LIVING WITH COVID19 SECOND REVIEW - Tuesday 16th March 2021 - NIHR Evidence
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

LIVING WITH
COVID19
SECOND REVIEW
Tuesday 16th March 2021
DOI: 10.3310/themedreview_45225
A dynamic review of the evidence
around on
ongoing Covid19
Ongoing Covid19
(often called Long Covid)
This is the second of
two dynamic reviews
of the evidence
around people’s
experience of the
enduring symptoms
following a Covid19
infection.
1 Living with COVID19
EXECUTIVE
SUMMARY
We published our first review of the evidence in October 2020. At the time there was
uncertainty about the extent to which there could be lasting effects, and most people
assumed a linear progression of a severe acute infection with a long recovery tail. Our
first review on “Living with Covid19” was informed by the experience of professionals
and we worked closely with a group of people with lived experience. In this review, we
focus on the published evidence. In addition, we report findings from a short survey
of people living with Covid19 that we embedded on our website. With over 3,000
responses it provided us with an insight into the key issues and challenges for people
living with Covid19.
Since October, the term ‘Long one month later and at least 10% to hospital and those who stayed
Covid’ has gained widespread use three months later. For those at home. The limited evidence of
and we have adopted it. But we who were admitted to hospital, correlation between past history
recognise it covers a wide range of between 50% and 89% have at and current pathology would
symptoms, including a high number least one enduring symptom after suggest a need to investigate
of post-viral fatigue cases that two months. Our own and Davis anyone with persistent symptoms,
appear to resolve spontaneously et al. (2020) preprint surveys including those who were never
by 8 to 12 weeks. suggest significant rates of Long admitted to hospital.
Covid beyond six months for
There is enormous variation people who were not hospitalised. There is also evidence of a group of
in the estimated prevalence Any estimates of incidence and people with cognitive processing
of Long Covid due to different prevalence must be considered disorders and anxiety with some
measurement criteria, making provisional. The ONS reported indication of neurological rather
comparing studies impossible. an incidence in December 2020 than social cause. A substantial
Many people were unable to of 301,000 people in the UK with number of people have symptoms
access Covid19 testing when symptoms lasting between 5 and they are not yet understood.
first ill and are excluded from 12 weeks. Long Covid appears to Some are similar to Myalgic
some studies as the infection is be more frequent in women and in Encephalomyelitis/Chronic Fatigue
not confirmed. This may mask young people (including children) Syndrome (ME/CFS) and others to
the true prevalence of Long than might have been expected orthostatic intolerance syndromes.
Covid. Uncertainty about a prior from acute Covid19 mortality. There is some evidence suggesting
infection means some people Long Covid is a still active disease,
report difficulty accessing services Whilst there is a growing list with immunological evidence
for their Long Covid symptoms. It of symptoms associated with of continued inflammatory
appears that at least 10% of those Long Covid, we know little about responses, lingering viral activity
infected with Covid19 experience different clusters and patterns of and/or blood clotting disorders.
at least one symptom for 12 symptoms (sometimes described For some people with Long Covid,
weeks or longer. For those who as phenotypes, syndromes or there appears to be the potential
were not admitted to hospital, at clusters). There is increasing for further deterioration.
least 20-30% experience at least evidence of organ impairment in
one enduring symptom around both people who were admitted
Living with COVID19 2
Long Covid can be very debilitating ongoing monitoring in secondary existing health conditions) who
and some people need help care. This will require joined- may not have been captured in
with personal care months after up care management across research to date and who may be
the initial infection. 71% of specialities and between primary tipped into a state of frailty.
respondents in our own survey and secondary care. New service
said Long Covid was affecting delivery models that provide rapid We conclude that the journey of
family life and 39% said it was access to an increasing number of Long Covid is not well understood
impacting their ability to care people with Long Covid need to be and it is important to continue to
for dependents. This is having an designed and evaluated. This will listen to the lived experience as
impact on the workforce, with 80% also require a multiprofessional we move into the second year of
of respondents in our own survey workforce strategy. this new disease. As we learn more
saying Long Covid had affected about the progression of Long
their ability to work and 36% said As well as clinical rehabilitation Covid, it is important to retain a
it was affecting their finance. care, some people need ongoing wide range of working hypotheses.
social care. Particular attention We make the following
Long Covid can be a multi-system should be paid to the impact of recommendations for the future
disease, and some people may Long Covid on vulnerable people, research agenda.
have active disease that needs (such as older people with pre-
• More research is needed on • We recommend that a rapid evaluation of different
the incidence of Long Covid minimum data set for service models and skill mix for
and its causes. This will help recording a wide range of supporting people with Long
to predict and prevent Long symptoms be agreed and Covid.
Covid in the longer term. used by both researchers and
• Seldom heard voices are
There is an urgent need to healthcare providers.
not visible in the current
research treatments and
• Some elements of Long evidence. We recommend
management for people with
Covid are similar to other research that is targeted at
Long Covid.
conditions and evaluations of vulnerable people (including
• The emergent nature of the interventions (pharmaceutical, older people and people
understanding of Long Covid psychological and physical with learning disabilities) as
emphasises the need to therapies) are needed that well as hard-to-reach groups
continue to explore a range may improve symptoms. including travellers and prison
of hypotheses in any research For non-pharmaceutical populations.
that is undertaken. interventions, a range of
• We recommend that people
research methodologies
• A precursor to research in all living with Long Covid (who
should be encouraged.
areas is a better understanding are experts by experience)
of the disease syndromes • Long Covid is a significant should be equal partners
and symptom clusters that health burden that is unlikely in setting the research
currently sit under the to be met by existing NHS agenda.
umbrella of Long Covid or services and new delivery
post Covid. models that allow rapid access
are needed. We recommend
3 Living with COVID19
Living with COVID19 4

NIHR Centre for Engagement and Dissemination
The National Institute for Health of all the evidence nor are they into account the UK infrastructure
Research (NIHR) Centre for guidance or recommendations and culture, often funded by the
Engagement and Dissemination for practice. Instead they are NIHR. Themed reviews include
(NIHR CED) aims to engage people narratives based on a selection both academic study and practical
in knowledge exchange to develop of different kinds of evidence wisdom from lived experience and
and improve health and social chosen to illuminate and inform are guided by our stakeholders.
care. One of the ways we do this discussions focused on actions for
is through our Themed Reviews. practice. As far as possible, they
These are not systematic reviews highlight UK evidence that takes
What are we aiming to achieve with
our Living with Covid19 reviews?
Our first review on “Living with may be particularly helpful for and the Scottish Intercollegiate
Covid19” was informed by the professionals who are increasingly Guidelines Network (SIGN) to
lived experience of patients and coming into contact with people develop guidelines on the long-
professionals and we worked with Long Covid, but not running term effects of Covid19. Working
closely with a group of people with specialist services themselves. with the Royal College of General
lived experience. In this review, we It may also be helpful for the Practitioners, the first of their
turn our attention to the published families or employers of people ‘living’ guidelines was published
evidence. In addition, we report experiencing Long Covid as well on 18th December 2020. In
findings from a short survey for as people living with enduring November 2020, the NIHR,
people living with Covid19 that symptoms. together with United Kingdom
we embedded on our website. Research and Innovation (UKRI)
As with many surveys, it was a Since October, there has been issued a call for research into the
self-selected sample that may not widespread acceptance that long- longer-term effects of Covid19
be representative of all people term symptoms exist and there in non-hospitalised individuals.
living with enduring symptoms. is increasing activity to refine Successful bids were announced
But, with 3,286 full responses it measurement. NHS England and on 18th February 2021.
provides valuable insight into key the Scottish Government asked
issues and challenges for people the National Institute for Health
living with Covid19. This review and Care Excellence (NICE)
5 Living with COVID19
More papers have been published since our last review,
Framing the but the evidence still resembles a ‘Swiss cheese’ with
evidence many gaps. Inconsistencies in findings reflect different
assumptions in the research design. In this review, we
try to make sense of the disparate body of literature
and clarify what is known, what needs further research,
and most importantly, what we know about
treating Long Covid.
This report is not a systematic narrative. We intend to outline a that many papers describe data
review of all published evidence. coherent picture from some of the collected at an early stage of the
We have not formally assessed the jigsaw pieces of evidence, and we pandemic and therefore cannot
quality of the included evidence. make no claims of completeness. include detailed information about
We searched academic databases the current duration of symptoms.
and sought recommendations In our first review, we opted to This also means that we do not
from a network of people looking exclude preprints because they know the impact of new variants
at Long Covid. We identified had not yet been peer-reviewed. or vaccinations on rates of Long
302 publications, some of which We still read them with caution, Covid (however defined). Whilst
were opinion pieces or personal however they identify themes that we do not think the evidence can
stories. We narrowed this down are relevant to policy, practice be synthesised, it can be used to
to research papers that addressed and future research questions, build a three dimensional picture
three themes: how common is Long so we discuss their findings of Long Covid and to illuminate
Covid? What causes Long Covid? as propositions rather than as what further questions need
and how might Long Covid be assured evidence. Where we to be asked. Summaries of
treated? The team decided which reference them, we identify that included studies can be found
papers to include in this review they are preprints. The nature in Appendix A.
based on how they added to the of research reporting means
Living with COVID19 6
What is ‘Long Covid’?
One of the features of Long Covid is the wide
range of symptoms. Davis et al. (2020)
preprint lists 205 different symptoms related
to 10 different systems. For some people, it
has a relapsing nature, often referred to as
the ‘corona coaster’, and for others, there is a
single symptom but with a typical progress.
This has significant implications for the
management of the disease.
More than one syndrome
Our first review was mindfully
called ‘Living with Covid19’ to
capture a range of symptoms
that persist following a Covid19
infection. We noted that people
may experience different clusters
of symptoms or syndromes (see
Figure 1). We proposed that some
people suffered permanent organ
damage and there may also be a
number of distinct syndromes,
including post intensive care
Figure 1: Measurement of symptoms, clusters or individual conditions
syndrome, post viral fatigue
syndrome and long-term Covid
syndrome. We also observed that future research should consider traumatic stress disorder”.
some people may be suffering with subtypes of Long Covid. Cirulli et
more than one syndrome at the al. (2020) preprint report of a large Sudre et al. (2020) preprint
same time. cohort study in the USA describes reported two different patterns of
diverse phenotypic presentations. symptomatology for Long Covid
Since then, others have been from the Zoe Covid Symptoms
reaching similar conclusions about Some authors have attempted to Study App; firstly, people reporting
distinct patterns. Ayoubkhani et classify the different syndromes. exclusively fatigue, headache and
al. (2021) preprint reporting on Venturelli et al. (2021) followed up upper respiratory complaints
the Office for National Statistics patients discharged from hospital (shortness of breath, sore throat,
(ONS) work notes that Long Covid, in Italy and noted three different persistent cough and loss of smell)
or post-Covid syndrome, is not a syndromes “it appears reasonable and secondly those with additional
single condition and Yong (2020) to try and separate those symptoms multi-system complaints,
preprint noted multiple different related to post-viral chronic fatigue including ongoing fever and
symptoms and potential disease syndrome, from those due to post- gastroenterological symptoms.
mechanisms and recommends that critical-illness syndrome, or post-
7 Living with COVID19
Amenta et al. (2020) propose confirm the undulating nature of noted that the ‘biphasic’ disease
three classifications: 1) residual Long Covid symptoms described pathway description of ‘acute
symptoms that persist after in our first review with 64% of illness’ and ‘post-acute illness’ did
recovery from acute infection; (2) respondents reporting a period of not match the lived experience
organ dysfunction that persists wellness before relapsing. reports of multiple and diverse
after initial recovery; and (3) new ongoing symptoms. Some patient
symptoms or syndromes that advocates are unhappy with the
Use of time frames to
develop after initial asymptomatic term ‘post Covid’ as it suggests
segment the patient
or mild infection. The Cochrane there is no active disease process.
population
Rehabilitation 2020 rapid living They point to both the evidence
systematic review (Ceravolo et Some have categorised ongoing on continuing viral presence and
al. 2020) used four categories symptoms by duration, noting the presentation of new symptoms
that might relate to Long Covid: significant resolution rates at after 12 weeks (see section on
1) symptoms continuing from the 5 weeks and again at 12 weeks. what causes Long Covid). NICE’s
acute phase of Covid19 and its The NICE guideline published in rationale for describing ‘post’
treatment; 2) symptoms causing December 2020, together with Covid19 syndrome was that it
a new health condition; 3) late SNOMED codes for medical reflected that the acute phase of
onset symptoms appearing as records released in the same illness had ended and they did not
a consequence of Covid19 but month, divide symptoms into intend for it to indicate that the
after the end of the acute phase; three time periods; acute Covid19 person had recovered.
4) impact on a pre-existing health up to four weeks; ongoing
condition or disability. symptomatic Covid19 from 4
to 12 weeks; and post-Covid19
syndrome developing during or
Undulating symptoms after an infection consistent with
and relapses Covid19 and continuing for more KEY POINTS
than 12 weeks and not explained Researchers have categorised
Salmon-Ceron et al. (2020) found
by an alternative diagnosis. The ongoing symptoms following a
that 43% of people followed
NICE categories do not relate to Covid19 infection both by their
up after discharge from a Paris
particular symptoms or groups of duration and by the number of
hospital had a symptom-free
symptoms. symptoms. The difference in their
interval before relapsing. They also
report that 76% presented new findings raises a question about
symptoms that were absent during
Lived experience whether different people need
the acute phase of their Covid19
perspectives different treatment and support.
infection. Davis et al (2020) Callard and Perego (2020) Indeed the duration of symptoms
preprint paper of an international described how patient advocates may correlate with different
web-based survey, led by people rather than researchers created syndromes or phenotypes and
with Long Covid, reported 86% the narrative and the name Long may be related to different causal
of respondents experienced Covid after connecting on social mechanisms.
relapses occurring in an irregular media and making visible the
pattern, or in response to specific persistent nature of a wide range
triggers (such as physical or mental of symptoms when attention
activity, stress, menstruation, heat, was primarily focused on acute
or alcohol). Our survey findings illness and mortality. They
Living with COVID19 8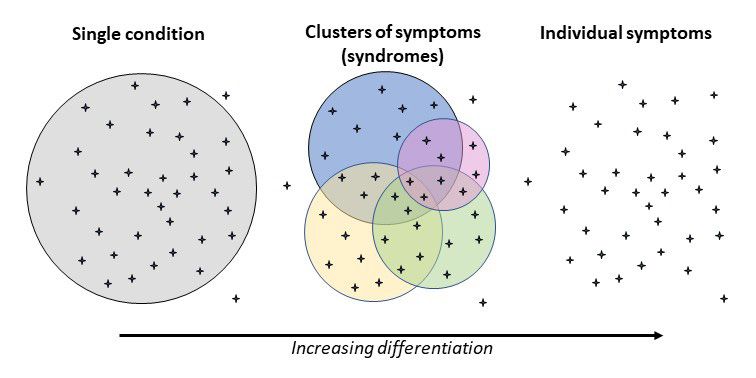
How many people who
have had Covid19 will
experience ongoing
symptoms?
Why is this important? Methodological challenges For many studies, a positive
antigen, polymerase chain reaction
Understanding how many The lack of a consistent definition
(PCR) or antibody test is required
people experience Long Covid is of Long Covid makes assimilating
to exclude people with symptoms
important for a number of reasons. findings from different studies
not associated with a Covid19
Firstly, the need to plan adequate difficult. As Figure 2 demonstrates,
infection. However, community
services (including assessment, studies have focused on different
testing was suspended in the
diagnosis, treatment and people, symptoms and time
UK in March 2020 and 82% of
supportive care) and the workforce intervals, and used different
respondents to our survey said
to deliver them. Secondly, knowing sample sizes. The early lack
community testing was not
how many people have ongoing of awareness of the range of
available at the time of their initial
problems informs decisions about symptoms associated with
infection. This lack of testing
funding for further research. Covid19 meant that many people
was also noted by Varsavsky et
Thirdly it helps to calculate the did not associated their symptoms
al. (2021), who reported that
potential impact on society in with Covid19 and therefore did not
only 40% of those who reported
the future, including the impact associate their enduring symptoms
classic symptoms on the Zoe
on those of working age and by with Long Covid. Conversely, the
Covid Symptom Study App had
extension the economy. Finally range of Long Covid symptoms is
gone on to receive a test. In our
there may be a new generation of not widely known and people may
survey, 56% of respondents had
carers for those with Long Covid not associate them with a prior
either had an antigen test or an
who have their own needs. Covid19 infection.
antibody test at a later date. Of
those tested, 46% tested negative,
despite having had symptoms
consistent with the virus. 67% of
respondents were told by a health
professional that their symptoms
might be due to Long Covid. Barker
Davies (personal communication),
reporting on the UK Defence
Medical Rehabilitation Centre
video assessment service, found
that service personnel who had
not been admitted to hospital were
75% less likely to have had a test
confirmation than those who were
admitted to hospital.
Figure 2
9 Living with COVID19They also found that those had may have been skewed. infection. For example, Cirulli et
received a test confirmation of Most studies report the frequency al. (2020) preprint of a large public
Covid19 had their assessment of at least one symptom, not health study in the USA showed
earlier than those who without necessarily the same symptom, that whilst people both with
a confirmation (8.5 weeks v rather than a cluster of symptoms. and without a history Covid19
16 weeks). The inability of a Many of the symptoms reported reported persistent new symptoms
significant number of people occur in a range of diagnoses, and over three months, those who
reporting Long Covid symptoms to a few studies have used controls tested positive for a Covid19
confirm an initial infection means to see if enduring symptoms are reported them twice as often.
sampling in some of the studies more common after a Covid19
Study No of participants in study Study No of participants in study
47,780 Covid19+ hospital Halpin et al. 100
Ayoubkani et al. (ONS) discharges (matched
to controls) Puntmann et al 100
9,063 Covid19+ with LC Tabacof et al. 84
ONS January
symptoms (from CIS Salmon-Ceron et al. 70
2021 update
survey of 150,000)
Raman et al. 58
Sudre et al. (Zoe App) 4,182
Vlachou et al 39
Davis et al. 3,762
Guedj et al. 35
NIHR CED survey 3,286
Doykov et al. 20
Munblit et al. 2,649
Yeoh et al. 27
Vaes et al. 1,837
Humphreys et al. 18
Huang et al. 1733
Kommoss et al. 13
Venturelli et al. 767
Dani et al. 6
357 Covid19+ ( 24,592
Ciculli et al.
non-matched controls) Ludvigsson et al. 5
Xiong et al. 538
Mandal et al. 384 Box 1 : Primary research studies (N.B. different research
361 Covid+ (83,924 questions and designs means size of sample is not necessarily
Hampshire et al. an indicator of relative quality)
non-matched controls)
Tenforde et al. 292
Moreno-Perez et al. 277
Bergamaschi et al. 207
Dennis et al. 201
Logue et al. 177
Barker Davies et al. 155
Carfi et al. 143
Landi et al 131
Buonsenso et al 129
Townsend et al. 128
D’Cruz et al. 119
Arnold et al. 110
Tomasoni et al. 105
Living with COVID19 10Range of prevalence compared. The NICE guideline samples chosen to represent
estimates (2020) evidence reviews 2 and everyone in the population and
3 noted the range of symptoms those where people self-select).
Measurement is reported as either
reported across studies was very
prevalence (proportion of a known
broad and that all the studies Estimates of the proportion of
population at a specified point in
reviewed were at high or moderate people who experience Long
time) or incidence (rate of new
risk of bias. Covid post-hospital discharge are
cases within a defined period of
more robust than for people who
time). The prevalence estimates
Seldom heard groups such as were not hospitalised. Studies
within the UK and internationally
travellers, prison populations, published to date show that a
(see Figure 3) vary widely, even
frail elderly people, care home higher proportion people who had
when measuring the same time
residents, those with learning been admitted to hospital go on to
frame. Estimates of people with
disabilities and children are experience Long Covid, although
symptoms that have not resolved
not well represented in the this may reflect definitions of Long
by eight weeks range from 4.5%
data. Published studies may Covid that relate to a particular
of people completing the Zoe
therefore not be representative of set of symptoms more common in
Covid Symptom App (Sudre
everybody who has Long Covid. those who were hospitalised (see
et al. 2020 preprint) to 89% of
section on what is Long Covid).
people who received a minimum
Studies also differ in the way they We also note that criteria for
of oxygen therapy in hospital for
collect data. Some follow up a being admitted to hospital vary
more than 48 hours (D’Cruz et
cohort of people (a fixed group of across countries. Even in the UK,
al. 2020). However, the studies
people studied over time), others reports do not always differentiate
used different case definition
use cross-sectional surveys (a between the different levels of
and different inclusion criteria
sample of people studied at a point care (those who received standard
and therefore cannot be directly
in time, and these differ between oxygen therapy, high flow oxygen
or Continuous Positive Airway
Pressure therapy [CPAP] and those
who were mechanically ventilated).
Symptom reporting
up to four weeks
Early studies looked at short term
effects. For example, Tenforde et
al. (2020) conducted a multistate
telephone survey in the USA of
292 adults who had a positive test
result for Covid19 but were not
admitted to hospital, finding 35%
had not returned to their usual
state of health two to three weeks
after testing. This included 20%
of 18–34 years with no pre-
existing conditions.
Figure 3: Range of prevalence estimates by duration
11 Living with COVID19Symptom reporting people eight weeks after discharge Moreno-Perez et al. (2021)
from 5 to 12 weeks from a UK hospital and found only prospective cohort study of adult
11% had no lasting symptoms; patients in Spain presenting
The ONS (January 2021)
39% were more breathless and/ at an emergency department
estimated that 20% of all people
or had a persistent cough; 57% with varying severity of disease
in the UK who had tested positive
reported sleep disturbance; and reported that 50% had a post-
for Covid19 exhibit symptoms
25% demonstrated post-traumatic acute Covid19 syndrome (Long
for five weeks or longer and 10%
stress disorder. Halpin et al. (2021) Covid) 10 to 14 weeks after the
exhibit symptoms for 12 weeks or
followed up people from another infection. Cirulli et al. (2020)
longer. They reported an incidence
UK hospital on average six weeks preprint paper reports an online
of 301,000 people with symptoms
after discharge and reported that survey of 21,359 people self-
lasting between 5 and 12 weeks
72% of post ICU patients and 60% selected from existing cohort
for the week commencing 27th
of those treated on the wards health studies in the USA to
December 2020.
reported new illness-related control for Covid19. Respondents
fatigue. Both groups reported were categorised into three groups
These are provisional estimates
breathlessness and psychological for comparison; those who tested
that may be revised as the follow-
distress. 69% of ICU patients and positive for Covid19, those who
up data mature and the study
46% of ward patients reported tested negative for Covid19 and
methodology is developed. The
lower health-related quality of life those not tested at all. All were
ONS survey collects data from a
scores. These UK studies mirror asked about new symptoms (due to
random, representative sample
international findings. Xiong et any illness) that had lasted longer
of the community population in
al. (2020) reported that 50% of than 30 days. 15% of those who
the UK through the Coronavirus
patients discharged from a hospital had tested positive for Covid19
Infection Survey (CIS). Everyone
in Wuhan reported one or more were still experiencing symptoms
in the sample is swabbed at every
persistent symptoms three months lasting three months or more,
follow-up visit, irrespective of
later. Carfì et al. (2020) found that compared to 8% of those who had
symptoms or recent contacts.
87% of patients discharged from never been tested.
Thus there is no dependence on
a Rome hospital after a Covid19
the broader community testing
infection were still experiencing The lowest estimate of enduring
paradigm of the day. ONS have
at least one symptom two months symptoms came from Sudre et al.
added a new question to the
after the onset on Covid19 and (2020) in their October preprint
CIS survey in 2021 allowing
40% said that the quality of their reporting on 4,182 self-selected
respondents to state the impact
life had been reduced. Tomasoni people who entered data on the
Long Covid has had on their day-
et al. (2021) found that 52% of Zoe Covid Symptom Study App and
to-day activities, and including
patients discharged in Milan had tested positive for Covid19.
an expanded list of symptoms.
reported persistent physical They found 4.5% reported having
Recognising that some people with
symptoms between one and three symptoms lasting more than eight
symptoms may test negative this
months after they had recovered weeks and 2.3% having symptoms
question will not be dependent on
from a Covid19 infection and 17% for longer than 12 weeks.
a positive test finding.
reported persistent cognitive
disorders. Mini–Mental State
People admitted to hospital have
examination of 25 of the patients
been followed-up more often
demonstrated scores that were
than those who stayed at home.
compatible with cognitive
D’Cruz et al. (2020) followed up
impairment in 40%.
Living with COVID19 12Symptom reporting at Munblit et al. 2021) including our people responding were aged 30-
six months own, where 81% of respondents 59.
were female, and we discuss
Huang et al. (2021) reported
possible biological sex differences There is growing evidence of Long
on the follow up of patients
in the section on what causes Long Covid in children. Buonsenso et
discharged from a hospital in
Covid. However, most research al. (2021) preprint followed up
Wuhan following a diagnosis of
findings do not then report in children who presented to an
Covid19. 76% of patients reported
detail whether the experience of Italian hospital with Covid19,
at least one symptom six months
Long Covid differs by sex. There excluding those with severe
after the infection onset, with
is little discussion about ethnicity disabilities. 53% had at least
incidence higher in women. Logue
in Long Covid, although this may one persisting symptom four
et al. (2021) surveyed people
be a sampling issue. Cirulli et months after diagnosis and 43%
with confirmed Covid19 infection
al. (2020) preprint reports an reported that it affected their
in the USA, 85% of whom had
investigation using a pre-existing daily activities. They note that
not been hospitalised. 33% of
public health cohort study in the three children developed multi-
non-hospitalised and 31% of
USA that matched people who system inflammatory syndrome;
hospitalised patients reported at
reported a Covid19 infection this syndrome in children with
least one persistent symptom six
with controls (people already in Covid19 is also noted by Ahmed
months after diagnosis. Munblit
the cohort study but who had not et al. (2020) systematic review.
et al. (2021) preprint follow up of
had a Covid19 infection). They Ludvigsson et al. (2020) case
patients discharged from a Russian
found no differences between report described five children with
hospital found that 47% reported
ethnicities in overall rates of long- symptoms lasting for six to eight
one persistent symptom six to
term symptoms, although they months after a clinical diagnosis of
eight months later and 11% had
acknowledged that the sample Covid19. None were hospitalised
multi-system symptoms.
size of non-white ethnicities was and although improving, none had
limited. returned to school. The Office
Demographics for National Statistics (ONS), in
The profile of people with Long Long Covid appears to be more their January 2021 update based
Covid does not seem to match common in younger people on their CIS household survey,
those hospitalised with Covid19 than would be anticipated from estimated that 12.9% of 2-11 year
or those who die from it. Most the rates of hospitalisation for olds and 14.5% of 12-16 year olds
surveys indicate that Long Covid Covid19. 67% of respondents in the UK were still experiencing
is more commonly reported by to our own survey were aged one of the symptoms in the survey
women (Yong. 2020; ONS 2020; between 25 and 54 and Davis et five weeks after testing positive
Sudre et al. 2020 Davis et al. 2020; al (2020) preprint report 87% of for Covid19.
KEY POINTS prevalence at six months. Our own and Davis et al.
(2020) preprint surveys suggest significant rates of
Prevalence estimates cluster into broad groupings,
Long Covid beyond six months for people who were
although caveats around bias and representation
not hospitalised. Any estimates of incidence and
mean they should be treated with caution. For those
prevalence must be considered provisional.
who were not admitted to hospital, it appears that
at least 20-30% experience at least one enduring
Long Covid appears to be more frequent in women
symptom around one month later and at least 10%
and in young people (including children) than might
three months later. For those who were admitted
have been expected from acute Covid19 mortality.
to hospital, between 50% and 89% have at least
There is little data about ethnicity and the incidence
one enduring symptom after two months and
of Long Covid in these groups is unclear.
more recent studies suggest there is still a high
13 Living with COVID19The causes of Long Covid
This section looks at the evidence about what causes Long Covid and its impact
physically, psychologically and socially. Understanding the cause of Long Covid
would help design treatments and to prevent it. Much of the evidence is speculative,
based on the symptoms people with Long Covid display or generalising from
conditions with similar symptoms. It is unclear whether the same pathology seen
in the acute phase of Covid19 also leads to Long Covid. As Yong’s (2020) preprint
observes, one puzzling feature of Long Covid is that its development is not predicted
by initial Covid19 severity.
We do not know whether symptom Immunology changes and persistent cell
patterns reflect already known defects may contribute to Long
The fact that so many physiological
syndromes or a unique new Covid. Doykov et al. (2020)
systems are involved in Long
disease of Long Covid. Salmon- analysed blood samples from
Covid led the British Society for
Ceron et al. (2020) raised several healthcare workers who had
Immunology (2020) to suggest that
theories about the cause of Long tested positive for Covid19 who
damage caused by the immune
Covid: continuing presence of were asymptomatic or who had a
system’s response, rather than
the virus, reinfection (the same mild acute infection and compared
the virus itself, may be causing
or possibly a different strain), their mass-spectrometry-based
the symptoms. Barker Davies
dysfunctional immune response assay profiles with those of a
et al (2020) noted inflammatory
leading to an inflammatory chronic similar control group who had
changes seen in Covid19 can result
condition, or a condition similar tested negative. All who had tested
in inflammation of blood vessels,
to ME/CFS. They observed that positive, both asymptomatic and
myocarditis (inflammation of the
post-traumatic stress could not be moderately symptomatic, retained
heart muscle) and arrhythmias
dismissed as a factor. a significant inflammatory
(heart beat irregularities) which
response two months later with
may explain some of the symptoms
Post Viral Fatigue raised biomarkers, especially
and diagnostic findings in Long
those related to anti-inflammatory
The most commonly reported Covid. This is borne out in Raman
responses and mitochondrial (the
enduring symptom following the et al. (2020) paper that found
part of cells that produce energy)
onset or Covid19 is fatigue. This damage visible on MRI scans
stress.
is a well-established symptom beyond just the lungs and reduced
following viral infections and exercise tolerance correlated with
Salmon-Ceron et al. (2020) suggest
was noted after the Spanish Flu serum markers of inflammation.
Covid19 may lead to autoimmune
pandemic and the more recent The British Society for
conditions in genetically
SARS, MARS and Ebola epidemics. Immunology suggest that
predisposed individuals. The
Fatigue is also observed after inflammatory responses may
British Society for Immunology
some bacterial infections. Lam et worsen pre-existing conditions, but
(2020) observed that other viral
al (2009) report a follow-up study equally may cause new ones. They
infections can trigger a range of
of 233 patients with Severe Acute also note that inflammation can
autoimmune diseases such as
Respiratory Syndrome (SARS) in lead to thrombotic complications.
Guillain Barré syndrome.
Hong Kong which showed that Bergamaschi et al. (2020) preprint
40% met the criteria for Chronic demonstrated that people
Fatigue Syndrome at four months needing hospital admission had
and 27% for longer than six delayed immune responses and
months. conclude that late inflammatory
Living with COVID19 14Yong. (2020) preprint notes that no difference in the prevalence discharge from hospital. Dennis
Long Covid can have similar of symptoms between patients et al. (2020) preprint reported on
symptoms to conditions such as with a negative test and those people thought to be at low risk
lupus and rheumatoid arthritis. who tested positive. Referring to from a Covid19 infection (82% of
Dani et al (2020) suggest a number of other publications, whom had not been hospitalised).
Long Covid symptoms may be Yong (2020) preprint also reported 66% of those with ongoing
explained by ‘immune-mediated that some patients still tested symptoms had some degree of
autonomic instability’ and may positive for Covid19 four months impairment in one or more organ
result in deconditioning (muscle later. They also noted the virus systems four months after initial
weakness), hypovolaemia (low has been detected in faeces for Covid19 symptoms. D’Cruz et
level of fluid in the body) or up to two months regardless of al (2020) used computerised
neuropathy (dysfunction of one gastrointestinal symptoms. tomography to scan the chests
or more nerves). They suggest Yong suggests that in certain of patients with persistent
that the symptoms of Long cases, the viral persistence may respiratory symptoms and/or
Covid are similar to orthostatic lead to a specific immune response blood oxygen saturation levels
intolerance syndromes (inability responsible for Long Covid dropping by more than 4% during a
to regulate blood pressure when symptoms. Sit to Stand test two months after
changing position) including being hospitalised for a severe
hypotension, fainting, tachycardia Yeoh et al (2020) reviewed people Covid19 infection. 66% had some
(racing heartbeat), palpitations, who had tested positive for degree of impairment in one or
breathlessness and chest pain. Covid19 and collected serial faeces more organ systems. 75% showed
This occurs when instead of blood samples up to 30 days after the Covid19 related interstitial lung
vessels constricting when a person virus was no longer detected. Gut disease (tissues surrounding the
changes position (so blood doesn’t microbiome (the type and range airways) and/or airways disease.
pool in the pelvis and legs), blood of microorganisms in the gut) was
vessels dilate leading to low blood significantly altered compared Although there is evidence of
pressure, dizziness and ultimately with people who had not had organ impairment, it is too early
fainting. Covid19 and was associated with to say whether it is reversible.
inflammatory markers in the blood; However, organ impairment should
Viral persistence they suggest the changes in the be considered when investigating
gut may contribute to Long any Long Covid symptoms. Given
Salmon-Ceron et al. (2020)
Covid symptoms. Long Covid is a multiple system
reviewed people who had tested
condition, impairment may be seen
positive for Covid19 and whose
symptoms had either lasted longer
Evidence of cardiac and across a multiple organs, all of
than two months from initial onset
respiratory and other organ which may be related.
or had recurred. They found that
impairment
25% still had positive PCR nose Puntmann et al. (2020) found 78%
Thrombo embolism
and throat swabs. They suggest of people who were followed up There has been significant
the virus may have continued to around ten weeks after hospital evidence of the impact of blood
replicate in the colonised sites, discharge had abnormalities clotting in people hospitalised
or had spread to other parts visible on cardiovascular magnetic with Covid19 infections, with the
of the body and in some cases, resonance imaging and 60% had introduction of anticoagulants for
people had been infected with a ongoing myocardial inflammation. hospital patients being an early
different strain of Covid19. Landi Mandal et al (2020) reported that treatment success. There is some
et al (2021) used PCR tests with 38% of patients in a Long Covid emerging evidence that thrombo
patients discharged from an Italian clinic had chest X-ray findings that embolism is a feature of people
hospital deemed to have recovered remained abnormal and 9% had with Long Covid symptoms.
from Covid19 and found 17% X- rays showing deterioration
tested positive, however there was seven to eight weeks after
15 Living with COVID19Mandal et al. (2020) found 30% Neurological impact not statistically related to gender
of people who had abnormal or age. The British Psychological
Wildwing and Holt’s (2021)
biomarkers when discharged from Association (2020) guidance on
overview of systematic review of
hospital had persistently elevated meeting the psychological needs
neurological symptoms in Covid19
D–dimer levels (a test used to of people recovering from severe
reported two types of neurological
help diagnose clotting) and 10% coronavirus (Covid19) suggest a
symptoms; life threatening
had raised levels of C-reactive range of symptoms may be seen
symptoms such as Guillain Barré
protein (CRP, which measures and recommends psychological
Syndrome and encephalitis, and
inflammation) eight weeks later. components of care to aid
chronic symptoms such as fatigue
Venturelli et al (2021) reported recovery.
and myalgia which appear very
17% of patients followed up after
similar to other neurological
hospital discharge had D-dimer Whilst a number of researchers
conditions such as Chronic
values twice the threshold for refer to the psychological needs
Fatigue Syndrome (CFS) and
diagnosis of pulmonary embolism of people with Long Covid, this
Functional Neurological Disorder
three months after they first tested does not mean that there is no
(FND). Baig (2020) suggests that
positive for Covid19. Kommoss et underlying and/or overlapping
Covid19 invokes different immune
al. (2020) noted that microvascular physical mechanisms and the
responses at different phases of
damage may also be a cause of psychological response to critical
the disease. They hypothesise
persistent lung damage in patients illness is well documented in
that vascular events causing
with enduring symptoms. Vlachou post- intensive care syndrome.
neurological problems are more
et al. (2021) found the risk for Saying the cause of symptoms
common in the severe acute phase,
pulmonary thrombosis remains is not yet understood is not
whereas neurological symptoms
raised least up to four weeks after synonymous with saying there
of Long Covid are a result of
discharge from hospital. is no physical cause and the
either a low grade ‘smouldering’
uncertainty around different
inflammatory response and/or
classifications of Long Covid
Biological Sex damaged nerve cells. Guedj et al
means a physical cause should
It has been widely acknowledged (2021) reviewed positron emission
be fully investigated. We know
that there is a higher prevalence tomography (PET) scans of the
from other long-term physical
of men requiring critical care brains of people with Long Covid
conditions (such as heart failure
support and men have higher more than three weeks after their
and lung disease) that adjusting
mortality rates from Covid19. initial infection and compared
to changed health status can lead
Takahasksi and Iwasaki (2021) them with healthy matches. They
to depression and anxiety. The
suggest biological sex differences found biomarkers consistent with
National Collaborating Centre for
in immunity may contribute to this, memory and cognitive impairment
Mental Health (2018) asserted
although this has not been tested and autonomic dysfunction that
that two-thirds of people with a
in practice. Conversely, Karlsson are seen in other diagnoses.
long-term condition will also have
et al. (2020) note the higher a mental health problem, mostly
incidence of Long Covid in females Psychological aspects
depression and anxiety disorders.
and question whether the different Using a validated hospital anxiety
T cell responses between males and depression scale, Tomasoni
and females is responsible for Long et al. (2020) found that 30%
Covid, through similar mechanisms of people had anxiety and/or
to those that are known to depression between one and
lead to other autoimmune or three months after clearance
inflammatory conditions which are of the Covid19 virus. These
higher in females. psychological conditions were
Living with COVID19 16Impact of Long Covid also evident in non-hospitalised One area of note is the impact on
cases including those who employment. In our survey, 67%
on daily living
reported no breathing difficulty. of respondents were aged between
As well as clinical needs, the Cognitive difficulties were not 25 and 55 and 81% had been
functional impairment seen in explained by differences in age, in paid employment at the time
some people with Long Covid may education or other demographic they became ill. 80% said it had
result in community and social care and socioeconomic variables. The affected their ability to work with
needs. Our survey asked about authors reported that problems 36% saying their symptoms were
other social impacts and 71% said demonstrated by those who were affecting their financial status.
Long Covid was affecting family not ill enough to be admitted to Similarly, Davis et al. (2020)
life and relationships with 39% hospital was unexpected. preprint paper found 45% of those
saying it was impacting their ability who did not recover within three
to care for their children or other Vaes et al. (2020) asked members month reported needing a reduced
dependents. of a Belgian Long Covid Facebook work schedule, and 22% were not
group who had not been admitted working six months later. Halpin
Cognitive difficulties to hospital to complete the et al. (2021) reported that 15% of
and ‘brain fog’ validated Care Dependency working people were off sick when
A frequently reported symptom is Scale (CDS). The scale asks 15 followed up four to six weeks after
‘brain fog’. Hampshire et al. (2020) questions about activities of discharge from hospital (rising
preprint analysed cognitive test daily living such as personal care, to 38% in those who had an
data from 84,285 self-selected household activities, and social and ICU admission).
Great British Intelligence Test recreational activities. Only 8%
participants. To avoid bias, of respondents reported that
promotional material did not they had needed help with
mention Covid19. Instead, people personal care before the onset KEY POINTS
were told they could undertake a of their Covid19 infection, but
Long Covid’s development is
free online assessment to identify this increased to 52% 11 weeks
not predicted by initial Covid19
their cognitive strengths. After after the infection, with 31%
severity. There is no clear evidence
the assessment they were asked meeting the threshold for being
or clinical consensus about the
to complete a questionnaire care-dependent. Venturelli et
cause of Long Covid. We do not
regarding suspected and confirmed al. (2021) reported that 18%
know whether symptom patterns
Covid19 infection. People who had of people who recalled having
reflect already known syndromes
recovered from Covid19 exhibited been totally independent prior
or a unique new disease of Long
significant cognitive deficits when to infection had some degree of
Covid. For some, the physical,
compared against controls. This dependency on others (defined
psychological and social impact
was particularly so for people who by the Barthel Index) three
can be severe.
had been hospitalised, but was months after hospital discharge.
17 Living with COVID19In our first review, we reported how
Diagnosing people who have enduring symptoms often
and predicting did not feel believed. Being able to predict
those at higher risk of developing Long Covid
the course of would be helpful. We could not find reliable
Long Covid evidence for Long Covid risk factors, although we
note that the ONS plans to capture data that will help.
Investigation and Diagnosis Covid19. Additionally, there (age, sex, comorbidities) nor the
was no association between symptoms of the initial disease
Dennis et al. (2020) preprint paper
routine laboratory markers of predicted the development of
on low-risk people who had had
inflammation and cell turnover and post-Covid (Long Covid) syndrome.
Covid19 (82% of whom had not
fatigue after Covid19. The only associations they found
been hospitalised) found 66% had
were for people with severe
some degree of impairment in one
D’Cruz et al (2020) concluded pneumonia, in whom higher heart
or more organ systems persisting
that chest X-rays two months rate and more lung abnormalities
for three to four months. However,
after discharge are a poor marker on admission to hospital were
the damage was more prevalent
of disease damage. Only 13% of associated with Long Covid. They
in those who had been admitted
people in their study had evidence concurred with Amenta et al
to hospital. Raman et al. (2021)
of Covid19-related lung disease (2020) that Long Covid symptoms
studied patients between two
on X–ray, but 46% reported higher can be subdivided into residual
and three months after discharge
breathlessness scores (compared symptoms, organ dysfunction and
from hospital and compared
with a pre-infection baseline), new inflammatory symptoms, the
them to matched controls as
and 75% of those who went on implication being that they may
part of the PHOSP COVID study.
to have CT scans were seen to have different predictors and
The Covid19 positive patients
have interstitial lung disease and/ require different diagnostic tests.
reported higher rates of symptoms
or airways disease. Dennis et al.
than the controls, and MRI scans
(2020) preprint also concluded Barker Davies and colleagues
showed abnormalities in their
that symptoms and blood tests (personal communication of
lungs (60%), heart (26%), liver
were not good predictors of organ a forthcoming paper) studied
(10%) and kidneys (29%). Whilst
damage. Current risk prediction 155 service personnel referred
abnormalities were more frequent
models may not accurately reflect to the UK Defence Medical
in people who had been most
long-term morbidity. This may Rehabilitation Centre following
severely ill, even patients who
explain Arnold et al. (2020) finding a Covid19 infection. They found
were not ventilated or did not
that although 74% of people no relationships between acute
receive vasopressor/ionotropic
in their study had persistent symptoms or the location of care
support or renal replacement
symptoms, notably breathlessness (home/hospital ward/ITU) and the
therapy showed evidence of organ
and excessive fatigue and limited need for post-Covid (Long Covid)
impairment.
physical ability, chest X-rays and rehabilitation. Indeed, people with
spirometry only showed lung delayed assessment (who were
Similarly, Townsend et al (2020)
abnormalities in 35%. more likely to have stayed at home
found no association between
with their initial infection) were
Covid19 severity (defined as
Risk of deterioration more likely to experience
need for inpatient admission,
supplemental oxygen or critical Moreno-Perez et al. (2020) found
care) and fatigue following that neither baseline features,
Living with COVID19 18shortness of breath, pain and clinical characteristics. This weeks after discharge from
anxiety/mood disturbance than showed higher rates of multi- hospital.
those with an early referral. organ damage across all ages and
The authors recommend prompt ethnicities. People discharged
referral for all patients (including from hospital following a Covid19
people who were not hospitalised infection were 3.5 times more KEY POINTS
and/or did not have confirmed likely to be readmitted and 7.7 The continuing uncertainty about
infections) as there may be times more likely to die within the aetiology of Long Covid
potential for deterioration in 140 days than controls. The risks means that it is difficult to predict
people finding difficulties accessing of readmission was greater for who will experience severe
rehabilitation. people under 70 than those consequences from it. All people
over 70 years, and for ethnic reporting enduring symptoms
Ayoubkhani et al. (2021) preprint minority groups than for the associated with a confirmed or
reported an ongoing ONS study white population. Similarly, suspected Covid19 infection
that compared 47,780 individuals Mandal et al (2020) reported should receive a full assessment.
discharged from hospital after a that 9% of patients in a Long
Covid19 infection with controls Covid clinic had X-rays showing
matched for demographic and deterioration seven to eight
Management
of Long Covid
The uncertainties around the causes of
Long Covid, have meant that management
has focused primarily on ruling out
other diagnoses, treating individual
symptoms and providing functional
rehabilitation. Interventions have drawn
on expert consensus and evidence from
other conditions. We could not find any
interventional studies evaluating the
treatment of people with Long Covid.
Access to services has been with Long Covid had not sought them develop a management plan.
variable. Humphreys et al (2020) any healthcare advice and a 49% said that although they were
preprint explored the experience further 32% had not been able to sympathetic, GPs were not able
of people living with Long Covid access all of the healthcare they to offer much help. Only 16% had
and found some unable to access thought they needed. GP practices accessed a psychologist or mental
advice from health professionals were the most frequently accessed health service and only 11% had
about managing their conditions. service, with 37% of respondents seen a physiotherapist.
In our survey, 15% of respondents saying they listened and helped
19 Living with COVID19The complexity of needs in some rehabilitation in the form of a new draft guideline on ME/CFS
people with Long Covid mirrors breathing exercises reduces for consultation in November
the needs of people with multiple breathlessness in chronic 2020, recommending that exercise
long-term conditions who obstructive airways disease should be personalised and
benefit from a holistic, integrated (Gloeckl et al. 2018; Hsieh et al. overseen by a physiotherapist
approach rather than symptom 2018) and Yong (2020) preprint or occupational therapist with
by symptom management. Many infers that it should work for specialist training and expertise.
people with Long Covid complain respiratory symptoms in Long It recommends that fixed
of fragmented care and 23% of our Covid. incremental increases in physical
survey respondents wanted a case exercise, for example graded
worker/key worker to co-ordinate Physical activity exercise therapy, should not
care. Dennis et al. (2020) pre– be used.
A key element of rehabilitation
print concluded that care should
is exercise. Exercise produces
be multidisciplinary. 77% of our On the other hand, physical
supercompensation to make the
survey respondents wanted a one- activity is a well-established
body stronger, but individuals
stop Covid clinic. rehabilitation intervention
have different levels of exercise
for people who have become
tolerance. Rehabilitation
deconditioned, including those
exercise therefore needs careful
Rehabilitation who have been bed ridden for
prescription and monitoring.
The Stanford Hall expert some time. Whilst exercise should
consensus statement be approached with caution in
The use of exercise as a therapy
(Barker-Davies et al. 2020) ME/CFS, it may be helpful in other
in Long Covid is contested. On
provides a framework of likely viral conditions, for example a
one hand, many have noted the
requirements of multidisciplinary systematic review of exercise
similarities between some of
rehabilitation for previously and cognitive function in people
the symptoms of Long Covid
active individuals post Covid19, living with HIV (Quigley et al
and Myalgic Encephalomyelitis/
based on evidence from other 2019) suggested that physical
Chronic Fatigue Syndrome (ME/
conditions and professional activity may preserve or improve
CFS) which can include exercise
expertise. The framework cognition, although none of the
intolerance. Studies of SARS
provides recommendations for studies were interventional and
survivors raised concerns that
rehabilitation of pulmonary, further research is needed.
exercise intolerance may persist
cardiac, musculoskeletal and for months after infection and
neurological consequences of Exercise tolerance/intolerance
Raman et al (2020) found exercise
Covid19. It recommends all should not be seen as binary
intolerance correlated with
patients requiring rehabilitation concept. A better term might
markers of systemic inflammation.
following Covid19 have a be “symptom-titrated physical
Many of the patients in Raman’s
functional assessment and those activity”. Using the term physical
study stopped Cardio Pulmonary
with post-intensive care syndrome activity instead of exercise therapy
Exercise Testing (CPET) early
should receive psychological, also highlights the need to think
because of generalised muscle
physical and cognitive about exercise as part of a person’s
ache and fatigue rather than
rehabilitation. The Defence day to day life and the need to pace
breathlessness. In July 2020 NICE
Medical Rehabilitation Centre at all activity. Pacing has parallels
made a statement on its website
Stanford Hall is currently running a with elite athletes who cannot
that it should not be assumed
two week residential intervention train to their maximum every
that the recommendations on
and a concurrent research study to day of the week and need to plan
graded exercise therapy in its
evaluate the programme. when to fit in the most demanding
2007 guideline on ME/CFS (CG53)
session and the lighter activity to
apply to people with fatigue
There is evidence that pulmonary complement it.
following Covid19. NICE issued
Living with COVID19 20You can also read