Pathology of Small Airways Disease
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Pathology of Small Airways Disease
Timothy Craig Allen, MD, JD
Ngenerally
Context.—The term small airways disease encompasses a
poorly understood group of lung diseases that
Data Sources.—Current literature is reviewed.
Conclusions.—Small airways diseases include a wide
may arise primarily within the small airways or secondarily variety of diseases of which the pathologist must consider.
from diseases primarily affecting the bronchi or lung Uncommon conditions such as diffuse idiopathic neuroen-
parenchyma. Their histology may be confusing; however, docrine cell hyperplasia and diffuse panbronchiolitis may
because treatments and prognoses vary, correct pathologic show relatively specific diagnostic features histologically;
diagnosis is important. however, most small airways diseases exhibit nonspecific
Objective.—To present a nonexhaustive review of the histologic features. Conditions not considered primary
pathology of primary and secondary small airways pulmonary diseases, such as collagen vascular diseases, bone
diseases, including small airways disease related to marrow transplantation, and inflammatory bowel disease,
tobacco; to various other exposures, including mineral must also be considered in patients with small airways
dusts; to diseases involving other areas of the lung with changes histologically. Clinical and radiologic correlation is
secondary bronchiolar involvement; and to recently important for obtaining the best possible diagnosis.
described bronchiolitic disorders. (Arch Pathol Lab Med. 2010;134:702–718)
Katzenstein,27 ‘‘[t]he literature in this area is confusing
A lthough diseases frequently involve the small airways,
the concept of small airways disease is one of which
many pathologists lack a strong understanding. There are
because many studies combine under one category several
pathologically distinct lesions, and terminology tends to
valid reasons for this lack of understanding. The definition be inconsistent.’’
of the term small airways disease varies based on the
physician’s perspective. Pulmonologists and other clini- CLASSIFICATIONS OF SMALL AIRWAYS DISEASE
cians often consider small airways disease as a group of Hogg and colleagues21 in 1968 first used the term small
lung disorders involving the terminal airways often airways disease to describe airway disease in patients
assessed for airflow obstruction1–8 or underlying etiolo- with variably severe chronic airflow obstruction charac-
gy.9–13 Radiologists generally evaluate small airways terized by loss of bronchioles, mucus plugs, and variable
disease by evaluating high-resolution computed tomog- amounts of inflammation and fibrosis that involve ‘‘the
raphy (CT) scan changes including ‘‘direct signs’’ of small smallest bronchi as well as the bronchioles, so that neither
airways disease, such as centrilobular nodules and bronchitis nor bronchiolitis is an appropriate term.’’
opacities, centrilobular bronchiolar dilation, and promi- Disease severity was noted to correlate with occlusion of
nent centrilobular branching structures, often yielding a airway lumen by mucus and inflammatory cells.21 This
characteristic ‘‘tree in bud’’ pattern; and ‘‘indirect signs’’ original, limited definition of small airways disease by
of fibrotic narrowing of small airways, including areas of Hogg and colleagues has given way during the years to an
reduced lung density, within which there is pulmonary expanded scope of diseases affecting the airways that are
vessel constriction, bronchial wall thickening, and bron- considered in various classification schemes as small
chiectasis.14–20 In contrast, the pathologists’ study of small airways disease. Because classifications of lung diseases
airways disease is histology-based.7,21–29 Depending on are in some respects dynamic and overlapping, classifica-
how broadly or narrowly one defines the term, there are a tions of small airways disease vary. There have been
variable number of diseases that may fall under the several proposed classifications of small airways disease,
heading of small airways disease, including those primary including, for example, one of the initial classifications by
to the bronchioles and those involving the bronchioles Myers and Colby in 1993 (Table 1) and a relatively recent
secondarily, with bronchiolar involvement only one of 2006 classification by Katzenstein (Table 2).17,23,27,30,31 An-
several features of the disease. Further, as stated by other recent classification that is descriptive of the various
pathologic patterns is listed in Table 3. One might classify
Accepted for publication September 8, 2009. these diseases according to whether the histologic
From the Department of Pathology, The University of Texas Health patterns, along with clinical and radiologic correlation,
Science Center at Tyler. show changes diagnostic of a particular disease; however,
The author has no relevant financial interest in the products or except for diffuse idiopathic neuroendocrine cell hyper-
companies described in this article.
Reprints: Timothy Craig Allen, MD, JD, Department of Pathology, The plasia and diffuse panbronchiolitis, and arguably follicu-
University of Texas Health Science Center at Tyler, 11937 Highway lar bronchiolitis and respiratory bronchiolitis-interstitial
271, Tyler, TX 75708-3154 (e-mail: timothy.allen@uthct.edu). lung disease, the histologic changes, such as cellular
702 Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—Allen
Table 1. Classification of Small Airways Disease, 1993a Table 3. Classification of Small Airways Disease, 2008a
Acute (infectious) bronchiolitis Cellular bronchiolitis
Bronchiolitis obliterans-organizing pneumonia; cryptogenic Acute bronchiolitis
organizing pneumonia Acute and chronic bronchiolitis
Constrictive (obliterative) bronchiolitis; bronchiolitis obliterans Chronic bronchiolitis, with or without fibrosis
Adult bronchiolitis Subtypes of cellular bronchiolitis
Respiratory (smoker’s) bronchiolitis-associated interstitial lung Follicular bronchiolitis
disease Diffuse panbronchiolitis
Mineral dust airways disease Bronchiolitis obliterans with intraluminal polyps
Follicular bronchiolitis Constrictive bronchiolitis
Diffuse panbronchiolitis Respiratory bronchiolitis
a Mineral dust-associated airway disease
Data were derived from Myers and Colby.23
Peribronchiolar metaplasia
Bronchiolocentric nodules
bronchiolitis and fibrotic changes, are typically not Asthmatic-type changes
specific for a distinctive etiology. One could also classify Chronic bronchitis/emphysema-associated small airways
changes
small airways diseases for whether the disease is primary
a
to the small airways or secondary to other lung disease, Data were derived from Cagle et al.39
such as smoking or asthma. Ultimately, what classification
scheme one prefers is less important than an understand-
mucosa to mucosa) diameter. In terms perhaps more
ing of the histologic features, the disease processes
useful for the pathologist on a daily basis, the term small
involved, the limitations of histologic diagnosis, and the
airways includes membranous bronchioles, respiratory
confidence one can make a specific diagnosis on a biopsy
bronchioles, and alveolar ducts29,36 (Figures 1 and 2).
of small airways disease.
Membranous bronchioles, bronchioles ranging from ap-
EVALUATION OF BIOPSIES WITH SMALL proximately 1 mm down to approximately 0.5 mm in
AIRWAYS DISEASE diameter, normally contain a layer of smooth muscle and a
layer of adventitia and are lined by ciliated columnar cells
Although small airways diseases as a group are
and Clara cells. Smooth muscle is diminished distally.
relatively common, many patients have straightforward
They lack cartilage and may contain rare goblet cells or
clinical and radiologic diagnoses and are treated without
seromucinous glands. The final generation of membranous
biopsy confirmation of the disease. Pulmonologists
bronchiole is termed terminal bronchiole and opens into a
performing bronchoscopy typically focus on biopsying
functional unit of the lung termed an acinus, which is
discrete masses rather than diseases that involve a diffuse
composed of respiratory bronchioles, alveolar ducts, and
but relatively peripheral portion of the pulmonary
alveoli. Another functional unit, the lobule, is composed of
airways. Features of the various small airways diseases
approximately 3 to 10 acini, enclosed by an interlobular
overlap, and a firm diagnosis may not be possible on
septum. Respiratory bronchioles have alveoli budding
limited endobronchial or transbronchial biopsy tissue,
from their walls, the number of which increases distally.
and diagnoses are often descriptive rather than specifi-
They are lined by columnar or simple cuboidal epitheli-
cally diagnostic of a specific entity. Clinical and radiologic
um.26 Small airways have been termed the lung’s ‘‘Achilles
correlation is necessary to provide the most accurate
heel’’ because of their importance in airflow and air
diagnosis.
distribution and their lack of bronchilike rigidity to protect
Small airways may be involved with disease primarily
them from collapsing during exhalation, especially when
or may be involved secondarily by diseases primarily
involved with disease.37
affecting bronchi or lung parenchyma. Although etiologies
The following is a nonexhaustive review of the
are numerous, small airways disease may be generally
pathology of some of the small airways diseases,
divided into small airways disease related to tobacco; to
specifically cellular bronchiolitis, including follicular
various other exposures, including mineral dusts; to
bronchiolitis and diffuse panbronchiolitis; granulomatous
diseases involving other areas of the lung, with secondary
bronchiolitis; tobacco smoke-associated small airways
bronchiolar involvement; and to idiopathic causes. In some
bronchiolitic diseases, hypersensitivity pneumonitis; or-
cases, small airways disease may be extremely subtle
ganizing pneumonia; constrictive bronchiolitis; mineral
histologically and can be missed on examination.22,24
dust exposure and various other exposure-associated
Although occasionally small airways have been described
bronchiolitic diseases; and 4 recently described bronchio-
with sizes other than less than 2 mm,32 small airways are
litic disorders, bronchiolitic disease due to ingestion of
currently defined as airways having a diameter of less than
Sauropus androgynus, airway-centered interstitial fibrosis,
2 mm.7,27,33–35 It is important to keep in mind that the less
idiopathic bronchiolocentric interstitial pneumonia, and
than 2-mm measurement is of luminal (ie, measuring from
bronchiolitis interstitial pneumonitis.
BRONCHIOLITIS
Table 2. Classification of Small Airways Disease, 2006a
The term bronchiolitis is a generic term used clinically
Cellular bronchiolitis
Constrictive bronchiolitis obliterans to define a variety of inflammatory conditions involving
Nonspecific chronic bronchiolitis the small airways. Bronchiolar and peribronchiolar
Respiratory (smoker’s) bronchiolitis inflammation may be focal or diffuse and may or may
Follicular bronchiolitis not be associated with scarring and bronchiolar metapla-
Diffuse panbronchiolitis sia. Bronchiolar mucosa may undergo bronchiolar, squa-
a
Data were derived from Katzenstein.27 mous, or goblet cell metaplasia.
Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—Allen 703
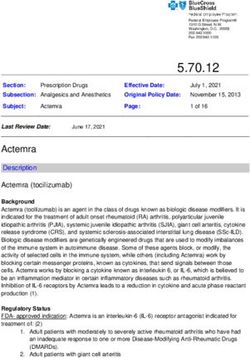
Figure 1. Medium-power image of membranous bronchiole with associated blood vessel and lymphatic vessel. Ciliated columnar cells line the airspace, beneath which is a thin layer of smooth muscle (hematoxylin-eosin, original magnification 320). Figure 2. Medium-power image of respiratory bronchiole with associated blood vessel. Simple cuboidal epithelial cells line the airway, and alveoli bud off of the airway wall. The respiratory bronchiole ends in an alveolar duct (hematoxylin-eosin, original magnification 320). Figure 3. Medium-power image of lambertosis, showing bronchiolar-type epithelium lining alveolar surfaces adjacent to the bronchiole (hematoxylin-eosin, original magnification 310). 704 Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—Allen
Peribronchiolar Metaplasia infiltrate23,24,39,66–72 (Figure 5). Most cases are treated symp-
Bronchiolar-type epithelium that grows along the tomatically, with generally excellent prognosis. Rare cases
alveolar surfaces adjacent to bronchioles has been termed exhibit long-term morbidity or mortality. In a small
peribronchiolar metaplasia or lambertosis, in reference to number of patients, long-term disease results in constric-
the canals of Lambert through which bronchiolar epithe- tive bronchiolitis. Drug treatments have not shown
lium was once considered to traverse to grow on alveolar convincing benefit; however, oxygen is generally admin-
septa21,29,38–41 (Figures 3 and 4). Peribronchiolar metaplasia istered in cases with significant hypoxia. Home oxygen
may be present in a variety of processes involving the therapy is being more frequently used to reduce hospital
small airways. Bronchiolarization may occur in the setting stay. Also, corticosteroids have reportedly shown benefit
of healed bronchiolitis or interstitial fibrosis and may also in some patients with croup, and nebulized saline has
be found in association with chronic hypersensitivity been reported to reduce morbidity and length of hospital
pneumonitis, constrictive bronchiolitis, or bronchiectasis. stay in patients with acute bronchiolitis.4 It is uncertain
Idiopathic foci of peribronchiolar metaplasia may also be what factors contribute to disease severity in infants;
found; these may represent healed sites of prior infection however, cell-mediated immune response to disease
or other localized injury. pathogenesis has been implicated. Recent studies have
estimated that 22% of cases in infants have a hereditary
CELLULAR BRONCHIOLITIS contribution to disease severity. Increased risk of severe
The term cellular bronchiolitis describes disease in acute respiratory syncytial virus bronchiolitis has been
which the primary pattern is an inflammatory infiltrate reported to correspond to a haplotype at the IL13-IL4
within the bronchioles. The inflammatory infiltrate may locus that is associated with increased interleukin (IL)-13
be acute, chronic, or both acute and chronic and may or production. Interleukin-8 levels have been reported to
may not be associated with peribronchiolar fibrosis or correlate with length of hospitalization, and IL-8 associ-
metaplasia.39,42 ated airway inflammation has been reported to relate
significantly to the severity of acute epidemic bronchi-
Acute Bronchiolitis olitis.45,51,65,66 Acute bronchiolitis in adults has a variety of
Acute bronchiolitis is most commonly found in infants potential causes, as listed in Table 4.
and young children.43–65 It is the most common respiratory
Acute and Chronic Bronchiolitis
ailment during the first year of life. Its etiology is generally
infectious, and although approximately three-fourths of Acute and chronic bronchiolitis is generally found in
cases are due to respiratory syncytial virus, numerous adults, and potential etiologies are numerous (Table 5).
other infections may be causative, including other viruses Although many cases are caused by infections, including
such as measles, adenovirus, influenza, and parainfluen- respiratory syncytial virus, other noninfectious etiologies
za; nonviral organisms such as fungi and mycoplasma; exist. Some cases are idiopathic.23,24,39,45,66–72 Patients often
and Bordetella pertussis.* It occurs most frequently during have mild symptoms but may present with shortness of
the winter months. Infants often present with tachypnea, breath of variable duration, with or without cough.
wheezing, and tachycardia, with more severely ill patients Pulmonary function tests may show an obstructive
exhibiting chest retraction and nasal flaring. Lung pattern.68,71,72 Histologically, bronchiolar lumen contain
hyperinflation is often found on x-ray. Some cases may purulent exudative material and sloughed bronchiolar
show patchy ground glass opacities or small centrilobular mucosal cellular debris and variable amounts of mucus,
nodules as well. High-resolution chest CT scan may show and bronchiole mucosa and walls contain a mixed
branching linear opacities or small centrilobular nodules. neutrophilic infiltrate and chronic inflammatory cell
Focal areas of nodularity may be present, representing foci infiltrate made up predominantly of lymphocytes and
of bronchopneumonia. In obvious cases of acute bronchi- plasma cells. The mixed acute and chronic inflammatory
olitis, chest radiology is more frequently being omitted.3 cell infiltrate extends into peribronchiolar tissue, and
Patients typically do not undergo open biopsy; however, edema may be present.23,24,39,67,68,71,72 In patients with
biopsy may be obtained in some cases having unusual disease caused by respiratory syncytial virus, various
presentations. Histologically, acute bronchiolitis consists chemokines, including regulated upon activation, normal
of bronchioles filled with necrotic debris and purulent T cell expressed and secreted; IL-8; IL-1; and IL-6 have
exudative material, as well as sloughed bronchiolar been implicated in recruitment and activation of inflam-
mucosal cells. The residual bronchiolar mucosa and matory cells, including neutrophils, macrophages, lym-
surrounding bronchiolar wall contain a neutrophilic phocytes, and eosinophils, to the infected area.65,69,70,72
Most patients have a good prognosis with generally full
*References 39, 42–49, 52, 55, 61, 63, 64, 66.
3References 39, 42, 43, 47, 52, 54–56, 62, 64, 66. 4References 42–44, 47, 52, 53, 55, 56, 59, 60, 73–79.
r
Figure 4. High-power image of lambertosis, showing ciliated cuboidal to low columnar epithelium lining alveolar septa (hematoxylin-eosin,
original magnification 340).
Figure 5. Medium-power image of acute bronchiolitis, with necrotic epithelial cells and neutrophils within the bronchiolar lumen and a
neutrophilic infiltrate involving the bronchiolar wall (hematoxylin-eosin, original magnification 320).
Figure 6. Low-power image of follicular bronchiolitis showing peribronchiolar lymphoid hyperplasia that extends into surrounding lung
parenchyma (hematoxylin-eosin, original magnification 34).
Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—Allen 705Table 4. Potential Etiologies of Acute Bronchiolitisa Table 5. Potential Etiologies of Acute and
Chronic Bronchiolitisa
Viral infection
Bacterial infection Viral infection
Acute exposure to fumes and toxins Bacterial infection
Local changes of acute bronchopneumonia Mycoplasma infection
Wegener granulomatosis (rarely) Hypersensitivity pneumonitis
a Respiratory bronchiolitis
Data were derived from Cagle et al.39
Aspiration pneumonia
Pulmonary involvement with collagen vascular disease
Posttransplantation, graft-versus-host disease
recovery. Patients with idiopathic disease may show Wegener granulomatosis
therapeutic response to antibiotics and immunosuppres- Bronchocentric granulomatosis
Diffuse panbronchiolitis
sive drugs; however, in these patients residual pulmonary Inhalation of fumes and toxins
impairment is frequent.39,66,70–72 Asthma
Inflammatory bowel disease-related small airways disease
Chronic Bronchiolitis Idiopathic
Chronic bronchiolitis describes a histologic pattern in a
Data were derived from Cagle et al.39
which bronchioles contain, and peribronchiolar tissues are
infiltrated with, chronic inflammatory cells. Germinal Eosinophilic Bronchiolitis
centers and constrictive bronchiolitis may or may not be
present, and if germinal centers predominate and con- Eosinophilic bronchiolitis is characterized histologically
striction of the airway lumen is significant, the diagnosis by bronchiolar walls containing increased numbers of
of follicular bronchiolitis should be considered. The eosinophils. Its presence may be secondary to asthma or
histologic features of acute and chronic bronchiolitis allergic bronchopulmonary aspergillosis, although pa-
may overlap with chronic bronchiolitis.24,39,71,72 Chronic tients with these diseases usually have increased eosino-
bronchiolitis may be a feature of various diseases (Table 6) phils within bronchi rather than bronchioles. Eosinophilic
and may be idiopathic.39,71,72 Fibrosis may or may not be pneumonia, drug reactions, and parasitic or fungal
present in association with chronic bronchiolitis. The infections may also occasionally exhibit eosinophilic
presence of fibrosis suggests some amount of irreversibil- bronchiolitis, but there is usually a predominant intersti-
ity of the process. Although chronic bronchiolitis with tial disease component present.95–99 One patient with a
fibrosis is a common feature of chronic obstructive prior diagnosis of diffuse panbronchiolitis and worsening
pulmonary disease, the lesion is rarely biopsied in that symptoms despite therapy subsequently was diagnosed
setting. as having eosinophilic bronchiolitis.96
Bronchiolar Necrosis Diffuse Panbronchiolitis
Histologically, bronchiolar necrosis describes mucosal Diffuse panbronchiolitis, an idiopathic, bilateral, pro-
necrosis and sloughing of mucosa into the airway lumen, gressive, obstructive, suppurative small airways disease
with or without necrosis of the bronchiolar wall.39 associated with sinusitis, primarily occurs in Japan, has
Bronchiolar necrosis may be identified in a variety of been increasingly identified within other Asian popula-
diseases, including infections (Table 7). tions, and is uncommon in the United States.29,100–126 The
term diffuse panbronchiolitis refers to its distribution in
Follicular Bronchiolitis both lungs (diffuse) and the inflammatory involvement of
Follicular bronchiolitis consists of lymphoid hyperpla- all layers of the wall or respiratory bronchioles (pan).122
sia of the bronchus-associated lymphoid tissue.29,80–90 It is Because diffuse panbronchiolitis is predominantly found
caused by altered immune response or immune stimulus in Japan, a genetic predisposition is assumed to play a role
of the bronchus-associated lymphoid tissue and is a in disease progression. Human leukocyte antigen alleles
feature of various immune-related disorders involving are thought to cause a genetic predisposition to diffuse
the lungs, including collagen vascular diseases, especially panbronchiolitis. Researchers have shown an association
rheumatoid arthritis and Sjögren syndrome; bronchiecta- with HLA-Bw54, found predominantly among East
sis and middle lobe syndrome; hypersensitivity reactions; Asians, and diffuse panbronchiolitis, with 63% of Japa-
and various types of immune deficiency states such as nese patients possessing the antigen compared with 11%
AIDS and congenital immunodeficiency disorders. Some of control subjects. Korean patients have been shown to
cases are idiopathic.29,80–83,85–89,91–93 It has been reported to have an association with HLA-A11. These findings
cause posttransplantation bronchiolitis obliterans syn- suggest a major HLA susceptibility gene for diffuse
drome.84 Radiologic features include reticulonodular panbronchiolitis.122,126–130 Patients average approximately
infiltrates or small nodules on chest x-ray. High-resolution 40 years of age at presentation; however, there is a wide
CT scan may show peribronchial nodules, with or without age range from the first to the seventh decades of life.
patchy ground glass opacities. Histologically follicular Males predominate, with a male to female ratio in Japan
bronchiolitis is characterized by peribronchiolar lym- reportedly between 1.4:1 and 2:1. No association with
phoid hyperplasia that extends into surrounding lung smoking or exposure to fumes or toxins has been proven.
parenchyma. Reactive germinal centers are present29,72 Patients typically present with a variable history of
(Figure 6). Therapy depends on the underlying causative chronic sinusitis, cough, and dyspnea. Some patients
process. Overall prognosis has been reported to be may produce purulent sputum. Pulmonary function
good.29,39,83,84,90 Patients with idiopathic disease may benefit studies show obstructive changes. Radiographically,
from steroids and bronchodilators.72,80–83,93,94 diffuse panbronchiolitis produces bilateral small nodules
706 Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—AllenTable 6. Potential Etiologies of Chronic Bronchiolitisa Table 7. Potential Etiologies of Bronchiolar Necrosisa
Infection Viral infections
Collagen vascular disease Adenovirus
Posttransplantation graft-versus-host disease Herpes virus
Inflammatory bowel disease-related small airways disease Influenza
Hypersensitivity pneumonitis Bronchocentric fungal infections
Pulmonary Langerhans cell histiocytosis Bacterial infections
Aspiration pneumonia Bronchocentric granulomatosis
Diffuse panbronchiolitis Exposure to fumes and toxins
Distal to bronchiectasis Wegener granulomatosis
Lymphoproliferative disorders a
Data were derived from Cagle et al.39
Local inflammatory reaction such as with middle lobe syndrome
Asthma
Chronic obstructive pulmonary disease disorders (Table 8).39,143–155 Clinical, radiologic, therapeu-
Idiopathic tic, and prognostic features are those of the underlying
a
Data were derived from Cagle et al.39 disease. Although not diagnostic, well-formed noncaseat-
ing granulomas suggest sarcoidosis; caseating granulo-
on x-ray and centrilobular lesions on high-resolution CT mas suggest infection; poorly formed nonnecrotizing
scan.1 On biopsy, yellow bronchiolocentric nodules granulomas, especially in association with interstitial
measuring approximately 1 mm to 3 mm are identified. lymphocytic infiltrates or organizing pneumonia, suggest
Histologically, diffuse panbronchiolitis is characterized by hypersensitivity pneumonitis; and noncaseating granulo-
transmural infiltration of the bronchiole and surrounding mas with associated foreign body giant cells or foreign
lung interstitium with foamy macrophages, plasma cells, material suggest aspiration pneumonia.
and lymphocytes. The changes involve terminal bronchi-
oles, respiratory bronchioles, and alveolar ducts. Predom- ORGANIZING PNEUMONIA WITH INTRALUMINAL
inantly respiratory bronchiole involvement is a distinctive POLYPS (BRONCHIOLITIS OBLITERANS WITH
feature of diffuse panbronchiolitis, as other forms of INTRALUMINAL POLYPS) (FORMERLY TERMED
constrictive bronchiolitis predominantly affect membra- BRONCHIOLITIS OBLITERANS ORGANIZING
nous bronchioles.122,133 Foamy macrophages and other PNEUMONIA/ORGANIZING PNEUMONIA PATTERN)
inflammatory cells may fill the bronchiolar lumen and Organizing pneumonia with intraluminal polyps, for-
may involve alveolar spaces; however, alveoli are rela- merly termed bronchiolitis obliterans organizing pneu-
tively spared in diffuse panbronchiolitis (Figure 7). monia/organizing pneumonia pattern, may occur sec-
Neutrophils may be identified in the bronchiolar lumen ondary to a wide variety of lung injuries (Table 9).29,39,156–186
as well. Follicular bronchiolitis can occur as part of the It may also be idiopathic, termed cryptogenic organizing
histologic changes, and superimposed acute or organizing pneumonia, formerly termed idiopathic bronchiolitis
pneumonia and bronchiectasis may be present. Terminal obliterans organizing pneumonia.44 Histologically, orga-
bronchioles may become ectatic as the disease advances. nizing pneumonia is characterized by plugs of granulation
Untreated disease generally progresses to bronchiectasis, tissue, composed of fibroblasts within a myxoid or
with resultant respiratory failure and death.122,125,126,134,135 edematous stroma, which are located within bronchiolar
Patients typically have associated infections, and Pseudo- lumens, alveolar ducts, and associated alveolar airspaces
monas infection is associated with a poor prognosis. (Figure 9). Within airspaces, these plugs of granulation
Significantly improved survival has been reported in tissue may form rounded nodules, termed Masson bodies.
patients treated with chronic low-dose macrolide antibi-
A variable interstitial lymphocytic infiltrate may be
otic therapy, with improved survival considered to be
present. If bronchiolar obstruction is a feature of the
caused by the drug’s antiinflammatory affects rather than
disease, foamy macrophages may be present within
its antibiotic properties.** Diagnosis is generally made
alveolar airspaces. Clinical history is often necessary to
based on the disease’s clinical, radiographic, and histo-
determine the etiology; however, histologic features that
logic features. Isolation from the sputum of Haemophilus
influenza and Streptococcus pneumoniae, and in advanced assist in specific diagnosis include viral inclusions
stages of disease, Pseudomonas aeruginosa, assists in suggestive of viral pneumonia, foreign body giant cells
making the diagnosis.122,126,134 Differential diagnosis in- suggestive of aspiration, and poorly formed granulomas
cludes xanthomatous bronchiolitis, rheumatoid arthritis- with multinucleated giant cells suggestive of hypersensi-
associated bronchiolitis and other collagen vascular tivity pneumonia. Typically, organizing pneumonia re-
disease and autoimmune diseases, human T-cell lympho- solves with no or minimal scarring; however, clinical
tropic virus type 1-associated bronchiolitis, and idiopathic course and prognosis depend on the type of and severity
bronchiolitis.33 of the underlying disease.29,39,156–186 If, after clinical corre-
lation and careful histologic examination for viral inclu-
GRANULOMATOUS BRONCHIOLITIS sions, foreign body giant cells, and poorly formed
Granulomatous bronchiolitis is characterized histolog- granulomas with associated giant cells, no etiology is
ically by granulomas within bronchiolar walls, with or determinable, the diagnosis of cryptogenic organizing
without giant cells or necrosis39 (Figure 8). Granuloma- pneumonia is appropriate. Cryptogenic organizing pneu-
tous bronchiolitis is a feature of a variety of pulmonary monia is a clinical syndrome generally occurring in
middle-aged to older women who often present with a
history of flulike illness and have shortness of breath and
1References 116–118, 120–126, 131–133.
**References 29, 122, 123, 125, 126, 136–138.
33References 122, 125, 126, 131, 139–142. 44References 29, 39, 156–178, 180, 181, 184–186.
Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—Allen 707Figure 7. High-power image of diffuse panbronchiolitis showing infiltration of foamy macrophages within the bronchiolar wall (hematoxylin- eosin, original magnification 340). Figure 8. Medium-power image of granulomatous bronchiolitis showing a nonnecrotizing granuloma adjacent to a membranous bronchiole in a patient with sarcoidosis (hematoxylin-eosin, original magnification 320). Figure 9. Medium-power image of organizing pneumonia showing a plug of granulation tissue lying within an alveolar duct (hematoxylin-eosin, original magnification 320). 708 Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—Allen
persistent nonproductive cough. Radiologically, patchy cellular infiltrates made up predominantly of lympho-
bilateral alveolar infiltrates may occur transiently and cytes and histiocytes within the bronchioles and infiltrat-
recur in different locations. Therapeutic response to ing into surrounding peribronchiolar tissue. Lying within
steroid therapy, and prognosis, are usually very good in the bronchiolar lumen and also within adjacent alveolar
patients with cryptogenic organizing pneumonia.11 ducts and alveoli, there are collections of macrophages
containing finely granular brown cytoplasmic pigment
CONSTRICTIVE BRONCHIOLITIS (Figure 10). Pigment-laden macrophages are also often
Constrictive bronchiolitis, also termed bronchiolitis found within the bronchiolar wall. Minimal to mild
obliterans and obliterative bronchiolitis, is an obstructive fibrosis may occur in the bronchial wall and adjacent
small airways disease identified in a variety of disorders alveolar septa. Metaplastic bronchiolar epithelium (lam-
(Table 10). Constrictive bronchiolitis is strongly associated bertosis) and type II pneumocyte hyperplasia may be
with chronic lung transplant rejection, for which it is a present. Membranous bronchiolitis may contain smooth
significant cause of morbidity and mortality. It may also muscle hyperplasia and adventitial fibrosis39 (Figure 11).
occur as idiopathic disease, predominantly presenting as Patients are typically asymptomatic; however, they often
persistent cough and dyspnea, in middle-aged to older show obstructive changes on pulmonary function tests.
women who are never-smokers. Patients with idiopathic The diagnosis is often made incidentally, and prognosis in
constrictive bronchiolitis have variable prognoses, ranging these patients is excellent with smoking cessation, with or
from slowly progressive disease to rapidly deteriorating without corticosteroid therapy.29,39,206–208 These histologic
disease.*** Histologically, constrictive bronchiolitis is changes are on a continuum, and when severe enough,
characterized by concentric bronchiolar lumen narrowing changes of respiratory bronchiolitis are termed respiratory
by submucosal fibrous tissue. The lumen narrowing may bronchiolitis-associated interstitial lung disease (RBILD).
range from slight and histologically subtle to marked, with
complete obliteration of the bronchiolar lumen leaving Respiratory Bronchiolitis-Associated Interstitial
only a residual fibrous scar (Figures 13 and 14). Chronic Lung Disease
inflammation may or may not be present in constrictive
Patients with respiratory bronchiolitis histologically,
bronchiolitis, and patients with idiopathic disease often
have little or no chronic inflammation within bronchiolar who are typically heavy smokers, with generally mild
walls or peribronchiolar tissues. Smooth muscle hyperpla- nonprogressive symptoms of dyspnea and cough, and
sia and adventitial fibrosis may occur in membranous with radiologic changes of interstitial lung disease, are
bronchioles. The plugs of granulation tissue found with diagnosed as having RBILD.444 The differential diagnosis
organizing pneumonia with intraluminal polyps are not a of respiratory bronchiolitis and RBILD is generally based
characteristic of constrictive bronchiolitis.333 on clinical and radiologic features. Some cases have been
reported in nonsmokers, and similar histologic features
TOBACCO SMOKE-ASSOCIATED have been seen in patients with asbestos and nonasbestos
BRONCHIOLITIC DISEASES mineral dust exposure.207,221 Chest x-ray results may be
Membranous Bronchiolitis and Respiratory Bronchiolitis normal or may show fine reticulonodular interstitial
opacities, corresponding to fibrosis involving the subpleu-
Variably extensive and variably severe inflammatory ral alveolar septa, that may be diffuse or predominate
and fibrotic changes caused by tobacco smoke that are within the lung bases. High-resolution CT scan shows
found in the terminal bronchioles and respiratory bron- ground glass opacities, centrilobular nodules, and intersti-
chioles are termed, respectively, membranous bronchi- tial thickening with an upper lung zone predominance.111
olitis and respiratory bronchiolitis.29,39,206–208 Patients are The histologic features of RBILD and respiratory bronchi-
typically asymptomatic, but pulmonary function studies
olitis are generally indistinguishable, although some cases
may show obstructive change.29,39,206–208 Other smoking-
of RBILD may show more pronounced changes. Histologic
related lung changes including chronic bronchitis, em-
diagnosis of RBILD requires more than mere collections of
physema, and desquamative interstitial pneumonia may
pigmented macrophages within bronchiolar airspaces, as
be present along with membranous bronchiolitis and
may be seen in healthy cigarette smokers.29,39,207,208 More
respiratory bronchiolitis. Histologically, both membra-
nous bronchiolitis and respiratory bronchiolitis contain pronounced cases of RBILD merge in the continuum with
cases of desquamative interstitial pneumonia29 (Figure 12).
11References 29, 39, 156–177, 179–181, 185, 187, 188.
***References 11, 15, 29, 39, 67, 71, 84, 189–203. 444References 14, 29, 38, 39, 206–220.
333References 29, 39, 67, 71, 189, 190, 192–194, 204, 205. 111References 14, 206–208, 210, 212, 222–224.
r
Figure 10. Medium-power image of respiratory bronchiolitis showing macrophages containing finely granular brown cytoplasmic pigment lying
within bronchiolar lumen and wall, as well as within surrounding peribronchiolar alveolar airspaces (hematoxylin-eosin, original
magnification 320).
Figure 11. Medium-power image of respiratory bronchiolitis showing membranous bronchiole with prominent smooth muscle hyperplasia
(hematoxylin-eosin, original magnification 320).
Figure 12. Low-power image of respiratory bronchiolitis-associated interstitial lung disease showing extension of pigmented macrophages
diffusely within surrounding alveolar airspaces, in a continuum with desquamative interstitial pneumonia (hematoxylin-eosin, original
magnification 34).
Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—Allen 709Table 8. Potential Etiologies of Table 9. Potential Etiologies of Organizing
Granulomatous Bronchiolitisa Pneumonia With Intraluminal Polypsa
Fungal infections Diffuse alveolar damage, organizing
Mycobacterial infections, including atypical mycobacterial Aspiration pneumonia, organizing
infections Resolving infections
Hypersensitivity pneumonitis Postobstruction organization
Sarcoidosis Hypersensitivity pneumonitis
Aspiration pneumonia Organization after exposure to fumes and toxins
Bronchocentric granulomatosis Collagen vascular disease
Crohn disease Acute lung transplant rejection
Wegener granulomatosis Drug reactions
Hard metal disease Secondary to bone marrow transplantation or other organ
a transplantation
Data were derived from Cagle et al.39
Reaction to radiation therapy or chemotherapy
Chronic eosinophilic pneumonia
Pulmonary Langerhans Cell Histiocytosis Secondary reaction with chronic bronchiolitis
Reparative process adjacent to abscess, necrotic tumor, infarct, etc
Pulmonary Langerhans cell histiocytosis commonly arises Secondary to a hematologic disorder
within a background of respiratory bronchiolitis and should Inflammatory bowel disease-related small airways disease
be considered as a possible concurrent disease process in Wegener granulomatosis
patients with respiratory bronchiolitis.39,225 Pulmonary Lan- Idiopathic
gerhans cell histiocytosis has recently been reviewed.226 a
Data were derived from Cagle et al.39
HYPERSENSITIVITY PNEUMONITIS (EXTRINSIC
ALLERGIC ALVEOLITIS) thickened bronchioles. Acutely, histologic changes in-
Although late-stage hypersensitivity pneumonitis can clude necrotic bronchiolar mucosa with a neutrophilic
mimic usual interstitial pneumonia and nonspecific infiltrate and sloughing. Pulmonary edema and changes
interstitial pneumonia, in earlier stage hypersensitivity of diffuse alveolar damage may also be present to variable
pneumonitis cellular bronchiolitis is one of its character- degrees. The acute stage is followed by an organizing
istic histologic features, along with organizing pneumonia stage characterized histologically by organizing pneumo-
and poorly formed nonnecrotizing granulomas.29,39,227 nia (organizing pneumonia with intraluminal polyps).
Hypersensitivity pneumonitis is often in the differential Patients who progress beyond the acute and organizing
diagnosis of cellular bronchiolitis, with and without stages of disease often recover without long-term lung
fibrotic changes. Detailed reviews of hypersensitivity changes. Some patients may, however, progress chroni-
pneumonitis have been recently published.228–231 cally and show constrictive bronchiolitis. Numerous
chemicals may cause bronchiolitic disease, including
MINERAL DUST-ASSOCIATED AND VARIOUS OTHER smoke, chlorine gas, phosgene, and hydrogen fluoride,
EXPOSURE-RELATED BRONCHIOLITIC DISEASES among others. Reports have recently shown that the
Mineral Dust-Associated Bronchiolitic Diseases inhalation of volatile diacetyl as part of the popcorn
manufacturing process has caused bronchiolitis, frequent-
Numerous mineral dust-associated airway diseases, ly constrictive bronchiolitis, in some workers. Other
including asbestosis, silicosis, and coal miner’s pneumo- exposures may also cause bronchiolitis, including fiber
coniosis, among others, may cause bronchiolitic dis-
inhalation in the nylon flocking industry. Recent reports
ease.29,39,67,232–257 The histologic changes typically consist of
have shown that some workers involved with flocking, in
varying degrees of fibrosis that ultimately may obstruct
which short synthetic fibers are applied to a backing
and completely occlude the airway. The exact histologic
fabric, have been diagnosed with chronic bronchiolitis,
pattern depends on the specific dust being inhaled and the
often follicular bronchiolitis (Figure 15). Toxin and fume
amount of dust inhaled. Care must be taken to make a
exposure may also show histologic features of organizing
correct diagnosis, and clinical and radiologic correlation is
necessary. For example, in some patients, especially heavy pneumonia with intraluminal polyps. That histologic
smokers, anthracotic pigment may be identified along pattern may predominate in cases of acute exposures.4444
alveolar ducts and respiratory bronchioles; however, there Drug Reactions
is typically less pigment deposition and less airway
fibrosis than in patients with mineral dust-associated A great number of drugs cause drug-induced pulmo-
bronchiolitic diseases.**** nary toxicity. There are several histologic patterns that
may occur, including diffuse alveolar hemorrhage, diffuse
Exposure to Fumes and Toxins alveolar damage, and nonspecific interstitial pneumonia.
The most serious pulmonary exposures characteristi- Bronchiolitic disease, including organizing pneumonia
cally cause overwhelming pulmonary edema, with or and hypersensitivity pneumonitis, may also occur as a
without diffuse alveolar damage, and frequently cause consequence of pulmonary drug reactions. Methotrexate
death. Lesser exposures to fumes and toxins may cause is one drug commonly associated with hypersensitivity
bronchiolitic disease.3333 Patients may have cough and pneumonitis-associated drug-induced lung injury, al-
dyspnea, as well as other symptoms such as vomiting, though many other drugs can give a similar histologic
dizziness, and headache. Radiographic studies may show pattern (Figure 16). Numerous drugs may cause an
organizing pneumonia pattern of injury.297–305
****References 29, 39, 67, 234, 236, 237, 239, 241, 244, 248, 250–
252, 254–257. 4444References 29, 39, 196, 197, 201, 244, 261, 263, 265, 267, 268,
3333References 29, 39, 196, 197, 201, 244, 258–296. 271, 273, 274, 279–281, 283, 284, 286–296.
710 Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—AllenTable 10. Potential Etiologies of described histologically centrilobular and bronchiolo-
Constrictive Bronchiolitisa centric fibrosis with patchy interstitial inflammation.
Granulomas are not characteristic of the process. Patients
Post lung transplantation
reportedly were predominantly middle-aged women.
Post bone marrow transplantation
Healed infection, especially adenovirus infection Prognosis was generally guarded, with 33% of patients
Drug reactions dead of disease and 56% alive with persistent progressive
Healed injury from exposure to fumes and toxins disease, with a mean follow-up period of 4 years with 9
Collagen vascular disease, especially rheumatoid arthritis patients. Compared with airway-centered interstitial
As a component or complication of: fibrosis, idiopathic bronchiolocentric interstitial pneumo-
Bronchiectasis
nia has a more substantial interstitial inflammatory
Cellular bronchiolitis
Asthma infiltrate. The diagnosis of idiopathic bronchiolocentric
Chronic bronchitis interstitial pneumonia is controversial, and whether these
Cystic fibrosis patients represent cases of hypersensitivity pneumonitis
DIPNECH or carcinoid tumorlets or nonspecific interstitial pneumonia remains to be
Inflammatory bowel disease-associated small airways disease determined. Differential diagnosis also includes usual
Idiopathic
interstitial pneumonia and RBILD.29,312–314
Abbreviation: DIPNECH, diffuse idiopathic neuroendocrine cell Fukuoka et al315 reported 15 cases of peribronchiolar
hyperplasia. metaplasia-related interstitial lung disease. These cases
a
Data derived from Cagle et al.39 differed from those reported by Churg et al and Yousem et
al in that although the patients had interstitial lung disease
OTHER BRONCHIOLITIC DISEASES clinically, the primary histologic finding on biopsy was
peribronchiolar metaplasia. The authors designated this
Finally, there are a few related relatively recently
finding peribronchiolar metaplasia-related interstitial lung
described bronchiolitic diseases that bear some discussion.
disease because of the analogy with respiratory bronchi-
Airway-Centered Interstitial Fibrosis, Idiopathic olitis and RBILD, in which respiratory bronchiolitis is a
Bronchiolocentric Idiopathic Pneumonia, and common incidental finding in smokers and RBILD is the
Peribronchiolar Metaplasia–Related Interstitial Lung Disease smoking-associated clinically significant interstitial lung
disease.315 The authors noted that although the cases
Three recently described airway-centered entities, possi- reported by Churg et al and Yousem et al contained cases
bly representing similar manifestations or differing points with peribronchiolar metaplasia, their cases did not have
of progression of the same disease or group of diseases, other features found in the cases reported by Churg et al
include airway-centered interstitial fibrosis, idiopathic and Yousem et al, including significant interstitial fibrosis
bronchiolocentric idiopathic pneumonia, and peribronchio- beyond the peribronchiolar region. The authors suggested
lar metaplasia-related interstitial lung disease. that the better prognosis identified in their cases relative to
Airway-centered interstitial fibrosis is the term used by those of Churg et al and Yousem et al may be related to the
Churg et al306 in 2004 to describe the histologic features of absence of significant interstitial fibrosis beyond the
interstitial fibrosis that is centered around bronchioles, peribronchiolar region.315 The authors note that peribron-
with associated peribronchiolar fibrosis extending into chiolar metaplasia frequently occurs as a histologic feature
surrounding lung parenchyma, increased bronchiolar in other interstitial lung diseases and that chronic
smooth muscle, and metaplastic bronchiolar epithelium hypersensitivity pneumonitis is the most important dif-
(lambertosis), with little interstitial inflammation.29,306–312 ferential diagnosis in cases with these histologic features.315
Increased alveolar macrophages and honeycombing are
not characteristics of airway-centered interstitial fibrosis. S androgynus Ingestion
This uncommon diagnosis remains controversial, as these Ingestion of S androgynus, a common Malaysian
histologic features may be due to other, established, vegetable also termed Sabah vegetable, was first associat-
diseases such as hypersensitivity pneumonitis and RBILD. ed with bronchiolitic disease in Taiwan and reported by
Whether airway-centered interstitial fibrosis ultimately is Lai et al316 and Lin et al317 in 1996.316–336 The plant was
classified as an individual, specific form of interstitial lung ingested as raw leaves or extract juice by predominantly
disease remains to be determined. Usual interstitial young to middle-aged women for the perceived weight
pneumonia and nonspecific interstitial pneumonia are loss benefit. Patients were reported to exhibit dyspnea and
also differential diagnoses in these patients. Lung injury cough with progressive respiratory failure developing.
due to environmental exposures has been proposed as a Some patients have died of disease. Cases have been
cause of disease. Patients reportedly are middle-aged, and reported in other countries, including Japan. Cause is
the majority are women. Chest x-rays generally show uncertain; however, T-cell mediated immunity is thought
peribronchial and perivascular fibrosis with interstitial to play a role in disease. Familial associations (mother and
thickening. Patients reportedly present with chronic daughter) have been identified. Intake cessation, cortico-
cough and progressive dyspnea. Treatment with bron- steroids, bronchodilators, cytotoxic agents, and plasma-
chodilators and corticosteroids has been generally unsat- pheresis have been attempted; however, lung transplan-
isfactory. Patients have a generally poor prognosis, with a tation has been considered to be the only effective
reported 40% dead of disease with follow-up periods of 1 treatment. Reports show histologic changes of segmental
to 10 years. Airway-centered interstitial fibrosis has necrosis of small bronchi with relative sparing of large
features in common with idiopathic bronchiolocentric bronchi, most bronchioles, and alveoli. As well, bronchial
interstitial pneumonia.29,306–312 arteries within walls of large bronchi show fibromuscular
Idiopathic bronchiolocentric interstitial pneumonia was sclerosis and obliteration. In some cases, constrictive
reported by Yousem and Dacic313 in 2002. The authors bronchiolitis and organizing pneumonia (organizing
Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—Allen 711Figure 13. Medium-power image of constrictive bronchiolitis, showing obliteration of bronchiolar lumen and scar formation (hematoxylin-eosin,
original magnification 320).
Figure 14. Medium-power image of constrictive bronchiolitis showing smooth muscle hyperplasia apparent on trichrome stain (original
magnification 320).
Figure 15. Medium-power image of a bronchiole with follicular bronchiolitis from a patient with flock lung (hematoxylin-eosin, original
magnification 320).
Figure 16. Medium-power image of a hypersensitivity pneumonitis-like pattern in a lung biopsy with a patient treated with methotrexate
(hematoxylin-eosin, original magnification 310).
pneumonia with intraluminal polyps) has been reported, bronchiolocentric interstitial pneumonia. Whether bron-
possibly representing indirect histologic changes.316–332,336 chiolitis interstitial pneumonitis is ultimately classified as
an individual, specific form of interstitial lung disease
Bronchiolitis Interstitial Pneumonitis remains to be determined, and further studies of cases
Bronchiolitis interstitial pneumonitis was described with these histologic features will help better characterize
recently by Mark and Ruangchira-urai.337 Histologically, these patients.
bronchiolitis interstitial pneumonitis reportedly shows
regional and occasionally widespread organizing pneu- CONCLUSION
monia with associated alveolar inflammation and alveolar Small airways diseases include a wide variety of
fibrosis in most cases. Many cases contained bronchiolar diseases of which the pathologist must consider. Although
scarring and mucus plugging, and some cases showed uncommon conditions such as diffuse idiopathic neuro-
purulent bronchiolitis. Differential diagnosis includes endocrine cell hyperplasia and diffuse panbronchiolitis
usual interstitial pneumonia, nonspecific interstitial pneu- have histologic features that allow for relatively specific
monia, organizing pneumonia, and constrictive bronchi- diagnoses, and although some conditions such as mineral
olitis, as well as the also recently described diagnoses of dust-associated small airways disease, RBILD, granulo-
airway-centered interstitial pneumonia and idiopathic matous bronchiolitis, eosinophilic bronchiolitis, and fol-
712 Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—Allenlicular bronchiolitis have histologic features that may be 24. Colby TV. Bronchiolitis. Pathologic considerations. Am J Clin Pathol.
1998;109:101–109.
diagnostic in the appropriate clinical and radiologic 25. Visscher DW, Myers JL. Bronchiolitis: the pathologist’s perspective. Proc
setting, most cellular and fibrotic changes found in small Am Thorac Soc. 2006;3:41–47.
airways disease are nonspecific. These nonspecific small 26. Tomashefski JF CP, Farver CF, Fraire AE, ed. Dail and Hammar’s
Pulmonary Pathology. 3rd ed. New York, NY: Springer; 2008.
airways findings are found in a variety of both primary 27. Katzenstein A-LA. Miscellaneous II: nonspecific inflammatory and
small airways diseases and diseases that affect the small destructive diseases. In: Katzenstein and Askin’s Surgical Pathology of Non-
airways secondarily, such as hypersensitivity pneumoni- Neoplastic Lung Disease. 4th ed. Philadelphia, PA: Elsevier; 2006:445–476.
tis, asthma, chronic obstructive pulmonary disease, and 28. Wang C-W, Muhm JR, Colby TV, Leslie KO. Small airway lesions. In:
Cagle PT, Allen TC, Beasley MB, eds. Diagnostic Pulmonary Pathology. 2nd ed.
Wegener granulomatosis. Diseases and conditions that are New York, NY: Informa; 2008:229–247.
not considered primarily pulmonary, such as collagen 29. Cagle PT. Color Atlas and Text of Pulmonary Pathology. 2nd ed.
vascular diseases, bone marrow transplantation, and Philadelphia, PA: Lippincott Williams & Wilkins; 2008.
30. Poletti V, Zompatori M, Cancellieri A. Clinical spectrum of adult chronic
inflammatory bowel disease, must also be considered in bronchiolitis. Sarcoidosis Vasc Diffuse Lung Dis. 1999;16:183–196.
patients with significant histologic changes in the small 31. Worthy SA, Muller NL. Small airway diseases. Radiol Clin North Am.
airways. More recently described entities such as airway- 1998;36:163–173.
centered interstitial fibrosis and bronchiolocentric inter- 32. James A, Carroll N. Transbronchial biopsy as a tool to evaluate small-
airways disease in asthma: cons. Eur Respir J. 2002;20:249–251.
stitial pneumonia must be further studied to determine 33. Vikgren J, Bake B, Ekberg-Jansson A, Larsson S, Tylen U. Value of air
whether these cases represent separate, independent trapping in detection of small airways disease in smokers. Acta Radiol. 2003;44:
diagnostic entities or whether they represent uncommon 517–524.
34. Sturton G, Persson C, Barnes PJ. Small airways: an important but neglected
presentations of recognized entities such as hypersensi- target in the treatment of obstructive airway diseases. Trends Pharmacol Sci.
tivity pneumonitis. 2008;29:340–345.
35. Lynch DA. Imaging of small airways disease and chronic obstructive
References
pulmonary disease. Clin Chest Med. 2008;29:165–179, vii.
1. Bake B. Is maximum mid-expiratory flow rate sensitive to small airways 36. Wang CW, Muhm JR, Colby TV, Leslie KO. Small airway lesions. In: Cagle
obstruction? Eur J Respir Dis. 1981;62:150–151. PT, Allen TC, Beasley MB, eds. Diagnostic Pulmonary Pathology. 2nd ed. New
2. Chen CZ, Lin CC, Lee CH, Chang HY, Hsiue TR. Small airways obstruction York, NY: Informa; 2008:229–249.
syndrome in clinical practice. Respirology. 2009;14:393–398. 37. Barbareschi M, Leslie K. Pathology of the large and small airways. In:
3. Cohen J, Postma DS, Vink-Klooster K, et al. FVC to slow inspiratory vital Leslie KO, Wick MR, eds. Practical Pulmonary Pathology. Philadelphia, PA:
capacity ratio: a potential marker for small airways obstruction. Chest. 2007;132: Churchill Livingstone; 2005:259–302.
1198–1203. 38. Ryu JH, Colby TV, Hartman TE, Vassallo R. Smoking-related interstitial
4. Kelman GR. Assessment of airway obstruction with particular reference to lung diseases: a concise review. Eur Respir J. 2001;17:122–132.
the small airways. J Soc Occup Med. 1980;30:157–163. 39. Cagle PT, Allen TC, Beasley MB, eds. Diagnostic Pulmonary Pathology.
5. Obtulowicz K, Laczkowska T, Kolarzyk E, Hudzik A. Obstruction of the 2nd ed. New York, NY: Informa; 2008.
small airways in the spirometric diagnosis of occupational bronchial asthma. J 40. Stanescu D, Veriter C. A normal FEV1/VC ratio does not exclude airway
Investig Allergol Clin Immunol. 1998;8:300–303. obstruction. Respiration. 2004;71:348–352.
6. Stanescu D. Small airways obstruction syndrome. Chest. 1999;116:231–
41. Colby TV, Yousem SA. Pulmonary histology for the surgical pathologist.
233.
Am J Surg Pathol. 1988;12:223–239.
7. Thurlbeck WM. The pathology of small airways in chronic airflow
42. Popper HH. Bronchiolitis, an update. Virchows Arch. 2000;437:471–481.
limitation. Eur J Respir Dis Suppl. 1982;121:9–18.
43. Penn CC, Liu C. Bronchiolitis following infection in adults and children.
8. Wright GD, Roberts SD, Finch MB, Martin B. Long-term follow up of small
Clin Chest Med. 1993;14:645–654.
airways obstruction in patients with rheumatoid arthritis. Ann Rheum Dis. 1998;
44. Andersen P. Pathogenesis of lower respiratory tract infections due to
57:258.
chlamydia, mycoplasma, legionella and viruses. Thorax. 1998;53:302–307.
9. Schlesinger C, Meyer CA, Veeraraghavan S, Koss MN. Constrictive
(obliterative) bronchiolitis: diagnosis, etiology, and a critical review of the 45. Harrison AM, Bonville CA, Rosenberg HF, Domachowske JB. Respiratory
literature. Ann Diagn Pathol. 1998;2:321–334. syncytial virus-induced chemokine expression in the lower airways: eosinophil
10. Vilchez RA, Dauber J, Kusne S. Infectious etiology of bronchiolitis recruitment and degranulation. Am J Respir Crit Care Med. 1999;159:1918–
obliterans: the respiratory viruses connection—myth or reality? Am J Transplant. 1924.
2003;3:245–249. 46. Hall CB. Respiratory syncytial virus and parainfluenza virus. N Engl J Med.
11. Valentine VG, Gupta MR, Walker JE Jr, et al. Effect of etiology and timing 2001;344:1917–1928.
of respiratory tract infections on development of bronchiolitis obliterans 47. Panitch HB. Bronchiolitis in infants. Curr Opin Pediatr. 2001;13:256–260.
syndrome. J Heart Lung Transplant. 2009;28:163–169. 48. Steiner RW. Treating acute bronchiolitis associated with RSV. Am Fam
12. Izumi T, Kitaichi M, Nishimura K, Nagai S. Bronchiolitis obliterans Physician. 2004;69:325–330.
organizing pneumonia: clinical features and differential diagnosis. Chest. 1992; 49. Fjaerli HO, Farstad T, Rod G, Ufert GK, Gulbrandsen P, Nakstad B. Acute
102:715–719. bronchiolitis in infancy as risk factor for wheezing and reduced pulmonary
13. Kitaichi M. Differential diagnosis of bronchiolitis obliterans organizing function by seven years in Akershus County, Norway. BMC Pediatr. 2005;5:31.
pneumonia. Chest. 1992;102:44S–49S. 50. Perrotta C, Ortiz Z, Roque M. Chest physiotherapy for acute bronchiolitis
14. Nakanishi M, Demura Y, Mizuno S, et al. Changes in HRCT findings in in paediatric patients between 0 and 24 months old. Cochrane Database Syst
patients with respiratory bronchiolitis-associated interstitial lung disease after Rev. 2005:CD004873.
smoking cessation. Eur Respir J. 2007;29:453–461. 51. Wong JY, Rutman A, O’Callaghan C. Recovery of the ciliated epithelium
15. Hansell DM. HRCT of obliterative bronchiolitis and other small airways following acute bronchiolitis in infancy. Thorax. 2005;60:582–587.
diseases. Semin Roentgenol. 2001;36:51–65. 52. Bush A, Thomson AH. Acute bronchiolitis. BMJ. 2007;335:1037–1041.
16. Hansell DM, Rubens MB, Padley SP, Wells AU. Obliterative bronchiolitis: 53. Calogero C, Sly PD. Acute viral bronchiolitis: to treat or not to treat-that is
individual CT signs of small airways disease and functional correlation. the question. J Pediatr. 2007;151:235–237.
Radiology. 1997;203:721–726. 54. Schuh S, Lalani A, Allen U, et al. Evaluation of the utility of radiography in
17. Hwang JH, Kim TS, Lee KS, et al. Bronchiolitis in adults: pathology and acute bronchiolitis. J Pediatr. 2007;150:429–433.
imaging. J Comput Assist Tomogr. 1997;21:913–919. 55. Thiessen PN. Acute bronchiolitis: there may be a treatment. BMJ. 2007;
18. Muller NL, Miller RR. Diseases of the bronchioles: CT and histopathologic 335:1109.
findings. Radiology. 1995;196:3–12. 56. Barben J, Kuehni CE, Trachsel D, Hammer J. Management of acute
19. Davies CW, Tasker AD, Padley SP, Davies RJ, Gleeson FV. Air trapping in bronchiolitis: can evidence based guidelines alter clinical practice? Thorax.
sarcoidosis on computed tomography: correlation with lung function. Clin 2008;63:1103–1109.
Radiol. 2000;55:217–221. 57. Marguet C, Bocquel N, Benichou J, et al. Neutrophil but not eosinophil
20. Stern EJ, Frank MS. Small-airway diseases of the lungs: findings at inflammation is related to the severity of a first acute epidemic bronchiolitis in
expiratory CT. AJR Am J Roentgenol. 1994;163:37–41. young infants. Pediatr Allergy Immunol. 2008;19:157–165.
21. Hogg JC, Macklem PT, Thurlbeck WM. Site and nature of airway 58. Smith J, Salinas R. Do systemic corticosteroids improve acute outcomes in
obstruction in chronic obstructive lung disease. N Engl J Med. 1968;278:1355– infants with RSV bronchiolitis? J Okla State Med Assoc. 2008;101:14.
1360. 59. Wright M, Mullett CJ, Piedimonte G. Pharmacological management of
22. Yousem SA. Small airways disease. Pathol Annu. 1991;26(pt 2):109–143. acute bronchiolitis. Ther Clin Risk Manag. 2008;4:895–903.
23. Myers JL, Colby TV. Pathologic manifestations of bronchiolitis, constrictive 60. Zhang L, Mendoza-Sassi RA, Wainwright C, Klassen TP. Nebulized
bronchiolitis, cryptogenic organizing pneumonia, and diffuse panbronchiolitis. hypertonic saline solution for acute bronchiolitis in infants. Cochrane Database
Clin Chest Med. 1993;14:611–622. Syst Rev. 2008:CD006458.
Arch Pathol Lab Med—Vol 134, May 2010 Pathology of Small Airways Disease—Allen 713You can also read