Mercy Medical Center Reverence Integrity Compassion Excellence
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Mercy Medical Center
Reverence
Integrity
Compassion
Excellence
Fiscal Year 2013
Community Benefit Report
Mercy Medical Center • Fiscal Year 2013 • Community Benefit Report

Executive Summary
This Community Benefit Report and Health Improvement Plan is a strong example of
Mercy Medical Center’s ongoing commitment to promote and support the health and
wellbeing of our Community members.
Our tradition of providing charitable aid to the poor and medically underserved is part of
our legacy. Despite declining revenue, Mercy provided more than $29 million in uncom-
pensated medical care to vulnerable, uninsured and underinsured members in our com-
munity in 2012.
The Community Benefit Report and Health Improvement Plan outline’s our dedication to
- and strategy for - optimizing the health of all of our County residents. Our commitment
remains to work collaboratively with local community partners to strengthen existing
public health programs and advance evidence- based wellness initiatives. Additionally,
Mercy will work to reinforce and expand health improvement and disease prevention
services currently offered by the hospital. Our long-term goal is to promote greater levels
of health, health awareness and wellness for everyone in our community.
At Mercy, we are committed to managing our resources and advancing our healing min-
istry in a manner that benefits the common good now and long into the future. Despite
today’s challenges, we see this as time of great hope and opportunity for the future of
health care.
We want to use this venue to also extend a special note of appreciation to the women
and men who, with a spirit of collaboration, work alongside us to help address the health
priorities of our community by offering an array of health and wellness programs and
services.
In accordance with policy, the Mercy Medical Center Board Members have reviewed and
approved the annual Community Benefit Report and Health Improvement Plan as of
June 21, 2013.
1 Mercy Medical Center 2010 Annual Report
Caring for our community 2
Mercy Medical Center
Community Health
Needs Assessment
Mercy Medical Center (Mercy) is a private, not-for-profit healthcare
174-bed medical center located on a 90-acre campus on the north side of
Roseburg, Oregon. Mercy is affiliated with Catholic Health Initiatives, the
second largest Catholic health network in the country. Founded in 1909
by the Sisters of Mercy, Mercy Medical Center’s core values are reverence,
compassion, integrity and excellence. Our mission is to nurture a healing
ministry by bringing it new life, energy, and viability. We emphasize
human dignity and social justice as we move towards the creation of
Healthier Communities.
Mercy’s specialized and comprehensive inpatient and outpatient care
includes: A 24-hour emergency center; acute medical and surgical
services; critical care (ICU and PCU); diabetes education; diagnostic
imaging; Shaw Heart and Vascular Center, including catheterization labs
and interventional cardiology and peripheral; Outpatient Imaging Center;
Family BirthPlace, laboratory services, spiritual care, rehabilitation
services, including physical, occupational and speech therapies; day
surgery, hospice, home health, and Parkway Mobility and Medical
Supply. Gifts and grants to Mercy are received and administered by the
Mercy Foundation, a 501(c)3, tax-exempt, non-private, charitable
foundation. Mercy’s inpatient market share is 67.1%
Community Description
Douglas County, Oregon extends west to east from sea level at the Pacific
Ocean to the 9,182 foot Mt. Thielsen in the Cascade Range. Douglas
County covers an expansive 5,071 square miles and is comprised of 12
incorporated cities Roseburg ñ the county seat, Canyonville, Drain,
Elkton, Glendale, Myrtle Creek, Oakland, Reedsport, Riddle, Sutherlin,
Winston, and Yoncalla. Douglas County, as with many rural jurisdictions,
faces the challenges of a migration of seniors as well as a baby boomer
aging population, high rates of unemployment and poverty, few educa-
tional opportunities, high rates of tobacco and other drug use, and fewer
local resources dedicated to addressing these and other known health risk
factors. Nearly 70% of residents live outside the county seat of Roseburg,
where most health services are provided. Douglas County is a federally
designated medically underserved area, as well as a primary care shortage
area.
3 Mercy Medical Center 2013 Annual Report
Population which is the largest employer in Roseburg proper; Cow
Creek Indian Tribe, city and county and federal govern-
According to the 2011 US Census Bureau’s American ment including the VA healthcare system, agriculture,
Community Survey, the demographics of Douglas the warehouse industry, building trades and education.
County’s 107,490 residents are as followed: 0-17
(20.1%), 18-64 (58.6%), and 65 and over (21.3%). Income Level
About 89% of the county’s population is white non-
Hispanic, as compared to 84% statewide, and approxi- Stagnant economic recovery continues to greatly im-
mately 5% of the population is Hispanic/Latino, pact the lives of all Douglas County residents, as it has
followed by 3% American Indian, 1% Asian/Pacific Is- one of the highest poverty and unemployment rates in
lander, and 0.3% African American. Over the last few Oregon— 11.1% (March 2013). Family-wage jobs
years, we have experienced an approximately 25% have diminished with the dwindling timber industry
outmigration rate of 20-45 year olds, with more seniors over the last two decades. As a large county with
moving to our county because of the seasonal weather many rural communities, our socio-economic profile is
conditions. like that of Appalachian America. According to the
2011 American Community Survey, 16.1% of Douglas
Economy County residents have a bachelor’s degree or higher
compared to the Oregon State average of 28.8%. The
Traditionally, the timber and wood product industries median household income is $38,502, compared with
have been the major employers in Douglas County. the Oregon State average of $46,876. 17.0% of all
Even with the downturn, it still remains one of the residents and 25.3% of children under 18 live in
biggest sources of employment in Douglas County; poverty, and 17.9% of all residents do not have health
with approximately 25% of Douglas County’s labor insurance. 68% of children in schools located outside
force employed in the forest products industry. The of Roseburg are on the free-and-reduced lunch pro-
largest timber supplier is Roseburg Forest Products. gram, a widely held poverty indicator.
Other large employers include Mercy Medical Center,
Caring for our community 4
Who was Involved
in the Assessment
The assessment process has taken place over the last two years, and was led by Mercy Medical Center staff in
partnership with community stakeholders. To ensure broad input from community residents and partners, out-
reach was conducted via a Community Perception phone survey, a Community Engagement Forum; one-on-one
interviews with key community leaders and residents; and a survey monkey was provided electronically to ap-
proximately 200 not-for-profit and human services organizations. In addition, results from Mercy’s 2012 Patient
Survey regarding access to and usage of healthcare services were used in determine the priority topics.
Initial stakeholders participating in one-on-one
interviews include:
Adapt Substance Abuse Treatment Program (ADAPT) - Jerry O’Sullivan, Pauline Martel
Douglas County Health and Human Service Department - Marylin Carter
Oregon Health Sciences University, Office of Rural Health - Troy Sonen
How the Assessment
was Conducted
The assessment was conducted over multiple phases. First was a review of state, county, city, and national statisti-
cal information:
Health Factors
The Robert Wood Johnson Foundation’s 2013 County Health Rankings rank Douglas County 30th out of 33 Ore-
gon Counties for Health Outcomes — which represent how healthy a county is, and 28th out of 33 counties for
Health Factors — which are what influences the health of the county. Douglas County rankings are significantly
worse than the state’s most metropolitan county that includes the City of Portland:
5 Mercy Medical Center 2013 Annual Report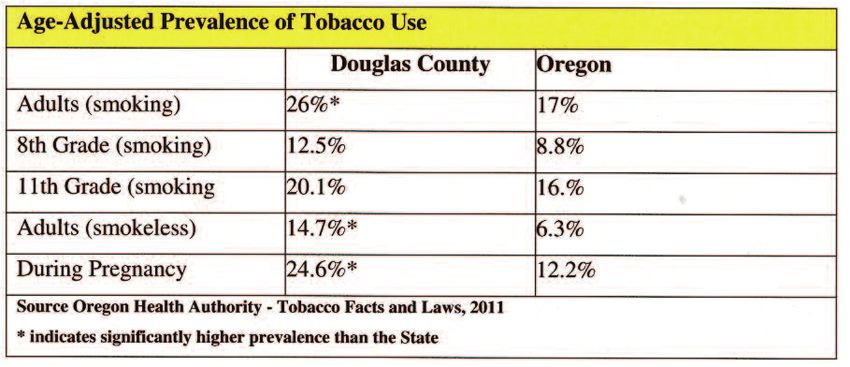
Chronic Disease
Douglas County has higher instances of major chronic diseases as compared to the state averages and poor health
behaviors, as shown by the table below.1
Caring for our community 6
Incidences of Violence
• Violence Prevention.
The impact of domestic violence in Douglas County:2
• Accident Mortality
• In 2009, there were over 8,309 allegations of abuse • Obesity
or neglect towards seniors and people with • Tobacco Usage
disabilities. 45% of these allegations indicated that • Motor Vehicle Crash Mortality
the perpetrator was an adult child, family member, • Access to Primary Care
spouse or intimate partner. • Dental Care
• Suicide Prevention
• Of the 35 impact of domestic violence deaths in • Asthma
2010, 48% had some known connection to • Lung Disease
Department of Human Services. They currently or
have in the past received Supplemental Nutritional Initial Goal Setting Process
Assistance Program (SNAP) benefits, medical
In order to determine the top three community needs
assistance, cash relief or utilized some other special
for Mercy to focus on, four factors were used:
assistance service.
1) The size of the problem (number of people affected)
• Over 4,000 shelter nights at Battered Persons
2) The seriousness of the problem
Advocacy (BPA) are reported for families fleeing
3) Community support (evidence that the issue is
domestic violence annually.
important to diverse community stakeholders)
4) Economic feasibility
• Over 700 restraining orders are filed each year in
Douglas County.
Through this process three priority Community Health
Improvement Needs were identified:
• Over 6,000 Crisis call occurrences are documented
annually.
• Reducing Incidence of Domestic Violence
• Reducing Obesity Rates
Community Benefit • Reducing Tobacco Usage
Perception Survey
A 13 question phone survey was conducted to assess
residents’ views on current health needs. Mercy
reached out to 4,955 residents and received responses
from 400 residents for a average response rate of 8.1%.
From this survey a list of 10 community health needs
were identified:
7 Mercy Medical Center 2013 Annual Report
Community Benefit Needs Government
Douglas County Health and Social Services
Assessment Partner Forum Department - Dawnelle Marshall
With the results of the Community Perception Survey Department of Human Services - Lisa Lewis
analyzed, and the priorities needs narrowed to three, a Douglas County Senior Resource Coalition -
partner forum was held with representatives from over Shawn Ramsey-Watson
16 community organizations. This meeting enabled
partners to come together to first brainstorm on identi- Description of What the Hospital Will do to Address
fying existing community resources that we could the Community Needs
collaborate with and second identify gaps in services Even with great challenges, Douglas County residents
associated with domestic violence, obesity, and have a strong history of collaboration on initiatives to
tobacco usage. improve the health of our community members.
Health and Human Services Organizations Stakeholders know that a healthier Douglas County is
not the responsibility of a single entity, nor a single
Mercy Medical Center-Kelly Morgan, President & CEO, sector of the community; rather, achieving measure-
Wally Gwaltney, CHI Corporate Responsibility Officer, able health improvements requires broad community
and Jean Larson, Controller involvement and collective action across all sectors of
Umpqua Training & Employment - Susan Buell our community3. Partnerships and collaborations are
Greater Douglas United Way - Bryan Trenkle, key to the success of any initiative undertaken by
Annette Rummell Mercy. Opportunities must be taken advantage of to
Cow Creek Health & Wellness - Sharon Stanphill, PhD support existing programs, and leverage community
Umpqua Health Alliance - Patti LaFrienere resources and expertise to build a more accessible and
Mark Herscher, DO - Family Practice Practitioner and sustainable network of programs and services for the
Mercy Medical Center Board Member prevention, early detection and management of
Battered Person’s Advocacy - Sami Gloria chronic disease.
Umpqua Community Health Ctr. - Christi Parazoo,
Brenda Lewis Efforts to improve the health of the community will
United Community Action Network (UCAN) Senior model The Spectrum of Prevention, “a fundamental
Services - Judy Applegarth, Carolyn Parks model in public health, acknowledges that a broad
range of factors play a role in health.”
School Districts
North Douglas School District - John Lahley
Oakland School District - Nanette Hagen
Roseburg School District - Larry Parsons, PhD
Sutherlin School District - Steve Perkins
Douglas County Educational Services District
Andy Boee
www.co.douglas.or.us/health/PH/livewell.asp
Caring for our community 8
Action Plans (SNAP, on-site wellness nurses, health resource refer-
rals and direct medical care to children through our
(see Attachment A) area schools.
Violence Prevention - Goal to Reduce Incidences of Adult
Domestic Violence
• Mercy’s dietary staff will work with hospital cafeteria
As domestic violence is the leading indicator of child staff to expand healthy food choices for employees
abuse, Mercy will continue the ongoing work of the and staff.
UP2US Now Violence Child Abuse Prevention Initia-
tive, and partner with stakeholders to develop • Mercy will work with Cow Creek Indian Tribe
programs to reduce incidences of domestic violence. and other local employers, to pilot and implement
Wellness Programs on their campus.
Work of the Collation includes:
Tobacco Usage - Goal to Reduce Proportion of
• Enhancement of Existing Home-Visit Prevention Residents Using Tobacco
Education Programs.
• Mercy will continue asking about tobacco use
• Conducting child abuse and domestic violence during and intake history and will provide materials
screening trainings to identified local medical and and resources to patients as requested.
social service providers of high-risk families.
• Mercy will work with our Education and Support
* Development of Interagency Referral System to Groups to expand smoking cession support group
identify high-risk families and provide intervention opportunities.
services.
• Mercy will utilize existing Mercy Community
• Implement Community Awareness campaigns. Programs to provided additional educational
opportunities on tobacco usage.
• Developing Legislation proposals regarding Oregon
State Domestic Violence laws. • Mercy will work with Douglas County Independent
Physician Association to promote ongoing staff
Obesity — Goal to Reduce Proportion of Child and education on clinical best practices for tobacco use
Adult Obesity screenings, referral and treatment options.
Mercy currently has successfully partnership with local
Douglas County Schools to deliver the Healthy Kids • Mercy will partner with the Douglas Health and
Outreach Project. The Healthy Kids Outreach Program Social Services Department to promote the Oregon
is the only program providing school based basic Tobacco Quit Line.
health education and healthcare to underserved, rural
school age children in Douglas County. Our program • Mercy will work with community partners to
provides health education, nutrition education with develop a social media campaign around tobacco
the Supplemental Nutritional Assistance Program usage.
9 Mercy Medical Center 2013 Annual ReportPriority Community Health Needs Not Being Mercy Medical Center
Board of Directors
Addressed by the Hospital and Reasons Why Joyce Akse
Neal Brown
Marty Daley
From the survey process the largest community need not being addressed
Tom Davidson
by Mercy is motor vehicle safety, including speeding, DUI occurrences, Bret Hansen, MD
motor vehicle crash mortality. While Mercy recognizes the seriousness of Mark Herscher, DO
this issue, we believe that our resources can be more effectively used to Gabrielle Jones, RSM
impact health needs currently in place. We are committed to supporting Dave Leonard
Gary McCormack
local government efforts to improve motor vehicle safety, and will partner
Kelly Morgan
in initiatives when possible, Mercy is not in a position to lead this effort at Amy Palm
this time. John Powell, MD
Joe Wilczek
Mercy Foundation
Approval Board of Directors
Mercy Medical Center is governed by at 13 member Board of Directors. Syndi Beavers
John Blodgett
The Board has designated the Mission Services to develop implementa-
Beverly Brandt
tion plan objectives. The Board and Senior Management staff of Mercy Peter Carhart
Medical Center will direct, monitor strategies and will review progress on Jerry Duncan
an annual basis. Linda Folk
Jacquelyn Groshong, MD
Tony Haber
Paul Kremser, MD
Dave Leonard
Jerry Moneke
Patrick Moore
Kelly Morgan
Kathleen Nickel
Lisa Platt
Tammy Rondeau
Julie Ryan
Christine Seals, MD
David Sutton, DDS
Gary Wayman
Mercy Medical Center
Executive Committee
Sarah Agsten, DO
Faye Ameredes, DO
Kurt Brickner, DO
Howard Feldman, MD
Deidre McCann, MD
Marc Smith, MD
Community Benefit Team
David Price
Lisa Platt
Kathleen Nickel
Nancy Lehrbach
Joan Sonnenburg
Katy Rowlands
Caring for our community 1011 Mercy Medical Center 2013 Annual Report
Caring for our community 12
13 Mercy Medical Center 2013 Annual Report
Caring for our community 14
Caring for our Community
Since 1909.
Mercy Medical Center
2700 Stewart Parkway
Roseburg, OR 97471You can also read