Monkeypox in Nigeria: by Dimie Ogoina - WHO | World ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Monkeypox in Nigeria:
Epidemiology, surveillance, and laboratory capacity:
what else is needed?
by
Dimie Ogoina
MBBS, FMCP-Infectious Diseases, FWACP, FACP
Niger Delta University/Niger Delta University Teaching Hospital, Bayelsa,
Nigeria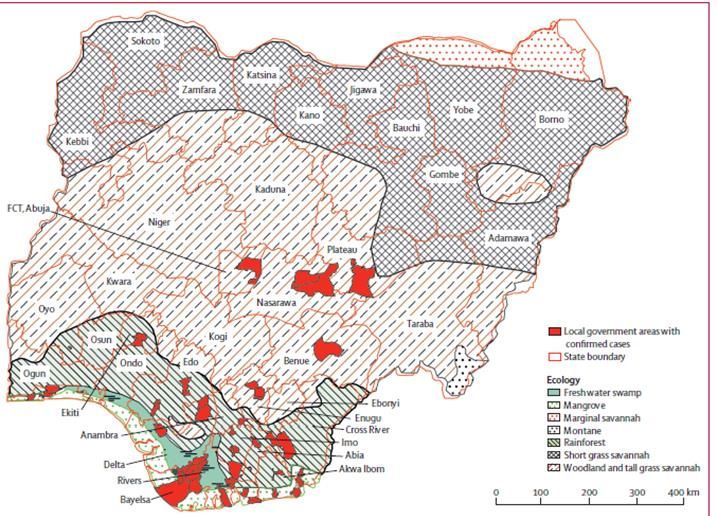
Outline • Introduction • Epidemiology of monkeypox in Nigeria • Root drivers of monkeypox re-emergence in Nigeria • What else is needed: recommendations

Global distribution of human monkeypox (HMPX)
As of 29th May 2022
https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON385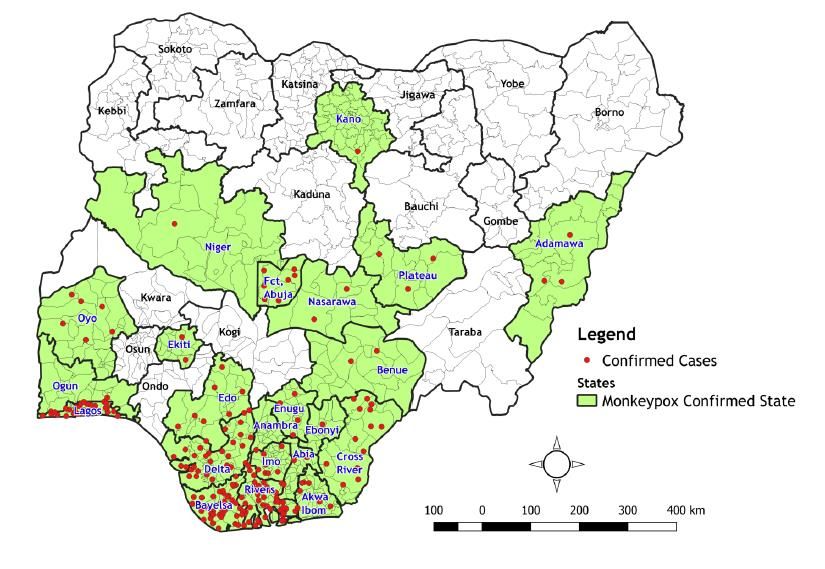
History of human monkeypox in Nigeria
• First case of human monkeypox in Nigeria
was reported in April 1971
• 4yr old female (unvaccinated)
• 24yr mother infected by 2° transmission
(unvaccinated)
• Unknown exposure
• Both recovered
• Third human case reported in Nov 1978 1978 Oyo
• 35yr old male (unvaccinated)
• Unknown exposure- said to occasionally
consume bush meat
Abia 1971
• Recovered
• Animal surveillance
• Orthopoxvirus serology was negative in 55
patas monkey screened
Breman JG et al: Bulletin of the World Health Organization, 58 (2): 165-182 (1980)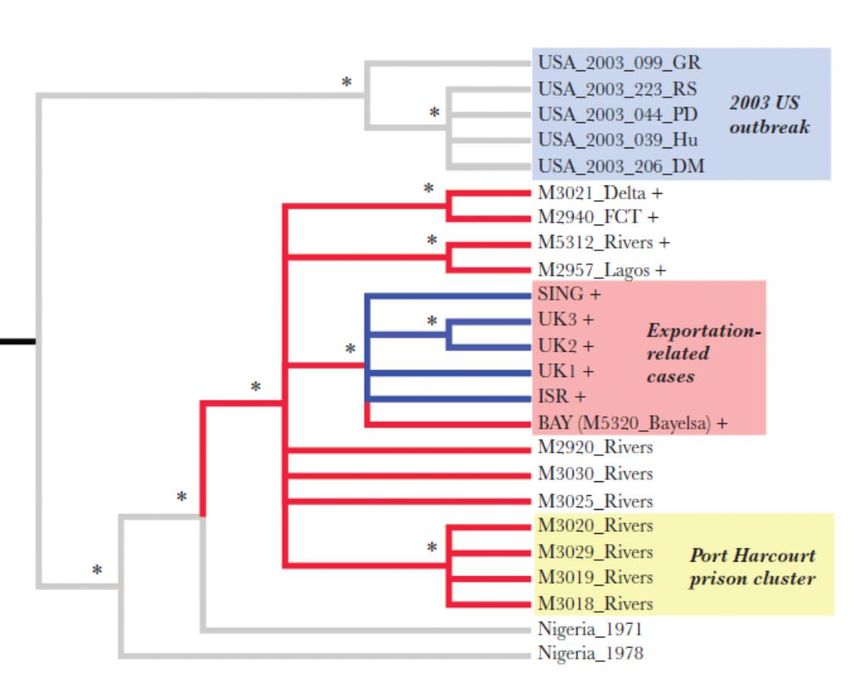
The 2017 human monkeypox outbreak in Nigeria
• After 38years, Nigeria
experienced a re-emergence of
human monkeypox outbreak in
Sept 2017
• Caused by the West African clade
of the monkeypox virus
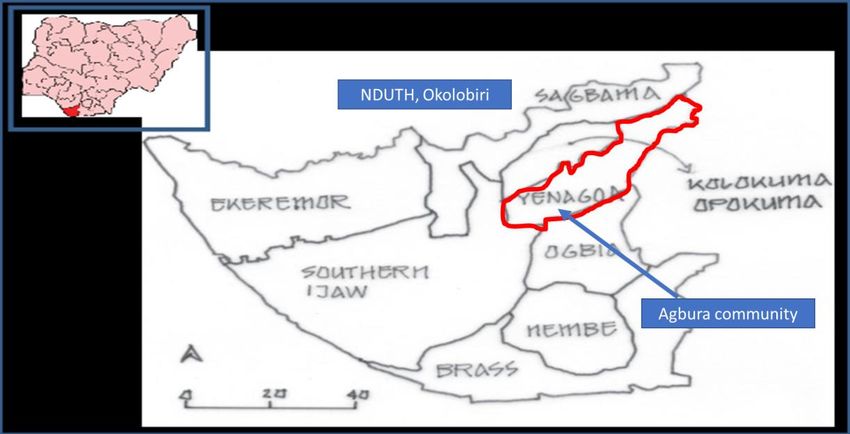
• First case reported in Bayelsa
state; managed at NDUTH
situated in the Niger Delta
Region of Nigeria
Lancet Infect Dis. 2019;19(8):872-879. doi:10.1016/S1473-3099(19)30294-4 https://ncdc.gov.ng/diseases/sitreps/?cat=8&name=An%20Update%20of%20Monkeypox%20Outbreak%20in%20Nigeria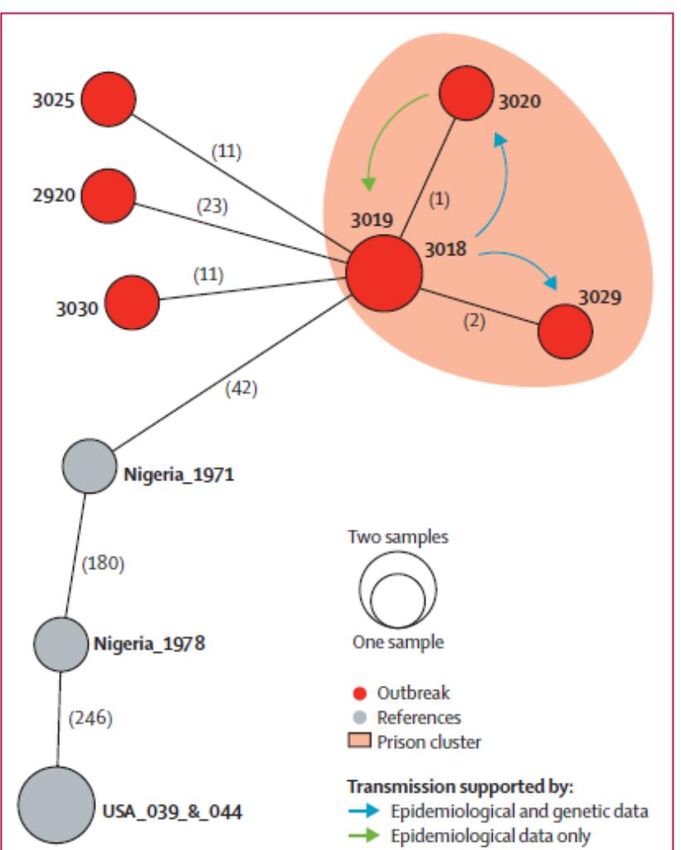
The Index patient (2017 HMPX outbreak in Nigeria)
• The index case
• 11-year-old boy with an 11-day history of fever,
generalized rash, headache, malaise, and sore throat
• Papulopustular rashes on the trunk, face, palms, and
soles of the feet. Associated oral and nasal mucosal
lesions and ulcers and accompanying generalized
lymphadenopathy
• Five other family members in the same household had
similar symptoms
• Uncle of index patient had vesiculopustular lesions
about 1 month earlier.
Emerg Infect Dis. 2018;24(6):1149-1151. doi:10.3201/eid2406.180017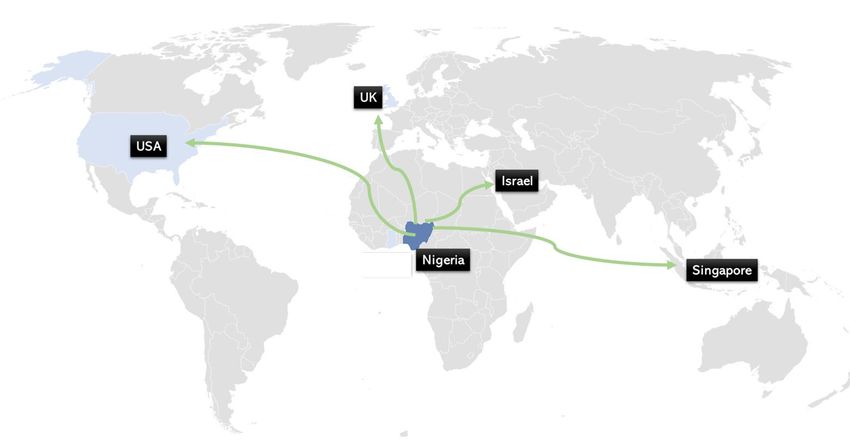
Initial laboratory diagnosis
• Laboratory diagnosis (by real-time PCR, IgM serology, and genomic
sequencing) were initially undertaken at
• Institut Pasteur (Dakar, Senegal), Redeemer’s University Laboratory (Ede,
Nigeria), and
• the US Centers for Disease Control and Prevention (Atlanta, GA, USA).
• Further diagnostics took place later at the NCDC National Reference
Laboratory
• with technical support from the US Centers for Disease Control and
Prevention.
Initial laboratory diagnosis
• Laboratory diagnosis (by real-time PCR, IgM serology, and genomic
sequencing) were initially undertaken at
• Institut Pasteur (Dakar, Senegal), Redeemer’s University Laboratory (Ede,
Nigeria), and
• the US Centers for Disease Control and Prevention (Atlanta, GA, USA).
• Further diagnostics took place later at the NCDC National Reference
Laboratory
• with technical support from the US Centers for Disease Control and
Prevention.
Geographical distribution of cases
Epidemiological features of
2017 outbreak (1)
• Between Sept 11, 2017, and Sept 16, 2018
• 276 suspected cases in 26 (70%) of States
• 118 (43%) confirmed cases in 17(46%) of States
• 4(1%) probable cases
• 7 (3%) deaths.
• Most cases were reported in the urban LGAs of
affected states
• 41 (34%) of all confirmed or probable cases were Temporal distribution of cases in Nigeria, 2017–18 (n=276)
reported in 2 LGAs in Rivers and Bayelsa states.
• Among 253 patients tested
• 104 (41%) had positive PCR results
• 14 (6%) had positive IgM results only.
• 135 (53%) patients negative for monkeypox virus
• 15 (11%) were positive for orthopoxvirus IgG.
Lancet Infect Dis. 2019;19(8):872-879. doi:10.1016/S1473-3099(19)30294-4Epidemiological features of 2017 outbreak (2)
• Age and sex distribution
• Median age-29 years
• (IQR 14; range 2 days to 50 years)
• 84 (69%) were male
• Occupation
• 24 (26%) –traders
• 18 (20%)-students
• 14 (15%) artisans
Age and sex distribution of cases in Nigeria, 2017–18
• 5 (5%)- each farmers, prison-inmates
• 4 (4%)-each teachers, housewives, health
workers
• 7(8%) children.
• Others- 2 (2%)-religious leaders, 2 (2%) factory
workers, 1 (1%) naval officer, 1(1%) was a
security guard
Lancet Infect Dis. 2019;19(8):872-879. doi:10.1016/S1473-3099(19)30294-4Epidemiological features of 2017 outbreak (3)
• Epidemiological link
• Of 122 cases, 36 (30%) had a link with people with similar lesions
• Of these 36 people, 12 (33%) were epidemiologically linked with a confirmed case.
• 7(58%) of these 12 people shared a household or had intimate contact with a confirmed case,
• 4 (33%) were inmates in the same prison as a confirmed case, and
• One was a health worker who treated a confirmed case.
• Cohort in Bayelsa had history of high-risk sexual behaviour (unpublished data)
• Incubation period – 3-34 days (median 9.5 days)
• Largest household clusters- 6 members (3 confirmed, 3 probable)
• Animal exposure- 10 (8.2%) patients reported contact with animals
• Two each with monkeys, rodents, and unspecified wild animal [consumed as meat—i.e., bush
meat]
• Four with domestic animals).
• No one reported contact with sick or dead animals.
Lancet Infect Dis. 2019;19(8):872-879. doi:10.1016/S1473-3099(19)30294-4Clinical features of human monkeypox in Nigeria (2017-2018)
(Epid. data-all cases)
• Fever not reported in 12% of
cases
• Distribution of rash:
• Face (95.4%)
• Legs (91.9%)
• Trunk (81.0%)
• Upper limbs (76.6%)
• Palms (71.4%)
• Genitalia (66.1%)
• Soles (63.3%)
Lancet Infect Dis. 2019;19(8):872-879. doi:10.1016/S1473-3099(19)30294-4Review of clinical management of hospitalized monkeypox patients during
the 2017-2018 outbreakMethodology • Retrospective review of case records of 40 HMPX patients hospitalized during the 2017-2018 outbreak in Nigeria. • Using a standardized checklist, we documented: • Constitutional signs and symptoms at presentation • Characteristics of skin rash • Systemic symptoms and signs • Clinical course and complications • Treatment received and sequelae at discharge or on follow-up • HIV status of each case • Differences in study variables in relation to HIV status were determined
Findings (1)
• The cases were 28 days to 54 years of age
(median, 32 years) and the majority (77.5%)
were male.
• Of 35 cases who gave details of their first
symptom,
• 23 (65.7%) had rash as the first symptom, while 12
(34.3%) had fever as first symptom.
• In 2 patients, genital rash associated with ulcer was the
first symptom.
• Skin rashes were observed on the following
sites:
• face (97.5%), trunk (92.5%), arms (87.5%), legs (85%),
genitalia (67.5%), scalp (62.5%), palms (55%), soles
(50%), mouth (37.5%), and eyes (25%).
• One case of concomitant chickenpoxFindings (2)
• Lymphadenopathy was observed in the following sites:
• cervical (n = 11), submental (n = 5), inguinal (n = 12), axillary (n = 10), and generalized (n = 12).
• Twenty-one of 40 (52.5%) cases developed 1 or more complications, including
• Secondary bacterial skin infection (n = 19)
• Gastroenteritis (n = 5)
• Sepsis (n = 4)
• Bronchopneumonia (n = 3)
• Encephalitis (n = 3)
• Keratitis (n = 3)
• Premature rupture of membrane at 16 weeks’ gestation and resultant intrauterine fetal death
(n = 1).
• All diagnoses were based on clinical judgement of the attending physician.
• Distressful complaints- Disfigurement from widespread skin lesions, pruritus, painful
pustular lesions, and genital ulcers
• Eleven of the 40 (27.5%) patients developed anxiety and depression requiring
psychological counseling.Monkeypox and HIV Type 1 Coinfection
• There were 9 HIV type 1 (HIV-1)/monkeypox-coinfected patients:
• 4 with newly diagnosed HIV-1 infection and 5 patients previously on
antiretroviral therapy (ART).
• Three of these 5 cases had apparently failed first-line ART and their CD4
cell counts at hospitalization were 101, 354, and 357 cells/μL,
respectively. The case with a CD4 count of 357 cells/μL had a viral load of
4798 copies/mL.
• Three of the 4 newly diagnosed HIV cases had CD4 counts of 20, 55, and
300 cells/μL. CD4 cell counts, and HIV viral loads were not available for
other patientsTable 1: Study variables in relation to HIV status (1)
Study variables Total HIV+ HIV- HIV+ vs HIV p value
N (%) N (%) N (%) OR (95% CI) P value
Age group (years) 0.12Table 1: Study variables in relation to HIV status (2)
Clinical Management of Patients
• Mainly symptomatic • Major symptoms and signs requiring
• Protect compromised intervention
skin and mucous • High grade fever with chills and rigors
membrane • Pruritus
• Nutritional support • Pain- mainly genital ulcer and ulcerated
• Psychosocial support scalp rash pain
• Treat co-morbidities • Skin rash with/without secondary bacterial
infection
• Oral sores
• Vomiting and dehydration
• Sore throat
• HIV co-infection
• Fear and anxietySpecific treatment of symptoms and signs
Symptoms/signs Management Remarks
Fever Stepid sponging Chills and rigors were especially common in
Antipyretics- PCM hospitalised patients
Itching/Pruritus Warm bath/warm clothing In most cases, this symptom was self limiting
Calamine Lotion
Antihistamines- Lorantidine
Oral sores Warm saline gurgle, vitamin C, multivitamins
Skin rashes/secondary Antiseptic cleaning Thirty-five (87.5%) of 40 patients had one or
bacterial infection Antibiotics- mainly ceftriaxone, amoxycillin and more antibiotics prescriptions.
metronidazole
Genital ulcers Warm saline Sitz bath (for vulvo-vagina ulcers) genital ulcers were dressed in gauze soaked with
Antiseptic cleaning/Honey antiseptic (Eusol) or Honey or Sofra-Tulle.
Light Sufratule dressing
Pain PCM or NSAIDS Majority improved on PCM. A few required
NSAID
Dehydration IV fluids D/S or N/S
Poor appetite Diet by choice Free meals were provided: patients were asked
to indicate what they wanted to eat
Anxiety/fear Counselling and reassurance Co-ordinated by psychiatrists and medical social
workersManagement of complications • Sepsis – antibiotics • Bronchopneumonia- antibiotics, empirical acyclovir, oxygen therapy • Secondary bacterial skin infection- antibiotics, skin care • Encephalitis- antibiotics, empirical acyclovir, anti-seizure • Miscarriage- evacuation, antibiotics • Gastroenteritis- rehydration, IV fluids • Keratitis-topical antibiotics, Vitamin A supplements
Outcome
• Five of the 40 (12.5%) cases died:
• 34-year-old man who died by suicide
• Female neonate aged 28 days -bronchopneumonia and encephalitis;
died after 8 days;
• 42-year-old man with HIV-1 infection – Sepsis; died after 37 days
• 43-year-old man with HIV-1 infection -CD4 count < 20 cells/μL; died
from encephalitis
• 27-year-old HIV-negative man- bronchopneumonia and sepsis; died
after 9 daysClinical sequelae • Only 18 of 35 HMPX survivors were seen on follow-up (1–8 weeks after discharge) • Sequelae observed in these cases included: • Hyperpigmented atrophic scars (n = 12) • Hypopigmented atrophic scars (n = 7) • Patchy alopecia (n = 6) • Hypertrophic skin scarring (n = 3) • Contracture/deformity of facial muscles (n = 1) • Repeat infection in a healthcare worker (10 months after 1st infection)
Clinical pictures
Active lesions Healed lesionsGenomic surveillance
• 7 samples sequenced from one
state (Rivers)
• Samples had >42 SNPs
difference from 1971 Nigerian
outbreak
Haplotype network of seven monkeypox samples from Rivers state, NigeriaAge and sex distribution of monkeypox (2017-
Human Monkeypox in Nigeria 2022 Nigeria)
(2017-2022)
Temporal trend of monkeypox in Nigeria (1970-2022)
Nigeria confirmed Monkeypox cases by the year of incidence-
September 2017- May 2022
State distribution suggesting monkeypox is Update of monkeypox in Nigeria.
moving outside the rainforest areas in Nigeria https://ncdc.gov.ng/diseases/sitreps/?cat=8&name=An%20Update%20of%20Monkeypo
x%20Outbreak%20in%20NigeriaExportation of monkeypox frow Nigeria (2018-2021)
Country 2018 2019 2020 2021
United States 2 (Travel-Nigeria)
United Kingdom 3 (Travel-Nigeria) 1 (Travel-Nigeria) 3 (Travel-Nigeria)
Israel 1 (Travel-Nigeria)
Singapore 1 (Travel-Nigeria)
Mauldin MR et al. Exportation of Monkeypox Virus From the African Continent. J Infect Dis. 2022;225(8):1367-1376.Phylogenetic analyses
of exported cases
• Samples were within the West
African clade of MPXV
• Exported cases shared a most
recent common ancestor with a
Bayelsa case
• Conclusions
• intermediate levels of genetic
variation, suggest a small pool of
related isolates is the likely source
for the exported infections.
• Source likely from within the
contiguous region of Bayelsa, Delta,
and Rivers states, or
• another more estricted, yet
unidentified source pool.
Mauldin MR et al. Exportation of Monkeypox Virus From the African Continent. J Infect Dis.
2022;225(8):1367-1376.Factors determining monkeypox re-emergence in Nigeria
• Declining smallpox vaccine-related population immunity
• Estimated population immunity was 2.6% in 2016 before 2017 outbreak
• Possible increased human contact with animal reservoirs
• Facilitated by intra-country mobility, trade, deforestation, animal husbandry, and
climate change
• Increased human to human transmission
• Facilitated by new route of transmission (?sexual), immunosuppression and
• Microbial evolution
• Advancement in diagnostic capacity
• Heightened public awareness during the 2017 outbreak
Nguyen PY et al. Reemergence of Human Monkeypox and Declining Population Immunity in the Context of Urbanization, Nigeria, 2017-2020. Emerg Infect Dis. 2021;27(4):1007-1014Improved public awareness of monkeypox?
Google trends for ‘Monkeypox’ in Nigeria (2015-2022)
2015 2017 2019 2021 2022
Google trends for ‘Monkeypox’ Worldwide (2015-2022)
2015 2017 2019 2021 2022What else is needed?
Recommendations
• Major priority interventions
• Improve monkeypox-related surveillance
• Improve sub-national capacity for monkeypox diagnosis
• Knowledge gaps needing attention in Nigeria
• Identification of animal reservoirs in Nigeria
• Understand clinical spectrum and severity of disease, including asymptomatic
carriage and risk factors for acquisition
• Improved description of outbreak patterns by size and duration
• Best IPC practices to adopt in resource-limited settings
• EUA/ Clinical trials of novel drugs/vaccines in Nigeria
• Post-infection immunity/latent infection/relapse
• Monkeypox/HIV coinfection
• Laboratory features
• Sexual behaviour/STI and monkeypox
• Microbial causes of secondary infections in monkeypoxThank you for listening
You can also read