Mobile health technology to improve maternal health awareness in tribal populations: mobile for mothers - Oxford Academic Journals
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Journal of the American Medical Informatics Association, 28(11), 2021, 2467–2474
doi: 10.1093/jamia/ocab172
Advance Access Publication Date: 30 August 2021
Brief Communications
Brief Communications
Mobile health technology to improve maternal health
awareness in tribal populations: mobile for mothers
Downloaded from https://academic.oup.com/jamia/article/28/11/2467/6359598 by guest on 28 October 2021
Avishek Choudhury ,1 Onur Asan ,1 and Murari M. Choudhury2
1
School of Systems and Enterprises, Stevens Institute of Technology, Hoboken, New Jersey, USA and 2Network for Enterprise
Enhancement and Development Support (NEEDS), Deoghar, Jharkhand, India
Corresponding Author: Onur Asan, PhD, School of Systems and Enterprises, Stevens Institute of Technology, 1 Castle
Point Terrace, Hoboken, NJ 07030, USA (oasan@stevens.edu )
Received 30 April 2021; Revised 29 July 2021; Editorial Decision 1 August 2021; Accepted 3 August 2021
ABSTRACT
Mobile health (mHealth) applications have the potential to improve health awareness. This study reports a
quasi-controlled intervention to augment maternal health awareness among tribal pregnant mothers through
the mHealth application. Households from 2 independent villages with similar socio-demographics in tribal
regions of India were selected as intervention (Village A) and control group (Village B). The control group re-
ceived government mandated programs through traditional means (orally), whereas the intervention group re-
ceived the same education through mHealth utilization. Postintervention, awareness about tetanus injections
and consumption of iron tablets was significantly (P < .001) improved in the intervention group by 55% and
58%, respectively. Awareness about hygiene significantly (P < .001) increased by 57.1%. In addition, mothers in
the intervention group who recognized vaginal bleeding, severe abdominal pain, severe blurring of vision, or
convulsions as danger signs during pregnancy significantly (P < .001) increased by 18.30%, 23.2%, 20.0%, and
4.90%, respectively. Our study indicates that despite the low literacy of users, mHealth intervention can improve
maternal health awareness among tribal communities.
Key words: mHealth, maternal health, sustainable development goals, health awareness, tribal mothers, antenatal care
INTRODUCTION Improving awareness regarding antenatal care (ANC) is one of
Most maternal deaths are avoidable, and the solutions to minimize many ways to minimize maternal health risks. ANC encompasses
maternal death are well known.1 Still, in 2016 about 830 women health awareness programs, such as prevention, detection, and treat-
died every day due to maternal health complications related to ment of existing ailments concerning maternal and child health.5
pregnancy.2 About 99% of global maternal deaths occur in devel- However, evidence shows that ANC has often been poorly executed,
oping countries—most often in rural areas, which contributes to underutilized,6,7 and disproportionately spread across the socioeco-
over half of these deaths.1 Authorities worldwide have been trying nomic gradient of developing nations.8–10 The lack of accessible
to minimize maternal deaths by fostering health awareness cam- healthcare resources11,12 also restricts people from availing them-
paigns at the community level.3 However, the effectiveness of selves of modern medicines. In addition, tribal and rural communi-
these health interventions or campaigns in rural societies has been ties typically refrain from modern healthcare13 and consider
negatively impacted primarily by 3 major factors: (a) Inadequate maternal death to be normal.14,15 Lack of maternal health aware-
antenatal care delivery, (b) Lack of maternal health awareness, ness has led to iron deficiencies16 (anemia and restricted fetal
and (c) Tribal belief systems.4 growth), tetanus toxoid (TT) infections,17,18 and poor hygiene (fail-
C The Author(s) 2021. Published by Oxford University Press on behalf of the American Medical Informatics Association.
V
All rights reserved. For permissions, please email: journals.permissions@oup.com
2467
2468 Journal of the American Medical Informatics Association, 2021, Vol. 28, No. 11
ure to comply with the “five cleans”: clean hands, surfaces, umbili- rather than written documentation was obtained. The consent form
cus, cord tie, and wrappings for the baby), causing harms, such as was read in Hindi by one of the project team members. All partici-
genital tract infection and puerperal sepsis.19 pants were informed that their participation was voluntary and that
Consumer health technology, particularly mobile health they had the right to skip questions they felt uncomfortable with or
(mHealth) technology, serves as a powerful tool for patient educa- stop answering at any time. Furthermore, they were informed that
tion.20 The Global Observatory for electronic health describes the data collected was intended for research purposes only.
mHealth as healthcare-related practice assisted by mobile devices.21
mHealth technologies have substantial potential to facilitate unprec- Study design
edented and tailored access to treatment advice.22 They are typically This was a quasi-controlled, cross-sectional analysis of 2 groups (ru-
used as digital tools to improve healthcare access by minimizing in- ral villages in India): (a) an intervention group receiving government
tervention costs and eliminating geographic barriers. mHealth’s text mandated programs through a mHealth application in Village A,
messaging interventions have improved maternal health by guiding and (b) a standard control group receiving government mandated
women through the various stages of pregnancy.23 mHealth technol- care programs through traditional means (orally) in Village B. These
Downloaded from https://academic.oup.com/jamia/article/28/11/2467/6359598 by guest on 28 October 2021
ogies have also demonstrated promising impacts on several public 2 villages have similar socio-demographics. Under the government
health issues, including patient management,24 communication in programs, community health workers visited pregnant women in
rural areas,25 family planning,26 and diabetes management.27 both villages and discussed maternal health concerns and measures
Mobile health applications are used in various areas; however, orally (one-to-one), ensured ambulance availability if needed, and
there is limited research capturing their effectiveness as an educa- provided financial incentives for women delivering at the hospital. In
tional tool, particularly in maternal health in developing countries the intervention village, the community workers leveraged mHealth
and rural communities.28 Thus far, most research in this domain has (MFM) technology to discuss maternal health concerns and meas-
emphasized developed nations28 where the consumers (mHealth ures. All communication occurred in their native language, Hindi.
users) are educated and/or typically familiar with smartphones in
general. However, mHealth projects are now being used in develop- Mobile health technology/mobile for mothers (MFM)
ing nations; therefore, it is essential to keep in mind the consumers’
MFM, a software application, was conceptualized by Network for
ability to interact with mobile phones. Furthermore, given the chal-
Enterprise Enhancement and Development Support (NEEDS), an In-
lenges faced in medical, especially maternal health, education in de-
dian nongovernmental organization (NGO), and Simavi, a Dutch
veloping countries (particularly issues of accessibility and
NGO. It was designed for low-literate users to operate on affordable
affordability), user-centered mHealth has enormous potential as a
Java-enabled phones or Android-based smartphones that run free
tool for teaching and spreading awareness.
and open-source applications containing registration forms, check-
This study implements a mobile health technology (mobile for
lists, tracking of danger signs, and instructional prompts. The MFM
mothers, MFM) as a supporting tool to improve maternal health
application consists of 4 modules: (1) Registration, (2) antenatal
awareness among tribal communities using a randomized quasi-
care, (3) intranatal care, and (4) postnatal care. In addition, the In-
controlled intervention.
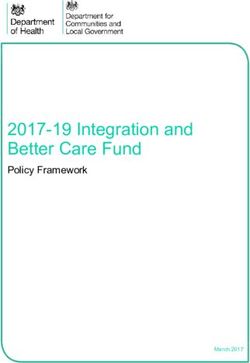
teractive Voice Recording System enabled mHealth to provide ma-
ternal health information through texts, photographs, and voice
prompts (in the user’s native language) to pregnant women and
MATERIALS AND METHODS mothers, as illustrated in Figure 1. All written information and voice
The study was part of a larger study conducted in collaboration with recordings were in the Hindi language .
the Rural Health Mission of the Government of Jharkhand under
the European Union-funded Initiative for Transparency and Good Intervention
Governance. The study received ethical clearance from the Institu- The intervention was led by trained, accredited social health acti-
tional Review Board Center, New Delhi, India. With consideration vists (ASHA). ASHA is a community-based health worker program
to the low literacy level among the study population, oral consent founded as part of the National Rural Health Mission by the Indian
Figure 1. Mobile for Mothers application (This is representative, the original language was Hindi).Journal of the American Medical Informatics Association, 2021, Vol. 28, No. 11 2469
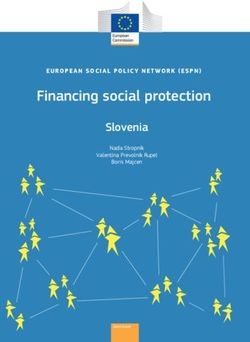
Ministry of Health and Family Welfare. ASHA staff visited each curred orally (one-to-one). Each encounter lasted for approximately
participant (mother) 4 times in the prenatal phase (the first visit oc- 45 minutes.
curring in the first trimester) and twice during the postnatal phase
(third and sixth month after childbirth), as illustrated in Figure 2. Data collection
The control group also received the same number of visits; however,
Pregnant mothers between the ages of 18 and 45 years were
ASHA workers did not use MFM with the control group. Each vil-
recruited from the control and intervention village, respectively. In
lage was allocated 400 ASHA workers (800 ASHA workers total).
January 2014, a team of trained project members administered a
During each home visit in the intervention group, the ASHA car-
paper-based survey to the mothers in 2 villages (control and inter-
ried and used the mHealth application to teach pregnant mothers
vention) to collect baseline data. Team members read the questions
about maternal healthcare and hygiene, as appropriate, at different
and marked the responses for all the participants including both illit-
stages of pregnancy. The intervention took place with one pregnant
erate and literate mothers. Note that ASHAs were not involved in
mother at a time (one-to-one counseling). Note that in the control
any survey data collection. The survey questionnaire was guided by
group, the same discussion about maternal health and hygiene oc-
the National Family Health Survey (NFHS)29 to assess maternal
Downloaded from https://academic.oup.com/jamia/article/28/11/2467/6359598 by guest on 28 October 2021
health and hygiene awareness, calculated as a binary variable where
Figure 2. Mobile for mothers intervention.2470 Journal of the American Medical Informatics Association, 2021, Vol. 28, No. 11
women were deemed aware of maternal health information if they Table 1. Demographics of the study population
responded “yes” correctly to the awareness questions suggested by
Control Intervention
NFHS (see Supplementary Appendix A).
N (%) N (%)
The mHealth intervention commenced soon after the baseline
survey was completed in early February 2014. The end-line (postin- Duration of stay in the village
tervention) data were collected between November 2015 and Janu- Less than 5 years 277 (37.4) 302 (40.8)
ary 2016. A team of trained project members who were familiar 5–10 years 338 (45.7) 35 (41.2)
with the region manually collected data by door-to-door visits using 11 years and above 125 (16.9) 133 (18.0)
Caste
the same approach as in baseline. Discussion confidentiality was
Scheduled Caste (SC)a 58 (7.8) 100 (13.5)
maintained, and no family members were allowed during the inter-
Scheduled Tribe (ST)b 22 (3.0) 27 (3.9)
vention and data collection to prevent external influences on the Other Backward Castes (OBC)c 523 (70.7) 542 (73.2)
respondents. Other than SC/ST OBC 63 (8.5) 69 (9.3)
Education level of women
Downloaded from https://academic.oup.com/jamia/article/28/11/2467/6359598 by guest on 28 October 2021
Illiterate 384 (51.9) 385 (52.0)
Data analysis
Primary (1–5years of schooling) 124 (16.8) 141 (19.1)
A priori power analysis was completed to estimate the minimum Secondary (6–10 years of schooling) 199 (26.9) 187 (25.3)
sample size for the study. This analysis included 2-tailed assump- Higher (11 and above years of schooling) 33 (4.5) 27 (3.6)
tions, an estimated power of 0.80, an alpha error probability of Occupational status of women
0.01, and an effect size of 0.2. The results of the a priori power anal- Working 56 (7.6) 95 (12.8)
ysis supported the inclusion of at least 1172 participants in data col- Housewife 684 (92.4) 645 (87.2)
lection. Age during intervention
First, we calculated descriptive statistics related to demo- 18–19 135 (18.2) 144 (19.5)
graphics. Then we calculated the percentage changes for each vari- 20–24 383 (51.8) 368 (49.7)
25–29 160 (21.6) 158 (21.4)
able between baseline and end line in each group. Finally, we used
30–34 47 (6.4) 49 (6.6)
the Pearson chi-square test of independence at a 99% confidence in-
35–45 15 (2.0) 21 (2.8)
terval to compare the percentage changes for each variable between Age at marriage of women
intervention and control groups. All analyses were conducted in Below 18 years 471 (63.6) 501 (67.7)
SPSS. 18 years and above 269 (36.4) 239 (32.3)
Religion
Hindu 684 (92.4) 556 (75.1)
RESULTS Muslim 47 (6.4) 173 (23.4)
Christian 4 (0.5) 8 (1.1)
The survey consisted of 1480 respondents, 740 women per group. Sarna 5 (0.7) 3 (0.4)
Table 1 shows the demographic characteristics of the respondents.
a
Table 2 shows all health and hygiene awareness of the study par- People belonging to Scheduled Castes (SC)—otherwise known as
ticipants before (baseline) and after (end-line) intervention. The “dalits”—are officially protected groups of individuals in the Constitution of
baseline and end-line columns report the percentage of participants India. This sub-community of the Indian caste system faces deprivation, op-
pression, and social isolation on account of their position at the very bottom
who responded correctly to the corresponding questions. The incor-
of the Indian caste system and perceived low status.30
rect responses were recorded separately as “No correct knowledge.” b
People belonging to Scheduled Tribes (ST) are indigenous individuals with
The Pearson chi-square compares the change in awareness between primitive traits, distinctive culture, and geographical and social isolation.30
the control and intervention groups between baseline and end-line. c
People who are identified (by the State and Central Government of India)
Our analyses indicated significant improvements after the as socially, economically, and educationally disadvantaged. However, there is
mHealth deployment in the intervention group compared to the con- still no clear definition for OBCs in the Indian Constitution.31
trol group. Although improvements were also noted in the control
group, the magnitude of improvements were significantly more in
the intervention group. We also observed negative change in the group who recognized vaginal bleeding, severe abdominal pain, se-
control group, as marked in red (see Table 2), where awareness vere blurring of vision, or convulsions as danger signs during preg-
about ANC and danger signs of pregnancy was reduced. nancy significantly (P < .001) increased by 18.30%, 23.2%, 20.0%,
Awareness about ANC during pregnancy significantly (P < .001) and 4.90%, respectively. Similarly, mothers in the intervention
improved in the intervention group. Participants acknowledging the group exhibited a higher level of awareness regarding danger signs
role of ANC in enhancing health, minimizing risks, and as a source during labor. Danger signs such as “failure to progress” and
of necessary tetanus toxoid (TT) injections and iron supplements in- “placenta does not come out within 30 minutes after the baby is
creased by 24%, 12.60%, and 61.20%, respectively. The number of delivered” were identified by 48.2% and 21.10% more mothers in
participants who responded incorrectly in the baseline survey also the intervention group.
decreased by 74.2%. Contrastingly, awareness about ANC was
noted to decrease in the control group, as shown in Table 2. Aware-
ness about TT injections and consumption of iron tablets were also
DISCUSSION
significantly (P < .001) improved among the intervention group by As maternal healthcare shifts to home and community-based set-
55% and 58%, respectively. Awareness about hygiene (the “five tings, consumer health technology applications hold promise for
cleans”) significantly (P < .001) increased by 57.1%, and incorrect augmenting patients’ awareness and, in turn, their ability to provide
knowledge about the same was significantly (P < .001) decreased by self-care. This study demonstrates how tribal communities—who
62.40% in the intervention group. Mothers in the intervention typically have no to minimal familiarity with mobile devices—Table 2. Comparing maternal health awareness in intervention and control groups
Site Baseline End-line Change from Pearson Chi-square Comparing the Hypotheses
baseline percent change (C) between the con-
trol and intervention group
A B C
(%) (%) (%) v2 P value
Hypothesis1 (H1): mHealth can improve pregnant mother’s awareness about the need to visit doctors/ANC during pregnancy.
Do you know why you need to visit Doctor/ANC during pregnancy?
Helps to identify (severe) problems and provide solutions Control 21.0 9.30 11.70 Accepts H1
Intervention 9.10 33.10 24.00 125.21Table 2. continued
2472
Site Baseline End-line Change from Pearson Chi-square Comparing the Hypotheses
baseline percent change (C) between the con-
trol and intervention group
A B C
(%) (%) (%) v2 P value
The placenta does not come out within 30 minutes after the baby is delivered Control 2.5 10.8 8.3
Intervention 1.2 23.3 22.1 34.71Journal of the American Medical Informatics Association, 2021, Vol. 28, No. 11 2473
learned information about maternal health and hygiene when deliv- may be a precursor to improved health outcomes and would be a
ered through an mHealth application in a user-centered manner (us- promising and essential area of future research. Third, ASHA work-
ing the local language and audiovisual communication). This study ers were responsible for carrying the mobile device with them during
also indicates how the mHealth application significantly enhanced each intervention. Pregnant mothers, being passive users, only used
the education and maternal health knowledge of pregnant women the mobile application in the presence of ASHAs. Further research is
when added to the typical standard of care in rural and tribal com- needed to capture the direct impact of mHealth on maternal health
munities. awareness in tribal communities when actively used by mothers
Our findings showed a significant improvement in the mHealth without receiving assistance from trained personnel such as ASHAs.
intervention group’s awareness of critical knowledge during the This research would be dependent on reaching the point where there
pregnancy, including the importance of doctor visits, TT injections, are sufficient smartphone owners in the tribal communities. Last,
iron tablets, danger signs, and hygiene (the five cleans). The findings the study only focused on 2 villages, though the sample size was suf-
exhibit the potential of mHealth as an educational and awareness ficient. Although more than half of the sample were illiterate, future
tool that provides structured information about maternal health for studies can focus only on the impact of mHealth use on illiterate
Downloaded from https://academic.oup.com/jamia/article/28/11/2467/6359598 by guest on 28 October 2021
pregnant mothers in rural and tribal communities. This study reiter- populations.
ates that health-related education holds value for patients in remote
regions to support self-management.22
Our study highlights the relevance of health literacy to mHealth. CONCLUSION
Proponents of digital health may acknowledge the dependence of
The results indicate that the mHealth intervention can improve ma-
mHealth on overall literacy and how low literacy deters the effec-
ternal health awareness and knowledge of tribal and rural communi-
tiveness of mHealth interventions in indigenous communities.32
ties despite low educational status when used as an education tool
However, our findings show that, if used correctly, mHealth inter-
by community workers. mHealth holds continued promise for ma-
ventions can be an effective audiovisual tool to educate people who
ternal health, but implementers and policy makers should addition-
have low literacy. The extent to which a user comprehends any in-
ally address health system and sociocultural factors that play a
formation delivered to them by an mHealth application determines
significant role in the uptake of recommended maternal health prac-
the effectiveness of the technology.33 Despite most participants hav-
tices, especially in rural communities of developing or underdevel-
ing no or minimal literacy, the mHealth intervention MFM effec-
oped countries.
tively improved maternal health awareness of pregnant mothers as
they easily adopted short and easy-to-read health information.
Availability of mHealth content in local tribal languages also con-
FUNDING
tributed to successful mHealth adoption. These findings were in line
with other studies,34–36 which incorporated local language into their The study was funded by Simavi, the Netherlands, under Grant Number
3312005 and Deutsche Welthungerhilfe under Grant Number WHHInd/1287
software.
(to the author, MMC). The content is solely the responsibility of the authors.
In support of existing literature,37,38 our study demonstrates that
mHealth applications have tremendous potential for supplementing
traditional channels of maternal health communication (campaigns,
AUTHOR CONTRIBUTIONS
posters, public announcements) as an evolving communication me-
dium for fostering maternal health awareness. According to the MMC conceived and designed the study, participated in data collection, and
Cognitive Theory of Multimedia Learning, people learn more effec- approved the final version for submission. AC and OA participated in the lit-
erature review, graphical illustration, data analysis, wrote the manuscript,
tively from words and images than words alone.39 This theory can
and approved the final version for submission.
partially explain why tribal communities learned new information
through mHealth significantly more than traditional health interven-
tion. The use of both auditory and visual channels in mHealth
SUPPLEMENTARY MATERIAL
(Dual-Coding Theory) potentially helped pregnant mothers learn
new knowledge. However, these assumptions require further explo- Supplementary material is available at Journal of the American Medical Infor-
ration and confirmation. matics Association online.
Finally, this study also exhibits the potential of mHealth to mini-
mize anchoring biases of indigenous communities40 where their
healthcare practices and beliefs are primarily determined by their DATA AVAILABILITY STATEMENT
faith in traditional knowledge, such as natural medicine, psychoso- The anonymized data underlying this article will be shared on reasonable re-
matic treatments, and religious rituals.40 Despite having a strong be- quest to MMC.
lief in the “traditional health care system,” tribal communities in the
intervention group (using mHealth tool) were noted to embrace the
scientific or modern maternal healthcare practices in addition to CONFLICT OF INTEREST STATEMENT
their traditional beliefs. None declared.
Some limitations of our study need to be acknowledged. First,
being a quasi-experiment where neither women nor ASHAs were
randomized, the findings might have been influenced by confound- REFERENCES
ing factors, such as differences between the villages or the ASHA 1. Mpembeni RNM, Kakoko DCV, Aasen HS, et al. Realizing wome ns right
staff. Second, this study did not measure any health outcomes of the to maternal health: a study of awareness of rights and utilization of mater-
pregnant mothers, but only change in health knowledge. Although nal health services among reproductive age women in two rural districts in
not demonstrated in the current study, improved health knowledge Tanzania. PLoS One 2019; 14 (5): e0216027.2474 Journal of the American Medical Informatics Association, 2021, Vol. 28, No. 11
2. WHO. The global strategy for women’s, children’s and adolescents’ health, 22. Rowland SP, Fitzgerald JE, Holme T, et al. What is the clinical value of
2016–2030. Secondary The global strategy for women’s, children’s and ado- mHealth for patients? NPJ Digit Med 2020; 3 (1): 4.
lescents’ health, 2016–2030. 2021. https://www.who.int/life-course/part- 23. Ngabo F, Nguimfack J, Nwaigwe F, et al. Designing and implementing an
ners/global-strategy/global-strategy-2016-2030/en/. Accessed June 2021. innovative SMS-based alert system (RAPIDSMS-MCH) to monitor preg-
3. Jaysawal N. Rural health system in India: a review. Int J Res Health 2015; nancy and reduce maternal and child deaths in Rwanda. Pan Afr Med J
3 (1): 29–37. Online First. 2012; 13:31.
4. Kumar MM, Pathak VK, Ruikar M. Tribal population in India: a public health 24. Mbuagbaw L, Thabane L, Ongolo-Zogo P, et al. The Cameroon mobile
challenge and road to future. J Family Med Prim Care 2020; 9 (2): 508–12. phone SMS (CAMPS) trial: a randomized trial of text messaging versus
5. Kearns A, Hurst T, Caglia J, et al. Focused antenatal care in Tanzania. usual care for adherence to antiretroviral therapy. PLoS One 2012; 7 (12):
Secondary Focused antenatal care in Tanzania 2014. https://cdn2.sph.har- e46909.
vard.edu/wp-content/uploads/sites/32/2014/09/HSPH-Tanzania5.pdf. 25. Jones CO, Wasunna B, Sudoi R, et al. “Even if you know everything you
Accessed June 2021. can forget”: health worker perceptions of mobile phone text-messaging to
6. Anya SE, Hydara A, Jaiteh LE. Antenatal care in the Gambia: missed op- improve malaria case-management in Kenya. PLoS One 2012; 7 (6):
portunity for information, education and communication. BMC Preg- e38636.
nancy Childbirth 2008; 8: 9. 26. L’Engle KL, Vahdat HL, Ndakidemi E, et al. Evaluating feasibility, reach
Downloaded from https://academic.oup.com/jamia/article/28/11/2467/6359598 by guest on 28 October 2021
7. Ghosh-Jerath S, Devasenapathy N, Singh A, et al. Ante natal care (ANC) and potential impact of a text message family planning information ser-
utilization, dietary practices and nutritional outcomes in pregnant and re- vice in Tanzania. Contraception 2013; 87 (2): 251–6.
cently delivered women in urban slums of Delhi, India: an exploratory 27. Yin Z, Lesser J, Paiva KA, et al. Using mobile health tools to engage rural
cross-sectional study. Reprod Health 2015; 12 (1): 20. underserved individuals in a diabetes education program in south Texas:
8. Arsenault C, Jordan K, Lee D, et al. Equity in antenatal care quality: an feasibility study. JMIR Mhealth Uhealth 2020; 8 (3): e16683.
analysis of 91 national household surveys. Lancet Glob Health 2018; 6 28. Donovan J, Bersin A, Donovan C. The effectiveness of mobile health
(11): e1186–e95. (mHealth) technologies to train healthcare professionals in developing
9. Yaya S, Uthman OA, Amouzou A, et al. Inequalities in maternal health countries: a review of the literature. BMJ Innov 2015; 1 (1): 33.
care utilization in Benin: a population based cross-sectional study. BMC 29. Minniti CP, Kato GJ. How we treat sickle cell patients with leg ulcers. Am
Pregnancy Childbirth 2018; 18 (1): 194. J Hematol 2016; 91 (1): 22–30.
10. Kumar G, Choudhary TS, Srivastava A, et al. Utilisation, equity and deter- 30. Article 366 (25): The scheduled castes and the scheduled tribes (preven-
minants of full antenatal care in India: analysis from the national family tion of atrocities) 1989 . https://legislative.gov.in/sites/default/files/A1989-
health survey 4. BMC Pregnancy Childbirth 2019; 19 (1): 327. 33_2.pdf. Accessed June 2021.
11. Chauhan P, Chauhan VK, Shrivastava P. Maternal mortality among tribal 31. Galanter M. Who are the other backward classes? An introduction to a
women at a tertiary level of care in Bastar, Chhattisgarh. Glob J Health constitutional puzzle. Econ Polit Wkly 1978; 13: 1812–28.
Sci 2012; 4 (2): 132–41. 32. Kreps GL. The relevance of health literacy to mhealth. Stud Health Tech-
12. Narayan L. Addressing language barriers to healthcare in India. Natl Med nol Inform 2017; 240: 347–55.
J India 2013; 26 (4): 236–8. Online First: 2014/04/25]. 33. Abejirinde I-OO, Ilozumba O, Marchal B, et al. Mobile health and the
13. Mahapatro M, Kalla A. Health seeking behaviour in a tribal setting. performance of maternal health care workers in low- and middle-income
Health Popul Persp Issues 2000; 23: 160–9. countries: a realist review. Int J Care Coord 2018; 21 (3): 73–86.
14. Some DT, Sombie I, Meda N. How decision for seeking maternal care is 34. Duysburgh E, Temmerman M, Ye M, et al. Quality of antenatal and child-
made: a qualitative study in two rural medical districts of Burkina Faso. birth care in rural health facilities in Burkina Faso, Ghana and Tanzania:
Reprod Health 2013; 10 (1): 8. an intervention study. Trop Med Int Health 2016; 21 (1): 70–83.
15. Echoka E, Makokha A, Dubourg D, et al. Barriers to emergency obstetric 35. Balakrishnan R, Gopichandran V, Chaturvedi S, et al. Continuum of care
care services: accounts of survivors of life threatening obstetric complications services for maternal and child health using mobile technology: a health
in Malindi district, Kenya. Pan Afr Med J 2014; 17 Suppl 1 (Suppl 1): 4. system strengthening strategy in low and middle income countries. BMC
16. Black RE, Victora CG, Walker SP, et al.; Maternal and Child Nutrition Med Inform Decis Mak 2016; 16: 84.
Study Group. Maternal and child undernutrition and overweight in low- 36. Medhanyie AA, Little A, Yebyo H, et al. Health workers’ experiences,
income and middle-income countries. Lancet 2013; 382 (9890): 427–51. barriers, preferences and motivating factors in using mHealth forms in
2013/06/12]. Ethiopia. Hum Resour Health 2015; 13 (1): 2.
17. Verma R, Khanna P, Dhankar M. Vaccination during pregnancy: today’s 37. Fiordelli M, Diviani N, Schulz PJ. Mapping mHealth research: a decade of
need in India. Hum Vaccin Immunother 2016; 12 (3): 668–70. evolution. J Med Internet Res 2013; 15 (5): e95.
18. Yaya S, Kota K, Buh A, et al. Prevalence and predictors of taking tetanus 38. Stoyanov SR, Hides L, Kavanagh DJ, et al. Mobile app rating scale: a new
toxoid vaccine in pregnancy: a cross-sectional study of 8,722 women in Si- tool for assessing the quality of health mobile apps. JMIR Mhealth
erra Leone. BMC Public Health 2020; 20 (1): 855. Uhealth 2015; 3 (1): e27.
19. Clark J. The global push for institutional childbirths—in unhygienic facili- 39. Mayer RE, ed. Cognitive theory of multimedia learning. In: The Cam-
ties. BMJ 2016; 352: i1473. bridge Handbook of Multimedia Learning (Cambridge Handbooks in
20. Bashi N, Fatehi F, Fallah M, et al. Self-management education through Psychology). Cambridge, UK: Cambridge University Press; 2014: 43–71.
mHealth: review of strategies and structures. JMIR Mhealth Uhealth 40. Tribal health problems, disease burden and ameliorative challenges in
2018; 6 (10): e10771. tribal communities with special emphasis on tribes of Orissa. In Proceed-
21. Kay M, Santos J, Mhealth TM. New horizons for health through mobile ings of National Symposium on “Tribal Health”; 19th–20th October;
technologies. World Health Organization 2011; 64 (7): 66–71. 2006; Citeseer.You can also read