Magnetic Resonance Imaging Contrast Enhancement of Brain Tumors at 3 Tesla Versus 1.5 Tesla
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
INVESTIGATIVE RADIOLOGY
Volume 37, Number 3, 114 –119
©2002, Lippincott Williams & Wilkins, Inc.
Magnetic Resonance Imaging Contrast Enhancement of Brain
Tumors at 3 Tesla Versus 1.5 Tesla
IRIS-MELANIE NÖBAUER-HUHMANN, MD,* AHMED BA-SSALAMAH, MD,* VLADIMIR MLYNARIK, PHD,*
MARKUS BARTH, PHD,* ALEXANDER SCHÖGGL, MD,† KARL HEIMBERGER, MD,* CHRISTIAN MATULA, MD,†
AMURA FOG, MD,§ ALEXANDRA KAIDER, MSC,‡ AND SIEGFRIED TRATTNIG, MD*
Nöbauer-Huhmann IM, Ba-Ssalamah A, Mlynarik V, et al. ITHIN THE past few decades, contrast-enhanced MRI
Magnetic Resonance Imaging Contrast Enhancement of Brain
Tumors at 3 Tesla Versus 1.5 Tesla. Invest Radiol
W has become the method of choice for visualization of
most abnormalities of the brain. The intravenous adminis-
2002;37:114 –119.
tration of gadolinium-DTPA for contrast-enhanced images
RATIONALE AND OBJECTIVES. To compare the diagnostic
efficacy of a standard dose of MRI contrast agent in the
has proved to be valuable in the evaluation of primary brain
evaluation of primary brain tumors and metastases using a tumors and metastases.1,2 Most of these tumors enhance
high-field 3 tesla MR unit versus a 1.5 tesla MR unit. with the use of contrast agents, with improved tumor delin-
METHODS. Sixteen patients with brain tumors were exam- eation and evaluation of internal tumor structure. An intra-
ined at both field strengths using identical axial T1-SE proto- venous dose of 0.1 mmol/kg has been established as the
cols pre- and postcontrast (0.1 mmol/kg gadolinium), and post-
contrast coronal 3D GRE with magnetization preparation
optimum dose on routine scanners.3,4 A recent study proved
(MP-RAGE), which was adjusted separately for each field that a higher dose is required for low field MRI scanners
strength. Evaluation of the images was performed quantita- such as 0.2 tesla.5 The strength of the static magnetic field
tively and, in the case of T1-SE images, also by visual ranges from 0.5 tesla to 1.5 tesla on routine clinical MR
assessment. scanners.
RESULTS. Tumor-to-brain-contrast after gadolinium admin-
istration using statistical evaluation of MP-RAGE scans was
Currently, clinical MR-scanners operating at a magnetic
significantly higher at 3 tesla (97.5) than at 1.5 tesla (46.3). The field of 3 tesla are offered by all major manufacturers (eg,
same was true for T1-SE sequences (93.0 vs. 72.1). Signal General Electrics, Philips, Bruker-Siemens and Marconi).
enhancement of the lesions in T1-SE sequences was not signif- With the development of high-field MRI scanners, spatial
icantly different between both field strengths. resolution and SNR can be improved significantly.6 The
CONCLUSIONS. Administration of a gadolinium contrast
agent produces higher contrast between tumor and normal
increasing availability of such instruments in the near future
brain at 3 tesla than at 1.5 tesla. raises the question of whether higher field scanners will
KEY WORDS. 3 tesla MRI; high field strength; gadolinium; improve the clinical evaluation of intracranial tumors after
MRI contrast agent; brain tumors. administration of contrast agents.
The magnetic field dependence of contrast enhancement
in tumors was addressed in several studies. In some of these
From the *Department of Radiology, †Department of Neurosurgery, and studies7,8 no difference in relative signal enhancement of the
‡Department of Medical Computer Sciences, University Clinic of Vienna,
Austria. lesions was found at different field strengths up to 1.5 tesla.
§From the Medical and professional Services Europe/International, Ny- However, other authors9,10 reported an increase in tumor-
comed-Amersham, Oslo, Norway. to-brain contrast at higher field strengths.
Supported by a research grant from Nycomed-Amersham, Oslo,
Norway. To our knowledge, no study has yet presented an exam-
Reprint requests to: Dr. Iris-Melanie Nöbauer-Huhmann, Klinik für ination of the intravenous administration of MRI contrast
Radiodiagnostik, Universitätsklinik Wien, Währinger Gürtel 18-20, a-1090 agents in the evaluation of primary brain tumors or metas-
Wien
Received July 14, 2001, and accepted for publication, after revision, tases at a field strength of 3 tesla, and no studies have been
November 25, 2001. published comparing contrast enhancement on 3 tesla MRI
114No. 3 MRI CONTRAST ENHANCEMENT AT 3TESLA 䡠 Nöbauer-Huhmann et al 115
images with conventional 1.5 tesla MRI images despite the scanners: axial T1-SE pre- and postcontrast (TR/TE ⫽
fact that 3 tesla MR units will become routine scanners in 650/14 milliseconds, 6 mm slice thickness, field of view
the near future. The present study was designed to evaluate [FOV] of 230 mm, matrix size of 256 ⫻ 256, 1 acquisition,
tumor enhancement and diagnostic efficacy of a standard and L-R phase encoding). The scan time of 2:15 minutes
dose of MRI contrast agent at 3 tesla relative to 1.5 tesla. was the same on both scanners. At 1.5 tesla, a contrast-
enhanced T1-weighted 3D-gradient echo sequence was used
Materials and Methods with magnetization preparation (MP-RAGE; TR/TE/TI ⫽
Patients 9.7/4/300 milliseconds; flip angle 12°; 1.56 mm apparent
A total of 16 consecutive patients were prospectively slice thickness; FOV of 230 mm; matrix size of 256 ⫻ 256;
examined after obtaining approval from the institutional one acquisition; L-R phase encoding) in the coronal orien-
ethics committee. Patients were included if they had a tation and a scan time of 4 minutes. The parameters for the
known primary brain tumor or metastases and were being MP-RAGE on the 3 tesla MR unit were: TR/TE/TI ⫽
scheduled for surgery or ␥-knife therapy. All patients were 24.9/5/800 milliseconds; flip angle 15°; apparent slice thick-
adults (age older than 19 years) and stable (patients with ness of 1.9 mm; matrix size of 256 ⫻ 192; FOV 210 mm;
severe space-occupying lesions were excluded so as not to 1 acquisition; and a scan time of 9 minutes. Established
delay therapy) without known contraindication against the imaging protocols for the 1.5 tesla unit also included axial
intravenous administration of gadolinium contrast agents or FLAIR-TSE and axial T2-weighted TSE images.
MRI examination. All patients gave written informed Qualitative assessment was performed for T1 sequences
consent. only, as the parameters for MP-RAGE differed in a way that
One patient had to be excluded because of technical might influence the perception of the readers. The images
problems with contrast agent administration. The ages of from both examinations were printed on films with field
the remaining 15 patients (9 men and 6 women) ranged strength and the name of the patient masked. Window
from 37 to 77 years (mean, 57 years). Regarding tumor settings were adjusted to minimize visual contrast differ-
histology, meningioma was found in seven patients, metas- ences in brain tissue between the two sets of images. The
tases in four patients, malignant glioma (two patients grade images were analyzed prospectively by three independent
IV- glioblastoma, one patient low-grade astrocytoma) in radiologists. This visual assessment was performed first to
three patients, and schwannoma in one patient. A subgroup ensure that the investigators had not seen the cases previ-
of patients with homogeneously enhancing tumors consisted ously. The following parameters were requested: (1) the
of nine patients (four men and five women; age range: visibility; (2) the delineation of the lesion; (3) the “contrast
41–77 years, mean: 56 years). Patient monitoring included enhancement” of the lesion, meaning the impression of the
past medical history, physical examination, and laboratory amount of enhancement of the tumor; (4) The “gray-white
tests. differentiation,” meaning the ability to discriminate be-
tween normal gray and white matter; and, finally, (5) the
Protocol subjective overall “diagnostic usefulness” as a general mea-
The images were acquired on a 3 tesla MR scanner sure of diagnostic value regarding the specific case was
Medspec 30/80 (Bruker, Ettlingen, Germany) using a head asked. All these factors were rated as 0 (non-existent), 1
birdcage transmit/receive coil and an actively shielded gra- (poor), 2 (acceptable, ie, good enough to be used), 3 (good,
dient system with a maximum gradient strength of 45mT/m. ie, satisfying), or 4 (excellent). Artifacts including motion,
On the 1.5 tesla MR unit (Siemens Vision; Siemens Medical susceptibility, other artifacts (eg, pulsation or ringing), and
Systems, Erlangen, Germany), a standard circular-polarized subjective image noise were graded as 1 (absent), 2 (mild),
head coil and a maximum gradient strength of 23mT/m was 3 (moderate), or 4 (severe).
used. At 1.5 tesla, a low-level raw data filter was routinely In image sets for which different grades had been chosen
applied. by the three radiologists, mean values were calculated for
All patients were examined in random order on both units final classification. Quantitative image assessment was per-
before and after administration of contrast agent. The ex- formed subsequently. Signal intensities of individual types
aminations were performed separately on both MR scanners of tissue and lesions were assessed by region of interest
with a time interval of at least 3 days. The contrast agent (ROI) measurements with ROI values placed identically on
used was gadodiamide, (Omniscan; Nycomed-Amersham, both series of images using the same sized circular ROI
Oslo, Norway). In all patients the typical dose of 0.1 from the software available on both scanners. Patients with
mmol/kg (0.2 mL/kg body weight) was administered intra- contrast enhancement limited to the periphery in a small,
venously as a bolus with a standard delay (10 minutes) rim-like fashion had to be excluded from quantitative image
between intravenous administration of gadodiamide and assessment, as the enhanced areas were too small to place
data acquisition. ROI values for reliable measurement. In total, nine patients
MR imaging included the following sequences on both could be evaluated quantitatively. In those patients, lesion-116 INVESTIGATIVE RADIOLOGY March 2002 Vol. 37
TABLE 1. Qualitative Assessment
Sequence 1.5 T 3T p3
Visibility of the lesion* T1 pre1 2 1.7 ⬍.05
T1 post2 4 3.7 n.s.
Delineation of the lesion* T1 pre1 2 1.7 n.s.
T1 post2 3.7 3.7 n.s.
Contrast agent enhancement of the lesion* T1 post2 3.7 4 n.s.
Gray-white differentiation of the normal brain* T1 pre1 2.3 2 ⬍.05
T1 post2 2.3 1.7 ⬍.05
Diagnostic usefulness* T1 pre1 2.3 1.7 n.s.
T1 post2 3.7 3.7 n.s.
Motion artifacts† T1 pre1 1.0 1.1 n.s.
T1 post2 1.1 1.2 n.s.
Susceptibility artifacts† T1 pre1 1.0 1.3 ⬍.05
T1 post2 1.0 1.3 ⬍.05
Other artifacts† T1 pre1 1.5 2.1 ⬍.05
T1 post2 2.1 2.4 ⬍.05
Image noise† T1 pre1 1.1 2.1 ⬍.05
T1 post2 1.2 2.1 ⬍.05
* Median values of visual assessment criteria in all patients at 1.5 T and 3T. on a scale of 0 (non-existent), 1 (poor), 2 (acceptable), 3 (good),
or 4 (excellent).
† Artifacts and subjective image noise on a scale of 1 (absent), 2 (mild), 3 (moderate), or 4 (severe).
1
T1 before and 2T1 after contrast agent administration. 3statistical significance of the differences.
to-brain-contrast and signal enhancement for the lesion paired t test was used to compare the tumor-to-brain con-
were evaluated as follows. trast and the signal enhancement between 3.0 tesla and 1.5
Numerical preinjection tumor/brain-contrast (RL0,B0) is de- tesla. The paired Wilcoxon signed rank test was used to
fined as compare the qualitative scores (visibility, delineation, and
contrast enhancement of the lesion, gray-white differentia-
SL0⫺SB0
SB0 䡠 100,
RL0,B0 [%]⫽ 8 tion, and overall diagnostic usefulness) and the respective P
values were corrected for the number of multiple compari-
with SL0 taken as the signal intensity of an ROI assessed sons using the Bonferroni-Holm method.11 For all tests,
over a lesion before contrast agent administration and SB0 significance was set at P ⬍ 0.05, and the SAS software was
taken as the signal intensities assessed over the contralateral used for statistical analyses.12
white matter. Numerical tumor-to-brain-contrast after gad-
olinium administration (RL,B) is defined as Results
SL⫺SB Qualitative assessment was performed in all patients. The
RL,B [%]⫽ S 䡠 100,8 results of visual assessment are summarized in Table 1.
B
In contrast-enhanced T1-SE, the visibility of the lesion
with SL taken as the signal intensity of an ROI assessed over was considered to be adequate in all patients. The delinea-
a lesion after contrast agent administration and SB taken as tion of the lesion in contrast-enhanced T1-SE was less than
the signal intensities assessed over the contralateral white “acceptable” in none of the cases at 1.5 tesla and in one case
matter. The signal intensity of a lesion was measured within at 3 tesla. For lesion delineation and visibility, the ratings in
an enhanced area. In inhomogeneously enhanced tumors, the postcontrast series were not significantly different,
the area of maximum uptake was chosen for measurement. whereas the plain T1-SE was considered better at 1.5 tesla
Signal enhancement of the lesion (EL) is defined as
than at 3 tesla for both parameters. The subjective impres-
SL⫺SL0 sion of contrast enhancement of the lesion did not differ
(EL [%]⫽ S 䡠 100,8 significantly with 3 tesla versus 1.5 tesla. The gray-white
L0
differentiation of T1-SE pre- and postcontrast series was
with SL0 taken as the signal intensity of an ROI assessed
significantly better with 1.5 tesla than with 3 tesla. Overall
over a lesion before, and SL taken as the signal intensity of
diagnostic usefulness was not significantly different for
an ROI assessed over a lesion after gadolinium administra-
either of the field strengths.
tion, respectively.
Motion artifacts did not differ in any of the series with
Statistical Analysis either scanner. Susceptibility and other artifacts (pulsation-
The signal intensity values in the quantitative measure- and ringing-artifacts were observed) were subjectively
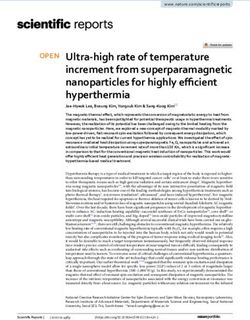
ments were expressed as mean ⫾ standard deviation. The higher at 3 tesla than at 1.5 tesla in all series. Image noiseNo. 3 MRI CONTRAST ENHANCEMENT AT 3TESLA 䡠 Nöbauer-Huhmann et al 117 Figure 1. A 77-year-old female patient with two fibroblastic meningiomas in the high frontoparietal region. The larger lesion shows a broad base to the falx. The plain axial T1-SE scan at 3 tesla (A) shows a tumor that is nearly isointense to the white matter, whereas it is slightly hypointense at 1.5 tesla (B). After contrast administration the marked enhancement of the bigger lesion is homogeneous, whereas the smaller lesion enhances inhomogeneously. The enhancement of both well-demarcated lesions was more pronounced at 3 tesla (C), than at 1.5 tesla (D). The tumor is well demarcated on the coronal contrast-enhanced MP-RAGE scans at 3 tesla (E), and at 1.5 tesla (F). was considered to be higher at 3 tesla on T1-SE pre- and contrast sequences was significantly higher on the 3.0 T postcontrast. images than on the 1.5 tesla ones (with P ⫽ 0.036; mean For the homogeneous subgroup, the calculation of all difference ⫽ 51.2; 95% CI, 4.4 –98.1). The same was true of parameters of visual assessment revealed comparable re- the T1-SE postcontrast scans (with P ⫽ 0.028; mean dif- sults (Fig. 1), apart from “other artifacts,” which were not ference ⫽ 20.86; 95% CI, 2.86 –38.87) (Fig. 1). The signal different in the postcontrast series. Quantitative image as- enhancement for the lesion (EL), in the T1-SE scans was sessment was performed in nine patients, after excluding six 11.2% higher at 3 tesla compared with 1.5 tesla. This patients in whom contrast enhancement was limited almost difference was not statistically significant. exclusively to the tumor periphery. Mean values ⫾ standard deviation of the parameters assessed in those patients are Discussion given in Table 2. On average, the tumor-to-brain-contrast It is well known that magnetic field strength influences after gadolinium administration (RL,B) in MP-RAGE post- the effect of contrast media. In our study, we evaluated the
118 INVESTIGATIVE RADIOLOGY March 2002 Vol. 37
TABLE 2. Quantitative Assessment
Sequence 1.5 T 3T P
Preinjection tumor-to-brain-contrast
(RLO,BO) T1 ⫺10.5 (⫾8.1) ⫺2.8 (⫾15.3) ns
Tumor-to-brain-contrast after
gadolinium administration (RL,B) T1 72.1 (⫾35.3) 93.0 (⫾41.7) 0.028
MP-RAGE 46.3 (⫾19.7) 97.5 (⫾62.7) 0.036
Signal enhancement of the lesion (EL) T1 91.0 (⫾27.9) 101.2 (⫾34.1) ns
Mean values ⫾ standard deviation of the ratios calculated from ROI-measurements in nine patients with homogeneous tumors at 1.5 T and
3 T and the statistical significance of the differences.
numerical ratios of signal intensities of tumors versus nor- mal brain tissue, significantly higher signal enhancement
mal brain and tumor enhancement and the subjective per- was found at 3 tesla.
ception of radiologists. In our study, we showed that in MP-RAGE, and even in
The effect and behavior of contrast agents at different postcontrast T1-SE not optimized for 3 tesla, the contrast
field strengths depends on the nuclear magnetic relaxation between the tumor and the surrounding normal brain is
dispersion and the field-dependent relaxation of the tissue.13 markedly higher at 3 tesla compared with 1.5 tesla. The
Generally, the water proton relaxation rates (1/T1) of brain observed increase in tumor-to-brain contrast is in accor-
tissues decrease when the field strength is increased from dance with studies at lower field strengths.9,10 Our results
1.5 tesla to 3 tesla.14 Similarly, the relaxivity of a paramag- confirm the previous expectations17 that although both the
netic ion to water protons, described by the Solomon- relaxation rate of the unenhanced tissue and the relaxivity of
Bloembergen-Morgan equation, may also be diminished at the contrast agent decrease with increasing field strength, it
higher magnetic fields.15 Thus, signal enhancement in T1- is not a proportional process.
weighted MR images produced by administration of a stan- The contrast effect of gadodiamide in brain tumors com-
dard dose of gadolinium contrast agent should depend on pared with normal brain (GM) has been found to be greater
actual relaxation times of nonenhanced (gray and white at 1.5 tesla than at 0.3 tesla in a recent study.9 Our findings
matter) and enhanced (tumor) tissues at a particular field. also correlate well with another study where the author
In a patient with normal extracellular fluid space, the found an increase in contrast enhancement in brain tumors
typical contrast dose of 0.1 mmol/kg body weight leads to a at 2.0 tesla compared with 0.5 tesla.10
target tissue concentration (TTC) of ⱖ 0.5 mmol/L.16 The In a study by Haustein,8 signal enhancement of the lesion,
relaxivity of gadodiamide has been tested in lower and EL, did not show significant field-strength-dependent differ-
higher field strengths up to 2 tesla. A decrease that becomes ences between 0.5 and 1.5 tesla, though a tendency toward
slower and is nearly proportional to the field strength above higher contrast at higher field strength was observed. How-
0.4 tesla has been demonstrated in vitro.3 The second effect ever, at a dose of 0.1 mmol/kg body weight, only 10 patients
is the increase in intrinsic T1 of tissue with field strength.13 could be examined at each field strength in this study. These
The increase in T1 relaxation times at 3 tesla compared with findings are in accordance with our results as well.
1.5 tesla is responsible for reduced gray-white differentia- In our study, the T1-weighted spin-echo protocol used at
tion in T1-SE images at 3 tesla. The repetition time opti- both field strengths was optimized for 1.5 tesla. Conse-
mized for 1.5 tesla is too long to produce sufficient gray- quently, it was not optimum for 3 tesla caused by longer T1-
white matter contrast at 3 tesla. Lower tumor visibility in and shorter T2-relaxation times of water protons, which
precontrast T1-SE images at 3 tesla can probably also be decreased the contrast in the 3 tesla images, at least between
attributed to these mechanisms. As T1 is shorter at lower gray and white matter. Despite this, tumor-to-brain contrast
magnetic fields, a further decrease caused by administration after contrast agent administration, RL,B, was higher at 3
of contrast agent seems to produce less contrast than at tesla than at 1.5 tesla. Conversely, we used MP-RAGE
higher field strengths. protocols optimized for each particular scanner by the
We found that signal enhancement for the lesion, EL, was manufacturer.
not significantly different at either field. The same observa- Although there are many differences in 1.5 tesla and 3
tion was reported for the signal enhancement at 0.5 tesla and tesla MP-RAGE acquisition parameters, only inversion time
1.5 tesla,8 though a tendency toward higher contrast at a and, to a lesser degree, TE and TR, affect the quantitative
higher field strength was observed. This is probably caused assessment criteria. Using the optimized MP-RAGE se-
by the fact that the precontrast tumor signal intensity varies quences, gadolinium-enhanced tumor-to-brain contrast was
significantly for different types of tumors and at different significantly higher at 3 tesla compared with 1.5 tesla. This
field strengths. When signal enhancement is related to nor- observation indicates that the benefit of 3 tesla MR imagingNo. 3 MRI CONTRAST ENHANCEMENT AT 3TESLA 䡠 Nöbauer-Huhmann et al 119
may be even higher when specific changes of the parameters where the contrast effect of gadodiamide proved to be lower
of human tissues (T1, T2-relaxation times) with increasing (0.3 tesla vs 1.5 tesla),9 which is in accordance with our
field strength are considered in the protocol design. findings. Correlation of lesion enhancement with histologic,
Regarding visual assessment, in the postcontrast T1-SE biologic, and functional parameters are the topic of continu-
sequences, the parameters that define the subjective percep- ing studies2,20 and may also be the subject of further studies
tion of the lesion did not differ significantly for either in high field MRI. In summary, we showed that the objec-
scanner. We suggest several reasons that could be respon- tive tumor-to-brain-contrast (the contrast between tumor
sible for what we initially considered a contradiction of the and surrounding normal brain) in MP-RAGE and even
objective values. nonoptimized T1-SE postcontrast sequences was markedly
First, the newly developed open head resonator used in higher at 3 tesla compared with 1.5 tesla.
our 3 tesla examinations improves patient comfort, but it
suffers from decreased sensitivity compared with the stan- References
dard resonator. Second, the parameters used in the T1-SE
1. Runge VM, Carollo BR, Wolf CR, et al. Gd-DTPA: A review of
sequence had been optimized for 1.5 tesla and not for 3 tesla clinical indications in central nervous system magnetic resonance
as the 3 tesla MR-unit is a research scanner not optimized imaging. Radiographics 1989;9:929 –958.
for routine imaging but for spectroscopy and functional 2. Runge VM. A Review of contrast media research in 1999 –2000.
Invest Radiol 2001;36:123–130.
studies. Another important factor might be that the experi- 3. Rinck PA, Muller RN. Field strength and dose dependence of contrast
enced radiologists are not yet familiar with the 3 tesla image enhancement by Gadolinium- based MR contrast agents. Eur Ra-
features and contrast. The subjective impression of contrast diol 1999;9:998 –1004.
4. Runge VM, Armstrong MK, Barr RG, et al. A clinical comparison of
enhancement was influenced not only by the contrast of the the safety and efficacy of MultiHance (gadobenate dimeglutimine)
enhanced lesion to the surrounding brain but also by intra- and Omniscan (Gadodiamide) in magnetic resonance imaging in
tumoral structure, which was reportedly more pronounced patients with central nervous system pathology. Invest Radiol 2001;
36:65–71.
at 3 tesla. Assessment of the MP-RAGE would be more 5. Brekenfeld C, Foert E, Hundt W, et al. Enhancement of cerebral
favorable because of higher CNR and SNR. Finally, visi- diseases: How much contrast agent is enough? Comparison of 0.1,
bility and delineation were reduced by susceptibility and 0.2, and 0.3 mmol/kg Gadoteridol at 0.2 T with 0.1 mmol/kg
Gadoteridol at 1.5 T. Invest Radiol 2001;36:266 –275.
pulsation artifacts, especially in infratentorial lesions. 6. Robitaille P-M, Abduljalil AM, Kangarlu A. Ultra high resolution
A limitation of our study was the arbitrary placement of imaging of the human head at 8Tesla: 2K ⫻ 2K for Y2K. J Comput
ROI values at the presumed greatest enhancement. We Assist Tomogr 2000;24:2– 8.
7. Parizel PM, van Hasselt BAAM, van den Hauwe L, et al. Effect of
attempted to reduce this error by placing the ROI in iden- field strength on Gadolinium enhancement in MR Imaging. Eur
tical locations for both field strengths. Slight differences Radiol 1994;4:557–560.
could not be excluded, however. Another limitation is the 8. Haustein J, Laniado M, Niendorf H-P, et al. Administration of Gado-
pentetate Dimeglumine in MR Imaging of intracranial tumors: Dosage
relatively small number of patients examined. As the objec- and field strength. AJNR Am J Neurordiol 1992;13:1199–1206.
tive of the study was to compare signal intensities at differ- 9. Akeson P, Vikhoff B, Stahlberg F, et al. Brain lesion contrast in MR
ent field strengths measured in identical settings (the same Imaging: Dependence of field strength and concentration of ga-
dodiamide injection in patients and phantoms. Acta Radiol 1997;
area of the brain of the same patient after administration of 38:14 –18.
an identical dose of the same contrast agent after a compa- 10. Chang KH, Ra DG, Han MH, et al. Contrast enhancement of Brain
rable time interval), each patient could serve as his/her own tumors at different MR field strengths: Comparison of 0.5 T and 2.0
T. AJNR Am J Neurordiol 1994;15:1413–1419.
control, which reduces the number of patients required to 11. Holm St. A simple sequentially rejective multiple test procedure. Scan
obtain reliable results. Currently, a major drawback of 3 J Stat 1979;6:65–70.
tesla is the specific absorption rate, which is markedly 12. SAS. The SAS system for Windows. Cary, NC: SAS Institute; 1996.
13. Rinck PA, Fischer HW, Van der Elst D, et al. Field-cycling Relaxom-
greater at 3 tesla than at 1.5 tesla. Hence, the region to be etry: medical applications. Radiology 1988;168:843– 849.
examined with 3 tesla was limited to the known tumor 14. Wansapura JP, Holland SK, Dunn RS, Ball WS. NMR relaxation times in
dimensions. In addition, because of longer T1 values, the the human brain at 3.0 Tesla. J Magn Res Imaging 1999;9:531–538.
15. Wood ML, Hardy PA. Proton relaxation enhancement. J Magn Res
optimum settings for T1-weighted sequences generally lead Imaging 1993;3:149 –156.
to slightly longer scan times. 16. Isselbacher KJ, Adams RD, Braunwald E, et al. Harrison’s principles of
As the objective of our study was to compare the ratios of internal medicine, 9th ed. Kogakusha, Tokyo: McGraw-Hill; 1980.
17. Elster AD. Field-strength dependence of Gadolinium enhancement: the-
signal intensities in different field strengths with exactly the ory and implications. AJNR Am J Neurordiol 1994;15:1420–1423.
same settings, we applied only the typical dose of contrast 18. Yuh WTC, Parker JR Carvlin MJ. Indication related dosing for magnetic
agent, although for specific indications, higher doses have resonance contrast media. Eur Radiol 1997;7(suppl 5):S269–S275.
19. Haustein J, Bauer W, Hilbertz T, et al. Double dosing of Gd-DTPA in
been recommended.18,19 Further studies are necessary to MRI of intracranial tumors. In: book of abstracts: Society of Mag-
show whether particular indications in high field MRI ne- netic Resonance in medicine 1990. Vol.1, Berkeley, CA: Society of
cessitate higher contrast doses or whether even lower doses Magnetic Resonance in medicine; 1990:258.
20. Tynninen O, Aronen HJ, Ruhala M, et al. MRI enhancement and
may be used. It has been proposed, however, that higher microvascular density in gliomas: Correlation with tumor cell pro-
doses might prove useful, especially at lower field strengths liferation. Invest Radiol 1999;34:427– 434.You can also read