Multisystem Inflammatory Syndrome in Children (MIS-C) and COVID-19
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Multisystem Inflammatory Syndrome
in Children (MIS-C) and COVID-19
ALLISON AGWU, MD, ScM
Associate Professor of Pediatric and Adult Infectious Diseases
NICOLE SALAZAR-AUSTIN, MD
Assistant Professor of Pediatrics
JODY HOOPER, MD
Associate Professor of Pathology
Session Overview • Epidemiology of COVID-19 in children • Clinical case presentation • Review of MIS-C clinical characteristics • Discussion of therapeutic options for MIS-C • Pathology presentation • Discussion

Epidemiology of COVID-19 in Children

Data in Children: China • Nationwide case series of 2135 pediatric cases of SARS-CoV-2 infection reported to Chinese CDC from 1/16/20 through 2/8/20 • Children =

Data in Children: China
• Illness severity definitions
• Asymptomatic: + SARS-CoV-2 PCR, no signs/symptoms, normal CXR
• Mild: Upper respiratory tract symptoms OR only digestive symptoms without
fever, normal lung exam
• Moderate: Pneumonia, not hypoxic, no SOB, abnormal lung exam OR no signs
or symptoms but CT findings of lung lesions
• Severe: Symptoms + oxygen saturation is
Data in Children: China
• Median age 7y [IQR 2-13 years]
• 1208 (56.6%) male
• >90% asymptomatic, mild, or moderate disease
• 94 (4.4%) asymptomatic, 1088 (51.0%) mild, 826 (38.7%) moderate
• 5.9% severe or critical (18.5% of adult cases in China severe or critical as
of Feb)
• 1 death
• Severe and critical cases by age group
• 10.6%
Data in Children: China
Dong Y et al. Pediatrics. 2020 Jun;145(6):e20200702. doi: 10.1542/peds.2020-0702. Epub 2020 Mar 16.
Data in Children: China
• Median number of days from illness onset to diagnosis = 2 days
(range: 0–42 days)
• Most cases diagnosed in the first week after illness onset occurred
Dong Y et al. Pediatrics. 2020 Jun;145(6):e20200702. doi: 10.1542/peds.2020-0702. Epub 2020 Mar 16.
Data in Children: United States • Baseline US demographics • 22% of population comprised of infants, children and adolescents 890,000 cases and >45,000 deaths worldwide • 239,279 cases and 5443 deaths in the US • Analysis of 149,760 laboratory-confirmed cases 2/12 through 4/2 • 2572 (1.7%) among children aged

Data in Children: United States
• 2572 pediatric cases • Median age 11 years
• 850 (33%) from New York City • 813 (32%) reported cases in
• 584 (23%) from the rest of New children 15-17y
York state • 682 (27%) in children 10-14y
• 393 (15%) from New Jersey • 398 (15%) in children agedData in Children: US Demographics
• 1408 (57%) in males (vs 53% in adults aged ≥18y)
• Predominance of males in all pediatric age groups
• Among the 184 (7.2%) with known exposure information:
• 168 (91%) had exposure to a COVID-19 patient
• 16 (9%) associated with travel
• Underlying conditions (data available on 13%)
• 23% had at least one, including all six admitted to ICU
• Most common: chronic lung disease, cardiovascular disease,
immunosuppression
MMWR Morb Mortal Wkly Rep 2020;69:422–426. DOI: http://dx.doi.org/10.15585/mmwr.mm6914e4Pediatric Clinical Data
• Signs and symptoms (data available
on 11% of patients)
• 73% had fever, cough, or dyspnea (vs.
93% adults 18-64y)
• 56% fever; 54% cough; 13% dyspnea
• Versus 71%, 80%, and 43% among adults
18-64y
MMWR Morb Mortal Wkly Rep 2020;69:422–426. DOI: http://dx.doi.org/10.15585/mmwr.mm6914e4Pediatric Clinical Data: U.S.
• Hospitalization status (data available on 29%)
• 5.7% hospitalized (vs 10% adults 18-64y)
• 0.58% to ICU (vs 1.4%)
• 20% of those for whom status known (vs. 33% adults)
• 2% to ICU (vs. 4.5%)
• ChildrenTake-Home Points • COVID-19 is typically less severe in children than adults • Serious illness resulting in hospitalization still occurs • Slight preponderance of cases in boys • Physical distancing and other measures remain important given concern that less symptomatic persons may still contribute to disease transmission
Multisystem Inflammatory Syndrome in
Children (MIS-C)Clinical Case
Case Presentation • 15 year old previously healthy African American female presented to another hospital with one week of epigastric pain, initially waxing and waning, then progressively worsening with loss of appetite. • 2 days prior to admission developed nasal congestion and rhinorrhea without sore throat, dyspnea, or cough. She also endorsed loss of smell and taste, which she attributed to nasal congestion. • One day prior to presentation developed myalgia • ROS: negative for fever, headache, nausea, vomiting, diarrhea, vaginal discharge (LMP 1 week prior to symptoms), urinary symptoms
History • PMH: none • SH: lives with mother and 2 sisters (both had sore throat and cold- like symptoms the week prior); +social distancing • FH: MGM hypothyroid
At the First Hospital • PE: T 36.5°C HR 88 RR 18 O2 Sat 100% on RA • mild epigastric tenderness without rebound/guarding • WBC 18.9 S15.7% • Urinalysis negative, urine pregnancy test negative • SARS-CoV-2 PCR NEGATIVE • Abdominal CT: Fat stranding and prominent lymph nodes (
JHU ED course • Tm 38.1°C HR 90s-110s BP 110s/50s Weight 95.7 kg (BMI 31) • PE: RUQ tenderness without rebound or guarding. • Labs: WBC 16.2 (S-91% L-5% M-1.5%), ALC 790 • Chemistries, urinalysis: unremarkable • ESR 74 CRP 24.3 • SARS-CoV-2 PCR NEGATIVE • GC/CT NEGATIVE • GI cocktail à unclear improvement, admitted for observation
Hospital Course • HD #1-2 (illness day 8-9): abdominal pain and fluid intake improved, but continued to have fever and tachycardia • Tm 38.9°C CRP 24.3 ESR 74 • HD #3 (illness day 10): worsening abdominal pain, diffuse myalgia (diffuse paraspinal), throat discomfort (L>R), pleuritic chest discomfort without shortness of breath. Faint erythematous maculopapular rash noted on chest, back, palms, and soles. • Tm 37.7°C, d-dimer 1.09, CRP 30.4, LFTs nl, troponin
Hospital Course • HD#4 (illness day 11): developed worsened fever (39.9°C), continued abdominal discomfort, tachycardia, hypotension requiring fluid boluses, and increased work of breathing. Transferred to PICU • CRP 33.7 ESR 107 d-dimer 1.55 • WBC 27.7 B-43% • Troponin >.04, proBNP 652, Fibrinogen 965 mg/dL (170-422) • Repeat imaging à
HD #1 HD #4
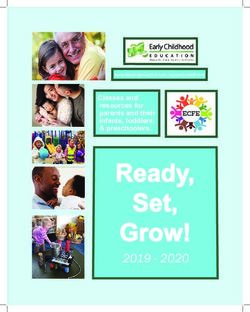
A C Figure 1. Imaging at hospital admission (Panels A and B)
and at admission to the PICU (Panels C and D). Axial CT of
the chest showed normal lungs (Panel A) with coronal IV
contrast enhanced CT (Panel B) showing enlarged
mesenteric and retroperitoneal nodes (arrows) and normal
bowel. On HD 4, repeat chest CT (Panel C) showed bilateral
lower lobe consolidation without pulmonary embolism
and coronal IV contrast enhanced CT (Panel D)
demonstrated new wall thickening of the distal transverse
colon, gallbladder wall edema, and mesenteric stranding
(arrows). Both chest and abdominal CT at that time
B D showed prominent diffuse supraclavicular, hilar,
mediastinal, abdominal, and retroperitoneal
lymphadenopathy (Panels C and D).MIS-C: Clinical Characteristics
Initial Report: Hyperinflammatory Shock Similar to Kawasaki
Disease and Toxic Shock Syndrome During the COVID-19
Pandemic
• Cluster of 8 children in London, mid April 2020
• Unrelenting fever, rash, conjunctivitis, peripheral edema, generalized extremity pain, GI
symptoms
• Warm, vasoplegic shock
• Refractory shock requiring ECMO (n=1)
• Children age 4 - 14 years without significant comorbidities
• Hyperinflammation: elevated CRP, procalcitonin, ferritin, TAG, D-dimer
• Dilated coronary vessels, giant coronary aneurysm; biventricular dysfunction
• All SARS-CoV-2 PCR negative; several with household exposures
Riphagen. Lancet 6 May 2020Second Case Report Describing New Syndrome Similar to
Kawasaki Disease During the COVID-19 Pandemic
Incidence of Kawasaki Disease Timing of KD Cases Among ED Visits
Bergamo, Italy 2015-2020 during COVID Epidemic
Bergamo, Italy Feb-Apr 2020
4-6 weeks after height
of epidemic
30-fold increased incidence of Kawasaki Cases appeared 4-6 weeks after peak
Disease COVID-19 cases
Suggests post-infectious inflammatory
syndrome
Verdoni, Lancet May 13, 2020Kawasaki Disease (KD) • Acute, self-limiting vasculitis of medium-size vessels involving multiple organs • 10x more common in Japan than US • Winter/spring predominance, often clustered • Associated with HCoV-NH and HCoV-229E • Young children • >90% of cases
Kawasaki Disease (KD) • Presentation: Fever, bilateral nonexudative conjunctivitis, mucositis, polymorphous rash, extremity changes, cervical lymphadenopathy • Inflammatory state: • ↑WBC, Plt, CRP, ESR, ↑AST/ALT, ↓albumin, normocytic anemia, sterile pyuria • Cardiac Involvement • Reversible coronary artery dilation or aneurysm • Mild to moderate ventricular dysfunction common • Rarely severe (KD Shock Syndrome) with associated myocarditis
Multisystem Inflammatory Syndrome (MIS-C) in Children
also known as Pediatric Inflammatory Multisystem Syndrome (PIMS-TS)
CDC Criteria WHO Criteria
• < 21 years • 0-19 years of age
• Fever for ≧24 hours • Fever >3 days
• Multisystem (≧ 2) involvement • Two of the following:
• Rash or bilateral nonpurulent conjunctivitis or mucocutaneous
• cardiac, kidney, respiratory, hematologic, signs
gastrointestinal, dermatologic or neurologic • Hypotension or shock
• Laboratory evidence of inflammation: • Myocardial dysfunction, pericarditis, valvulitis, coronary
abnormalities
• Increased CRP, ESR, Fibrinogen, D-dimer, Ferritin, LDH, • Coagulopathy (RT, APTT, D-dimer)
IL-6
• Acute gastrointestinal problems (v/d/pain)
• Low albumin
• Elevated neutrophils, reduced lymphocytes • Elevated markers of inflammation (ESR, CRP,
procalcitonin)
• No alternative diagnosis
• No other obvious cause
• Positive SARS-CoV-2 (PCR, serology, antigen) or • Positive COVID-19 testing or likely contact with
known exposure within the prior 4 weeks COVID-19
Royal College of Physicians (UK): Fever, Inflammation, Single or multiorgan dysfunction with special characteristics, No
alternative diagnosis, +/- evidence of SARS-CoV-2MIS-C Presentation Similar to but Different from Kawasaki
Disease
• Older children (median 7-10 years)
• Prominent GI symptoms (50-95%)
• Exploratory laparotomy in several patients
• Prior to onset of KD-like symptoms and shock
• Neurologic (20-30%)
• Irritability, headache, confusion and meningeal
signs
• Polymorphous Rash (50-60%)
• Maculopapular, targetoid, etc.
• High proportion of patients with cardiac
dysfunction and shock (45-80%)
• LVEFWider Spectrum of Illness than Initially Described
• Retrospective case series at 8 hospitals in the UK
• Collected all clinical and laboratory data on children meeting UK, WHO
and/or CDC criteria
• 3 Distinct Syndromes
1. Persistent fever and elevated inflammatory markers (n=23)
2. Kawasaki Disease-like (n=13)
3. Shock with clinical, echo and lab evidence of myocardial injury (n=29)
Whittaker, et al. JAMA 8 June 2020Inflammatory Markers Distinguish MIS-C from other Pediatric
Inflammatory Disorders
Higher Lower
Older Age Higher WBC Neutrophil Count Lymphocyte Count Lower Platelet Count
Higher CRP Higher Ferritin Higher Troponin Higher D-dimer
Whittaker, et al. JAMA 8 June 2020Inflammatory Markers Distinguish Children with MIS-C at
Risk of Shock but not Coronary Artery Abnormalities
• Children with MIS-C and shock showed signs of higher inflammation and cardiac damage
• Higher CRP and neutrophil counts, lower lymphocyte counts and albumin
• Elevated troponin and proBNP
• No clinical or laboratory markers distinguished children with MIS-C who developed
coronary artery dilatation or aneurysms (n=8)
• Found in all 3 subsets
• Not associated with degree of inflammation
• Important implications for evaluation and treatment
• No distinguishing laboratory characteristics for children who did and did not have
evidence of SARS-CoV-2
Whittaker, et al. JAMA 8 June 2020Clinical Case
Hospital Course (cont’d) • HD#4 (illness day 11): • ECHO: normal LV systolic function, normal coronary arteries • Received cefepime, metronidazole, doxycycline • Initially improved and weaned vasoactive support
Hospital Course (cont’d)
• 12 hours after transfer to PICU
• SARS-CoV-2 IgG and IgA positive
• IVIG administered due to concern for MIS-C
• Developed progressive hypoxemic respiratory failure à intubation
• Hypotension developed post-intubation, requiring norepinephrine and
vasopressin support
• Ultrasound: severely diminished LV EF and adequate right ventricle filling with
normal septal position. Pro-BNP 8328 pg/mL
• IL-6 239 CRP 30.9 ESR 118
• WBC 37.5, B-28%, ALC 750, PLT 280KMIS-C: Treatment
Treatment of Kawasaki Disease
• IVIG
• Reduced coronary artery aneurysms by 75% and mortality by 95% when given in the
first 10 days of illness
• ASA
• Reduce risk of coronary thrombosis, given for 4-6 weeks
• Enoxaparin for large/giant aneurysms
• Steroids
• IVIG non-responders or at high risk of IVIG resistance
• Immunomodulators for IVIG and steroid-resistant KD (10-15%):
• Infliximab
• Anakinra (Phase 1/II ongoing)
Newburger Circulation 2004 Tremoulet Lancet 2014
Burns PIDJ 1998 Burns J Pediatr 2008
Kobayashi Lancet 2012 Dusser Front Pharmacol 2017Minimal Data to Guide Treatment of MIS-C
• General Approach • Treatment
• Apply KD therapeutic • IVIG: Universal
principles • ASA: coronary artery abnormalities and KD
• Individualized Plans • Steroids: Shock, ventricular dysfunction
• Collaborative approach • Immunomodulators: Unresponsive to IVIG and
between many subspecialties steroids
• Anakinra, Infliximab, Tocilizumab
• Outcomes
• Limited data
• Rapid recovery with IVIG ± steroids
• Cardiac function restored in 70% by ICU
discharge
• Some deaths reported
Riphagen. Lancet 6 May 2020 Toubiana BMJ 26 May 2020
Verdoni, et al. Lancet 13 May, 2020 Whittaker, JAMA 8 June 2020
Belhadjer. Circulation 17 May 2020 Capone J Pediatrics 10 June 2020Clinical Case
Hospital Course (cont’d)
• PICU course
• Hypotension persisted despite bolus epinephrine à pulseless electrical
activity arrest à CPR à quick return to perfusing rhythm à 2 additional
PEA arrests
• Attempt to initiate ECMO (refractory hypotension and cardiac dysfunction),
unsuccessful due to engorged femoral vein and retrograde flow into the
femoral artery.
• 90 minutes of CPR following 3rd arrest, resuscitative efforts were ceased
• 3rd SARS-CoV-2 PCR positiveAutopsy Findings
Jody E. Hooper, MD
Director of Autopsy
Director, Legacy Gift Rapid Autopsy Program
Associate Professor of Pathology and OncologyAutopsy Results • Diffuse cardiac inflammatory infiltrate, most marked in septum. • Inflammation in small arterioles, veins, & lymphatics. • Only very focal myocardial damage seen. • No significant inflammation in other organs. • No significant abdominal/GI findings. • Limited procedure did not verify clot in aorta. • Inflammatory syndrome likely caused more myocardial damage than visible, triggering sequence of events ending in death.
MIS-C: Key Points • There appear to be three distinct syndromes: • Prolonged fever with elevated inflammatory makers with variable symptoms • Syndrome similar to Kawasaki disease • Shock with myocardial injury • There is no single diagnostic test, though patterns of inflammatory markers distinguish it from other pediatric inflammatory disorders • Most children have a rapid recovery with IVIG and Steroids • There are limited data on long-term outcomes
“Please say her name and share her story. Teach others. I don’t
want my baby to have died in vain.”SLIDES & RECORDINGS ARCHIVED ONLINE https://bit.ly/2Y2DIDj
You can also read