KOL WEBINAR WITH DR. FRANK GIORDANO - NOX-A12 & RADIOTHERAPY COMBINATION: A DIFFERENTIATED AND PROMISING NEW APPROACH TO TREATING BRAIN CANCER ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
KOL WEBINAR WITH DR. FRANK GIORDANO
NOX-A12 & RADIOTHERAPY COMBINATION:
A DIFFERENTIATED AND PROMISING
NEW APPROACH TO TREATING BRAIN CANCER
November 23, 2021 | 8:00 AM EST / 2:00 PM CET
© NOXXON Pharma
1
WEBINAR PRESENTERS
MODERATOR PRESENTERS
Guillaume van Dr. Frank Giordano Aram Mangasarian
Renterghem Chair & Director CEO
Managing Director Radiation Oncology Dept. NOXXON Pharma
LifeSci Advisors University Hospital Bonn
Lead investigator of NOX-A12
GLORIA Phase 1/2 study
2
Forward Looking Statements The information and opinions contained in this representatives, or any of their respective directors, being accurate. This presentation contains forward presentation and any other information discussed at officers, employees, direct or indirect shareholders, looking statements. These statements reflect the this presentation are provided as at the date of this agents, affiliates, advisors or any other person accept Company’s current knowledge and its expectations presentation and are therefore of a preliminary nature, any responsibility whatsoever for the contents of this and projections about future events and may be have not been independently verified and may be presentation, and no representation or warranty, identified by the context of such statements or words subject to updating, revision, amendment or change express or implied, is made by any such person in such as “anticipate,” “believe”, “estimate”, “expect”, without notice and in some cases has not been relation to the contents of this presentation. “intend”, “plan”, “project”, “target”, “may”, “will”, audited or reviewed by the Company’s auditors. This “would”, “could”, “might” or “should” or similar presentation is selective in nature and does not purport Certain information in this presentation is based on terminology. By their nature, forward looking to contain all information that may be required to management estimates. Such estimates have been statements are subject to a number of risks and evaluate the Company and/or its securities. Neither made in good faith and represent the current beliefs of uncertainties, many of which are beyond the the Company nor any other person is under any applicable members of management. Those Company’s control that could cause the Company’s obligation to update or keep current the information management members believe that such estimates actual results and performance to differ materially from contained in this presentation or to correct any are founded on reasonable grounds. However, by their any expected future results or performance expressed inaccuracies in any such information which may nature, estimates may not be correct or complete. or implied by any forward looking statements. The become apparent or to provide you with any Accordingly, no representation or warranty (express or Company undertakes no obligation to publicly release additional information. No reliance may or should be implied) is given that such estimates are correct or the results of any revisions to any forward looking placed for any purpose whatsoever on the information complete. Where this presentation quotes any statements in this presentation that may occur due to contained in this presentation, or any other information information or statistics from any external source, it any change in its expectations or to reflect events or discussed verbally, or on its completeness, accuracy or should not be interpreted that the Company has circumstances after the date of this presentation. fairness. None of the Company, its investment banking adopted or endorsed such information or statistics as 3
Introductory remarks on
NOXXON Pharma
Aram Mangasarian
CEO
NOXXON Pharma
4
ABOUT NOXXON: Strong Value Proposition Through
Differentiated Pipeline Targeting the TME
Clinical stage Expert in Tumor Focus on 2 large orphan Robust
Upcoming
biotech Microenvironment cancer indications commercial
Catalysts
company protection
~$6.5bn Addressable Market
Mission to improve In brain cancer (1st line GBM) Q1 2022
cancer treatment and pancreatic cancer Brain cancer
outcomes, when indications Thanks to Phase 1/2 read-out
Listed in 2016, Euronext tumor orphan drug status
Growth Paris microenvironment Technology leverageable to and
significantly limits numerous other solid tumors: patent families
survival - Combination with covering H1 2024
HQ in Berlin, Germany
Radiotherapy NOX-A12 & NOX-E36 Pancreatic cancer
NOX-A12’s highly - Combination with Phase 2 read-out
differentiated dual Immunotherapy
mechanism of action
5
Treating Seed and Soil:
Targeting CXCL12 in the Glioblastoma
Tumor Microenvironment
Frank A. Giordano, MD
Professor of Radiation Oncology
Director and Chair, Department of Radiation Oncology
University Hospital Bonn
Lead investigator of NOX-A12 GLORIA Phase 1/2 study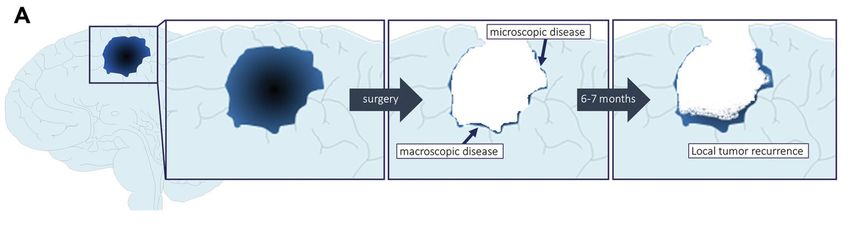
Brain tumor incidences (primary brain tumors)
California Dept. of Public Health, 2008
A case to remember ➢ 45 y/o female patient with a history of MS ➢ underwent MRT q3mo (for MS), last scan was before Xmas 2014 ➢ came to ER in April 2014: progressive vertigo, nausea and muscle weaknesses

Standard of care for GBM: components
Surgery or Biopsy Radiotherapy Maintenance
+ Chemotherapy Chemotherapy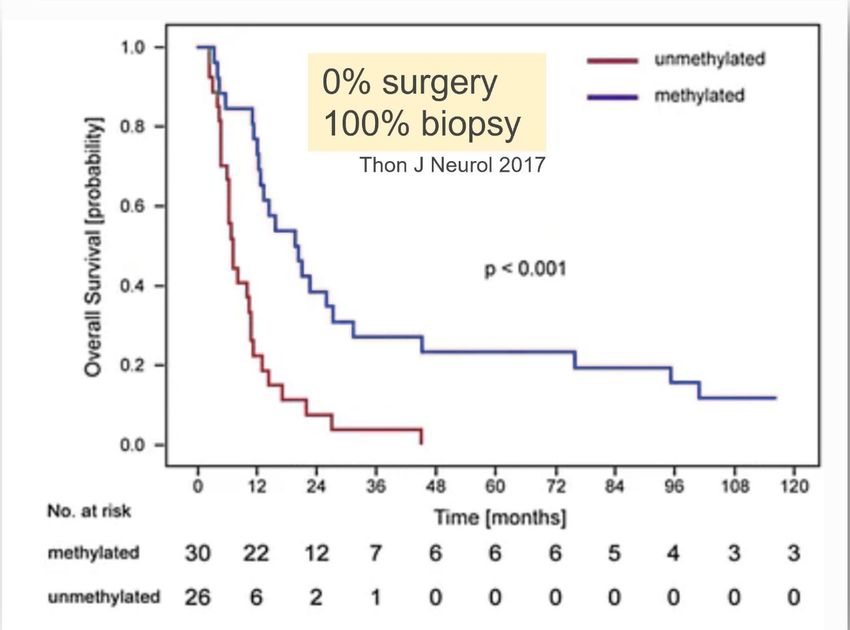
Standard of care for GBM: outcome
Stupp et al., 2005Role of MGMT expression in GBM
PROM DNAMGMT
CH3
TMZ
(Methylhydrazin)
ApoptosisRole of MGMT expression in GBM
PROM DNAMGMT
CH3
TMZ
(Methylhydrazin)
ApoptosisRole of MGMT expression in GBM
PROM DNAMGMT
CH3
83% surgery TMZ
17% biopsy (Methylhydrazin)
Hegi NEJM 2005 Thon J Neurol 2017
ApoptosisGBM recurrence patterns
local 97-99% combined ~1-3% distantReasons for rapid local recurrence
Giordano Neurosurgery 2019
- residual tumor cells remain even after “perfect” (or supramaximal) surgery
- GB stem cells show a high degree of radio- and chemoresistance
- highly effective revascularization after radiotherapyReasons for rapid local recurrence
Giordano Neurosurgery 2019
- residual tumor cells remain even after “perfect” (or supramaximal) surgery
- GB stem cells show a high degree of radio- and chemoresistance
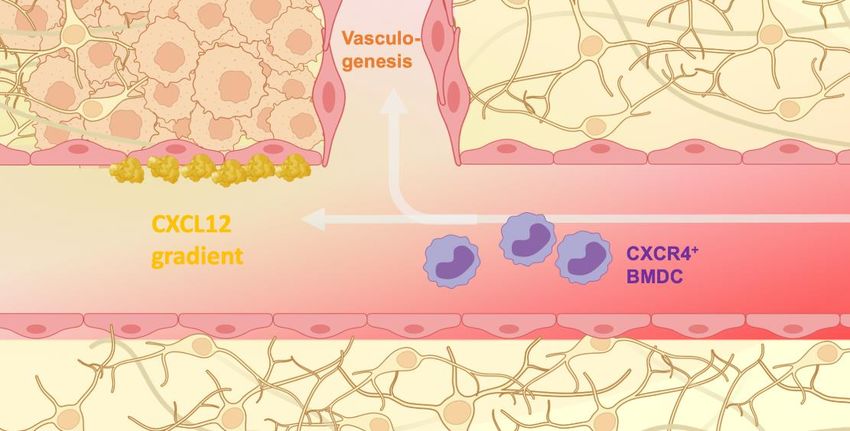
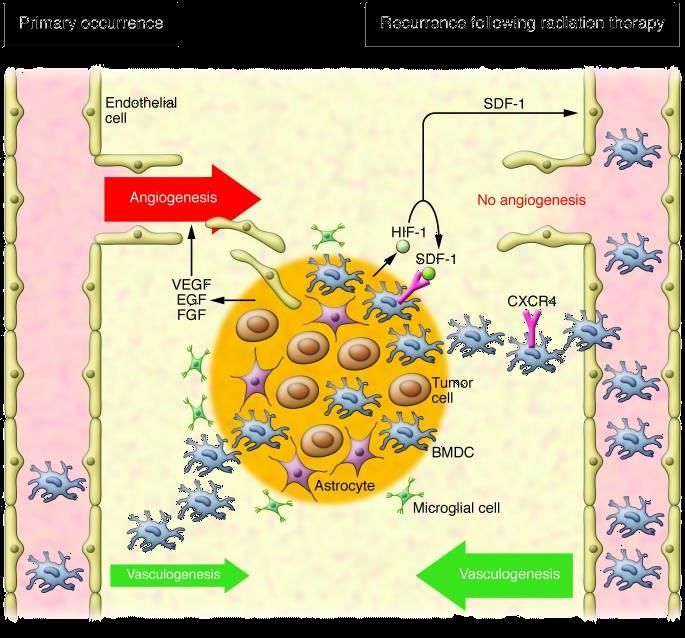
- highly effective revascularization after radiotherapyMechanism of revascularization after RT
Chemoattraction
towards gradient
CXCR4+
SDF-1
(=CXCL12)
CXCR4+ myeloid cells
MP/TAM (microglia is CXCR4 negative)
monocytes (would not persist in intact brain)
CD11b+CD14+CD33+ myeloid-derived suppressor cells
Greenfield J Clin Invest 2010 BMDC, Bone Marrow-Derived Cell
CXCR4, C-X-C Chemokine Receptor Type 4 Vasculogenesis Immunosuppression
EGF, Epidermal Growth Factor
FGF, Fibroblast Growth Factor
HIF-1, Hypoxia-inducible factor 1
SDF-1, Stem cell Derived Factor 1 (= CXCL12)
VEGF, Vascular Endothelial Growth FactorMechanism of revascularization after RT
Targeting CXCL12 in other cancers
mRNA expression of CXCL12 in various cancers
Broad Institute Cancer Cell Line EncyclopediaTargeting CXCL12 in other cancers
mRNA expression of CXCL12 in various cancers
Broad Institute Cancer Cell Line EncyclopediaStrong pre-clinical evidence for radiotherapy + NOX-A12
EFFECTS OF TREATMENTS
Autochthonous brain tumor model in rats
Radiotherapy
• Spontaneous tumor development in immuno-competent at day 0
host
• Diversity of tumor cell types with therapeutic resistance
comparable to human situation
• Refractory to standard therapies
Tumor
recurrence
detected
only in 1/3 of
animals
Pregnant rats:
ENU (carcinogen)
on gestational age
day 17 - 18
Radiotherapy + NOX-A12 resulted in 100% complete response (66% durable)
in a rodent brain cancer model
Liu Neuro-Oncology 2014Background and rationale
Olaptesed pegol (OLA, NOX-A12)
RNA Spiegelmer (L-stereoisomer)
binds & neutralizes
Ceradini, Nat Med 2004
Greenfield, J Clin Invest. 2010
Kioi, J Clin Invest. 2010
OLA
NOX-A12 CXCL12
Liu, Neuro Oncol. 2014
CXCR4, C-X-C Motif Chemokine Receptor 4 (receptor for CXCL12)
BMDC, bone marrow derived cells
TME, tumor microenvironment
- 22 -GLORIA Phase I/II Trial
Key inclusion criteria: RT
• Newly-diagnosed supratentorial 60 Gy (2 Gy x 30)
glioblastoma WHO IV 40.05 Gy (2.67 Gy x 15)
• unmethylated MGMT promoter
• Incomplete resection/biopsy only OLA (NOX-A12) Follow-
• ECOG ≤ 2 continuous i.v. infusion at three doses (200, 400, 600 mg/week) up
Inclusion 6 26
Safety monitoring
Advanced MRI (perfusion/diffusion)
CODEX® (multiplexed immunofluorescence imaging)
Primary Endpoint: Safety as per # of patients with treatment-related adverse events
Secondary Endpoints: OLA/NOX-A12 plasma levels, tumor vascularization/perfusion (advanced MRI),
PFS-6, mPFS, OS, QoL, NANO
- 23 -CONSORT of GLORIA and controls
GLORIA Matched Imaging Control Cohort**
11 screened
25 screened
2 excluded
9 enrolled
12 no advanced MRI
RT + 200 mg/week
3 cohort 1 9 advanced MRI 13 advanced MRI
OLA
RT + 400 mg/week
3 cohort 2
OLA 1 CODEX* 7 CODEX*
RT + 600 mg/week
3 cohort 3
OLA
21 no paired samples
28 screened
** Only performed for paired samples from 1st and 2nd surgery.
** Matched per MGMT promoter methylation status and extent of resection.
** Patients in the control cohort needed to have at least 3 consecutive scans.
CODEX Control Cohort
- 24 -Primary EP: Safety (AE relationships)
RT
All: n=170 n = 29
cut-off date: 10/15/2021
20
2
5
OLA 2
n = 17
38
9* 4
Tumor-related
n = 49
*OLA-only related AE
GGT increased G3
2 x ALT increased G2
Dyspnea G1
3 x Leukocytosis G1
Paresthesia G1
Pyrexia G1
- 25 -Best response under OLA (volume of T1 enhancing lesions)
VT1 GLORIA Independent Central Review VT1 Matched Imaging Control Cohort
300
(n=9) (n=13)
300
Max. change from baseline [%]
Max. change from baseline [%]
200 200
100 100
PD PD
0
SD SD
> 300 %
PR PR
-100 -100
p=0.0026
Non-parametric Mann Whitney U test
- 26 -Best response in cellularity and tumor perfusion under OLA
ADC mean
ADC mean rCBV mean FTBhigh
(Independent Central Review, n=9) rCBV
(Independent mean
Central Review, n=9) FTB
(Independent highReview, n=9)
Central
300 300 300
Max. change from baseline [%]
Max. change from baseline [%]
Max. change from baseline [%]
200 200 200
low cellularity high perfusion increase in highly perfused fraction
100 100 100
0 0 0
high cellularity low perfusion decrease in highly perfused fraction
-100 -100 -100
ADC, apparent diffusion coefficient (derived parameter from DWI sequences)
rCBV, standardized relative cerebral blood volume (derived parameter from DSC sequences)
FTBhigh , fractional tumor burden with rCBV > 1.75
- 27 -Exemplary response to RT/OLA
OLA / NOX-A12 TMZ
RT W26
Baseline W9 W18 W34 W39
C1-003
OLA / NOX-A12
Baseline
RT W26 W49
W9 W18
C1-001
re-surgery for suspected PD
CODEX
path report: Ki67CODEX: RT/OLA reduces CXCL12 levels in the tumor endothelium
Baseline Post RT / under OLA
CXCL12+ cells
Patient C1-001
GLORIA
20 50
C1-001
Out of CD31+ cells (%)
Out of total cells (%)
40
15
DAPI
CD31 30
Baseline Post RT/TMZ CXCL12 10
20
5
10
0 0
e
e
12
12
in
in
A
A
el
el
X-
X-
as
as
O
O
B
B
References
N
N
er
er
nd
Baseline Post RT/TMZ/NIVO
nd
/u
/u
T
T
R
R
st
st
Po
Po
Images show areas of pathologist-confirmed tumor tissue
- 29 -CODEX: RT/OLA reduces tumor cell proliferation
Baseline Post RT / under OLA
Proliferating cells
GLORIA Patient C1-001
C1-001 15
Out of total cells (%)
DAPI 10
Baseline Post RT/TMZ Ki67
5
0
e
12
in
A
References
el
X-
as
O
Baseline Post RT/TMZ/NIVO
B
N
er
nd
/u
T
R
st
Po
Images show areas of pathologist-confirmed tumor tissue
- 30 -CODEX: Cytotoxic T cell infiltration and activation
Baseline Post RT / under OLA
CD8+ GNZB+ CD8+
Patient C1-001 Patient C1-001
GLORIA 2.0 0.8
Out of total cells (%)
C1-001 1.5 0.6
DAPI 1.0 0.4
CD8
Baseline Post RT/TMZ GNZB 0.5 0.2
0.0 0.0
12 /
e
12 /
e
X- RT
in
X- RT
in
el
el
N st
as
N st
as
A
A
Po
Po
B
B
O
O
r
r
de
de
un
un
References
Out of Ki67+ cells (%)
100 CD8+ GNZB+ T cells
Baseline Post RT/TMZ/NIVO CD8+ GNZB- T cells
10
Other cells
1
0.1
0.01
12 /
e
X- RT
in
el
N st
as
A
Images show areas of pathologist-confirmed tumor tissue
Po
B
O
r
de
- 31 -
unCODEX: Cytotoxic T cell infiltration and activation
Baseline Post RT / under OLA
CD8+ GNZB+ CD8+
Patient C1-001 Patient C1-001
GLORIA 2.0 0.8
Out of total cells (%)
C1-001 1.5 0.6
1.0 0.4
0.5 0.2
Whole slide spatial Analysis 0.0 0.0
12 /
e
12 /
e
X- RT
in
X- RT
in
Baseline Post RT / under OLA
el
el
N st
as
N st
as
A
A
Po
Po
B
B
O
O
Tumor cells Tumor cells
r
r
de
Proliferating or cytotoxic CD8 Proliferating or cytotoxic CD8
de
un
un
Out of Ki67+ cells (%)
100 CD8+ GNZB+ T cells
CD8+ GNZB- T cells
10
Other cells
1
0.1
0.01
12 /
e
X- RT
in
el
N st
as
A
Images show areas of pathologist-confirmed tumor tissue
Po
B
O
r
de
- 32 -
unConclusions – GLORIA Study
• Combined RT + OLA (NOX-A12) treatment is feasible and safe
• Initial promising efficacy signals
o 8 out of 9 patients showed a response as per volume of T1-contrast (2 x PR)
o reduced cellularity in 8 out of 9 patients
o reduced perfusion 7 out of 9 patients
• Tissue analysis (re-surgery under OLA) confirms mode(s) of action:
o CD31/CXCL12 co-localization is abrogated
o Strong reduction in tumor cell proliferation
o CD8+ T cell count increases by 15-fold
o De-novo clusters of proliferating and cytotoxic CD8+ T cells
• Follow-up ongoing, expansion cohorts planned
- 33 -Acknowledgements
UKB Radiation Oncology UKB Neuropathology Uni Heidelberg
Julian P. Layer Thorsten Pietsch UH Mannheim
Katja Klever Lea Friker Elena Sperk
Katharina Sahm
UKB Exp. Oncology UC London Michael Platten
Michael Hölzel Sotirios Bisdas
Sonia Leonardelli UH Leipzig
Roberta Turiello UKB Neuroradiology Clemens Seidel
Alexander Radbruch Peter Hambsch
UKB Neuro-Oncology Daniel Paech Nadja Talhi
Ulrich Herrlinger Franziska Grau
Christiane Landwehr UH Essen
Thomas Zeyen Martin Glas
Christina Schaub Sied Kebir
Mirco Muscheid Sarina Agkatsev
Frank.Giordano@ukbonn.de
- 34 -Expansion Cohorts of Phase 1/2 Trial in Brain Cancer
Q4
2022
2021
Newly diagnosed brain Cohort Complete tumor resection
cancer (glioblastoma) A NOX-A12 + RT
MGMT promoter
unmethylated population:
chemotherapy will be Cohort Incomplete tumor resection
B NOX-A12 + RT + anti-VEGF
ineffective, so not used
NOX-A12 dose:
600mg/week
Planned
Cohort
Incomplete tumor resection
C NOX-A12 + RT + anti-PD-1
Expansion cohorts aim to provide additional clinical data to support the pivotal
study trial design and discussions with the regulators
35Next Step: Pivotal Trial in 1st line MGMT Promoter Unmethylated
Patients – 2025 Read-out
Target Target
Pivotal Study in Start Completion
newly diagnosed
brain cancer 2022 2025
(glioblastoma)
Treatment until
MGMT promoter
Radiotherapy + NOX-A12 progression to
unmethylated
population: assess:
chemotherapy VS.
known to be PFS, OS, other
ineffective1 Standard of Care efficacy
RT ± Temozolomide endpoints
Centers in EU & US
36 1. Hegi et al. (2005) NEJM 352:997Q&A Session
Dr. Frank Giordano Aram Mangasarian
Chair & Director CEO
Radiation Oncology Dept. NOXXON Pharma
University Hospital Bonn
Lead investigator of NOX-A12
GLORIA Phase 1/2 study
37Thank you!
Contact Us:
noxxon@noxxon.com
38You can also read

















































