Molly, are these your bath salts? - A look at contemporary drug abuse 2014 Midwest Pediatric Trauma Conference
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Molly, are these your bath salts?
A look at contemporary drug abuse
2014 Midwest Pediatric Trauma Conference
May 2, 2014
1
Disclosures
I have no relevant financial
relationships to disclose.
Thanks for asking.
Rebecca L. Tominack MD
Medical Director, Missouri Poison Center
Adjunct Professor, Saint Louis University School of Medicine
and College for Public Health and Social Justice 2
In 2011, 1.25 million ED visits related to illicit drugs
& 1.24 million for nonmedical use of pharmaceutical
1 Cocaine 505,224
2 Marijuana 455,668
3 Heroin 258,482
4 Amphetamine /meth 159,840
5 PCP 75,538
6 Synthetic cannabinoids 28,531
7 MDMA (Ecstasy) 22,498
8 Bath Salts 22,904
9 Diphenhydramine 19,012
10 Dextromethorphan 14,684
3
Treatment priorities for bath salts/K2
• Calm the agitated patient
– Benzodiazepine: lorazepam, diazepam, midazolam.
– Add haloperidol or a 2nd generation antipsychotic
such as olanzapine (Zyprexa), ziprasidone (Geodon)
or risperidone
• If serotonin toxicity is suspected, can add
cyproheptadine or chlorpromazine
• Pulse ox, basic serum labs, CK, urine for myoglobin
• Supportive care including cooling, hydration,
electrolytes, oxygen, etc.
4
Designer drugs
• Designer drugs --Intentional, rational
chemical synthesis
• Known structure-activity relationships to
incorporate desired mechanisms of action
• Changing the molecular structure renders
the new molecule legal
• China is the main source
5
Synthetic cannabinoids
• Research compounds, to characterize the
newly discovered cannabinoid receptors
– Examples: JWH-018, CP-47,497, HU210,
AM2201, resurrected by illicit drug
manufacturers
• Supported by unprecedented internet
marketing, “user forums,” and bold
exploitation of loopholes in the drug
control laws
6
Structure-activity
THC relationship of
synthetic
cannabinoids
JWH018
4-5 x more potent
HU210
100-800 x more potent
Also an NMDA antagonist
7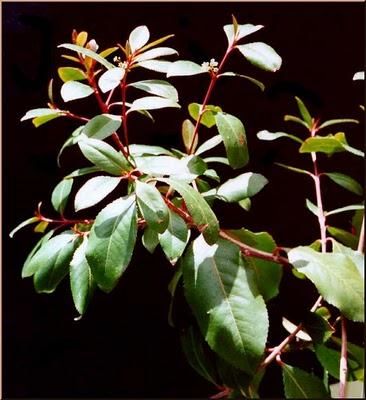
First seen as “brands” K2 and Spice as “herbal products” or “incense” blends Active agent Sprayed on unidentified vegetable matter 8

“Legal highs” sold in gas stations,
convenience stores, head shops.
Target teens and young adults
9
Note the reasonable price of $10 -15
10Synthetic cannabinoid presentation
• Significant psychotoxicity:
Paranoia, thought disorder, disorganized
behavior (ie, psychosis)
Anxious and depressed
Perhaps with intense suicidal thoughts or
behavior.
11Long duration of psychiatric features
• Abnormalities linger for days to weeks
• If K2-agent presentation includes
psychotic features, the duration of
hospitalization is 13 days vs 4-5 days
• Variations in the agent can cause variable
presenting symptoms
– Example: one K2 agent - and only one so far
- is specifically toxic to kidneys
12“Crazy Clown” toxicity in 22 patients
Brunswick, GA Aug 22 - Sept 9, 2013
• Nausea, vomiting (n = 8; 36%) • Confusion (n = 7; 32%)
• Tachycardia (n = 13; 59%) • Aggression (n = 7 32%)
• Hyperglycemia (n = 13; 59%) • Coma (n = 7; 32%)
• Seizures (n = 3; 14%)
• Hypokalemia (n = 9; 41%)
• 2 pneumonia, 1 rhabdo, 1 MI
• Acidosis (n=7; 32%)
ADB-PINACA (N-(1-amino-3,3-dimethy-1-oxobutan-2-yl)-
1-pentyl-1H-indazole-3-carboxamide), a previously
unrecognized synthetic cannabinoid related to indole
compounds recently identified in Europe and Japan
13“Bath salts”
• Not your mother’s bath salts
• Hallucinogenic amphetamines -- designer
chemistry and modern marketing
14Marketing & advertising of bath salts
• Packaged as innocuous household products:
bath salts, fertilizer/ plant food, stain remover,
etc
• True nature is passed by “word of mouth,” and
via the internet
• May also be sold as
“research chemicals”
• Either way, labeled “Not
for human consumption” to
to try to escape the drug control
laws
15Khat: the origin of bath salt chemistry A flowering shrub native to Ethiopia/Somalia region of Africa and Arabian peninsula, chewed as mild stimulant 16
Tender new shoots and leaves
17Must be used fresh to preserve potency
18WHO considers khat mild-moderately
habituating, not seriously addicting
19Cathinone (Khat)
CH3
Amphetamine Cathinone
More lipid soluble so
more CNS effects
20What can be done to enhance lipid
solubility and CNS action?
Add a methyl group
Amphetamine Methamphetamine
21Add a methyl group to cathinone
CH3
CH3 CH3
Cathinone Methcathinone
22Add yet another methyl group!
4-methyl methcathinone
“meow- meow”
Mephadrone
Internet available in 2007, spread throughout Europe by 2010
23Mephedrone , as shown on previous slide
• May also be sold as “research chemicals”
24Meow-meow mephedrone
• Nasal: Onset minutes; peak 30 min, lasts 2-3 hrs
• Euphoria, mood elevation, better mental
function, mydriasis, mild sexual stimulation
similar to cocaine, amphetamine, or Ecstasy
• Bruxism, tachycardia, sweating, poor
concentration and short term memory,
hallucinations, delusions, anxiety, paranoia
esp if high dose or prolonged/repeated use
25What else can be done with the basic
cathinone structure?
Make it a catechol like epinephrine, NE, dopamine
Norepinephrine Dopamine
Like NE except missing OH 26What does mother nature suggest?
• “Methoxy” groups on natural hallucinogens–
a combination of hydroxyl (such as on
dopamine) plus a methyl group for lipid
solubility and enhanced CNS effects
CH2
Mescaline in peyote Myristicin in nutmeg
27Methylene dioxy methamphetamine
CH3
CH3
methamphetamine
28Methylene dioxy methamphetamine
MDMA Ecstasy “Molly”
CH3
CH3
Methylene dioxy methamphetamine
29Ecstasy effects
• Releases serotonin, NE, DA and oxytocin -
hormone that facilitates bonding and
trust, released during birthing & lactation
• Unique effect - empathogen - feelings of
empathy, love, security, emotional
closeness
• Adverse effects: poor concentration,
bruxism, anorexia, dry mouth and thirst;
dehydration, hyponatremia
30Ecstasy overdose: serotonin toxicity
and/or stimulant psychosis with
amphetamine-like cardiovascular effects
• Hyperactivity, hyperthermia, hyper-
reflexia, muscle rigidity, rhabdomyolysis
• Confusion, agitation, paranoia, delusions,
hallucinations, amnesia, coma
• Tachycardia, hypertension, stroke, angina,
MI, dyspnea
31Serotonin…
5-HT; 5-hydroxy tryptamine
Note the
mixed-ring
indole
It has many actions, which it carries out mainly by
modulating the effects of *other* neuro-
transmitters; eg, enhances dopamine release
32The serotonin-dopamine connection
is seen in serotonergic psychedelics
• Excess dopamine activity induces
hallucinations & other features of psychosis.
• Certain serotonin-like agents induce
dopamine release so *they* cause
hallucinations.
–examples: Psilocybin, LSD
33Psilocybin “magic” mushrooms
4 position CH3
N CH3
Psilocin
5 position
Serotonin
34Lysergic acid
diethylamide (LSD)
Serotonin
35PCP; phencyclidine
Phenyl Cyclohexyl Piperidine
• Dissociative anesthetic, sigma agonist & NMDA
receptor antagonist, blocking glutamate action
• Detachment from immediate surroundings and
experiences; no pain registers
• Hallucinations, disordered thoughts,
catatonia…very close clinically to schizophrenia
• Also seen in ketamine, dextromethorphan, and
HU-211, a synthetic cannabinoid
36Dextromethorphan
PCP
37To understand the possible effects of a drug, consider all relevant
receptors that a drug interacts with
From Drugs, Brains and Behavior by C. R. Timmons & L. W. Hamilton
of 69 38N-BOMe derivatives (“N-Bomb”)
“Hallucinogenic empathogen”
2,5 I-NBOMe [2-(4-iodo-2,5- dimethoxyphenyl) -
N-[(2-methoxyphenyl)methyl]ethanamine]
CH3
CH3 CH3
Basically a double up on 2CI: 2,5-dimethoxy-4-
iodophenethylamine; also come in chloro and fluoro flavors 39The clinical bottom line on the current
trend in designer drugs
• Structures & mechanisms of action are being
mixed and matched so that distinctions
between types of agents are clinically
irrelevant
• Novel & untested agents, by-products from
uncontrolled synthesis, adulterants, co-
ingestants, underlying psychiatric conditions,
size of dose, frequency, route, chronicity, etc.
• Treat the patient, not the poison.
40Menu of possible effects • Psychosis including hallucinations, extreme agitation, disorganized thinking, paranoia, compulsion for violence and/or self-harm, which may not resolve quickly or completely • Serotonin toxicity including clonus, hyper-reflexia, agitation, diaphoresis, tremor, fever • Adrenergic overload including hypertension, tachycardia, arrhythmia, fever, restlessness, tremor, hyperglycemia, hypokalemia • Misc Catatonia, muscle rigidity, rhabdomyolysis, seizures, secondary trauma, direct renal toxicity, etc • Contributions from co-ingestants 41
Treatment priorities for bath salts/K2
• Calm the agitated patient
– Benzodiazepine: lorazepam, diazepam, midazolam.
– Add haloperidol or a 2nd generation antipsychotic
such as Olanzapine (Zyprexa), ziprasidone
(Geodon) or risperidone
• If serotonin toxicity is suspected, can add
cyproheptadine or chlorpromazine
• Pulse ox, basic serum labs, CK, urine for myoglobin
• Supportive care including cooling, hydration,
electrolytes, oxygen, etc.
42You can also read