested and
implemented in a range
of acute hospitals.
17Sepsis
Improvement programmes
Sepsis is one of the biggest causes of mortality Successes:
in the UK with 44,000 deaths annually and all The Emergency Departments have implemented
age groups being affected. NHS hospitals treat the sepsis protocols and are now embedding
around 150,000 cases of severe sepsis each the use of the sepsis screening tool and
year and many more with uncomplicated sepsis. BUFALO interventions.
It causes more deaths every year than breast,
bowel and prostate cancer combined but, with Sepsis has also been incorporated into an
early recognition and treatment, it is thought e-learning package as part of the Acute Kidney
that mortality can be cut significantly. Injury programme.
The Sepsis programme of work is closely
aligned to our work on reducing avoidable
AIM: to improve the identification and deterioration.
management of red flag sepsis patients
and to reduce the mortality rate from red
flag sepsis and septic shock. OUR AMBITION is to reduce mortality
resulting from Sepsis by 30%.
In the short term we aim to roll out use
In 2015 we tested and developed an intervention of the sepsis screening tool and BUFALO
package for clinical areas to provide reliable and interventions across the Trust in 2017.
effective sepsis care: this consists of a screening
tool and the “BUFALO” interventions.
18Parkinson’s Disease
In August 2016 we launched our improvement Successes:
collaborative with 16 clinical areas, to improve Working with carers, our faculty and front line
the care of patients with Parkinson’s. This teams have already:
was in response to feedback from patients’
families, and in this collaborative, patients and • Raised awareness across the wards and in a
carers are actively involved. Our ward areas are launch event
testing small scale tests of change, using the • Created a real time list of current inpatients
breakthrough series collaborative model. with Parkinson’s Disease
• Developed educational material
AIM: for all patients with Parkinson’s
to receive timely administration of
OUR AMBITION is that all our
medication and holistic care on pilot areas
patients with Parkinson’s receive timely
by June 2017.
administration of medication and holistic
care. We aim to further involve our patients
and carers, to work in partnership with us
to improve the quality of care we provide.
19Transforming End of Life Care
Improvement programmes
LTHT has been selected as one of 10 acute Successes:
Trusts across the UK to take part in the national The Palliative Care Team have implemented
‘Building on the Best’ programme to improve small changes to the care dying patients and
palliative and end of life care. Supported by their families receive in the final days/hours of
a partnership between the National Council life which have made a positive impact:
for Palliative Care, Macmillan Cancer Support,
NHS England, and NHS Improving Quality, the • Comfort care packs are offered to families
programme will run for two and a half years. who wish to stay overnight at the bedside of
their loved one. These include items to enable
family members to freshen up, sleep more
comfortably in a chair and buy a snack
AIM: to ensure all dying patients who are
experiencing terminal agitation have an • We have a number of different charities making
effective, individualised plan of care, cloth bags out of beautiful fabric, for patients
to be able to carry their syringe pumps with
improve accessibility to palliative care
them. All wards have a supply of these bags.
services in the outpatient setting,
empowering patients to discuss advanced • Working with the car parking team, we have
care planning. been able to extend the free car parking passes
issued to family members, to last for 7 days,
which reduces the need to renew them and
Two work streams have been established, one also covers the time when families attend the
focusing on the care the patients with terminal bereavement office to collect death certificates.
agitation and the other improving access to This holistic approach to care, not only puts
palliative care services in outpatients patients at the centre of everything we do, but
Interventions such as education sessions in also their families.
terminal agitation, and promotion of written
information in outpatient pilot areas, are being
tested. OUR AMBITION is that all dying
patients in LTHT and their families receive
Improvement measures have been established
exemplary care at all times.
and this data is being collected so we know if
we are making real improvements. To avoid hospital admission from the pilot
outpatient clinics we are aiming to offer a
palliative care in-reach service for complex
symptom management.
20Patient Experience -
‘Always Events’
‘Always Events ‘were first introduced in the Progress to date:
United States by The Institute for Healthcare So far, work has been undertaken to put the
Improvement and the Picker Institute. They building blocks in place for patients and the
focus on ensuring events that matter to patients public to be consulted on what is important
happen every time, for every patient. Successful to them. Development of a patient reference
use of this positive approach to improving group is underway and this group will be key
patient care is supported by ‘Always Events’ to influencing the creation of Always Events for
methodology. the Trust. The first group meeting is planned for
An Always Event is a clear, action-orientated, January 2017.
and pervasive practice or set of behaviours that
provides the following:
• A foundation for partnering with patients OUR AMBITION is to develop Always
and families Events, in consultation with patients, and
to drive improvements in the quality of
• Actions that will ensure optimal patient our patient experience through the Trust
experience and improved outcomes wide implementation of these.
• A unifying force that demonstrates an on-
going commitment to person and family care.
AIM: to develop, in consultation with
patients, a series of ‘Always Events’ that
demonstrate learning from what the Trust
does well, and focus on the elements of
care that patients value most,
to use ‘Always Events’ to promote
positive practices and behaviours of staff
and improve the hospital experience for
patients and families.
21Integrated Care with partners
Improvement programmes
Over the last two years, the Trust has been actively Examples:
involved in the Integrated Care Improvement Cardiac rehabilitation data collected as part
Programme led by Leeds Institute for Quality of the LIQH Cardiovascular Disease Programme
Healthcare (LIQH), which promotes a cross-city showed that over an 11 month period, 340
approach to improving quality of care by: patients who had had a Myocardial Infarction
• enabling clinicians to develop shared had been discharged from specialties other
expertise, and than cardiology; consequently the majority
would not have received hospital based cardiac
• developing a rigorous approach to rehabilitation or any community based support.
professional accountability using data to Work has been undertaken to promote the
review variation and decision-making Cardiac Rehabilitation service using posters
across the Trust, and the service strengthened
The Trust has been actively involved in six
with an ‘in reach service’ on the SJUH site, link
change programme workstreams;
nurses on wards, and information booklets
• Chronic obstructive pulmonary disease available for patients. This initiative is already
(COPD) ensuring more patients receive the cardiac
rehabilitation they need to improve outcomes
• Cardiovascular disease
for these patients.
• Fracture neck of femur
Fracture neck of femur work stream used a
• Improving diabetes care multi-disciplinary team approach to develop
• Improving dementia care a community falls clinic for frail patients who
were screened as high risk on the basis of their
• Improving cancer care electronic frailty assessment score. 90% of
patients who attended clinic went on to have
Our priorities moving forward will be on the
one or more interventions to reduce their risk
following two pathways with are linked to
of falls.
CQUINS* in 2016/17;
• Respiratory Pathway Review
• Cardiology Pathway Review
2223
Local (CSU/Specialty) Quality
Local Quality Improvement examples
Improvement examples
Here are just a few examples where our staff ‘Druggles’
have improved the services they provide. The Neonatal Unit at LTHT hold a weekly
Anyone can be involved in quality improvement; ‘druggle’ - a safety huddle focused on drugs
one person or team can make a change. and led by the pharmacist. It is a five minute
presentation aimed at increasing MDT
Parent Pagers communication on medicines related topics,
The Children’s Post-Anaesthetic Care Unit (PACU) highlight areas for improvement and encourage
team at Leeds Children’s Hospital trialled the use discussion. It includes a hot topic, an anonymised
of ‘Parent Pagers’ in operating theatres, to ensure error of the week (for real time feedback and
parents know exactly when they are needed learning), and results from the weekly prescribing
after their child’s surgery. The pagers were well standards audit. Feedback has been extremely
received, and are now being rolled out to the positive and there are plans to roll out weekly
parents of all children undergoing surgery in the druggles to all paediatric wards.
Leeds Children’s Hospital. They offer parents or
carers a sense of reassurance and freedom of Patient Services Confidentiality Card
movement whilst their child is in surgery. One member of our Outpatients staff
designed a card to go in front of the case
notes in the clinic trolleys. This ensures that no
patient record in clinic can be seen by other
patients, and also prompts staff to maintain
confidentiality. The card is now being widely
used throughout the Trust.
Nasogastric Tube Safety
To improve safety around the use of nasogastric
tubes (NGTs), radiographers were trained to
interpret and provide an electronic report on
Children’s Hospital Quality Improvement the position of the NGT at the time of the x-ray,
(QI) Forum and to act upon their findings. This information
Established in January 2016, this monthly is immediately available on the PACS system
multidisciplinary forum incorporates teaching enabling ward doctors to make an informed
on aspects of QI, alongside presentations from decision to use the NGT. This has led to a
frontline teams involved in QI. This is an example reduction of ‘never events’ in this area.
of how we are building capacity through
education and training, so that staff can lead
quality improvement activities within their teams.
24Chronic Pain Service Coffee Evening Breast Unit Telephone Clinic
The Chronic Pain Service has introduced a A telephone clinic has been implemented in the
bi-monthly coffee evening to give patients Breast Unit to prevent patients who have had
considering spinal cord stimulators to help negative cancer test results having to attend
manage pain, the opportunity to talk to other a further clinic appointment for their results.
patients about their experiences with the devices. Patients are given results over the phone at
The event was initiated as a result of feedback a specified time by a skilled and experienced
from patients who wanted more information nurse, avoiding an unnecessary visit to hospital
before taking such a significant step and felt and wasted time in clinic.
that user experience would help them with their
decision making. The event has received very Learning Disability Champions
positive feedback from patients, and volunteers Leeds Children’s Hospital has trained all Play
continue to offer support for the meeting. Specialists and Youth Workers to be Learning
Disabilities Champions. They will help support
Radiotherapy Assessment and Supportive and advise staff on wards to assess and provide
Care Lounge (RASCL) reasonable adjustments for patients, parents
In response to patient feedback, the nursing and carers with Learning Disabilities. Learning
staff in the Radiotherapy Review Clinic Team Disability Champions provide support and
worked with colleagues in the Planning and advice on a wide range of topics.
Estates Department to create a comfortable
and private environment for patients to Ophthalmology Day Case Unit
continue their care during the course of After receiving regular feedback from patients
their radiotherapy. The area has access to about long waiting times for cataract surgery,
clinical equipment, hand washing facilities, there are now two arrival times; morning and
and curtained areas to provide privacy. The afternoon. Friends and Family Test results show
area has allowed patients to maintain their that patients appreciate the shorter waiting times.
independence and well-being during long and
challenging periods of treatment, and has also
provided a safe area where patients can receive
OUR AMBITION is that anyone can get
medical and nursing care which may enable
involved and for everyone to be empowered
them to avoid admission to hospital.
and supported to improve their service.
More examples of local (CSU/Specialty) Quality Improvement can be seen in the annex to this strategy.
25Complementary strategies
Complementary strategies
Caring the Leeds Way Medicines Optimisation
‘Caring the Leeds Way - Our Professional The aim of the Medicines Optimisation Strategy is
Commitment’ was launched at the beginning of to use medicines safely and in the most effective
April 2016, setting out key objectives for nursing way, in partnership with our patients: making
and Allied Health Professionals for 2016-18. improvements in use of medicines links to many
of our quality improvement programmes.
It highlights new improvement initiatives to:
We put safety first with medicines to reduce
• improve the experience and safety of our
avoidable harm. We are focussing on medicines
patients
in our priority patient care pathways such as
• identify ways nurses, midwives and AHPs can improved management of Acute Kidney Injury
achieve financial savings through better use and Parkinson’s disease.
of resources
We monitor and share our learning from
• use clinical simulation to provide learning medicines harm, and put actions in place to
from complaints improve safety.
• maintain closer links with University Partners We support our health economy by taking a
to develop clinical research career pathways leading role in local collaborative initiatives.
• improve the experience of our staff through We are improving what we do to optimise our
leadership development and succession use of medicines by;
planning programmes.
• providing information about medicines
Key work streams to achieve these objectives by • recording and handover of medicine details
2018 are well underway. Further information at transfer of care
can be found on the Nursing and Midwifery
• improving the provision of medicines, for all
page on the intranet.
in and out patients.
OUR AMBITION is to:
• continue to learn and so improve our
use of medicines,
• optimise their benefit for all patients,
• involve patients in choices about their
medicine options.
26Our future priorities
Future priorities
Continual development of our
OUR AMBITION is for Leeds Teaching Improvement Programmes
Hospitals to never stop improving our We will build on all the work we have been
services and to become an organisation doing on our existing improvement programmes
with continual learning and improvement across the Trust, and add in some new ones.
at the heart of everything we do. We will be actively seeking to involve more
patients and carers in our improvement
programmes.
Culture
We will support our Clinical Service Units and
We want every member of our staff to feel they
Specialties to plan their improvement priorities
have an important part in improving the care
in partnership with patients and families, and
we provide. We will ensure training in Quality
support individual members of their staff and
Improvement methods is accessible to all staff
their teams.
so staff are empowered to carry out their own
improvement work, coming up with ideas,
testing small changes, and implementing those
that prove successful. Training courses will be
available in-house by December 2016. You
can sign up to the new Quality Improvement
Training Programme via the Organisational
Learning Training Calendar.
In this way we want to achieve a patient safety
culture where we do no harm to our patients, and
a learning culture, celebrating our learning when
things don’t work, and spreading our successes.
Communication
Sharing our learning locally and Trust-wide will
be a key priority, building on the existing features
in Start the Week and InTouch by including
departmental improvement work in our Leeds
Improvement Method Report Outs. We want to
celebrate the successes from all our improvement
work, Ward to Board, and also our learning from
things that have not been successful.
27How to get involved
Get involved
This is only a sample of the quality improvement You can book onto a training course, or talk to
work taking place across the Trust: there are someone who has already been involved. Contact
lots of opportunities for everyone to be involved details for the project leads can be found on our
in these. website or you can contact our QI steering team.
There may be improvement work already We want all our staff to have the opportunity to
underway that you would like to join, or you take part in quality improvement.
may wish to develop your own. The best ideas
Many members of staff already contribute to
for change come from the staff who deliver our
our Trust-wide improvement programmes. If
services, having a go and testing small changes
you would like to be involved, please contact a
and learning from their successes and failures.
member of the Steering Team on page 30.
Trust-wide improvement programmes 2017-20
Acut
on
Pressure ulcers
e Kid
falls
ati
ior
es
ney
ient
ter
dl
Pa
ud
rk
de
Injur
yh
Inpat
in
nt
so
t
Se
fe
En
tie
n’
y
Sa
ps
s’
d
sD
nt
Pa
of
is
nt
ve
ise
lif
tie
sE
as
Re e &
Pa
ca
ay
ine
e
spi re - edic ients
lw
rat
ory C e
‘A
Patient Safety t
pa OPD arg l m P pa
thw - ch ina
ay
(harm free care) Dis dom : TUR
Cardio ab gery wn
vasc t Experie sur p do
cardio ular diseas ien re ste
Improvement Method
nc Ca
logy p
athw -
e at Critic
al
across the health
economy (LIQH)
ay
P
e
Integrated care
value streams
rvices
Patient se
Leeds
CHOC - total hip
and
knee replacement
P
e
at
ien nc
t Experie
28Resources
Resources
Leeds Improvement Method web page Details of training courses can be found in the
http://lthweb.leedsth.nhs.uk/sites/leeds- following places:
improvement-method
Quality Improvement training page
Trust Quality Improvement web page http://lthweb.leedsth.nhs.uk/sites/
http://lthweb.leedsth.nhs.uk/sites/quality/ quality/quality-improvement-1/quality-
quality-improvement-1 improvement-strategy-framework/
training-1/training
Trust Training Calendar
https://traininginterface.leedsth.nhs.uk/
29Meet the team
The Steering team
Dr Yvette Oade Professor Suzanne Hinchliffe CBE
Chief Medical Officer Chief Nurse/Deputy CEO
Craig Brigg
Director of Quality
Dr Alison Cracknell Lorna Johnson
Consultant Geriatrician Quality Improvement
and Trust Lead for Nursing Lead
Patient Safety
Helen Gilbert Julia Roper
Leeds Improvement Quality Improvement
Method Lead Management Lead
Liz Mellor Dr Anna Winfield
Medicines Safety Lead Patient Safety and
Quality Manager Lead
Scott Armitage
Informatics Lead
For further information, please contact Sarah Smith.
Email: sarah.braidford-smith@nhs.net • Tel. 0113 206 5450
3031
Published by the Quality Improvement Team The Leeds Teaching Hospitals NHS Trust June 2017 MID Code: 20161130_010/NR
You can also read