Meeting Targets and Maintaining Epidemic Control (EpiC) Project - Cooperative Agreement No. 7200AA19CA00002
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Meeting Targets and Maintaining Epidemic Control (EpiC) Project Cooperative Agreement No. 7200AA19CA00002 ESWATINI SEMI-ANNUAL PROGRESS REPORT OCTOBER 1, 2020 TO MARCH 31, 2021 SUBMITTED BY FHI 360: MAY 20, 2021

EpiC Eswatini Semi-Annual Progress Report
October 1, 2020 to March 31, 2021
A. Executive Summary
Key Population (KP) programming transitioned from LINKAGES to EpiC at the start of FY21. Programming
continued to be dynamic adjusting to the COVID-19 status in country, which included a second wave from
mid-December 2020 through the end of February 2021. EpiC Eswatini formally began programming with
two new key populations (KPs): transgender persons (TG) and people who inject drugs (PWID). Focus for
both includes access to basic clinical services, as well as advocacy to expand the current enabling
environment to allow for more specialized services and development of targeted programs. EpiC
conducted a high-level TG Stakeholder meeting, including the TG community, Ministry of Health (MOH),
Deputy Prime Minister’s Office, Royal Eswatini Police Services, USAID/Eswatini and USAID/Southern
Africa, a health care worker who supports gender affirming care (informally) and UNAIDS. This meeting
provided approval to develop a TG strategic plan with the Ministry of Health. The program continued to
expand services to the KPIF implementing partners1 including transitioning of all psycho-social services
(PSS), TG demand creation, as well as worked to transition all Female Sex Worker (FSW) outreach workers,
which will be finalized in April 2021. On the service provision side, the program focused on the
introduction of decentralized drug distribution (DDD) for both ART and PrEP through home-based
appointments, as well as expanded services to include viral load testing, starting in January 2021. Detailed
achievements for this program are presented in Section I of this report.
The National Emergency Response Council on HIV and AIDS (NERCHA)2 program transitioned to EpiC from
the prior USAID project HC4 and received equipment and vehicles in November 2020. Eight staff were
hired and trained on data management using Community Data Action Platform (CDAP) in November 2021,
with the Strategic Information Advisor starting in December 2021. As programming was ramping up,
Eswatini began experiencing the start of the second wave mid-December, which was impacted by the
identification of the South African variant B.1.351. Routine programming was only able to return on
second week of March 2021 when the government relaxed its restrictions on movement and meetings at
the community level. COVID-19 impacted and delayed program implementation as most activities require
face to face meetings and trainings to capacitate community leadership on the program. Detailed
achievements for this program are presented in Section II of this report.
Under the EpiC consortium partner PSI, 4,506,000 male condoms were distributed, of which 56 percent
went to retail outlets and 44 percent to partners. PSI continued to promote condom access and use on
social media and radio. Condom sales continued through the self-sustainable model developed with
PSI/South Africa (SA). An increase of 33 percent in condom sales was seen during the shift from the
integrated retail distribution model to the full commercial self-sustainable model. Commercial lubricants
were introduced to the product portfolio, further providing choice and convenience to consumers.
Detailed achievements for this program are presented in Section III of this report.
The report is organized as follows:
• Section I: Key Populations Program – page 2
• Section II: EpiC Eswatini/NERCHA: Community Strengthening Program – page 38
• Section III: EpiC Eswatini Condom Program – page 52
1
HealthPlus 4 Men, House of Our Pride, Rock of Hope and Voice of our Voices
2National Emergency Response Council on HIV and AIDS (NERCHA) was created to coordinate and facilitate the National Multisectoral HIV/AIDS
response and oversee the implementation of the national strategic plans and frameworks in the Government of the Kingdom of Eswatini.
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 1
Section I: Key Populations Program
B. Key Results by Objective
1. Attain and maintain HIV epidemic control among at-risk adult men, women and priority
populations (PP)
Men who purchase sex (MWPS)3 is a target group under the EpiC Key Population Investment Fund
(KPIF), which is implemented through the EpiC Eswatini project. KPIF focuses on demand creation for
identified populations that are at risk in Eswatini, and the EpiC Eswatini project provides clinical services
thus the reporting below only captures those reached with clinical services.
Under the KPIF program, through Voice of our Voices our FSW-led partner, FSW peers mobilized their
clients to access services as follows:
▪ 70 MWPS, of which 50 are transport operators (TOPS), were provided with clinical services and
66 MWPS that were eligible received HIV testing and results, two tested positive and was
initiated on treatment, for a three percent case finding rate.
▪ Reaching MWPS has been a challenge during COVID-19 as hotspots were closed, which was the
primary way to access and to refer them to services.
▪ Most MWPS have been reluctant to access services at the community center hence marketing
the space will be done to improve access, especially for TOPs, who are reached primarily as
MWPS.
EpiC consortium partner PSI leads on national level condom programming technical assistance. Activities
and accomplishments under the condom programming are reported in Section II.
3
Previously referred to as Clients of Sex Workers (CSW)
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 2
2. Attain and maintain HIV epidemic control among key populations (KP) Female Sex Workers (FSWs) Reach (KP_PREV)4 A total of 5,711 FSWs have been reached with prevention package of services. This accounts for 56 percent (5,711/10,284) of the annual target. A total of 52 percent (2,963/5,711) were known positive of which 1,418 accessed community level services such as as-one-on one discussion or were given condoms and lubricants but did not access clinical services. 4,293 FSWs, or 75 percent of all FSWs reached, accessed our clinical services. Of those that accessed our clinical services 1,898 accessed testing services, 1,545 were known positive (included in the 52 percent noted above), 6 declined and 844, or 15 percent (844/5,711) were not due for testing but accessed non-testing services. The program implemented an EPOA in the first quarter of the year, identifying 15 female sex worker seeds, ten were through EpiC with five additional seeds identified through the Key Population Investment Fund (KPIF), to facilitate mobilization and inject new networks to the outreach workers. Impacts relating to COVID-19 are captured under the enhanced development of sustainable prevention programs section that focused on the peer outreach and demand creation aspect of the program. FSW accessing testing services and case finding: Of the 1,904 FSWs that were eligible5 for testing, 99 percent or 1,898 tested 6 , and six declined testing services. This has accounted for 113 percent (1,898/1,684) against the annual testing target. Of those that tested, six percent (120/1,898) were for PrEP refills. The restarting of community testing from Q4 FY20 along with the fact that the program integrates other clinical services within the other community based HTS resulted in a high testing volume in Q1 FY21. The high testing volume is also a result of the FSW focused organization, VOOV, who had just introduced their Outreach Workers (ORWs) under the KPIF in March 2020 (FY20), right at the start of COVID-19. The ORWs were in the middle of training when it was cancelled due to safety around COVID-19 and the remaining training modules were provided virtually. When community testing was “un-paused” on August 4th it included mobilization by these additional eight ORWs from VOOV. As new ORWs start, we see a general low case finding as they are learning programming and understanding how to work and identify hotspots. With COVID-19 dynamics and virtual mentoring we have seen that VOOV has still not found their footing in terms of performance. This is important to note as they provide demand creation support for the clinical services for FSWs and MWPS. During the reporting period VOOV demand creation accounted for 26 percent (505/1,898) of those that accessed testing services. Anecdotally we believe there has been a rapid increase in testing linked to COVID-19 as a shift in preference to access health services, not just access to testing, through our comprehensive clinical services. 4 Number of key populations reached with individual and/or small group-level HIV prevention interventions designed for the target population: risk assessment, HIV education, condom and lubricants promotion and provision (CLPP), direct provision/navigation to HIV Testing Service (HTS) 5 Eligible clients: This refers to clients that have not tested for HIV in the last two months and those that have never tested for HIV. Eligible clients are identified by service providers in the clinical service points as we don’t include self-reported data at the community level through the ORWs due to disclosure issues and safety of data at the community level. 6 HIV testing services (HTS) noted in the report under HTS_TST (and HTS_POS as applicable) include HIV rapid test under voluntary counselling and testing (VCT), index testing of contacts identified as well as confirmations for HIV Self testing for those that have screened positive, and for those that have screened negative but want to start PrEP EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 3

It is important to note that such volume was not maintained in Q2 FY21. Due to the COVID-19 second
wave the program reduced the number of clients that could access services during outreaches, focusing
mainly on HIV care and treatment and prevention services.
Figure 1: Trends in Case Finding Among FSW from FY20 Q1 – FY21 Q2
“pause” in community testing “Un-pause” in community testing
Out of those who tested and got results, 122 tested positive with six percent case finding (122/1,898) but
when adjusted for testing connected to PrEP refills the case finding rate is seven percent (122/1,778). This
represents 35 percent (122/352) against the annual tested positive target.
As show in Figure 1 the program began to see a lower volume and higher case finding during FY21 Q2, as
we reduced services as a precaution against COVID-19. During this time, we only promoted HIV care and
treatment and prevention services not our more comprehensive services and reduced the number of
clients we can support.
The modality with the largest volume of clients that access testing is community outreach accounting for
72 percent (1,369/1,898) of total testing and for 70 percent (85/122) of all positives found, while the
community center accounts for 23 percent (442/1898) of testing and 26 percent (32/122) of all positives
found; appointment based testing (including decentralized drug distribution (DDD), HIVST confirmations
and Index Testing) for five percent (87/1,898) and 4 percent (5/122) of all positives found. This distribution
was driven by a 7 percent case finding through community centers and 6 percent through community
testing and appointment-based testing.
The program conducted an Enhanced Peer Outreach Approach (EPOA) campaign among FSW (and MSM)
in FY21 Q1. Fifteen seeds were identified, of which 93 percent (14/15) were 30 years and above. From the
EPOA data tracked, through the coupon system and linked to the seeds, 32 FSW were tested, with a case
finding of 22 percent (7/32). During the EPOA we saw an increase in HIV testing during the first two weeks.
Testing went from an average of 91 tests per week in the two weeks prior to the EPOA to an average of
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 4
186 per week in the first 2 weeks of the EPOA. Not all of these are formally linked to the EPOA, as they
did not return coupons, but often word of mouth about the EPOA circulates among the networks resulting
in increased numbers of people who come to access services but without coupons.
Both community outreach and community center testing include clients that want to receive HIVST
confirmatory test and Index Testing, as we offer all modalities to ensure that the location or time of testing
is not a barrier. The results specific to index testing and HIVST are presented in those specific sections.
Improvement strategies:
The FSW program is currently over target with HIV testing and under target with positive cases identified.
To improve on HTS_TST_POS while reducing over testing, the program is planning to:
▪ Conduct an EPOA, with priority for seeds only 30 years and above who will be tasked to mobilize
at-high-risk FSWs age 30 and above and to find seeds in hard to reach sub-population types (strip
clubs, mid-to high end hotels etc).
▪ Expand access to new FSW networks, through MWPS to mobilize FSWs.
▪ Recruit peer energizers in priority sub-FSW groups to support mobilization and linking their
networks to outreach workers for continuity of support.
▪ Intensify mentoring of ORWs, using both in person and virtual support.
▪ A TA plan will be developed to support the FSW led organization (VOOV) to improve on their
performance.
Men having sex with Men (MSM)
Reach (KP_PREV)7
A total of 2,752 MSM have been reached with a prevention package of services. This accounts for 87
percent (2,752/3,152) of the annual target. A total of 13 percent (357 /2,752) were known positive, of
which 19 accessed community level services such as one-on-one discussions or were given condoms and
lubricants but did not access clinical services. 2,733 MSM, or 99 percent of all MSM reached, accessed
clinical services, 61 were at non-FHI 360 services. Of those that accessed our clinical services 1,930
accessed testing services, 338 were known positive (included in the 13 percent noted above) and accessed
our non-testing services, 9 declined testing and 395, or twenty percent were not due for testing but
accessed non-testing services. The program implemented an EPOA in the first quarter of the year,
identifying eight seeds, through KPIF partners, to facilitate mobilization and inject new networks to the
outreach workers.
Impacts relating to COVID-19 are captured under the enhanced development of sustainable prevention
programs section that focused on the peer outreach and demand creation aspect of the program.
MSM accessing testing services and case finding: The program reached 2,752 MSM and of those 70
percent (1,939/2,752) were eligible for testing and 99 percent or 1,930 tested, while 9 declined testing
services. This has accounted for 154 percent (1,930/1,266) against the annual testing target. Of those that
tested, 12 percent (225/1,930) were for PrEP refills. Like the FSWs, the MSM also saw a rapid increase
7 Number of key populations reached with individual and/or small group-level HIV prevention interventions designed for the target population:
risk assessment, HIV education, condom and lubricants promotion and provision (CLPP), direct provision/navigation to HIV Testing Service
(HTS).
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 5
since community testing was “un-paused”, as shown below in Figure 2. While 12 percent of the testing is attributed to PrEP, as noted above, this is still a big increase compared to FY20 Q3. Out of those who tested and got results, 65 tested positive with 3.3 percent case finding (65/1,930) but when adjusted for PrEP refills the case finding rate is 3.8 percent (65/1,705). The absolute number of newly identified positives in Q1 was high, compared to prior quarters, but there was a drop in Q2, which was during the second wave. While the absolute numbers are not cause for concern, the overall case finding has dropped and is a concern as we are over testing. The potential reasons for over testing are noted below. The program is working to address this underperformance, with the improvement strategies noted at the end of this section. The modality with the largest volume of clients that access testing for MSM is through the Community Outreach testing accounting for 97 percent (1,909/1,930) of the total testing, which does include HIV ST confirmations, and 100 percent (65/65) of all positives found, while index testing accounts for one percent (21/1930) of testing and 0 percent (0/65) of all positives founds. As with FSWs the community outreach testing can include clients that want to conduct HIVST confirmations and Index Testing, as we offer all modalities to ensure that the location or time of testing options is not a barrier. The results specific to index testing and HIVST are reviewed in those specific sections. Figure 2: Trends in case finding amongst MSM for FY20 – FY21 Q2 Within the MSM program there have been no programmatic shifts from prior quarters, but we continue to see high volumes of testing and low case finding. Anecdotally it is believed that due to COVID-19 the ORWs have reverted to closer networks, which are easier to reach and to mobilize, and are often under 30 years old and regularly test. Figure 3 below shows a decline in reaching and testing older MSM and increase in reaching younger MSM, below age 30. Testing for MSM below age 30 went from an average of 55.5 percent from previous quarters to 65.5 percent in both FY21 Q1 and Q2. MSM under age 30 consistently have low case finding. EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 6

During the EPOA campaign conducted in FY21 Q1 we reported an increase volume of testing based on word of mouth, but not linked to the coupon distribution that is used to track EPOA specific performance. For example, in the first two weeks of the EPOA we had an average of 202 MSM accessing services, compared to the two weeks prior average of 107 MSM, but only 72 MSM returned coupons during the whole EPOA campaign. The EPOA did not contribute to case finding as only 3 percent (1/32) MSM tested positive from those identified through the coupon-returned system. This low case finding is based on the eight seeds identified by the KPIF partners, with only 50 percent (4/8) being 30 years and above, which is our target age group. As a result, 57 percent (41/72) of those mobilized were below age 30. The selection of “right” seeds is to be corrected in the next EPOA, starting in FY21 Q3. In FY21 Q2 there was a drastic drop in overall testing, but this is attributed to the second wave of COVID- 19 that started at the end of December and went through the end of February. As a result of the second wave, the program reduced the number of services due to restrictions on how many people can access the mobile at a time, as well as curfews that impacted the hours of the mobile and community center. As noted below in Figure 3, there was a slight increase of 7.6 percent in reaching older MSM (30 years and above) in FY21 Q2 from Q1. Figure 3 shows the overall trends for testing by age from FY20 through FY21 Q2. There has been an average of 10 percent (from 52 percent to 62 percent) increase in MSM under the age of 30 accessing testing services from FY20 Q1 – Q3 and FY 20 Q4 – FY21 Q2. Yet the under 30 age group accounted for close to the same HIV testing distribution with 43 percent to 45 percent from FY20 Q1 – Q3 and FY 20 Q4 – FY21 Q2 respectively. The program mobilized and provided testing services to a larger number of MSM under 30, as also explained above, which historically has a much smaller case detection rate, thus impacting performance and supporting an increase in testing but a low case detection rate. Figure 3: Trends in HIV testing distribution by age group amongst MSM It is worth noting that prior to COVID-19 the program focused on mobilization of MSM that are medium to high risk for HIV, and following the restart of the community-based testing, additional risk factors (e.g. EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 7

GBV, psychosocial needs, willingness to access none-MOH clinical services) were taken into account when
assessing for HIV testing eligibility besides risk factors included in the program’s community risk screening
tools. This has been discussed with the KPIF partners, but it has been complicated to address in the
context of both MSM programming and COVID-19.
Under the MSM program, our risk assessment tool results report a high number of medium and high-risk
clients being reached whereas their testing results indicate a low case finding. We believe that this is
partially linked to the above informal reclassification of who is at risk, but we have also begun the process
of reviewing the risk assessment tool to strengthen possible gaps. MSM ORWs will be re-trained to make
sure they improve their scoring, and their supervisors will provide more mentorship in terms of how to
help navigate those MSM that are at medium to high risk for HIV and need access to testing and
prevention methods and those that need other services. In the interim, the KPIF partner’s program
managers have been encouraged, and they have started, to do more field supervision to support and
correct any errors from ORWs when using the risk assessment tool.
Improvement strategies:
The MSM program is currently over target with HIV testing while on target with positive cases identified.
To maintain achievement on HTS_TST_POS while reducing over testing, the program is planning to:
▪ Conduct an EPOA, with seeds only 30 years and above who will be tasked to mobilize at-high-risk
MSM age 30 and above. This is based on data evidence of higher HIV cases among this age group.
▪ Continue to focus on index testing and RNR with fidelity among MSM clients.
▪ Improve strategy of distributing HIVST, focusing on distribution to those high risk for HIV.
▪ Strengthen the targeted testing at the TRUE community centers and mobile sites by targeting only
high-risk clients, for HIV, through the risk assessment tools with improved mentoring and
supervision by the KPIF partners who manage the ORWs.
Transgender (TG)
This is the first formal program period for transgender persons under PEPFAR programming. Demand
creation for TG is under one of the KPIF partners, House of Our Pride (HOOP). HOOP has engaged two TG
outreach workers to help mobilize. During the first reporting period, 68 TG8 have been reached with a
prevention package of services. Mobilization for TG women currently includes access to community
programming (one on one or access to condoms and lubricants) and clinical services that are KP friendly,
but do not include gender affirming care, which is a gap in the program. Gaps in programming are due to
lack of funding to support a comprehensive TG program in FY21, and the need for MOH approval.
For the TG program, current performance for KP_PREV is at 62 percent (68/110). A total of 45 TG were
referred for testing within this period and accessed FHI 360 clinical services, of which 34 TG accessed
testing services, or 110 percent (34/31) of our annual target with zero positives identified to date. An
additional 23, out of the 68 reached, were either referred for testing, but FHI 360 was not able to provide
mobile services to that area, or they accessed services at a MOH clinic, but did not provide an update on
the visit.
8
There is currently no size estimate for TG persons in country, but informally mapping of the population through LINKAGES, TransSwati (the
TG-led CBO in country) and the recently completed IBBSS and Size Estimation that allowed us to review a subset of the MSM population
through inclusion of TG questions, has the population sized between 100-200 TG persons (including both Trans Women and Trans Men).
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 8
The program has also worked with TransSwati, a local TG-led organization, that is not part of the KPIF, to
collaborate on TG programming. While HOOP is responsible for demand creation of TG women under the
program, collaboration with TransSwati will support a stronger program to support the TG community.
HOOP will work closely with TransSwati during the remaining portion of the program to increase demand
for services to meet the set targets. TransSwati will also conduct an update of mapping and size estimation
for TG community at hotspots/networks level as well as TG 101 discussions, which is about engaging the
TG community on issues pertaining their identity, under the KPIF.
Improvement strategies for TG programming:
▪ Conduct training of all HOOP ORWs on transgender issues so they can all support TG mobilization.
▪ Conduct transgender health talks on different topics: psychosocial services (PSS), gender-based
violence (GBV), sexual behaviour, prevention, treatment, and care issues related to TG to increase
mobilization and visibility of this community through issues of interest to them.
▪ Engage a seed for the planned Q3 EPOA from the TG community.
▪ Conduct weekly feedback sessions with TG ORWs.
▪ Promote the True Eswatini online programs within TransSwati social media platforms as another
mobilisation strategy to the TG community.
People who inject drugs (PWID)
This is the first formal program period for PWID under PEPFAR programming. 19 PWID received clinical
services (6 females and 13 males) 12 percent (19/164) of our annual target; 11 PWID who were eligible
were tested for HIV and received their results, 31 percent (11/35) of the annual target; 1 tested positive
and was initiated on treatment, 25 percent (1/4) of the annual target.
Under the PWID program FHI 360 collaborates with the Global Fund partner who leads on PWID
programming in country, Alliance of Mayors Initiative for Community Action on HIV /AIDS at the Local
Level (AMICAALL). We continue to work with them to grow their program, which has struggled under
Global Fund, in part due to a lack of a formal harm reduction program which leaves both Global Fund, and
PEPFAR, without any specific program to help attract PWID. Thus, the introduction of some basic service
provision for PWID as noted above is expected to make a big impact, but also requires a greater
stakeholder involvement for the sustainability of the program and future harm reduction initiatives.
Improvement strategies for PWID Programming:
The program has started some of the strategies in the reporting period and will be expanding in the next
semi-annual period. These include:
▪ Training of service providers:
o Short term: Will receive support from the FHI 360 India program to put together a training
package and train our service providers on basics of service provision to PWID
o Long-term: the program will plan a comprehensive training for providers with the MOH
based on feedback from the first training.
▪ IEC material:
o The program has received material from the FHI 360 India program and will adapt
according to what can work in our context.
▪ Expand mobilization of PWID for service access:
o The program engaged a mobilizer for short-term to mobilize PWID specifically.
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 9o Peer Energizers from PWID will identified and trained.
o Conduct EPOA specific for PWID after the EPOA for other populations.
Pre-Exposure Prophylaxis
PrEP trends among all populations in FY21
As shown in Figures 4-6, 3,770 KPs (1,776 FSWs, 1,865 MSM, 34 TG, 10 PWID and 85 MWPS) tested
negative during the reporting period and over 99 percent were offered PrEP, of which 32 percent
(1,189/3,644) started on PrEP (544 FSWs, 627 MSM, 8 PWID, 9 TG, 1 MWPS). This is 110 percent
(1,189/1,085) of our FY21 PrEP_NEW target for all population types; 79 percent (544/686) for FSWs, 159
percent (627/394) for MSM and 180 percent (9/5) for TG. This also shows a 31 percent (544/1,776) uptake
of PrEP services for FSWs; 34 percent (627/1,865) for MSM and 26 percent (9/34) for TG persons, one
percent (1/103) for MWPS and 80 percent (8/10) for PWID.
Of the 1,189 PrEP_NEW, 80 percent (946/11,89) initiated through the mobile clinic, 19 percent
(226/1,189) at the community centers, and 8 through DDD, 2 after HIVST confirmations and 7 during
Index.
Among the 1,189 KPs new PrEP starts, 57 percent (677/1,189) refilled after 1 month. We also have an
additional 601 PrEP refill visits during the reporting period. During the reporting period we have a
cumulative 1,461 for PrEP_CURR, over 86 percent (1,461/1,700) of our FY target. Of those that reported
to be current on PrEP, 48 stopped PrEP due to various reasons including mild side effects, no longer feeling
at risk, unable to find time to go for their re-fills. Some stopped without giving a reason. We also had eight
clients restart PrEP.
Figure 4: Negative Cascade for FSW – FY21 YTD
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 10Figure 5: Negative Cascade for MSM – FY21 YTD
Figure 6: Negative Cascade for TG – FY21 YTD
During FY21 the program expanded PrEP refills to be included in our DDD services, of which 43 percent
(156/370) PrEP refills were through DDD services.
We continue to see strong uptake of PrEP for both MSM and FSWs, and during this quarter among TG as
well, but the reasons noted for not taking PrEP remain similar as prior quarters. Clients verbalizing not
being at risk, not ready for a daily pill and the need to discuss with partners. We also took the opportunity
to address misinformation during the discussions with PrEP clients, whereby some believed that
protection would have been reached through one pill only as opposed to taking a daily pill.
To improve on the retention on PrEP, for those still at risk the program did the following:
• Submitted a concept note to the MOH to roll out PrEP specific bill bottle labels, to reduce the
stigma of PrEP not being ART and to provide pill containers for PrEP to allow for more privacy
around PrEP usage and to make it easier to carry. These will be rolled out in Q3.
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 11• Conducted a push on accurate information about PrEP through our HCWs and through our online
platforms under the KPIF.
• The FHI 360 Linkage Case Manager (LCM) has been working closely with KPIF partner’s LCMs on
improving follow up of PrEP clients focusing on counseling support.
• The program has also worked to re-distribute PrEP educational videos to be played on the ground
at the community centers and at outreaches.
Recency Testing
Eswatini is implementing surveillance for HIV-1 recent infections: – Eswatini HIV-1 Recent Infection
Surveillance (EHRIS) Program. EHRIS implementation began with 39 sites on 1 July 2019 with FHI 360
activation in January 2020 through the implementation organization leading this as research, ICAP, on
behalf of the MOH. While still considered research, it is standard of care in all health facilities that have
been trained and have the required resources to take DBS or VL.
For the semi-annual reporting, 192 tested positive with 83 percent (159/192) of all positives having
recency done, including those that are not included in reporting for KPs or PPs. This is 45 percent
(159/354) of our annual target. The 33 that were not done (10 in Q1 and 23 in Q2) are due to a gap in
training that was addressed in October and in Q2 due to data quality gaps as recency was done but the
data was not entered into the recency data base for ICAP, thus their results were not processed at the
laboratory. Additional training and weekly checks were instituted once the data gap was discovered in
March, as this had not previously been an issue9. The clinical register and daily reporting tools have been
revised to capture recency done with providers sharing all used bar codes to the HTS focal person for
entry.
In Q1, providers (new nurses and counsellors) were trained on the overview of EHRIS protocols, EHRIS
procedures in routine HTS, ethics and consent and data collection. The training also included practicals on
conducting quality EHRIS procedures.
All providers were provided a refresher training, in Q2 by ICAP, the EHRIS supporting partner. The training
focused on mentorship with emphasis on improving data collection.
9
In Q3, during the first week of April, this gap was discussed during an index refresher training. As of that training the HTS officer now checks
all tablets to ensure all clients have been entered.
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 12Linkage and initiation to treatment Figure 7: Trends in Linkage to ART Among All Populations - FY20 – FY 21 Q2. The linkage to treatment rate in FY21 is 78 percent (136 TX_NEW and 14 TX_NEW_VERIFY), this is a decrease from FY20 which had a cumulative linkage rate of 102 percent (408/399) as shown above in Figure 7. Post reporting an additional 10 clients have been verified as linked to treatment for a revised linkage to treatment rate of 83 percent (160/192). EpiC Eswatini does not have treatment targets under COP but ensures that our clients have support across the treatment cascade. The program has not reached the 95 percent linkage to treatment benchmark by PEPFAR, as driven by low linkage rate among FSW compared to MSM; but it has continued to improve with more clients directly initiating with FHI 360 and staying within our cohort of services making it easier to verify and track. The program continues to use the MOH’s Linkage Case Management approach, and links clients to ORWs, who are trained on peer navigation. Sixty one percent (118/192) of all HIV positive clients accepted an ORW as a peer navigator. The main reason why clients do not want to link with an ORW is due to privacy reasons, but they are linked to the Linkage Case Manager (LCM) from FHI 360, or from one of the KPIF partners, who have an LCM. Twenty-nine percent of HIV positive clients (56/192) did not initiate on the same day, and of those 51 percent (30/56) have since initiated. All clients that did not initiate on the same day or are still pending initiation are being followed up and supported through counselling by the ORW, if linked, and by the LCM until they overcome the barriers of enrolling into treatment. There are also 9 clients that we are not able to locate due to incorrect contact information. While we try to verify all contact information on site, clients will claim they do not have their phone with them or will say they are borrowing the phone to call a family member instead, and then subsequently give a false number. We continue to experience delays in verification, for clients that choose to initiate at MOH clinics, due to COVID-19, as clinic visits to verify ART registers have not been safe, and verification over the phone has mixed results as HCWs at the clinics are overburdened. The program continues to work with clinical partners and use the MOH’s electronic medical record system (CMIS) to verify but often see a gap in data entered. The MOH has noted there are delays in data entry for “down time forms” so data from the CMIS is not always up to date, with months back log at some clinics. We also continue to also see difficulty based on demographic information not matching information in the CMIS. EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 13
The issues relating to verification of clients at MOH clinics will be addressed in Q3 as the program moves
towards an integrated data collection platform for our clinical data, directly linking with the MOH’s CMIS.
This will allow the program to directly verify clients access at MOH clinics, and it allows us to register the
client directly in CMIS during service provision, thus when they go to the clinic the demographic
information will match. We are also in discussion with the MOH about requiring clients to have their
national IDs when accessing services to ensure verification. This is currently not a requirement for the
MOH, but we continue to see discrepancies, as does the MOH, where clients will initially present under
one name for testing but will then return to initiate or refill under a different name, with their national
ID. This on its own is not abnormal to our program but it is further complicated as we are not within the
larger MOH system until we move to the CMIS projected to be in FY 21 Q3.
Linkage and initiation to treatment for FSW: In Q1-Q2, 83 FSWs were directly initiated to ART by EpiC,
and 15 were confirmed to have linked to treatment with their preferred clinic, resulting in 80 percent
(98/122) of clients confirmed on treatment10 as shown in Figure 8 below. Delays in verification of clients
initiating at MOH clinics is discussed above. The FHI 360 LCM provides support for all FSWs, as during the
KPIF program VOOV does not have an LCM on staff.
To address the low linkage to treatment rates EpiC Eswatini will implement the following strategies:
a. Review schedule for the community center and home-based appointments/DDD, which supports
initiations, to ensure that times/days work for the FSWs.
b. As the MSM LCMs continue to grow, shift focus to FSWs to intensify support.
c. Work with health care workers to ensure that counselling and support during services is strong
and guide on counselling areas for those that “want to think about it”, “want to consultant their
partner” or “those that are just not ready”.
Figure 8: Positive Cascade for FSWs – FY21 Year to Date
10Clients are tracked in two categories: treatment initiation through direct service delivery (TX_NEW) and those that we can directly verify at
the clinic where they access their services and are supported through the program through appointment reminders, counselling as required,
peer navigation support at the community level (TX_NEW_VERIFY).
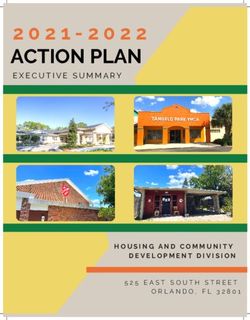
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 14Linkage and initiation to treatment for MSM: In Q1-Q2, 50 MSM were directly initiated to ART by EpiC, and 15 were confirmed to have linked to treatment with their preferred clinic resulting in 100 percent (65/65) of clients confirmed on treatment as shown in Figure 9 below. The LCM’s under the KPIF partners have been working hard to ensure that all MSM that do not initiate on the same day are linked to the MOH clinic or are provided with home-based initiations. Figure 9: Positive Cascade for MSM – FY21 Year to Date Continuation on treatment11 During the reporting period, a total of 296 clients were due for ART refills, and of those 86 percent (255/296) received their ART refills, 16 percent (40/255) refilled through DDD, as shown in Figure 10, 13 percent (32/255) through community mobile outreach and 72 percent (183/255) through the two community centers. For the 14 percent (41/296) who interrupted treatment, 12 percent (5/12) were refilled and returned to treatment. Of the 36 that have interrupted treatment, 10 are part of the FHI 360 cohort (receiving treatment through FHI 360) and 26 were receiving treatment at MOH clinics. 27 of the 36 were not reachable as they have changed numbers or have moved and did not inform our team to where they have moved. Permanent site refills12 identified in FY20 Q4 failed to take off with few ART clients preferring refills at the community centers or nearest facilities. This has been reviewed with the need to go to areas that need services or that are further away from the public health facilities. Further development of this activity was suspended due to the 2nd wave of COVID-19, and focus moved to home based DDD to scale up for ART refills, as well as PrEP refills. 11 The program supports ART refills through the following methods: Community Centers, which are KP focused drop-in centers; DDD which is normally home-based appointments for refills for clients devolved from our own community centers or from MOH clinics and through Mobile Outreach which is our routine clinical services, which includes initiations and refills for locations we routinely frequent. 12 Permanent site refills are “hotspots” where FHI 360 will return monthly with our mobile, allowing for refills for ART, and PrEP. EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 15
Figure 10: ART refills for FY 21 year to date, with the breakdown for DDD refills
ART Refills
70
59
60
47
50
39 39 39
40 32
30
20
10 19
3 11 7
0
Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
Total Refills DDD Refills
Figure 11: TX_NEW and TX_CURR services for FSWs for FY21 Q1-Q2
For FY21 Q1-Q2, 152 FSWs have reported to be current on ART, with ten of those clients having been
returned to treatment, as shown above in Figure 11. This overall provides a loss of 59 clients from our last
reporting period (FY20 Q4). This loss is based on TX_CURR_VERIFY being impacted by COVID-19, as noted
above. The impacts for FSWs are greater as often FSWs use different names when accessing services and
requires addition verifications to ensure it is the same person, and there are more clinics that FSWs prefer
compared to MSM, just based on overall larger numbers of FSWs. If we are not able to verify that they
went to their visit, when scheduled, we are not able to report them as TX_CURR_VERIFY. This does not
mean they did or did not honor their appointments it means we are not able to verify. While we call
clients, we often find self-reporting does not match what is found at clinics. We hope that with the
adjustments noted above and with the introduction of CMIS into our data system we are better able to
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 16capture this in real time, and thus provided adjusted support to clients that are truly interrupted in treatment. Figure 12: TX_NEW and TX_CURR services for MSM for FY21 Q1-Q2 For FY21 Q1-Q2, 154 MSM have reported to be current on ART, with three of those clients having been returned to treatment. This overall provides a net gain of 24 clients from our last reporting period (FY20 Q4). This gain is based on the follow up done by the KPIF Partner’s LCMs with guidance from the FHI 360 LCM officer and through support through the ORWs, for those linked. 255 clients received 3 MMD (Multiple month distribution) out of 289, or 88 percent, but there is a need to increase to 6 MMD after getting clients VL results, with suppressed results. The 34 that did not receive 3 MMD but received less is due to supply issues around expiration dates, and the clients not being eligible for 3 months. 100 percent of clients are provided with TLD (TDF,3TC, DTG) treatment regimen. Documentation of Viral Load Testing Suppression FHI 360 coordinated with AHF to start the process of taking VL for the clients accessing services from FHI 360. Taking VL from clients at FHI 360 services started in January 2021. Current VL report captures clients from the FHI 360 cohort and MOH cohort, as we only started conduct VL directly in Q2. As we conduct VL testing in future quarters we will break out the reporting accordingly. As of Q2, 112 clients were eligible for VL, of which 53 have been taken and 31 have received results. Of the 31 results received, 29 are suppressed and two unsuppressed, providing a viral load suppression rate of 94 percent (29/31) with 22 are awaiting results. VL Clients are mainly reached through DDD and community center services. The two unsuppressed are undergoing Stepped Up Adherence counselling13. The status for the two unsuppressed clients is that one has been redrawn, post the reporting period, 13 Stepped up adherence counselling (SUAC) is a MOH approved counselling tailored for clients with poor adherence or unsuppressed VL. It is found in the 2018 HIV care guidelines. A client with unsuppressed VL is called and informed of the result. Client is refilled monthly and follow up done by LCM with assistance from the ORWs linked. EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 17
and now suppressed and the second has been booked for viral redrawn and has been provided counselling support. FHI 360 collects blood samples, through whole blood and spin, and submit to AIDS Health Care Foundation (AHF), our mother facility, that then submits to the National Lab. There are currently gaps in getting test results returned as the national ID (or a secondary option is a phone number) is used to track the lab samples and results are directly returned in to the MOH electronic medical records (EMR), the CMIS. For most of our clients we do not require, but do request, a national ID to initiate or to obtain refills. This is becoming a gap within the submission of the VL data, which we will work to address with the MOH. The program has not started VL DBS blood draws pending SOP approval from the MOH. When approved, EpiC will be able to send DBS samples directly to the National Lab without the need to spin as dried samples can be kept for two weeks. The TX_PLVS_VERIFY reporting still has gaps in terms of providing a comprehensive view of TX_PVLS/TX_PVLS_VERIFY for KPs but the ability to report this data shows an increase in improved success accessing VL results due to access of results at the clinic level, which was not the case at the start of the FY. During the current reporting period there is no VL data related to MWPS and PWID as they are not yet eligible. Commodity distribution: The program distributed 601,106 male condoms; 91,630 female condoms and 415,294 lubricants to KPs during clinical services and through the community outreach workers. 58 percent of all distribution is through outreach workers at the community level. Index testing Figure 13: Index testing cascade for all populations, FY21 Semi-annual report EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 18
Index testing was offered to 291 (186 FSWs, 94 MSM, 1 MWPS, 1 PWID and 2 non-KP) with 191 being newly tested clients and 100 known positive clients. Of those offered, 84 percent (244/291) accepted index testing and provided 349 contacts or a 1:1.43 ratio as noted in Figure 13. EpiC Eswatini does not have COP targets linked to index testing but we implement it as it is standard of care under the MOH. The following results are as of the time of submission of this report, or as of April 20, 2021, while the graph above depicts the results as of the time of reporting in DATIM. Out of the 349 contacts that had been elicited, 137 (43 percent) were found and either tested or reported as known positive. Of the 137, 63 percent (86/137) were known positive and 51 were tested and two tested positive (4 percent case finding). Among the 212, not reached, 53 were un-reachable through the numbers provided, 17 continue to not answer our calls, and we are not able to find them in person, 18 declined testing, 87 are pending contact and 37 have been reached but not yet tested during the reporting period. Thus only 295 clients (elicited contacts minus those unreachable) were viable contacts. Of the 37 pending visits, two continue to not pick up the phones when confirming their appointments,4 phones have been off since we originally set an appointment with the client, two have tested positive (and will be reported in Q3), six were negative (and will be reported in Q3), three are known positive, one declined, 19 continue to reschedule their appointments. The two that tested positive, during the reporting period, requested to initiate at a facility of choice and are being contacted to confirm if linked on treatment and two clients were initiated on PrEP. In Q2 the program offered virtual indexing, reported in the above, to four clients who had been identified in a review of our index tracker as not having contacts elicited during routine services and three accepted and six contacts were elicited for a ratio of 1:2. Of those contacts we have reached 16 percent (1/6) with one testing, with a positive result. The program continues to utilize virtual indexing if any clients are missed during clinical services. Figure 14: Index testing cascade for FSW and MSM, FY21 Semi-annual The population specific index cascades, as shown in Figures 14, look similar with consistent gaps that need to be addressed. We also conduct index testing for PWID and MWPS (and will for TG when eligible) but currently the numbers are too small to determine any population specific needs for PWID and MWPS. The main gaps are discussed in the Table 1: Eswatini TA on Index Testing Action Plans. The program has a low rate of finding elicited contacts, per Figure 13. We are at less than 50 percent for both males and females. Historically the program had partnered with PSI and TLC to help conduct tracing for hard-to-find clients, if not found after 14 days, due to their ability to canvas a neighborhood to enable EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 19
them to test the targeted index client. In 2019 PEPFAR changed how Clinical and Community partners
were asked to collaborate around index testing interrupting this approach. EpiC Eswatini will reach out
and see if we can re-establish this collaboration. Starting at the end of the reporting period we began
trying to verify contact information for the contacts elicited through the main mobile carrier in country,
MTN to see if their numbers are registered and confirm the names. This will help in ensuring we have
accurate phone numbers as the starting point.
Index testing is offered through our community centers, community outreach and available through
appointment/home-based testing services. During the counselling we work with the client to identify
what is the best service option to ensure we do not disclose the index clients KP status. Overall index
testing is primarily done through booking contacts for home-based testing and followed up by a nurse
who offers testing services and offers ART to positive clients and PrEP to the negative clients. Index testing
while a targeted activity with two dedicated days weekly continues to require extensive focus due to the
number of contacts we can test daily through appointment-based testing. While we organize by
geography, we are only able to support three to five contacts per day, as most choose appointment-based
services versus accessing our mobile outreach or the community centers, and often contacts reschedule
last minute or do not show up for the appointment. For efficiency we combine index testing with HIV ST
confirmations, and DDD services which are also done through appointment-based services.
Three EpiC Eswatini staff were trained on Intimate Partner Violence (IPV) and index testing, as trainer or
trainers, with training materials that speak to the needs of our populations. The team then cascaded the
training to the eight additional HCWs that support EpiC Eswatini clinical services. An additional training is
planned for April to train any new HCWs, as well as to provide a refresher on Index Testing. During this
reporting period an SOP IPV for Index Testing (and HIV ST and PrEP) was completed and approved.
The Eswatini team engaged support from the EpiC technical assistance team. We reviewed current data,
identified where we need to improve programming, and identified approaches to support improving our
performance under index testing, captured in Table 1.
Table 1: Eswatini TA on Index Testing Action Plan
Issue Actions to Consider Status
Observe providers when providing ▪ All HCWs were observed when providing index testing. Feedback was
Improving index testing and assist them where provided to all HCWs. The main gaps identified were:
contact there are gaps. A. Not providing index testing to those that are known positive or not
eliciting documented for viral load, or in some cases not offering indexing.
B. Index testing being offered posttest when program guidance is to index
prior to testing.
C. Not asking about other sexual partners or associates besides the stable
partner
Consider a mystery client approach ▪ We received feedback from pre-identified clients on their indexing
who can give a feedback on where to experience. The main feedback provided was:
strengthen support. A. Known positive clients were not asked their viral load
B. Associates and children not asked during index testing. The program is not
able to conduct testing services on children, and thus all those indexed will
have to be referred to a regional clinical partner.
C. If partner is on ART, the client was not asked when ART was started and if
the viral load was taken.
▪ The program will conduct a more formal mystery client approach in Q3.
Training of providers should also ▪ Inclusion of complex case studies was included in the index refresher
discuss complex case studies and how course held in Q3, on April 7th-9th
to deal with them.
Review current index testing script ▪ Current scrips were reviewed, but it was determined that these were
and make it stronger. sufficient.
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 20Issue Actions to Consider Status
Eliciting from clients who have HIV+ ▪ This is being reviewed by our clinical team to help to document this
partners under indexing.
Tracking TX_CURR and ▪ Program has re-discussed with HCWs that all HIV + clients that are not
TX_CURR_VERIFY cohorts: yet suppressed, are not yet on treatment or have only recently become
suppressed, are indexed. Anyone that might be identified as missed,
post service provision, is virtually indexed.
Eliciting RNR from clients: ▪ The program utilizes peer energizers (to support access to risk
This will require adding narrative of networks) and we implement an EPOA. In addition, we are integrating
RNR in the eliciting script and RNR into our index approach including documentation in the index
recording separately in the tools. reporting documents and updating the script. The indexing script to
include RNR needs to be completed with our KPIF partners to ensure
we are sensitive to the populations. We expect this to occur in Q3.
HIVST
Figure 15: HIV Self Testing Cascade all populations, FY21 Semi-annual
Figure 16: Trends in HIV Self Testing Among all Populations – FY21 Semi-annual
EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 212,077 KP and priority populations (PP) received (were distributed to) HIVST kits (1,477 FSWs, 366 MSM, 21 PWID, 111 MWPS, 26 TG and 76 were uncategorized), this is 23 percent (2,077/8,904) of our annual target. The current quarterly allocation from CMS, of 1,750 per quarter, will not allow us to reach our annual target. In addition, we only received our allocation for Q2 at the beginning of March but had started to run out in December. Of those distributed 96 percent (1,997/2,077) were through assisted and 80 unassisted distribution. Program beneficiaries primarily choose assisted at the community level to allow support on completing the HIVST screening and providing ability to access an appropriate referral to necessary care and quick access to confirmations for those that have screened reactive or want to start PrEP. As shown in Figure 15, 91 percent (1,888/2,077) were reported used and of those 4.7 percent (88/1,888) were reported as screened reactive, 71 FSWs, 10 MSM, 6 MWPS, and 1 TG. Seventy-nine, or 90 percent (79/88) were provided testing for confirmation by the program and 8 were confirmed at a facility of choice. Of the 79, 47 (32 FSWs, 9 MSM and 6 other) were confirmed positive, or a 2.4 percent case finding, 0 were known positive and 32 were confirmed negative and of the eight confirmed at facility of choice no results were provided. One percent (1/88) were pending confirmation of results at the end of March, not including the eight that have refused to provide their results. For those pending confirmation they are attributed to ORWs who resigned, and we can no longer trace their contacts, and to clients not scheduling for confirmations to be completed or confirming at another clinic but not providing us the information. As of April 30, 2021, of the 1,888 that were reported as used, 116, or 6.1 percent, screened reactive, with 81 confirmed as reactive, for a 4.2 percent (81/1,888) and 94 percent (76/81) were confirmed linked to treatment. As a program we continued with the process of strengthening demand creation for and distribution of HIV ST kits at the community level. This reporting period, distribution of HIV ST was focusing on clients who are at medium and high-risk, according to the risk assessments thus not to anyone that wants a kit. This was a shift from previous implementation experience. In addition, the ORWs used the risk network referral (RNR) method. After the Outreach Worker has assigned a risk score to a peer, that is high or medium, the peer is given HIV ST kits to give to their networks and follow up is made on the used HIVST kit. Community distributions of HIVST kits continued in Q1 and the beginning of Q2 to allow KPs to have access but was not active in hotspots like bars, hotels, and clubs because they were closed. These community distributions have since been reduced as the lockdown restrictions were lifted and ORW were able to move and conduct one on one distributions. There was a challenge with community distributions as the ORW were not able to track the use of these kits and follow ups were difficult due to incorrect contacts left at the distribution point. HIVST contributes to 24 percent (47/192) of all cases identified through the main testing modalities, but currently we have a 2.4 percent case finding rate, but as noted in Figure 16, both December and February having high percentage reactive rates, 16.7 percent, and 8.3 percent respectively. There were no new approaches or interventions used during that time so we plan to further look at disaggregation of the HIVST data to help guide where we can improve distribution to see if that is the reason for this shift. We do think it is based on some KP partners being stronger at identification of medium to high-risk individual and when they distribute during the program period. As the current HIVST case finding by KPIF partner and FHI 360 are: EpiC Eswatini Semi-Annual Report (FY21 Q1-Q2 October 2020 to March 2021) 22
You can also read