MEDICAl JournAl RHODE ISLAND - Spotlight: RIMJ Timeline of COVID-19 in 2020
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
RHODE I S LA N D
M E D I C A l Jo u r n a l
Spotlight: RIMJ Timeline of COVID-19 in 2020
See page 74
F ebru a r y 2 0 2 1 VOLUM E 104 • NUM BE R 1 ISSN 2327-2228
URGENT RESOURCES
FOR URGENT TIMES.
In a pandemic, speed and access to information and You can access Coverys’ industry-leading Risk
resources are vital. Management & Patient Safety services, videos, and staff
training at coverys.com.
Knowledge saves time, and you need all the time you can
get to save lives. Introducing the COVID-19 Resource Center. All in one place, for our policyholders as well as for all
Right here, right now, for you. healthcare providers.
On our website, you’ll find the latest information and Thank you. For all that you are doing. You are our heroes,
resources for important topics like: and we are here if you need us.
• Telemedicine: including best practices and plain
language consent forms
• Links to infectious disease prevention guidance
• Education and resources for healthcare providers on
the front lines
Medical Liability Insurance • Business Analytics • Risk Management • Education
COPYRIGHTED. Insurance products issued by ProSelect® Insurance Company and Preferred Professional Insurance Company®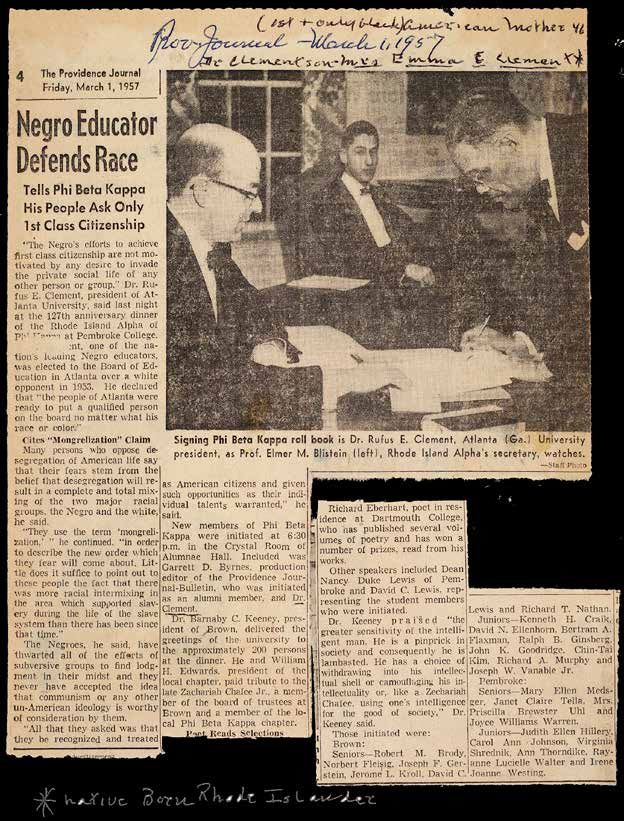
RHODE I S LA N D
M E D I C A l Jo u r n a l
14 Clinicians’ Update:
Kidney Transplantation in End-Stage Renal Disease (ESRD)
Reginald Gohh, MD
Guest Editor
Reginald Gohh, MD
15 Frailty and Kidney Transplantation
George Bayliss, MD
20 Management of Cardiovascular Risk Factors
in Dialysis-Dependent End Stage Kidney Disease
Harshitha Kota, MD
Reginald Gohh, MD
25 Malignancy After Renal Transplantation: A Review
Edward Medeiros, DO
Basma Merhi, MD
31 Managing Side Effects of Immunosuppressants
Krista Mecadon, PharmD
34 Transplantation of Hepatitis C-Infected Kidneys
into Uninfected Recipients: A Review of the Literature
Haley Leesley, MD, MS
Adena J. Osband, MD
3
RHODE I S LA N D
M E D I C A l Jo u r n a l
8 C OMMENTA RY
Why don’t doctors return phone calls?
Joseph H. Friedman, MD
Gender-based Differences in the Societal
Impact of the COVID-19 Pandemic
Christina Matulis, MD
Mehrnoosh Samaei, MD, MPH
Ghada Bourjeily, MD
Alyson J. M c Gregor, MD, MA
6 7 RIMS NeW S
Working for You
7 1 RIMJ Around the World
Providence, Rhode Island
Dublin, Ireland
7 4 SPOTLIGHT
RIMJ COVID-19 Retrospective
Mary Korr
7 8 HERITA GE
Dr. Carl Russell Gross Collection
documents RI’s Black History and Heritage
GP served his patients for decades but was
denied hospital privileges in Providence
Mary Korr
4
RHODE I S LA N D
M E D I C A l Jo u r n a l
In the news
Dean Gary Liguori 82 86 Martin A. Weinstock, MD
of URI College of Health Sciences, Robert Dellavalle, MD
updates ACSM’s “Guidelines for basal cell carcinoma chemo-
Exercise Testing and Prescription” prevention VA trial funded
Rhode Island 82 87 Brian J. Pickett, MD
receives $70.4M to expand COVID-19 Stephanie Krusz, MD
testing, vaccine distribution efforts join South County Health
Brown researchers 83 as South County Primary Care
designing adverse event monitoring system
for post-covid-19 vaccination impacts 88 Michael F. Armey, Phd
in elderly nursing home residents Melanie Bozzay, Phd
of VA, Butler awarded DHHS
Trio of centenarian Navy veterans 83 $2.24M grant to study
receive COVID-19 vaccination sleep disruption, suicide risk
Lung Association Report 85 89 Lifespan Urgent Care
RI has mixed grades in ending tobacco use opens 3rd location in Providence
CARE NEW ENGLAND 86 89 Developer closes
expands services in South County on former Memorial Hospital site
P eop le/ P LA C ES
Maria Ducharme, DNP, RN 90 91 Elizabeth Damoura Moreira
named Miriam Hospital President appointed Pawtucket's Public Health
and Equity Leader
Patrick Tigue 90
confirmed as OHIC’s 92 Michael J. Frank, PhD
new Commissioner of Carney Center, honored by
National Academy of Sciences
Tiffney Davidson-Parker 90
named President, COO 92 Marie Ghazal
of The Providence Center recognized with RI Foundation
Murray Family Prize for
Angela Bannerman Ankoma 91 Community Enrichment
named V-P, Director of
Equity Leadership Initiative 93 Obituaries
at Rhode Island Foundation George N. Cooper, Jr., MD
Christine Foley, MD 91 David C. Lewis, MD
elected to Fellowship Charles J. McDonald, MD
in Minimally Invasive Michael Anthony Passero, MD
Gynecologic Surgery Board
5
F E B RUA RY 2 0 2 1
VOLUME 104 • NUMBER 1 RHODE I S LA N D
P u b l is h er
M E D I C A l Jo u r n a l
R h o d e Isla n d Medica l Society
P resi d ent
Cat h e r in e A. C u mmin gs , M D
P resi d ent - e l ect
E l i z ab e t h B. La n ge, MD
V ice presi d ent
T h o m as A. Bleds oe, MD C ase ReportS
S ecretary 37 Retinopathy in a Full-Term Infant with Cri-du-Chat Syndrome
K a r a S tavr os, MD
Nisarg Chhaya, MD; Tineke Chan, MD
T reas u rer
K wa m e D a pa a h -Afriy ie, MD, M BA
40 Iatrogenic Pneumothorax and Pneumomediastinum
E x ec u tive Director
N e w e l l E. Wa rde, Ph D
in a Patient with COVID-19
Vijairam Selvaraj, MD; Kwame Dapaah-Afriyie, MD
E d itors - in - C h ie f
W i l l i am Bin der, MD
Ed wa rd Feller, MD
C ontri b u tion S
A ssociate e d itor
K e n n e t h S. K orr, MD
42 Childhood Overweight/Obesity and the Physical Activity
E d itor - in - C h ie f E merit u s
Environment in Rhode Island
J o s e p h H. Friedma n , MD Shelby Flanagan, MPH; Michelle L. Rogers, PhD; Lynn Carlson, MA,
GISP; Elissa Jelalian, PhD; Patrick M. Vivier, MD, PhD
P u bl ication S taf f
47 Lowering A1c Through Integrated Behavioral Health Group Visits
M anaging e d itor
M ary Korr Siddharth Marthi, BA, MD’22; Jamie Handy;
m k o r r @ r i med.o rg Kristin David, PsyD; Martin Kerzer, DO
G rap h ic d esigner
51 Treatment Retention in Older Versus Younger Adults
M ar i an n e Migliori
A d vertising A d ministrator
with Opioid Use Disorder: A Retrospective Cohort Analysis
D UL CINEIA C OSME from a Large Single Center Treatment Program
d c o sm e @ ri med.o rg
Alyssa Greenwood Francis, MPH; Julie Croll, MPH;
Himanshu Vaishnav, MS; Kirsten Langdon, PhD;
Francesca L. Beaudoin, MD, PhD
55 COVID-19 in Pediatric Patients: Observations from the
Initial Phase of the Global Pandemic in Rhode Island
Rebecca A. Levin, MD; Hoi See Tsao, MD; Siraj Amanullah, MD, MPH;
Alicia Genisca, MD; Laura Chapman, MD
61 COVID-19 and Public Interest in Ophthalmic Services
and Conditions
John C. Lin; Lan Jiang, MS; Ingrid U. Scott, MD, MPH;
Paul B. Greenberg, MD, MPH
RH O D E I S L A N D M E D I C A L J O U R N A L
(USPS 464-820), a monthly publication, is P UBLIC HEA LTH
owned and published by the Rhode Island
Medical Society, 405 Promenade Street, Suite
65 Vital Statistics
A, Providence RI 02908, 401-331-3207. All Roseann Giorgianni, Deputy State Registrar
rights reserved. ISSN 2327-2228. Published
articles represent opinions of the authors and
do not necessarily reflect the official policy
of the Rhode Island Medical Society, unless
clearly specified. Advertisements do not im-
ply sponsorship or endorsement by the Rhode
Island Medical Society.
© Copyright 2013–2021, Rhode Island
Medical Society, All rights reserved.
6
Ready for
Tomorrow
Keep moving toward
your goals with HUB.
When you partner with us, you’re at the center
of a vast network of healthcare industry experts
who help practices like yours prepare for the
unexpected with:
ý Medical liability and business insurance to
protect your practice, your reputation and
your assets
ý Employee benefits that help you navigate
change and support your people
ý Personal insurance and wealth management
to help you protect your home and family
For more information about our tailored solutions,
visit, hubinternational.com/rimed
Put our resources to work for you.
Daniel Nissi, LIA 800-649-9111 daniel.nissi@hubinternational.com
Advocacy | Tailored Insurance Solutions | Peace of Mind
C ommentary
Why don’t doctors return phone calls?
Joseph H. Friedman, MD
A ll doctors get called who answer the calls, seen every few months so the effects of
by their patients. Some saving the doctors a lot medication changes aren’t known for
are better than others of time. And since the long periods of time if one relies only
in answering them. My nurses are usually less on the actual face-to-face office meeting.
patients often report that time constrained, they Usually that is sufficient. It is important
their doctors, whether usually spend more time, for patients who are not tolerating med-
PCPs or specialists, according to my patients, ications to report this to their treating
never call them back. My and seem a lot more
daughter, in California, interested, and more
doesn’t get her calls re- empathetic. Other offices One neurologist I know wrote
turned. Another close rel- have computer “portals” a book for patients and made
ative, a physician, herself, in which non-emergency his patients purchase it. When
doesn’t get her calls returned. This is calls are handled throughout the day,
they called, the secretary
such a frequent refrain that I have to probably by nurses or advanced practice
wonder if it is the norm, now, through-
would transmit the questions
providers.
out the U.S. As you might expect, One neurologist I know wrote a and he would instruct the sec-
some patients call more than others. book for patients and made his patients retary to tell the patient what
Most calls are necessary. “This new purchase it. When they called, the sec- chapter to read in his book.
medicine is causing side effects. What retary would transmit the questions
should I do?” “I’m hallucinating.” “My and he would instruct the secretary to
husband is confused. He couldn’t find tell the patient what chapter to read in physician in a timely manner and not
the bathroom last night.” “My wife fell his book. As best I could tell, he was simply show up 4 or 6 months later
down three times today.” “He’s in the not popular with patients, or his staff. and say, “I took one dose and felt lousy
hospital and the doctors won’t listen They felt that he demeaned his patients so I stopped it.” That’s 4 months water
to me about his medication schedule.” by his behavior. This made them feel under the bridge.
The list is endless. And the patients badly for the patients and also felt that Back in the days before Covid ,
often feel helpless. Yet some doctors this behavior reflected poorly on them. when I used to occasionally attend
don’t call back. I am not sure why that And, I suspect (based on limited personal national meetings, one of my colleagues
is. Of course, I assume that most of the experience) that secretaries in medical remarked what a great service I had
explanation is time. We want to get practices where the doctors routinely performed by writing an article that
home at the end of the day. We don’t fail to answer patient calls resent being was widely distributed by the Ameri-
want to call during the day and cause put in the middle. I suspect that the can PD Association. It was an article
waiting patients to be taken late into turnover rate for secretaries in these outlining when PD patients should go
the office. If we schedule time that we practices is high. to the Emergency Room. I pointed out
can’t bill for we lose money. Return calls are crucial in Parkinson’s the common experience of my own
Many offices, particularly academic disease, and probably most disorders, patients, who would feel frustrated by
centers and group practices, have nurses acute and chronic. In PD, patients are their PD acting up. Their medicines
R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 8
C ommentary hadn’t worked all day. The dyskinesias are very important, it was rarely the make the calls. had gotten out of control. Their walking cause of the worsened PD. Obviously, I don’t know why calling patients back was worse than usual. They took their if your doctor doesn’t return calls, you has fallen so out of favor that it appears medication doses too close together may have no choice but to go to the ED. to have become routine, possibly even and were worried. And what happened A study in Manhattan showed that the norm. Perhaps with the introduc- when they went to the ED? They waited PD patients who called frequently tion of telemedicine, with appropriate 3 hours to be seen, had a multitude of generally suffered more from anxiety billing, we doctors won’t feel it such an tests performed, waited another 5 hours than from other PD-related problems. encumbrance and will again consider it for the results to come back and either Some patients call daily with the same part of our routine practice. v the ED doctor then tried to reach me, or problem. What they really want is not the doctor simply told them to go home a cure for the problem, which clearly Author and call their neurologist the next day. wasn’t getting solved, but the reassur- Joseph H. Friedman, MD, is Editor- The message of my article was that if ance that the doctor knows about their in-chief Emeritus of the Rhode Island the problem was related to PD, call the problem, is still there and cares about Medical Journal, Professor and the Chief PD doctor. If it was a medical issue like them. After decades of experience, I still of the Division of Movement Disorders, fever, cough, chest pain, urinary burn- don’t know how to deal with these calls, Department of Neurology at the Alpert ing, then call the PCP or go to the ED. other than to occasionally point out that Medical School of Brown University, ED doctors weren’t neurologists and the problem had been ongoing for a long chief of Butler Hospital’s Movement generally weren’t going to be able to fix time and didn’t sound different this time Disorders Program and first recipient a PD problem, but were adept at dealing than any of the others. This is intended of the Stanley Aronson Chair in Neuro- with general medical conditions such as to be reassuring, but, to be honest, also degenerative Disorders. infections, or chest pain. While these registers a degree of annoyance. But I do R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 9

C ommentary
Gender-based Differences in the Societal Impact
of the COVID-19 Pandemic
Christina Matulis, MD; Mehrnoosh Samaei, MD, MPH; Ghada Bourjeily, MD; Alyson J. M c Gregor, MD, MA
COVID-19 has been referred to as the as an increase in sexual exploitation and resource utilization, such as telephone
‘great equalizer,’ given that anyone can arranged marriages. Subsequently, these
1
hotlines, but decreased use of shelters
be affected by the virus. However, as girls were ostracized upon returning and safe living arrangements.3
the pandemic continues, it has become to school. Implementing unique ways to screen
apparent that sociocultural factors are Unique challenges are also evident and support IPV victims, such as
intricately tied to vulnerability and ill- among boys, particularly in Latin through telehealth, will be essential
ness severity, as well as post-viral com- America, where poverty leading to given the risks to physical and mental
plications. There is evolving evidence work demands and societal stereotypes health associated with IPV.
regarding the influence of biological sex cause boys to disengage at the second-
in COVID-19 susceptibility, pathophys- ary school level.1 It is essential to use Declining Mental Health
iology, and more. Additionally, with lessons from previous emergencies to Disasters are often accompanied by an
physical distancing, patterns of daily enact services to prevent widening of increase in psychopathologies, such as
life have been disrupted and differen- the pre-existing gender gap between PTSD, anxiety, and depression. Early
tial consequences relating to societal children worldwide. data confirms that COVID-19 is no dif-
gender identity have emerged. While ferent, where the prevalence of depres-
not all inclusive, several key sociocul- Intimate Partner Violence sive symptoms in the US is more than 3
tural areas impacted by COVID-19 are Similar to previous emergencies, this times higher than pre-pandemic.4 Those
outlined below. pandemic has coincided with a rise in with reduced access to socio-economic
intimate partner violence (IPV). While resources and stressors such as job loss
Educational Gap IPV affects everyone, globally, the bur- exhibit increased symptoms. Women are
Educational systems have been affected den is borne mostly by women, with more likely than men to have depressive
worldwide by the need for physical dis- 1 in 3 experiencing sexual violence in symptoms both pre- and during the
tancing. It is estimated that 23.8 million their lifetime, according to the World pandemic. Additionally, specific sub-
children that were enrolled in school, 11 Health Organization. Additionally,
2
populations are differentially affected.
million of whom are female, are at risk marginalized communities, such as In Italy, healthcare workers (HCWs)
of dropping out. The implications of
1
those with lower socioeconomic status reported higher rates of depressive and
disrupted education are vast, as many and underrepresented minorities, are post-traumatic stress symptoms (PTSS).
children will be without access to dig- particularly at risk. Female sex and single status were asso-
ital learning resources and appropriate Social distancing has resulted in vic- ciated with higher levels of depression,
nutrition through school lunches. tims being confined to close quarters while female sex and older age were
In many countries, access to education with their abusers and without adequate associated with increased PTSS.5
is already tenuous for girls, and during resources for assistance. Key places for Pregnant women are at particularly
a pandemic many are pressured to stay IPV screening, like shelters and clinics, high risk, with 18–25% experiencing
home to help with housework. During have dramatically decreased, leading anxiety and 18% reporting depression
the Ebola epidemic, there was a rise in to difficulty in accessing resources. during pregnancy pre-pandemic.6 This
teen pregnancies due to reduced acces- Locally, the RI Coalition for Domestic is increased from baseline US charac-
sibility to reproductive resources as well Violence has seen an increase in some teristics, where 8% of the population
R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 10C ommentary
experiences depression and 16% expe- persists, these differences must be Global Leadership
riences generalized anxiety. recognized to prevent worsening of pre- Although women comprise 70% of
Alarmingly, a Canadian study found existing differences in academia. the global health workforce, they con-
that pregnant women experienced stitute only 24% of COVID response
increased psychological stresses com- Cultural Influences on Mortality committees.14 Low representation of
pared to pre-pandemic cohorts, with Thus far, it is established that COVID- women in leadership roles in healthcare
37% reporting depressive symptoms and 19 mortality is reported to be higher in is not new, and not surprisingly, only
57% reporting anxiety. Factors contrib- men, though this may reflect a deeper 3.5% of COVID-19 national task forces
uting to this include isolation, job loss, gender disparity. In Afghanistan, men show gender parity.15 Lack of leadership
and misinformation disseminated from comprise 70% of COVID-19 cases and skills is not an adequate reason for lack
some social and other media platforms. 74% of mortality.9 Is this difference of representation of women in deci-
Examining maternal health across dif- due to females’ biological advantage or sion-making bodies. Female-led coun-
ferent countries is essential, given this rather due to decreased access to care tries (including Iceland, New Zealand,
particularly high-risk group at baseline. and lack of autonomy in healthcare Norway, and Taiwan) had less death per
decision making? Additionally, there capita and lower excess mortality due to
Impacts on Academic Productivity are other deviations from the worldwide COVID-19. Similarly, states governed
Social distancing has caused an inter- trend worth highlighting. According to by females were more successful in
section of household, school, and work the Global Health 50/50 and US Gender/ controlling COVID-19.16 While many
commitments, inevitably affecting Sex COVID data, there are at least eight factors contribute to these correlations,
productivity in academia. Gender dif- countries and nine US states where increased diversity in leadership will
ferences have been previously charac- mortality in females exceeds males.10,11 benefit all.
terized with regard to compensation, Additionally, female HCWs dispro-
tenure, and female representation in the portionately face a higher rate of infec- Conclusion
sciences. Early research suggests that
7
tion and death from COVID-19. This is Various disparities have emerged with
women in academia exhibited decreased partly, but not fully, explained by the the COVID-19 pandemic and recogniz-
productivity during the pandemic. higher percentage of women in health- ing those who are disproportionately
While there was an increase in overall care. Personal Protective Equipment affected by the virus is critical in order
social science-related submissions by (PPE) can effectively lower the risk of to prevent deepening of pre-existing
35% during the first 10 weeks of the infection, but fit testing of respirators inequalities. As the pandemic contin-
pandemic, female academic research demonstrates that pass rates are lower ues, efforts must be made to understand
productivity dropped 13.9% compared in female and Asian HCWs.12 A study risk based on the interaction of sex,
to males. In this analysis, males were
7
showed that female sex was an indepen- gender, race, age, and other social deter-
found to be more productive than dent risk factor for proven or suspected minants of health. Combining available
females, who maintained their baseline COVID-19 infection of HCWs following data with knowledge from previous
productivity, suggesting widening of a intubation.13 The CDC has taken into emergencies can help build more equi-
gendered productivity gap. account the effects of various facial table societies. v
Women consistently authored 20% hairstyles on the functionality of face
of academic papers since 2015, but masks in men, yet has failed to consider Disclaimer
authored only 12% of COVID-19 related the biological differences between male The views and opinions expressed in this
Commentary reflect those of the authors
data. Reasons are likely multifactorial
8
and female facial contours that predis-
alone and not necessarily those of the
and include increased home and teach- pose women to increased infection risk institutions or organizations they are
ing commitments. As the pandemic
8
even with PPE. associated with.
R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 11C ommentary
References Authors
1. UNESCO. Addressing the gender dimensions of COVID-related Christina Matulis, MD, Department of Emergency Medicine,
school closures COVID-19 education response. Issue Note 3.1. Warren Alpert Medical School of Brown University and Rhode
2020 https://unesdoc.unesco.org/ark:/48223/pf0000373379 [Ac- Island Hospital, Providence, RI.
cessed 25 Nov 2020].
Mehrnoosh Samaei, MD, MPH, Division of Sex and Gender in
2. Moreira D, Pinto da Costa, M. The impact of the Covid-19 pan-
Emergency Medicine, Department of Emergency Medicine,
demic in the precipitation of intimate partner violence. Int J
Law Psychiatry. 2020;71:101606. Warren Alpert Medical School of Brown University,
Providence, RI.
3. Zero O, Geary M. COVID-19 and intimate partner violence: a
call to action. R I Med J. 2020;103(5):57-59. Ghada Bourjeily, MD, Department of Medicine, The Miriam
4. Ettman CK, et al. Prevalence of depression symptoms in US Hospital, Warren Alpert Medical School of Brown University,
adults before and during the COVID-19 pandemic. JAMA Netw Providence, RI.
Open. 2020;3(9):e2019686. Alyson J. McGregor, MD, MA, Director, Division of Sex and
5. Di Tella M, Castelli L. Mental healthcare workers during the Gender in Emergency Medicine (SGEM); Director, Sex and
COVID-19 pandemic in Italy. J Eval Clin Pract. 2020;26(6):1583- Gender in Emergency Medicine (SGEM) Fellowship; Associate
1587. Professor of Emergency Medicine, Warren Alpert Medical
6. Lebel C, et al. Elevated depression and anxiety among pregnant School of Brown University, Providence, RI.
individuals. J Affect Disord. 2020; 277:5-13.
7. Cui R, Ding H, Zhu F. Gender inequality in research productivi- Correspondence
ty during the COVID-19 pandemic. SSRN. 2020. Alyson_McGregor@brown.edu
8. Viglione G. Are women publishing less during the pandemic?
Here’s what the data say. Nature. 2020;581(7809):365-6.
9. Gupta AH, Faizi F. ‘Data shows fewer Afghan women than men
get Covid-19. That’s bad news.’ The New York Times, 3 Oct 2020.
https://www.nytimes.com/2020/10/03/world/afghan-women-
men.html / [Accessed 15 Oct 2020].
10. Dataset. Global health 50/50. https://globalhealth5050.org/the-
sex-gender-and-covid-19-project/dataset/[Accessed 10 Dec 2020].
11. US Gender/Sex COVID-19 Data Tracker. Harvard GenderSci Lab
2020. https://www.genderscilab.org/gender-and-sex-in-covid19/
#CaseDeathRatebySex. [Accessed 13 Oct 2020].
12. Regli A, Sommerfield A, von Ungern-Sternberg BS. The role of
fit testing N95/FFP2/FFP3 masks: a narrative review. Anaesthe-
sia. 2021;76(1):91-100.
13. Turner MC, Marshall SD. Can gendered personal protec-
tive equipment design account for high infection rates in fe-
male healthcare workers following intubation? Anaesthesia.
2020:10.1111.
14. ILO. Policy brief: the COVID-19 response: getting gender equal-
ity right for a better future for women at work. 2020, 1-11.
https://www.ilo.org/wcmsp5/groups/public/---dgreports/---gen-
der/documents/publication/wcms_744685.pdf [Accessed 15 Oct
2020].
15. van Daalen KR, et al. Symptoms of a broken system: the gen-
der gaps in COVID-19 decision-making. BMJ Glob Heal.
2020;5(10):e003549.
16. Coscieme L, Fioramonti L, Mortensen LF, Pickett KE, Kubisze-
wski I, Lovins H, et al. Women in power: female leadership
and public health outcomes during the COVID-19 pandemic.
medRxiv. 2020; 2020.07.13.20152397.
R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 12Aetna® is proud to support the members
of the Rhode Island Medical Society.
©2020 Aetna Inc. Aetna.com
2017308KIDNEY Transp lantation
Clinicians’ Update:
Kidney Transplantation in End-Stage Renal Disease (ESRD)
Reginald Gohh, MD
Guest Editor
Kidney transplantation remains the optimal treatment Health, which calls for reform in the organ procurement and
option for the management of end-stage renal disease management system in the United States to significantly
(ESRD), providing a longer life span, a better quality of life, increase the supply of transplantable kidneys, with the goal
and lower healthcare costs compared with long-term dial- of doubling the number of kidneys available for transplant
ysis treatment. Given recent encouraging developments in by 2030. Additionally, the order encouraged the expanded
the field, this issue of the Rhode Island Medical Journal support for living donors through compensation for costs
is devoted to discussing clinical topics in transplantation such as lost wages and child-care expenses.
relevant to the entire medical community. Rhode Island Hospital established its kidney transplant
Ongoing improvements in graft and patient survival in program in 1997 with the goal of providing convenient and
both deceased donor and living donor kidney transplants quality services to our local community. We have since per-
are reported annually. According to the Scientific Registry formed close to 1,500 kidney transplants, of which approx-
of Transplant Recipients (SRTR), the 10-year all-cause graft imately 50% were derived through living donation. This
failure rate declined to 51.6% for deceased donor recipients success has required the active involvement of a wide range
who underwent transplantation in 2006 compared to 57.2% of healthcare specialists in a multidisciplinary approach.
for transplantations performed in 1998. Ten-year death- Our transplant team also emphasizes close consultation and
censored graft failure similarly declined from 33.7% to 26.2% cooperation with referring nephrologists and primary care
during this period. Living donor recipients who underwent physicians of transplant candidates as they progress from the
transplantation in 2006 experienced a 10-year all-cause and initial evaluation to post-operative care and management.
death-censored graft failure of 34.2% and 18%, respectively. We hope this issue of RIMJ will help the Rhode Island med-
These superior outcomes have been attributed to several ical community meet the ongoing challenges for patients
factors, including better organ procurement and preserva- with ESRD seeking successful kidney transplantation.
tion, more effective immunosuppressive medications and
medication regimens and improved selection of both recip-
ients and donors. Equally encouraging is that more trans- Guest Editor
plants are being performed than ever, with the number of Reginald Gohh, MD, Brown Medicine, Division of Nephrology and
donors and transplants performed in 2019 in the United Hypertension; Medical Director, Division of Kidney Transplanta-
States reaching all-time highs, mostly due to increases in tion, Rhode Island Hospital; Professor of Medicine, Alpert Medical
deceased donors. This has resulted in a decline in the num- School of Brown University, Providence, RI.
ber of patients waiting for a kidney transplant for the fourth
Correspondence
year in a row. Nevertheless, the mismatch between organ
Reginald Gohh, MD
need and supply remains severe, with the average wait time
Rhode Island Hospital
to receive an organ offer between 3–5 years at most centers 593 Eddy Street
and even longer in some regions of the country. Ambulatory Patient Center, 921
It is evident that kidney transplantation should be sought Providence, RI 02903
for all medically and psychosocially qualified patients with 401-444-8562
ESRD. Recently, former President Donald Trump signed Fax 401-444-3283
an Executive Order entitled Advancing American Kidney Rgohh@Lifespan.org
R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 14KIDNEY Transp lantation
Frailty and Kidney Transplantation
George Bayliss, MD
A BST RA C T INTRODU C TION
Two significant policy changes, one in the way people Chronic kidney disease is a growing worldwide problem and
are put forward for kidney transplants and the other in one from which the US is not immune. And while a func-
the way in which kidneys are distributed to people on tioning kidney transplant is seen as the ideal and ultimate
the waiting list, make the question of whether some- renal replacement therapy, there is an overall shortage of
one is too frail to receive a transplant all the more rel- organs compared to the number of people on the waiting list.
evant, particularly in Rhode Island. An executive order The number of people waiting for a deceased donor kidney
signed by President Donald Trump1 stresses that efforts has decreased steadily from over 100,000 in 2014 to 92,906
to treat kidney disease need to concentrate on provid- at the start of 2018. Some 33,879 candidates were added to
ing more people with kidney transplants and increasing the list in 2018 while 34,591 were removed from the list.
the number of organs transplanted rather than discard- The ranks of those removed included 14,784 who received a
ed. An effort to decrease waiting times for kidneys in deceased donor kidney transplant and 6,120 who received a
large metropolitan areas2 potentially means that young- living donor transplant. It also included 4,193 who died on
er, more desirable kidneys will be shipped out of New the waitlist and 4,240 who were removed as too sick.3 The
England, leaving longer waiting times and less desirable decline in numbers on the waiting list reflects the effects of
organs for transplantation in our region. The net effect an earlier change in kidney allocation policies to help better
of these changes may mean that potential older or more match survival of the organ with expected survival of the
frail recipients could be faced with accepting kidneys recipient, decrease the number of organs discarded, and that
from older or less desirable donors or spend more time backdated credit for waiting time to when a candidate initi-
on the waiting list and never receive a credible kidney ated dialysis.4
offer. This raises the specter of poor outcomes from mar- In 2019, President Trump signed an executive order that
ginally functioning kidneys transplanted into marginally sought to decrease the number of people receiving in-cen-
functioning recipients or increased rates of death on the ter hemodialysis and increase the number of people getting
waiting list. While organ allocation policies are beyond dialyzed at home and getting kidney transplants. The order
the ability of transplant nephrologists in Rhode Island to envisioned an additional 17,000 kidney transplants.5 More
change, we will need to assess patients more closely for recently, efforts to reduce large disparities in waiting times
signs of frailty and work with referring doctors to reverse around the country have led to changes in the way points
frailty when possible so that patients can take advantage are awarded that are used to determine one’s standing on the
of a kidney transplant even if the organ isn’t ideal. This list when an organ is offered. The net effect of this change is
article will review the concept of frailty; how to asses it that organs that might have stayed in New England, where
in general and in the context of a transplant evaluation; average wait times for a deceased donor kidney are around
the risk of frailty in transplant outcomes and the bene- 5 years, would be transported to regions like New York,
fits of transplant in reversing frailty; whether markers of where wait times are closer to 10 years.6 While the changes
frailty can be improved and whether that improves trans- in kidney allocation will reduce waiting times in some
plant outcomes. regions, waiting times will increase in regions that become
K E YWORDS: kidney transplant, chronic kidney disease, net exporters of kidneys. These changes raise the possibility
frailty assessment, donor waitlists that as older or more frail candidates move on to list, they
will have to wait longer and will receive kidneys offers that
reflect the diminished survival prospects of the recipient, or
risk dying on the list before they are matched with a kidney.
To keep transplantation going in the region will require
more careful evaluation of candidates as well as increased
efforts to improve candidates’ chances of surviving on
the waiting list to receive an organ offer and thrive after
R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 15KIDNEY Transp lantation
transplantation. The concept of frailty plays into this calcu- standardize assessment of frailty in transplant candidates
lus. This paper will review the concept of frailty and address and generate ideas for further research.10 In a survey of AST
ways to assess it in general and as part of the transplant members concerned with kidney transplantation, 98.9%
evaluation. The paper will look briefly at the risk to patient considered frailty in transplant candidates a risk factor for
and transplant outcomes from frailty versus the potential poor outcomes after transplantation, while 93.3% felt the
benefit from transplant toward reversing frailty. The paper need for a frailty score in making decisions on whether to
will examine potential ways to reverse elements of frailty transplant, and 67.1% thought age should be included in
to improve transplant prospects and whether such precondi- assessing frailty. Optimizing dialysis and volume status,
tioning works. The literature is vast, but this review will try nutrition, physical therapy and psychotherapy were thought
to touch briefly on these important concepts. essential components in improving frailty in patients with
kidney disease awaiting transplant in the AST survey.
Much work has gone into looking at individual components
FRAI LT Y of frailty, as well as association of age, comorbidities and
Frailty is often equated with old age or increased comor- frailty. Reviews on measuring frailty cite up to 75 functional
bidities. And while age and illness can factor into frailty, assessment tools available currently, including questionnaires
they are not substitutes for frailty. In their seminal paper on assessing physical capacity, tools like the Karnosky Perfor-
describing a frailty phenotype, Fried and colleagues wrote mance Scale to assess physical performance, tools to quan-
that frailty “may have a biological basis and be a distinct tify perceived frailty like the Fried’s frailty phenotype (FFP),
clinical syndrome”7 and sought to develop a standardized a frailty index of cumulative deficits, physical performance
definition. Using data from the Cardiovascular Health Study, scores like walking speed, grip strength, ability to stand and
they evaluated 5,317 men and women, including 582 Blacks, balance, involuntary loss of muscle mass (sarcopenia), cardio-
from 4 to 7 years of follow-up. They defined frailty as a clin- pulmonary fitness testing to assess oxygen utilization.11
ical syndrome based on three or more of five characteristics: In a recent survey of US kidney transplant programs,
unintentional weight loss of 10 pounds or more in the previ- McAdams-DeMarco and colleagues found the bulk of pro-
ous year (shrinkage), self-reported exhaustion, weakness on grams that responded to the survey (133/202) considered
a test of grip strength, slow walking speed over a set dis- frailty a clinically relevant concept (99.2%) but only 96%
tance and low physical activity as defined on a standardized said they thought frailty should be used in making decisions
questionnaire.8 In their study, frailty was associated with about whether someone was a transplant candidate. The
increased age, female gender, Black race, having a lower level survey found great heterogeneity in assessing frailty with
of education and income, poorer health, and higher rates of respondents reporting that they used some 18 different tools
chronic comorbid diseases and disability. They found that to assess it. The most used test – by 19% of respondents –
the frailty phenotype independently predicted falls, wors- was a timed walk. Some 8% of respondents used the FFP
ening mobility, hospitalization and death over three years. while 8% used the Montreal Cognitive Assessment and 8%
They defined intermediate frailty as having one or two of the also used sarcopenia. Two-thirds of respondents said they
characteristics, signaling an increased risk of becoming frail used more than one test.12
over 3–4 years. They defined frailty as a downwardly spiral- Without a standardized method to assess frailty, clinicians
ing physiologic process of declining energy utilization and often fall back on perceptions of frailty, which can be deceiv-
“loss of homeostatic capability to withstand stressors and ing, with the consequence of potentially denying access to
resulting vulnerabilities.” While they noted some overlap transplantation among those perceived as frail. Salter and
with disability and illness, they stressed that those concepts colleagues looked at differences in perceived and measured
are not synonymous with frailty. frailty in 146 adults undergoing hemodialysis at a single
dialysis unit in Baltimore.13 Patient characteristics of frailty
as perceived by nurse practitioners, nephrologists or patients
NEE D T O A S S E S S F R AI LT Y were compared with measured assessment of frailty using
There is a clear consensus, however, that frailty is a com- the FFP. Older age and comorbidities were associated with a
mon feature of people with end-stage organ damage await- greater likelihood of being perceived as frail by nephrologists
ing a transplant. The data also bear this out. According to while women and non-African Americans were more likely
a national study pooling data from three major centers, an perceived as frail by nurse practitioners. At the same time,
estimated 16.4% of all kidney transplant candidates were of patients classified by the FFP as frail, only 42% were per-
considered frail between 2008 and 2018 while 14.3% of all ceived as frail by nephrologists, 39.2% by NPs and 4.9% by
kidney transplant recipients were considered frail during the patients themselves. The risk, according to the authors, was
same time.9 that older dialysis patients and women perceived as frail but
The American Society of Transplantation (AST) spon- not actually demonstrating frailty risked not being listed for
sored a consensus conference on frailty in February 2018 to transplantation.
R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 16KIDNEY Transp lantation
And yet for frail patients, the risk of not being listed is identified what they described as high-risk kidney trans-
significantly higher. In study of 7,078 transplant candidates plant patients (59 years or older, diabetes and or more than
between 2009–2018, frail patients were 38% less likely to be three years on dialysis) and evaluated them using the FFP
listed for transplant, regardless of age or other demographic and Short Physical Performance Battery. They found that
factors. Frail Black kidney transplant candidates were 46% both frailty and physical performance were significantly
less likely to be listed than non-frail, non-Black candidates. associated with death on the waiting list (hazard ratio 6.7,
They were 32% less likely to be transplanted compared to 95% confidence interval 1.5–30.1; P=0.01). They also found
non-frail patients and they were 70% more likely to die on that the relationship between frailty, physical performance
the waiting list.14 score and death on the waiting list were independent of age,
The relationship between aging, frailty and chronic kid- diabetes or length of time of dialysis.19
ney disease is central since aging increases the risk of poor Time on the waiting list can also increase frailty, such that
outcomes from the cumulative burden of correlates for some suggest measuring changes in frailty over the course
frailty like cognitive impairment, poly-pharmacy, disability, of time between listing and transplantation. Researchers
multiple comorbidities, malnutrition, and dialysis.15 In the at Johns Hopkins noted that 22% of 569 kidney transplant
Rhode Island experience, the relationship between age and candidates enrolled in their cohort study of frailty became
loss of kidney transplant and death after transplant was sig- increasingly frail while 24% became less so. While Black
nificant in patients who were inactive, smoked, had COPD, race was associated with becoming less frail and diabetes
had peripheral vascular disease or required dialysis within a was associated with remaining stably frail, the longer can-
week after transplantation (delayed graft function).16 didates remained on dialysis, the less likely they were to
Age alone does not seem to define frailty in patients become less frail. Given the dynamic change in frailty in
undergoing dialysis and transplantation and as a single some patients, these researchers recommended assessing
entity, does not portend poorer outcomes. Researchers at frailty at the time of listing and time of transplantation
Johns Hopkins, the University of Michigan and the Uni- since candidates who became more frail faced longer hos-
versity of California, San Francisco, pooled cohorts to com- pitalization times post-transplant as well as a higher risk of
pare frailty in subjects older than 65 and younger than 65 mortality post-transplant.20 Researchers at Columbia Uni-
at three time points: within six months of starting dialysis; versity used a timed “get up and go” test for patients on
at time of kidney transplant evaluation; at time of admis- the waiting list to see if that might predict outcomes after
sion for kidney transplant. Overall, frailty in all three time transplant. In the end, participants in the study who were
points was more prevalent in older patients who were also transplanted had shorter times on the test than those who
more likely to have slowness and weakness. Younger sub- remained on the waitlist. However, there was no associa-
jects were more likely to experience exhaustion in all three tion between test time and probability of removal from the
time points. The authors concluded that while frailty was waitlist or prolonged hospitalization after transplantation or
more prevalent in older subjects, younger subjects still had a 30-day readmissions.21
high burden.17 A registry-based study at Oslo Hospital of all In an ongoing trial, a group of Canadian researchers hopes
potential kidney transplant recipients age 65 or older who to better evaluate whether frailty is associated with death on
received a deceased donor kidney transplant between 2000 the waitlist, withdrawal from the waitlist as well as whether
and 2014 found no difference in outcomes between those frailty is associated with hospitalization, quality of life and
who received a first kidney and those who received a sec- even being listed. Their plan is to evaluate potential can-
ond kidney re-transplant. Five-year survival censored for didates using the FFP, the frailty index, the Short Physical
death with a functioning graft in those receiving a second Performance Battery and the Clinical Frailty Scale (CFS) at
transplant was 88% versus 90% for those receiving a first the time of initial evaluation for listing and annually after
transplant (P = 0.475%).18 Risk factors for increased chance that. The goal is to understand the association of frailty and
of death with a functioning graft also included longer time outcomes from patient on the waitlist before incorporating
on the waiting list before re-transplantation, although the measurement of frailty into the regular waitlist workup.22
authors noted that overall waiting time at their center was The association between waitlist mortality and frailty
small such that their findings might be even more applicable is not clear. The CFS, a validated instrument in dialysis
at centers with longer waiting times. patients, uses overall clinical impression to award a single
point for each degree of perceived frailty. In a cohort of inci-
dent dialysis patients assessed between 2009 and 2013, each
FRAI LT Y WH I L E WAI T I NG point increase in the CFS was associated with an increase
The risk of death on the waiting list for frail patients has led in the hazard ratio of death (HR 1.22; 95% CI, 1.04–1.43;
to much thought about whether chances to receive a kidney P=0.02).23 In a separate multi-center study, researchers
can be enhanced by “preconditioning” of frail candidates to assessed whether an association existed between frailty on
improve physical stamina. Researchers at the Mayo Clinic the waitlist and accumulated burden of comorbidities as
R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 17KIDNEY Transp lantation
assessed by the Charlson Comorbidity Index. In a study of FRA ILTY A FTER TRA NSP LA NT
2,086 candidates on the kidney transplant waitlist, 18.1% Does transplantation improve frailty among kidney recipi-
were frail and 51% had a high comorbidity burden. They ents? Again, the data appear mixed. Researchers in the Neth-
found that among non-frail patients, a high comorbidity erlands studied 176 kidney transplant recipients at their
score was associated with a statistically significant risk center in Groningen between 2015 and 2017 and followed
of mortality (HR 1.66 95% CI 1.17–2.35). But among frail for up to three years. Using their own frailty scale (Gronin-
patients, high burden of comorbid conditions did not show gen Frailty Indicator), they found that 34 non-frail patients
an association with mortality. Stratified by age, the higher became frail after transplantation, 125 patients remained
comorbidity index portended worse mortality in patients unchanged, and 19 frail patients were no longer frail. The GFI
waiting for kidney transplantation who were under 65, while includes 15 questions in eight functional domains including
a high burden of comorbidities was not associated with wait- mobility, vision, hearing, nutrition, comorbidities, cogni-
list mortality in patients age 65 and greater on the waitlist.24 tion, psychosocial functioning and physical fitness. Changes
in cognition and psychosocial functioning contributed most
to the shift from not frail to frail after transplantation.29 In
INTERVEN T I O N S contrast, researchers at Johns Hopkins and the University of
The question then becomes whether one can intervene with Michigan assessed frailty using the FFP and then examined
frail candidates to improve their survival on the waitlist, changes in health-related quality of life (HRQOL) in 443 kid-
their chances of getting a kidney and survival after trans- ney transplant patients at their centers between 2014 and
plantation. Part of the problem in increasing exercise tol- 2017 for three months post-transplant. At the time of trans-
erance among kidney transplant candidates is that people plant, frail patients had worse HRQOL scores than non-frail
enter the waitlist already in poor physical shape. According patients, but both groups showed improvement one month
to one study, 95% of new starts on dialysis have physical post-transplant. At three months, frail transplant recipi-
fitness levels below the 20th percentile for the general popu- ents had statistically significant continued improvement in
lation, and just over half (56.4%) are able to walk one block, physical HRQOL but non-frail patents did not. The same
23.8% can climb 24 stairs, and only 18.5% said they could held true for changes in mental HRQOL. Both frail and non-
walk a mile.25 Researchers at several centers are looking frail transplant recipients reported improvement in kidney
into adapting an exercise module developed by the Ameri- disease specific HRQOL.30
can College of Sports Medicine to create an exercise module
for people transitioning to dialysis. The idea is to develop a
practical and cost-effective package to help patients starting C ONC LU SION
dialysis overcome barriers to exercise.26 The topic of frailty in chronic kidney disease and transplan-
Researchers at the Mayo Clinic used supervised exercise tation remains in flux. The transplant community knows
sessions in frail patients with stage IV chronic kidney disease that frailty is a poor indicator for outcomes in transplan-
or greater to see whether their intervention could improve tation. Frailty can affect not only if patient can get trans-
strength. They enrolled 21 patients in two supervised out- planted once placed on the waitlist but also whether that
patient exercise sessions per week for eight weeks. The person can even get on the list to begin with. As older peo-
intervention, which included strength, endurance and flexi- ple undergo transplant evaluation and face the prospect of
bility training, led to improvement in frailty parameters like only getting offers of kidneys from more marginal donors,
walk speed, grip strength and fatigue, although none of the assessing candidates for frailty and finding ways to reverse
changes were statistically significant. Scores on the Short the components of frailty that are amenable to improvement
Physical Performance Battery did improve significantly. The becomes all the more important. However, the transplant
authors suggest that their results are encouraging and war- community remains divided on the best tool(s) to use to
rant evaluation in a larger, multi-site study.27 make the assessment and whether exercise conditioning can
The transplant clinic at Stanford University began doing help give people more strength, stamina and improve energy
physical assessments of transplant candidates once their metabolism. The Organ Procurement and Transplantation
accumulated waiting time put them in the top of the center’s Network (OPTN) has temporarily put on hold the imple-
waitlist. Rather than assessing frailty, the clinic assessed 60 mentation of changes in the kidney allocation system while
second sit-to-stand and 6-minute walk tests. They found the Department of Health and Human Services reviews
that the lower the scores on the two tests, the higher risk of concerns about the changes that were submitted just before
removal from the waitlist or death on the waitlist.28 the new rules were due to take effect December 15, 2020.
Whatever the outcome of that review, efforts to improve a
transplant candidate’s conditioning and stamina could also
be important tools in improving access to and survival after
kidney transplantation.
R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 18KIDNEY Transp lantation
References 20. Chu NM, Deng A, Ying H, et al. Dynamic frailty before kidney
1. Executive Order on Advancing American Kidney Health. 10 transplantation: time of measurement matters. Transplanta-
July 2019. www.whitehouse.gov. (25 December 2020, date last tion. 2019;103:1700-1704.
accessed). 21. Michelson AT, Tsapepas DS, Husain SA, et al. Association
2. Organ Procurement and Transplantation Network. Kidney Al- between the “timed up and go test” at transplant evaluation
location System. http://optn.transplant.hrsa.gov. (25 December and outcomes after kidney transplantation. Clin Transplant.
2020, date last accessed). 2018;32:e13410. doi: 10.1111/ctr.13410.
3. Hart A, Smith JM, Skeans MA, et al. OPTN/SRTR 2018 Annual 22. Tennankore KK, Gunaratnam L, Suri RS, et al. Frailty and
Data Report: Kidney. Am J Transplant. 2020 Jan; 20 Suppl s1: the kidney transplant waitlist: protocol for a multicenter
20-130. doi: 10.1111/ajt.15672. prospective study. Can J Kidney Health Dis. 2020 Sep
4. Israni AK, Salkowski N, Gustafson S, et al. New allocation poli- 10;7:2054358120957430. doi: 10.1177/2054358120957430.
cy for deceased donor kidneys in the United States and possible 23. Alfaadhel TA, Soroka SD, Kiberd BA, Landry D, Moorhouse P,
effect on patient outcomes. J Am Soc Nephrol. 2014:251842- Tennankore KK. Frailty and mortality in dialysis: evaluation of
1848. a clinical frailty scale. Clin J Am Soc Nephrol. 2015;10:832-40.
5. Remarks by President Trump at signing Executive Order on 24. Perez Fernandez M, Martinez Miguel P, Yinh H, et al. Comor-
Advancing American Kidney Health. 10 July 2019. www.white- bidity, frailty and waitlist mortality among kidney transplant
house.gov. (25 December 2020, date last accessed) candidates of all ages. Am J Nephrol. 2019;49:103-110.
6. Organ Procurement and Transplantation Network. Eliminate 25. Johansen KL, Chertow GM, Kutner NG, et al. Low level of
the use of DSA and region from kidney allocation policy. 3 De- self-reported physical activity in ambulatory patients new to
cember 2019. http://optn.transplant.hrsa.gov. (25 December dialysis. Kidney Int. 2010;78:1164-1170.
2020, date last accessed). 26. Jagannathan R, Ziolkowski SL, Weber MB, et al. Physical ac-
7. Fried LP, Tangen CM, Walston J et al. Frailty in older adults: tivity promotion for patients transitioning to dialysis using the
evidence for a phenotype. J Gerontol A Biol Sci Med Sci. “Exercise is Medicine” framework: a multi-center randomized
2001;56:M46-M156. pragmatic trial (EIM-CKD trial) protocol. BMC Nephrology.
8. Taylor HL, Jacobs DR Jr., Schucker B, et al. A questionnaire for 2018 Sep 12;19:230. doi: 10.1186/s12882-018-1032-0.
the assessment of leisure time physical activities. J Chron Dis. 27. Lorenz EC, Hickson LJ, Weatherly RM, et al. Protocolized ex-
1978;31:741-755. ercise improves frailty parameters and lower extremity impair-
9. Haugen CE, Thomas AG, Chu NM, et al. Prevalence of frailty ment: a promising rehabilitation strategy for kidney transplant
among kidney transplant candidates and recipients in the Unit- candidates. Clin Transplant. 2020 Sep;34:e14017. doi: 10.1111/
ed States: estimates from a national registry and multicenter ctr14017.
cohort study. Am J Transplant. 2020:20:1170-1180. 28. Cheng XS, Myers J, Han J, et al. Physical performance testing
10. Kobashigawa J, Dadhania D, Bhorade S, et al. Report from the in kidney transplant candidates at the top of the waitlist. Am J
American Society of Transplantation on frailty in solid organ Kidney Dis. 2020. doi: 10.1053/j.ajkd.2020.04.009.
transplantation. Am J Transplant. 2019;19:984-994. 29. Quint E, Schopmeyer L, Banning LBD, et al. Transitions in frail-
11. Basu A. Role of physical performance assessments and need for ty state after kidney transplantation. Langenbecks Arch Surg.
a standardized protocol of selection of older kidney transplant 2020;405:843-850.
candidates. Kidney Int Rep. 2019;4:1666-1676 30. McAdams-DeMarco M, Olorundare IO, Ying H, et al. Frailty and
12. McAdams-DeMArco MA, Van Pilsum Rassmussen SA, Chu postkidney transplant health-related quality of life. Transplant.
NM, et al. Perceptions and practices regarding frailty in kidney 2018;102:291-299.
transplantation: results of a national survey. Transplantation.
2020;104:349-356. Author
13. Salter ML, Gupta N, Massie AB, et al. Perceived frailty and mea- George Bayliss, MD, Division of Organ Transplantation, Rhode
sured frailty among adults undergoing hemodialysis: a cross-sec- Island Hospital, Providence, RI; Division of Kidney Diseases and
tional analysis. BMC Geriatrics. 2015 Apr 2415:52. doi: 10.1186/
Hypertension, Brown Medicine, E. Providence, RI; Alpert Medical
s12877-015-0051-y.
School of Brown University, Providence, RI.
14. Haugen CJ, Chu NM, Ying H, et al. Frailty and access to kidney
transplantation. Clin J Am Soc Nephrol. 2019;14:576-582.
Financial disclosures
15. Harhay MN, Rao MK, Woodside KJ, et al. An overview of
frailty in kidney transplantation: measurement, management None
and future considerations. Nephrol Dial Transplant. 2020;35:
1099-1112. Correspondence
16. Yango AF, Gohh RY, Monaco AP, et al. Excess risk of renal al- George Bayliss, MD
lograft loss and early mortality among elderly recipients is as- Division of Organ Transplantation
sociated with poor exercise capacity. Clin Nephrol. 2006;65: 593 Eddy Street
401-407. Ambulatory Patient Center, Floor 9
17. Chu NM, Chen X, Norman SP, et al. Frailty prevalence on Providence, RI 02903
younger end-stage kidney disease patients undergoing dialysis
and transplantation. Am J Nephrol. 2020;51:501-510. United States
18. Heldal K, Hartmann A, Lønning K, et al. Should patients older 401-444-8562
than 65 years be offered a second kidney transplant? BMC Ne- Fax 401-444-3283
phrology. 2017;18:13 doi: 10.1186/s12882-016-0426-0. gbayliss@lifespan.org
19. Lorenz EC, Cosio FG, Bernard SL, et al. The relationship be-
tween frailty and decreased physical performance with death
on the kidney transplant waiting list. Prog Transplant. 2019;29:
108-114.
R I M J Arc h i v e s | F e br u a r y I S S UE W e bp a g e | R I M S February 2021 Rhode isl and m edical journal 19You can also read