Journal of Health Monitoring - Health and health care of women aged 50 years and older - Results of the research project 'Frauen 5.0'
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
JUNE 2020 FEDERAL HEALTH REPORTING
ISSUE
2 JOINT SERVICE BY RKI AND DESTATIS
Journal of Health Monitoring
Health and health care of women aged
50 years and older – Results of the research
project ‘Frauen 5.0’
1Journal of Health Monitoring Index
Health and health care of women aged 50 years
and older – Results of the research project
‘Frauen 5.0’
3 Focus Reasons for women aged 50 years and older
to seek gynaecological advice and treatment
15 Focus Gynaecology and general practitioner services
utilisation by women in the age group 50 years
and older
26 Fact sheet Barriers for women aged 50 years and
older to accessing health care in Germany
35 Fact sheet Demographics of the female
population aged 50 years and older in Germany’s
north east region – Selected aspects
Journal of Health Monitoring 2020 5(2) 2Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
Journal of Health Monitoring · 2020 5(2)
DOI 10.25646/6065
Reasons for women aged 50 years and older to seek gynaecological
Robert Koch Institute, Berlin
advice and treatment
Laura Krause 1, Lorena Dini 2, Franziska Prütz 1 Abstract
Gynaecological care is generally perceived as focused on reproductive health. However, when women enter the non-
1
Robert Koch Institute, Berlin reproductive life phase, other reasons to seek gynaecological care gain in importance. This paper presents findings on
Department of Epidemiology and the reasons for women in the 50 years and older age group to seek gynaecological consultation and treatment. Our
Health Monitoring
findings are based on data from the German Health Interview and Examination Survey for Adults (DEGS1, 2008–2011),
2
Charité – Universitätsmedizin Berlin
Institute of General Practice
conducted by the Robert Koch Institute (RKI), as well as the 2016 claims data from the Associations of Statutory Health
Insurance Physicians (KVen), provided by the Central Research Institute of Ambulatory Health Care in Germany (Zi). At
Submitted: 03.04.2020 this age, cancer screening and menopausal complaints can become, as DEGS1 data shows, important reasons to seek
Accepted: 03.06.2020 gynaecological services. Around 65.0% of 50- to 79-year-old women took advantage of breast palpation examinations
Published: 30.06.2020
during the last twelve months, and 58.0% underwent cervical cell smear tests (pap smear). 47.2% of women had their
last menstrual period at age 50 or later. KV data shows that with 45.3% and 33.1% of cases respectively, menopausal
symptoms (International Statistical Classification of Diseases and Related Health Problems, 10th revision, ICD-10: N95)
and screening for malignant neoplasms (ICD 10: Z12) were the most frequently billed services. The data clearly shows
reasons for consultation and treatment of women aged 50 years and older and these should therefore be considered in
treatment planning and design.
GYNAECOLOGY · REASONS TO SEEK TREATMENT · OUTPATIENT CARE · OLDER WOMEN · GERMANY
1. Introduction following menopause, conditions such as urinary inconti-
nence, osteoporosis and uterine prolapse become more
The public and research community primarily relate gynae- frequent [5, 6]. Some conditions may necessitate surgery
cological care to reproductive health and questions such that requires outpatient medical aftercare [7–9]. From the
as family planning, pregnancy and birth [1]. As women near perspective of prevention, cancer early detection gains great
the end of their reproductive years, new reasons to seek importance in gynaecological practice [10]. For women of
consultation and treatment with outpatient gynaecological specified age groups, statutory health insurance offers can-
service providers arise, in part due to hormonal changes cer screening tests as a standard benefit. In January 2020,
that occur during menopause [2–4]. Breast and endome- early detection of cervical cancer was changed from an
trial cancer incidence rates increase with age and, opportunistic screening offer to an organized screening
Journal of Health Monitoring 2020 5(2) 3Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
programme, including an annual cervical cell smear (20- to gain an overview of the levels of care that are provided
DEGS1 to 34-year-old women) or a cervical cell smear and human and, building on this, develop concepts to secure outpatient
Data holder: Robert Koch Institute papilloma virus test every three years (age 35 and older). gynaecological care for this group within the population.
Objectives: To provide reliable information about the For the early detection of breast cancer, women aged 30 This paper describes gynaecological conditions that
population’s health status, health-related behaviour years and older are offered annual breast palpation exam- affect women aged 50 years and older over time, and pos-
and health care in Germany including analysis of
temporal developments and trends.
inations, and 50- to 69-year-old women can undergo a sible reasons for gynaecological appointments. The results
mammography of both breasts within the scope of a bien- are based on data from the German Health Interview and
Survey method: Questionnaires, physical examina-
tions and tests, a physician interview, a medication nial mammography screening [11]. Some patients will Examination Survey for Adults (DEGS1, 2008–2011), con-
interview and laboratory investigations (blood and request further consultation on mammography screening ducted by the Robert Koch Institute (RKI). This data allows
urine sample).
by their gynaecologist [12]. us to determine the possible reasons why women in this
Population: German resident population, aged 18
and above
With regard to the provision of gynaecological services, group sought gynaecological consultation and treatment.
the health of women aged 50 years and older is not the only Furthermore, data from the Associations of Statutory
Sampling: Registry office sample; randomly selected
individuals from 180 communities in Germany were factor to be considered, as the overall uptake of gynaeco- Health Insurance Physicians (KVen), provided by the Cen-
invited to participate (120 original sample points of logical services also considerably decreases with age (see tral Research Institute of Ambulatory Health Care in Ger-
the German National Health Interview and Examina-
tion Survey 1998 and 60 new sample points). Focus Article Gynaecology and general practitioner services many (Zi), reveals the most frequent diagnoses in gynae-
Participants: N=8,151 (4,283 women; 3,868 men). The utilisation by women in the age group 50 years and older in cological practices in 2016.
sample included persons who were newly recruited this issue of the Journal of Health Monitoring). Demo-
and those who had already participated in the Ger-
man National Health Interview and Examination Sur- graphic ageing, moreover, is leading to an increasing num- 2. Methodology
vey 1998 (mixed design). ber of older women (see Fact Sheet Demographics of the 2.1 Sample design and study implementation
Response rate: 62% among revisiting participants female population aged 50 years and older in Germany’s
and 42% first time participants north east region – Selected aspects, also in this issue of As no representative data exists for Germany that indicates
Survey period: 2008 to 2011 the Journal of Health Monitoring). Against this backdrop, which gynaecological symptoms or need for consultation
Data protection: DEGS1 is subject to strict compliance and due to the increasing difficulties related to ensuring and treatment lead to an uptake of the services provided
with the data protection regulations of the Federal outpatient care in rural regions, the project ‘Frauen 5.0’ by gynaecological practices, this paper builds on multiple
Data Protection Act and has been approved by the
Federal Commissioner for Data Protection and Free- (Regionale Versorgung von Frauen über 49 Jahre durch data sources that allow us to approximately describe the
dom of Information in Germany. Charité – Univer Fachärztinnen und Fachärzte für Gynäkologie und für All- situation.
sitätsmedizin Berlin’s ethics committee assessed the
ethics of the DEGS1 study and provided its approval gemeinmedizin) was developed, which is funded by the Between 2008 and 2011, as part of DEGS1, the RKI col-
(No.EA2/047/08). Participation in DEGS1 was volun- Innovation Fund of the Federal Joint Committee [13]. The lected representative data on the health of the German pop-
tary. The participants were informed about the aims
and contents of the studies and about data protection. project analyses the provision of gynaecological and gen- ulation aged 18 to 79 years. This study, which covered 8,151
Informed consent was obtained in writing. eral practitioner (GP) services to women aged 50 years and participants, included questionnaires, interviews, physical
More information in German is available at older in Germany’s north east region (Berlin, Brandenburg examinations and tests. The DEGS1 concept and survey
www.degs-studie.de
and Mecklenburg-Western Pomerania). The project aims design have previously been described in detail [14, 15].
Journal of Health Monitoring 2020 5(2) 4Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
DEGS1 included questions on gynaecological conditions 2.2 Statistical methods
and symptoms which could lead women to seek gynaeco-
logical services [5–10]. We can group these reasons into On the basis of data from DEGS1 (2008–2011), we ini-
the following four categories: ‘gynaecological cancer screen- tially determine gynaecological conditions and operations
ing’, ‘menopause and contraception’, ‘diseases and com- in 18- to 79-year-old women (n=4,198). We also report
plaints’ and ‘gynaecological operations’. These are thereby potential reasons to seek gynaecological consultation
only reasons for which women potentially sought gynae- and treatment by women aged 50 years and older
cology services; the survey did not ask whether women (n=2,287) and provide these as prevalences (in percent).
then actually visited a gynaecologist. DEGS1 calculations were carried out using a weighting
Claims data from the KVen, provided by the Zi (2016) factor that corrects deviations within the sample from
provide further indicators of actual service provision and the population structure (as of 31 December 2010) with
uptake. Every three months, the KVen provide the Zi with regard to age, sex, region, citizenship, type of municipal-
pseudonymised claims data from the quarterly accounts ity and education [14].
of office-based physicians. The information on the treat- Based on the 2016 KV claims data that we received from
ment cases, which this data contains, makes it possible the Zi, the most frequent ICD-10 diagnoses (three-digit
to precisely record the coded diagnoses [16]. Therefore codes) in gynaecology and GP practices are presented as
this data permits an assessment of actually provided the number of cases and proportion (in percent) of all
gynaecology services in outpatient practices either across cases.
Germany or for certain regions. Based on a special eval-
uation on request of the RKI, this paper presents the ten 3. Results
most frequently recorded codes from the 10th revision of
the International Statistical Classification of Diseases and The prevalence of conditions and symptoms that women
Related Health Problems (ICD-10, three-digit codes) in receive treatment for in gynaecology practices increases
gynaecology practices for women aged 18 years and older with age (Table 1). They include urinary incontinence, osteo
in Germany. Furthermore, we report the 20 most fre- porosis, uterine prolapse, as well as breast cancer and gynae-
quently recorded ICD-10 codes (three digits) for women cological cancers such as cervical, endometrium and ovar
aged 50 years and older in gynaecology practices in the ian cancers. The proportion of women who undergo
north east region (Berlin, Brandenburg and Mecklen- gynaecological surgeries, such as hysterectomy and ovariec-
burg-Western Pomerania). We also present data from GP tomy, also, as expected, increases with age.
practices that refer to gynaecological diagnoses. Figure 1 presents the prevalences for these conditions
as recorded in DEGS1 data for the group of 50- to 79-year-
old women, as well as further possible reasons to seek an
Journal of Health Monitoring 2020 5(2) 5Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
Table 1 Age group
Prevalence of specific diseases and 18–29 years 30–39 years 40–49 years 50–59 years 60–69 years 70–79 years
operations in 18- to 79-year-old women by age Diseases
(n=4,198) Urinary incontinence (currently, n=3,276) 4.2% 11.4% 17.1% 23.2% 30.1% 42.3%
Source: DEGS1 (2008–2011) Osteoporosis (lifetime, n=313) n.s. n.s. n.s. 4.1% 12.7% 25.2%
Uterus prolapse (lifetime, n=136) 0.2% 0.0% 2.5% 4.7% 4.6% 7.6%
Breast cancer (lifetime, n=112) 0.0% 0.1% 1.3% 2.9% 5.4% 6.2%
Gynaecological cancers (lifetime, n=87) 0.2% 0.9% 1.1% 3.3% 3.6% 1.7%
Operations
Hysterectomy (lifetime, n=784) 0.0% 0.5% 10.2% 26.8% 35.2% 38.0%
Ovariectomy (lifetime, n=349) 0.0% 1.1% 4.5% 9.2% 15.8% 19.5%
n.s. = not surveyed
appointment at a gynaecology practice. Cancer screening, screening programme and during normal practice). 65.0%
in particular, plays an important role: 73.1% of women had had undergone breast palpation during the last twelve
Cancer screening is one undergone a mammography during the last two years months and 58.0% cervical cancer screening (cervical cell
of the main reasons for (examinations carried out as part of the mammography smear test, pap smear).
women aged 50 years and
older to seek outpatient Gynaecological cancer screening
gynaecological services. Mammography (during the last two years)
Palpation of the breast (during the last twelve months)
Cervical cancer cell smear test (during the last twelve months)
Menopause and contraception
Last menstrual period
Use of hormone therapy (currently)
Use of contraception (currently, age range 50–65 years)
Diseases and complaints
Urinary incontinence (currently)
Osteoporosis (lifetime)
Uterine prolapse (lifetime)
Breast cancer (lifetime)
Gynaecological cancer* (lifetime)
Operations
Figure 1 Hysterectomy (lifetime)
Reasons for 50- to 79-year-old women Ovariectomy (lifetime)
to seek consultation and treatment at
0 10 20 30 40 50 60 70 80
gynaecology practices (n=2,287)
Proportion (in %)
Source: DEGS1 (2008–2011) *
Cervical, endometrium and/or ovarian cancer (lifetime: lifetime prevalence)
Journal of Health Monitoring 2020 5(2) 6Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
Menopause is a further reason to seek consultation and a contraceptive coil and 27.9% said they used the pill (data
treatment. Nearly half of all women (47.2%) had their last not shown). However, due to the low number of cases
menstruation at the age of 50 or later (average age for the (n=80), these results should be interpreted with caution.
last menstrual period in Germany: 49.7 years [17]). Over one Nonetheless, they do show that a need for consultation
third of women (35.5%) stated that they used menopausal and, in some cases, medical check-up examinations may
hormone therapy. also exist here [18–20].
Gynaecological conditions and post-operative care can An analysis of the most frequent diagnoses billed by
also lead women to seek an appointment at gynaecology gynaecology practices for women aged 18 years and older
practices: at the point of survey, 30.8% of women stated showed that menopausal and climacteric states (ICD-10:
they had acute urinary incontinence, and around one third N95) ranked fourth (Table 2). The diagnoses ranked sec-
(32.7%) had undergone hysterectomy. Osteoporosis (with ond and third (N89: other specified noninflammatory dis-
a lifetime prevalence among 50- to 79-year-old women of orders of vagina, Z12 encounter for screening for malignant
Menopausal symptoms also 13.1%), uterine prolapse (5.5%), breast cancer (4.7%), as neoplasms) are, as the following analyses show, also fre-
frequently lead women to well as gynaecological cancers (cervical, endometrium, quently billed for women aged 50 years and older.
seek gynaecological services; ovarian cancer 2.9%) could be further reasons to seek Figure 2 presents the 20 most frequently billed diagnoses
nearly half of all women aged gynaecological treatment. in gynaecology practices for women aged 50 years and older
6.5% of 50- to 65-year-old women said they used con- in the north east region in 2016. The largest recorded pro-
50 continue to menstruate.
traceptives. Of these, 22.9% used condoms, 46.6% used portion, 45.3% or 655,459 cases, concerned menopausal
Rank ICD-10 Code Diagnosis Number of cases Proportion
1 Z30** Contraceptive management 18,734,546 39.15%
2 N89 Other noninflammatory disorders of vagina 12,931,229 27.0%
3 Z12** Special screening examination for neoplasms 11,447,844 23.9%
4 N95 Menopausal and other perimenopausal disorders 7,036,573 14.7%
5 Z01** Other special examinations and investigations of persons without 6,418,212 13.4%
complaint or reported diagnosis
6 N76 Other inflammation of vagina and vulva 4,835,146 10.1%
7 N94 Pain and other conditions associated with female genital organs and 4,410,731 9.2%
Table 2 menstrual cycle
The ten most frequent ICD-10 codes (three 8 N92 Excessive, frequent and irregular menstruation 3,883,673 8.1%
digits) used by gynaecological practices for 9 R10 Abdominal and pelvic pain 3,122,270 6.5%
women aged 18 years and older in Germany 10 C50 Malignant neoplasm of breast 2,063,227 4.3%
ICD-10 = International Statistical Classification of Diseases and Related Health Problems, 10th revision
Source: Central Research Institute of *
Quarterly collection of case numbers, multiple registration of responses possible
Ambulatory Health Care in Germany (2016)* [21] **
Z diagnoses describe factors influencing health status and contact with health services.
Journal of Health Monitoring 2020 5(2) 7Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
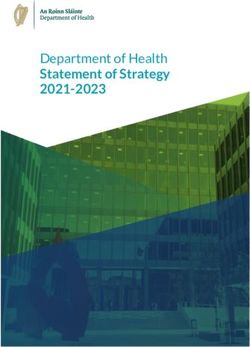
Figure 2 N95 Menopausal and other perimenopausal disorders
The 20 most frequent ICD-10 codes (three digit) Z12 Special screening examination for neoplasms
recorded by gynaecological practices for Z01 Other special examinations and investigations of
persons without complaint or reported diagnosis
women aged 50 years and older in the region
N89 Other noninflammatory disorders of vagina
north east (Berlin, Brandenburg and Mecklen-
I10 Essential (primary) hypertension
burg-Western Pommerania) (n=1,448,162)
C50 Malignant neoplasm of breast
Source: Central Research Institute of N81 Female genital prolapse
Ambulatory Health Care in Germany (2016) [21] Z30 Contraceptive management
N76 Other inflammation of vagina and vulva
Z90 Acquired absence of organs, not elsewhere classified
D25 Leiomyoma of uterus
N64 Other disorders of breast
F45 Somatoform disorders
E66 Obesity
N39 Other disorders of urinary system
R10 Abdominal and pelvic pain
F32 Depressive episode
Z80 Family history of malignant neoplasm
N60 Benign mammary dysplasia
N85 Other noninflammatory disorders of uterus, except cervix
0 5 10 15 20 25 30 35 40 45 50
Proportion of all cases (%)
ICD-10 = International Statistical Classification of Diseases and Related Health Problems, 10 revision
th
states (ICD-10: N95). Second came encounters for screening absence of organs (Z90: 140,106, 9.7%). One possible rea-
for malignant neoplasms (Z12: 478,683 cases, 33.1%). Other son for the frequency of breast cancer as a billing diagnosis
special examinations (Z01: 316,622 cases, 21.9%), which also could be, considering the relatively early age at the onset of
include general gynaecological examinations, ranked third. disease and the often good prognosis, regular aftercare.
Further frequently billed diagnoses were noninflammatory Gynaecology practices not only bill gynaecological diag-
disorders of vagina (N89: 291,281 cases, 20.1%) and other noses but also internal medicine diagnoses such as hyper-
inflammations of the external genitals such as vaginitis and tension (I10) and obesity (E66). Further diagnoses
vulvitis (N76: 141,013 cases, 9.7%), but also hypertension included conditions with a psychological/psychiatric back-
(I10: 194,762, 13.4%), breast cancer (mammary carcinoma, ground, such as somatoform disorders (F45) and depres-
C50: 178,947, 12.4%), uterine prolapse (N81: 164.941, 11.4%), sive episodes (F32), as well as unspecified diagnoses (Z01,
contraception (Z30: 155,573, 10.7%) as well as acquired Z12, Z90).
Journal of Health Monitoring 2020 5(2) 8Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
The results for the 20 most frequent diagnoses coded TK were prescribed hormone therapy during menopause.
by gynaecological practices for women aged 50 years and The figures for 2010 and 2000 were 9.6% and 37.0%,
older are widely congruent between the north east region respectively [24]. DEGS1 data shows considerably higher
and Germany as a whole, whereby the order of these con- figures for the proportion of women who use hormone
ditions sometimes differs slightly (data not shown). The therapy during menopause (35.5% between 2008 and 2011),
20 most frequent diagnoses coded for women aged 50 but this data refers to a different age range and includes
years and older by GPs in the region north east and for policy holders of all insurers. International studies estimate
Germany as a whole include no gynaecology-related diag- a uterine prolapse prevalence of around 30% [25–27]. How-
noses (data not shown). ever, these results are based on gynaecological examina-
tion data; how many of these women actually had symp-
4. Discussion toms was not considered in the studies. Current prevalences
of cancer are shown in the report 'Cancer in Germany' of
The results highlight that certain gynaecological conditions the Center for Cancer Registry Data and the Association of
and operations occur more frequently with age, and give Population-based Cancer Registries in Germany e.V. [28].
Women aged 50 years and an overview of reasons why women aged 50 years and older Comparisons between DEGS1 data and cancer registry data
older are an important group might seek gynaecological consultation and treatment. show differences in the disease spectrum and in the aver-
of gynaecological patients. DEGS1 data (2008–2011) and KV data (2016) both indicated age age of cancer diagnosis. This indicates that the survey
that cancer screening and menopause were the most fre- participants are not representative of women with a cancer
quent reasons for appointments at gynaecology practices. diagnosis in Germany in general. Women with severe
Inflammatory and noninflammatory disorders of the exter- courses of disease are likely to be underrepresented. Also,
nal genitals, uterine prolapse, as well as breast cancer and the number of cases (Table 1) is too small to achieve the
gynaecological cancers were among the further identified – actually desirable – differentiation to validly map different
key reasons to seek consultation and treatment. Gynaecol- types of cancer according to age.
ogy practices also billed some typical GP diagnoses, such Representative studies by the Federal Centre for Health
as hypertension and obesity. GPs, however, very rarely diag- Education (BZgA) on use of contraception showed that in
nose gynaecology-related conditions. Germany in 2018, 39% of 40- to 49-year-old women took
Prevalence estimates that could be compared to DEGS1 the pill, 34% used condoms and 20% a contraceptive coil
data are rare. According to international studies, the aver- (2011: 34%, 26% and 13%, respectively) [20]. One in two
age age for the onset of menopause is around 51 years [22, women that used some kind of contraception stated that
23]. Data from the Techniker Krankenkasse (TK) health questions on contraception had led to an appointment in
insurance on menopausal hormone therapy shows that in gynaecology practices [20]. The study did not examine con-
2017, 6.6% of the 45- to 65-year-old women covered by the traceptive behaviour of women aged 50 years and older.
Journal of Health Monitoring 2020 5(2) 9Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
BZgA studies show gynaecologists to be important contact women should seek treatment (in the sense of a medical-
persons for women’s health-related questions, yet the isation of life phases [32]), but should, rather, contribute
(potential) reasons to seek consultation and treatment in to ensuring that middle-aged and older women also receive
gynaecology practices can obviously only represent a pro- adequate care, for example regarding cancer screening
portion of all female health concerns. Due to be published examinations. Against this backdrop, we should mention
this year, the women’s health report of Federal Health two further findings: the decreasing number of women who
Reporting will contain a comprehensive overview of the seek appointments with gynaecologists with age – around
diverse aspects of women’s health [29]. 80% of 18- to 29-year-olds, but only 60% of 50- to 79-year-
Both survey and claims data have their limitations. While old women have at least one appointment per year in a
DEGS1 is generally representative for the German popula- gynaecology practice – as well as the increasing number of
tion, the survey tends to underrepresent people living in older women due to demographic ageing and the frequently
institutions, as well as older and less healthy people, an higher average age found in rural regions [33, 34]. When
aspect which an analysis concerned with middle-aged and planning care, it is important to consider that the screen-
older women should take into account. Health conditions ing programmes for the ealy detection of breast cancer
are self-reported in the survey, which could lead to a certain and – since January 2020 – cervical cancer have an influ-
level of recall bias. Events such as a hysterectomy, however, ence on the use of gynaecological services, as have the
are remembered with a high degree of reliability [30]. In addi- decreasing number of women who use hormone therapy
tion, DEGS1 did not ask women whether health problems during menopause [24] and the declining number of hys-
actually led them to seek outpatient gynaecology services. A terectomies [35]. Reasons for seeking gynaecological ser-
strength of claims data is the large sample size and that it vices from the perspective of women themselves were
comprises all women covered by statutory health insurance. analysed by the project ‘Frauen 5.0’, as were concepts to
However, the data is collected for billing purposes, and it is ensure that women in the 50 years and older age group
therefore impossible to directly deduce the prevalences for receive adequate gynaecological services, in particular in
particular conditions in the population. Moreover, since the sparsely populated rural regions, and regional models that
introduction of lump sum payment in 2008, data is only include the relevant actors were developed [1].
available for cases per quarter and practice [31].
Women are in the reproductive phase for less than half Corresponding author
of their entire lifespan. A perception of women’s health as Dr Laura Krause
being primarily reproductive health does not do justice to Robert Koch Institute
Department of Epidemiology and Health Monitoring
this fact and veils the consultation and treatment needs of
General-Pape-Str. 62–66
women aged 50 years and older. Taking these needs into 12101 Berlin, Germany
account does not imply postulating new reasons why E-mail: KrauseL@rki.de
Journal of Health Monitoring 2020 5(2) 10Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
Please cite this publication as References
Krause L, Dini L, Prütz F (2020) 1. Charité – Universitätsmedizin Berlin (Ed) (2020) Frauen 5.0 –
Reasons for women aged 50 years and older Executive Summary: Regionale Versorgung von Frauen 50+ durch
to seek gynaecological advice and treatment. Fachärztinnen und Fachärzte für Allgemeinmedizin und Gynäko-
Journal of Health Monitoring 5(2): 3–14. logie.
https://allgemeinmedizin.charite.de/fileadmin/user_upload/
DOI 10.25646/6065 microsites/m_cc01/allgmed/DOCS/Executive_Summary_
Frauen50_Printed.pdf (As at 26.03.2020)
The German version of the article is available at: 2. Maschewsky-Schneider U, Hellbernd H, Schaal W et al. (2001)
Über-, Unter-, Fehlversorgung und Frauengesundheit. Ein For-
www.rki.de/journalhealthmonitoring schungsgegenstand für Public Health. Bundesgesundheitsbl
44(8):771–779
Data protection and ethics 3. Kreienberg R, Digel S (2005) Krebsvorsorgeuntersuchungen bei
älteren Patientinnen. Der Gynäkologe 38(12):1074–1079
DEGS1 is subject to strict compliance with the data protec-
tion regulations of the Federal Data Protection Act and has 4. Bundesministerium für Familie, Senioren, Frauen und Jugend
(1999) Bericht zur gesundheitlichen Situation von Frauen in
been approved by the Federal Commissioner for Data Pro- Deutschland. Eine Bestandsaufnahme unter Berücksichtigung
tection and Freedom of Information in Germany. Charité der unterschiedlichen Entwicklung in West- und Ostdeutschland.
https://www.bmfsfj.de/blob/94878/0d550875836e1adc15c12e20e-
– Universitätsmedizin Berlin’s ethics committee assessed 9a92e54/prm-24001-umschlag-sr-band-209-data.pdf
the ethics of the DEGS1 study and provided its approval (As at 20.04.2020)
(No.EA2/047/08). Participation in DEGS1 was voluntary. 5. Kolip P, Hurrelmann K (2016) Handbuch Geschlecht und
Gesundheit. Männer und Frauen im Vergleich. 2., vollständig
The participants were informed about the aims and con- überarbeitete und erweiterte Auflage. Hogrefe Verlag, Bern
tents of the study and about data protection. Informed 6. Berufsverband der Frauenärzte e.V. (Ed) (no date) Körperliche
consent was obtained in writing. Veränderungen.
https://www.frauenaerzte-im-netz.de/de_koerperliche-veraende-
rungen-die-veraenderungen-im-einzelnen_256.html
Funding (As at 08.02.2018)
DEGS1 was funded by the Robert Koch Institute and the 7. Farquhar CM, Sadler L, Harvey SA et al. (2005) The association
of hysterectomy and menopause: a prospective cohort study.
Federal Ministry of Health. BJOG 112(7):956–962
The project ‘Regionale Versorgung von Frauen über 49 8. Prütz F, Knopf H, von der Lippe E et al. (2013) Prävalenz von
Jahre durch Fachärztinnen und Fachärzte für Gynäkologie Hysterektomien bei Frauen im Alter von 18 bis 79 Jahren: Ergeb-
nisse der Studie zur Gesundheit Erwachsener in Deutschland
und für Allgemeinmedizin (Frauen 5.0)’ received funding (DEGS1). Bundesgesundheitsbl 56(5/6):716–722
from the Innovation Fund of the Federal Joint Committee
9. Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen
(funding code: 01VSF16030). Fachgesellschaften e.V. (AWMF) (2015) Indikation und Methodik
der Hysterektomie bei benignen Erkrankungen. Registernummer
015 - 070.
Conflicts of interest http://www.awmf.org/leitlinien/detail/ll/015-070.html
The authors declared no conflicts of interest. (As at 08.02.2018)
Journal of Health Monitoring 2020 5(2) 11Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
10. Berufsverband der Frauenärzte e.V. (no date) Krebsfrüherken- 19. Bundeszentrale für gesundheitliche Aufklärung (2019) Verhütung
nung in der Krankenversicherung. in der Lebensmitte.
https://www.frauenaerzte-im-netz.de/frauengesundheit/krebs- https://www.familienplanung.de/verhuetung/wechseljahre/
frueherkennung-kfu/kfu-in-der-krankenversicherung/ (As at 30.03.2020)
(As at 01.04.2019) 20. Bundeszentrale für gesundheitliche Aufklärung (Ed) (2020) Ver-
11. Gemeinsamer Bundesausschuss (G-BA) (2020) Richtlinie des hütungsverhalten Erwachsener – Ergebnisse der Repräsentativ-
Gemeinsamen Bundesausschusses über die Früherkennung von befragung 2018. BZgA, Köln
Krebserkrankungen, (Krebsfrüherkennungs-Richtlinie/KFE-RL). 21. Zentralinstitut für die kassenärztliche Versorgung in Deutschland
https://www.g-ba.de/downloads/62-492-2002/KFE-RL_2019- (2016) Behandlungsfallzahlen von Frauen für die Fachgruppen
12-05_iK-2020-01-01.pdf (As at 25.05.2020) Allgemeinmedizin und Gynäkologie 2016, bundesweit. Sonder-
12. Deutsches Krebsforschungszentrum (dkfz) (2017) Brustkrebs. auswertung. Zi, Berlin
https://www.krebsinformationsdienst.de/tumorarten/brust- 22. Sapre S, Thakur R (2014) Lifestyle and dietary factors determine
krebs/frueherkennung.php (As at 01.04.2019) age at natural menopause. J Midlife Health 5(1):3–5
13. Gemeinsamer Bundesausschuss (G-BA) (2016) Geförderte Pro- 23. Schoenaker DA, Jackson CA, Rowlands JV et al. (2014) Socioeco-
jekte des Innovationsausschusses zur Förderbekanntmachung nomic position, lifestyle factors and age at natural menopause: a
Versorgungsforschung vom 8. April 2016. systematic review and meta-analyses of studies across six conti-
https://innovationsfonds.g-ba.de/downloads/media/50/Versor- nents. Int J Epidemiol 43(5):1542–1562
gungsforschung-Uebersicht-gefoerderte-Projekte-2016.pdf 24. No author (2018) Weniger Hormonpräparate gegen Wechseljah-
(As at 07.06.2019) resbeschwerden verordnet.
14. Kamtsiuris P, Lange M, Hoffmann R et al. (2013) The first wave https://www.aerzteblatt.de/nachrichten/96654/Weniger-
of the German Health Interview and Examination Survey for Hormonpraeparate-gegen-Wechseljahrsbeschwerden-verordnet
Adults (DEGS1). Sampling design, response, weighting, and (As at 30.03.2020)
representativeness. Bundesgesundheitsbl 56(5/6):620–630 25. Barber MD (2016) Pelvic organ prolapse. BMJ 354:i3853
15. Gößwald A, Lange M, Dölle R et al. (2013) The first wave of the 26. Hendrix SL, Clark A, Nygaard I et al. (2002) Pelvic organ pro-
German Health Interview and Examination Survey for Adults lapse in the Women’s Health Initiative: gravity and gravidity. Am
(DEGS1). Recruitment of participants, fieldwork, and quality J Obstet Gyneco 186(6):1160–1166
assurance. Bundesgesundheitsbl 56(5/6):611–619
27. Samuelsson EC, Victor FT, Tibblin G et al. (1999) Signs of genital
16. Heuer J (2016) Die 50 häufigsten ICD-10-Schlüsselnummern prolapse in a Swedish population of women 20 to 59 years of age
nach Fachgruppen aus dem ADT-Panel des Zentralinstituts, Jahr and possible related factors. Am J Obstet Gyneco 180(2 Pt 1):
2015. Zentralinstitut für die Kassenärztliche Versorgung in 299–305
Deutschland (Zi).
28. Robert Koch-Institut (Ed) und die Gesellschaft der epidemiologi-
https://www.zi.de/projekte/adt-panel/ (As at 24.09.2018) schen Krebsregister in Deutschland e.V. (Ed) (2019) Krebs in
17. von der Lippe E, Prütz F (2016) Age at natural menopause: Deutschland für 2015/2016. 12. Ausgabe. RKI, Berlin
Results from the German Health Interview and Examination 29. Bundesministerium für Gesundheit (BMG) (2017) Robert
Survey. Eur J Public Health 26(Suppl 1):301–302 Koch-Institut erstellt neuen Frauengesundheitsbericht. Presse-
18. Deutsche Gesellschaft für Gynäkologie und Geburtshilfe (DGGG), mitteilung.
Österreichische Gesellschaft für Gynäkologie und Geburtshilfe https://www.bundesgesundheitsministerium.de/presse/presse-
(OEGGG), Schweizerische Gesellschaft für Gynäkologie und mitteilungen/2017/1-quartal/beauftragung-rki-frauengesund-
Geburtshilfe (SGGG) (2019) Hormonelle Empfängnisverhütung heitsbericht.html (As at 26.05.2020)
(S3-Leitlinie, AWMF-Registernummer 015/015) 30. Brett KM, Madans JH (1994) Hysterectomy use: the correspon
https://www.awmf.org/leitlinien/detail/ll/015-015.html dence between self-reports and hospital records. Am J Public
(As at 30.03.2020) Health 84(10):1653–1655
Journal of Health Monitoring 2020 5(2) 12Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
31. Ohlmeier C, Frick J, Prütz F et al. (2014) Nutzungsmöglichkeiten
von Routinedaten der Gesetzlichen Krankenversicherung in der
Gesundheitsberichterstattung des Bundes. Bundesgesundheitsbl
57(4):464–472
32. Kolip P (Ed) (2000) Weiblichkeit ist keine Krankheit. Die Medika-
lisierung körperlicher Umbruchphasen im Leben von Frauen.
Juventa, Weinheim und München
33. Krause L, Prütz F (2020) Gynaecology and general practitioner
services utilisation by women in the age group 50 years and older.
Journal of Health Monitoring 5(2):15–25.
www.rki.de/journalhealthmonitoring-en (As at 30.06.2020)
34. Nowossadeck E, Prütz F, Thißen M (2020) Demographics of the
female population aged 50 years and older in Germany’s north east
region – Selected aspects. Journal of Health Monitoring 5(2):35–41.
www.rki.de/journalhealthmonitoring-en (As at 30.06.2020)
35. Statistisches Bundesamt (2017) Fallpauschalenbezogene Kranken-
hausstatistik (DRG-Statistik). Operationen und Prozeduren der
vollstationären Patientinnen und Patienten in Krankenhäusern.
www.gbe-bund.de (As at 17.09.2019)
Journal of Health Monitoring 2020 5(2) 13Journal of Health Monitoring Reasons for women aged 50 years and older to seek gynaecological advice and treatment FOCUS
Imprint
Journal of Health Monitoring
Publisher
Robert Koch Institute
Nordufer 20
13353 Berlin, Germany
Editors
Johanna Gutsche, Dr Birte Hintzpeter, Dr Franziska Prütz,
Dr Martina Rabenberg, Dr Alexander Rommel, Dr Livia Ryl,
Dr Anke-Christine Saß, Stefanie Seeling, Martin Thißen,
Dr Thomas Ziese
Robert Koch Institute
Department of Epidemiology and Health Monitoring
Unit: Health Reporting
General-Pape-Str. 62–66
12101 Berlin, Germany
Phone: +49 (0)30-18 754-3400
E-mail: healthmonitoring@rki.de
www.rki.de/journalhealthmonitoring-en
Typesetting
Gisela Dugnus, Kerstin Möllerke, Alexander Krönke
Translation
Simon Phillips/Tim Jack
ISSN 2511-2708
Note
External contributions do not necessarily reflect the opinions of the
Robert Koch Institute.
This work is licensed under a
Creative Commons Attribution 4.0 The Robert Koch Institute is a Federal Institute within
International License. the portfolio of the German Federal Ministry of Health
Journal of Health Monitoring 2020 5(2) 14Journal of Health Monitoring Gynaecology and general practitioner services utilisation by women in the age group 50 years and older FOCUS
Journal of Health Monitoring · 2020 5(2)
DOI 10.25646/6808
Gynaecology and general practitioner services utilisation by
Robert Koch Institute, Berlin
women in the age group 50 years and older
Laura Krause 1, Lorena Dini 2,
Franziska Prütz 1 Abstract
There are relatively few representative data on the utilisation of physician services in Germany and its influencing. Based
1
Robert Koch Institute, Berlin on data from the German Health Interview and Examination Survey for Adults (DEGS1, 2008–2011), we analyse the
Department of Epidemiology and
utilisation of gynaecology and general practitioner (GP) services, with a focus on women aged 50 years and older. We
Health Monitoring
2
Charité – Universitätsmedizin Berlin
compare these findings with data from the German National Health Interview and Examination Survey 1998 (GNHIES98)
Institute of General Practice and, based on this and further data, discuss possible developments. Figures for seeking GP services (over 80%) are
constantly high across the entire lifespan, whereas figures for gynaecology services drop with age. Around 60% of women
Submitted: 03.04.2020 aged 50 years and older go to a gynaecological practice at least once a year. Socioeconomic status and place of residence
Accepted: 22.06.2020
are important determinants for the utilisation of services. Around half of all women aged 50 years and older sought both
Published: 30.06.2020
gynaecology and GP services at least once over a one-year period. Under 10% had only been to a gynaecologist, and
around one third sought GP services only. Compared to GNHIES98, figures for GP and gynaecology services were
considerably higher in DEGS1, health insurance data, however, shows no increase in the use of gynaecology services
between 2008 and 2018. The results highlight the need to increase awareness among GPs of the needs of middle-aged
and older women for gynaecological consultation and treatment.
UTILISATION · GYNAECOLOGY · GENERAL PRACTITIONER · GP · WOMEN · GERMANY · DEGS1
1. Introduction women the relevant issues differ from those of women
still at reproductive age [5] and will be focused more on
Outpatient care in Germany is mainly provided by spe- cancer screening, menopause, uterine prolapse and
cialists in private practice [1].Generally, the use of outpa- incontinence [6–8]. In particular, the importance of can-
tient medical services is higher in women than in men cer screening increases: while a majority of women under-
[2, 3]. These differences by sex are most pronounced at go mammography and cervical cancer screening, uptake
a younger age. This is very likely due to, at least in part, still decreases with age [9]. A Focus article in this issue
the utilisation of gynaecological and obstetric services of the Journal of Health Monitoring analyses the Reasons
[3, 4]. However, adequate gynaecological care is impor- for women aged 50 years and older to seek gynaecolog-
tant at every stage in life; for middle-aged and older ical advice and treatment.
Journal of Health Monitoring 2020 5(2) 15Journal of Health Monitoring Gynaecology and general practitioner services utilisation by women in the age group 50 years and older FOCUS
Socioeconomic status (SES) and place of residence are Medical needs and the increasing number of older
DEGS1 important determinants for the utilisation of medical care women make it extremely important to ensure adequate
Data holder: Robert Koch Institute [2, 3, 10–15]. People in the low SES group more frequently gynaecological care also for this population group. The
Objectives: To provide reliable information about the seek general practitioner (GP) services, while those in the impact of these demographic developments is twofold –
population’s health status, health-related behaviour high SES group tend to visit medical specialists more often. both the population and doctors are ageing [19]. The effect
and health care in Germany including analysis of
temporal developments and trends.
People in cities see specialist physicians more often than is particularly notorious in rural regions, where ever fewer
those in rural regions, and people in rural regions more doctors attend to the needs of a growing number of older
Survey method: Questionnaires, physical examina-
tions and tests, a physician interview, a medication often GPs [2, 12]. people. A Fact Sheet in this issue of the Journal of Health
interview and laboratory investigations (blood and Regional differences also exist regarding the availability Monitoring describes the demographic developments for
urine sample).
of outpatient medical care [1]. The concentration of GPs and women aged 50 years and older in Berlin, Brandenburg and
Population: German resident population, aged 18
and above
medical specialists is greater for urban than for rural areas. Mecklenburg-Western Pomerania.
In Germany, the Associations of Statutory Health Insurance Funded by the Innovation Fund of the Federal Joint Com-
Sampling: Registry office sample; randomly selected
individuals from 180 communities in Germany were Physicians (KVen) have to ensure that everybody has access mittee (G-BA), the project ‘Frauen 5.0’ (Regionale Ver-
invited to participate (120 original sample points of to adequate levels of health care services in close proximity sorgung von Frauen über 49 Jahre durch Fachärztinnen
the German National Health Interview and Examina-
tion Survey 1998 and 60 new sample points). to where they live [16]. Need related planning is used as an und Fachärzte für Gynäkologie und für Allgemeinmedizin
Participants: N=8,151 (4,283 women; 3,868 men). The instrument to categorise types of doctors into different lev- [20]) has therefore assessed gynaecology and GP services
sample included persons who were newly recruited els of care (for example GP care, general medical specialist for women aged 50 years and older in the north east region
and those who had already participated in the Ger-
man National Health Interview and Examination Sur- care) with planning regions of different sizes. GP services (Berlin, Brandenburg and Mecklenburg-Western Pomera-
vey 1998 (mixed design). are planned at the smallest scale. For general medical spe- nia). The project aimed to gain an overview of actual levels
Response rate: 62% among revisiting participants cialist care, the level that includes gynaecologists, districts of care provided, and, based on this, develop concepts for
and 42% first time participants and district free towns are the basic unit of planning, taking adequate outpatient gynaecology services to this popula-
Survey period: 2008 to 2011 surrounding areas into account too. Need related planning tion group.
Data protection: DEGS1 is subject to strict compliance can be adapted according to regional conditions, for exam- This overview included a general analysis of the utilisa-
with the data protection regulations of the Federal ple, with regard to demographic factors. Regions with a tion of gynaecology and GP services by women focused
Data Protection Act and has been approved by the
Federal Commissioner for Data Protection and Free- higher proportion of older women, for example, are assumed on the age group 50 years and older, which is in the cen-
dom of Information in Germany. Charité – Univer to require fewer gynaecologists [16]. In 2019, in Oberspree- tre of this paper. Gynaecology services for this group are
sitätsmedizin Berlin’s ethics committee assessed the
ethics of the DEGS1 study and provided its approval wald-Lausitz, a district in the state of Brandenburg with a rarely the focus of such analyses. As we do not have any
(No.EA2/047/08). Participation in DEGS1 was volun- high proportion of women aged 50 years and older (58%), more up-to-date population representative data on the
tary. The participants were informed about the aims
and contents of the studies and about data protection. for example, there were nine gynaecologists per 100,000 utilisation of specialist medical services from Robert Koch
Informed consent was obtained in writing. people [17, 18]. In the district free town of Potsdam, where Institute (RKI) health monitoring, we have opted to take
More information in German is available at the proportion of women aged 50 years and older is smaller the following approach: based on data from the German
www.degs-studie.de
(41%), there were 24.5 gynaecologists per 100,000 people. Health Interview and Examination Survey for Adults
Journal of Health Monitoring 2020 5(2) 16Journal of Health Monitoring Gynaecology and general practitioner services utilisation by women in the age group 50 years and older FOCUS
(DEGS1, 2008–2011), we illustrate the utilisation of gynae- In addition to sex and age, DEGS1 also surveyed the
cology and GP services by women throughout their life- sociodemographic variables SES and place of residence.
time. For women aged 50 years and older, we will also SES was determined by applying a multidimensional index
analyse the utilisation according to SES and place of res- comprising data on education and occupational training,
idence, as well as the correlations between the use of occupational status and net household income (needs-
gynaecology and GP services. To evaluate trends, we will weighted). Based on this, participants were subdivided into
discuss utilisation data from DEGS1 by comparing it to low, medium and high SES groups [23]. As regards place
the figures reported in the precursor German National of residence, rural and urban environments are divided
Health Interview and Examination Survey 1998 (GNHIES98). into four subcategories: rural (100,000
screening uptake data. inhabitants) [2].
2. Methodology 2.2 Statistical methods
2.1 Sample design and study implementation
Based on DEGS1 data, the 12-month prevalence for the uti-
With DEGS1 the RKI has collected representative health lisation of gynaecology and GP services by 18- to 79-year-
data for the 18- to 79-year old German adult population. old women (n=4,283) was analysed over the course of age.
The study programme included interviews, physical exam- Then, the utilisation of gynaecology and GP services by
inations and tests. 8,151 people took part. A description of women in the age group 50 years and older was mapped,
the concept and design of DEGS1 has previously been pro- and differences by SES and place of residence were report-
vided [21, 22]. ed (n=2,287). Regarding indicators on utilisation, preva-
In addition to health status and health behaviour, a focus lences and the results of multivariate binary logistic regres-
was on the utilisation of health services. In this category, sion were calculated, as were average values and linear
DEGS1 asked about the use of medical specialists from dif- regression results for indicators of contact frequency.
ferent disciplines. Participants were asked how often during Regression analysis were adjusted for age (categorical),
the last twelve months they had seen a resident physician SES and place of residence. A statistically significant differ-
(12-month prevalence of utilisation). They could also report ence between groups is assumed for corresponding p-val-
how many times they had contacted physicians (12-month ues below 0.05. Cross table analysis between the uptake of
prevalence of contact frequency). Gynaecology and GP ser- gynaecology and GP services were then conducted in a final
vices were among the 13 specialisations participants could step and tested for correlations between the two variables
choose from [2]. by applying Pearson chi square tests.
Journal of Health Monitoring 2020 5(2) 17Journal of Health Monitoring Gynaecology and general practitioner services utilisation by women in the age group 50 years and older FOCUS
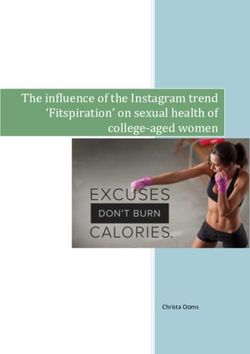
Figure 1 DEGS1 calculations were carried out using a weighting 90
Proportion (%)
12-month prevalence of the utilisation of factor that corrects deviations within the sample from the
gynaecology and general practitioner services by 80
population structure (as at 31 December 2010) with regard
18- to 79-year-old women over time (n=4,238) 70
to age, sex, region, German citizenship, district type and
Source: Modified according to Rattay et al. 2013 [2]
education [21]. All analyses were conducted with Stata 15.1 60
(Stata Corp., College Station, TX, USA, 2017) using the 50
DEGS1 data set (Version 18). Stata survey commands were
40
used in all analyses to account for the clustering of partici
pants at examination locations, weighting was used in the 30
calculation of confidence intervals and p-values [24]. 20
10
Utilisation of gynaecology 3. Results
services by women decreases 18 – 29 30 – 39 40– 49 50 – 59 60 – 69 70 – 79
Around 80% of women across all age groups take up GP Age group (years)
with age, figures for GP services within one year (Figure 1). For the use of gynae- General medicine Gynaecology
services are constantly high cology services, in contrast, 12-month prevalence decreas-
across all age groups. es with age, in particular for older age groups: while around annual utilisation of gynaecology services than women in
three quarters of 40- to 49-year-old women visited a gynae- higher status groups. In contrast, women from the high
cology practice during the 12-month period before the sur- SES group most seldom see a GP. Socioeconomic differ-
vey (75.4%), in the 50- to 59-year-old age group this figure ences are also evident for the 12-month prevalence of con-
drops to just over two thirds (68.7%). Over the entire tact frequency: women in the low and medium SES groups
lifespan, the 12-month prevalence for the utilisation of with 5.5 and 4.8 contacts respectively, saw GPs more often
gynaecology services almost halves, from 80.4% to 44.2% than women with high SES (3.6 contacts).
for 18- to 29-year-old and 70- to 79-year-old women, respec- For the utilisation of GP services by 50- to 79-year-old
tively. women, we can see differences in relation to place of res-
59.4% of the 50- to 79-year-old women have visited a idence (Table 1) – figures are lower for women living in
gynaecologist at least once within the past year. On aver- large cities than for those from rural areas. Overall, the
age, 1.5 contacts were made. 82.6% of women of this age statistical probability that a woman will have had at least
group consulted a GP at least once a year, with an average one appointment with a GP during the last year is 2.5 times
4.8 contacts made per year. higher for women living in rural areas. While we found no
Table 1 shows utilisation for 50- to 79-year-old women differences in relation to place of residence for the 12-month
according to SES: women in the low SES group show lower prevalence of gynaecology services utilsation, they were
Journal of Health Monitoring 2020 5(2) 18Journal of Health Monitoring Gynaecology and general practitioner services utilisation by women in the age group 50 years and older FOCUS
Table 1 Utilisation of gynaecology services Utilisation of general practitioner services
12-month prevalence for the utilisation of % (95% CI) OR (95% CI) p-value % (95% CI) OR (95% CI) p-value
gynaecology and general practitioner services Socioeconomic status
by 50- to 79-year-old women and results of Low 47.1 (41.1–53.1) 0.56 (0.37–0.84) 0.005 81.8 (75.8–86.6) 1.22 (0.82–1.82) 0.317
multivariate binary logistic regression analysis Medium 61.8 (58.5–65.0) 0.88 (0.65–1.20) 0.428 84.7 (82.4–86.8) 1.63 (1.19–2.23) 0.003
(odds ratios) by socioeconomic status and High 68.0 (62.3–73.2) Ref. Ref. – 75.7 (70.4–80.3) Ref. Ref. –
place of residence (n=2,287) Place of residence
Source: DEGS1 (2008–2011) Rural 55.6 (49.7–61.3) 0.79 (0.57–1.11) 0.175 89.6 (85.9–92.4) 2.46 (1.55–3.91) < 0.001
Small towns 56.4 (52.0–60.7) 0.78 (0.59–1.03) 0.076 82.4 (77.7–86.2) 1.29 (0.87–1.92) 0.208
Medium-sized towns 60.6 (55.8–65.2) 0.87 (0.66–1.15) 0.327 83.1 (80.0–85.8) 1.36 (0.96–1.91) 0.082
Large cities 62.8 (58.0–67.3) Ref. Ref. – 78.3 (73.3–82.6) Ref. Ref. –
CI=Confidence intervals, OR=Odds ratio, Ref.=Reference group
A considerable decrease in
found for contact frequency: whereas women in rural areas once per year (utilisation across all age groups is 69.6%)
the utilisation of gynaecology
on average visited a gynaecologist 1.3 times per year, the [2]. Analyses of the Study of Health in Pomerania (SHIP)
services is observed for figure was 1.8 for women in large cities. for the region Western Pomerania provide similar results
women in the 50- to 59-year Cross-table analysis reveals a correlation between the [25]: utilisation of gynaecology services decreases from
age group. 12-month prevalence for the utilisation of gynaecology and 86.3% to 36.6% for 20- to 29-year olds and women aged
GP services (pJournal of Health Monitoring Gynaecology and general practitioner services utilisation by women in the age group 50 years and older FOCUS
and that people in this group also less frequently use pre- which analyses the utilisation of outpatient services. In
vention-oriented services as early detection and screening 2008, 26.6% of the population took up gynaecology ser-
examinations [2, 30]. vices [32], in 2018 25.0 % [33]. In the case of utilisation,
Differences in the utilisation of GP and specialist med- therefore, no important developments were found, these
ical services by the German population found between figures were, however, not differentiated by age groups.
urban and rural areas [2, 12] are in part reflected in the Due to the different data basis and methodology (such
group of women aged 50 years and older: compared to as including men in the calculations) a comparison with
women in large cities, women in rural areas more frequently the DEGS1 data is not possible. Data on the utilisation of
seek GP services, with no differences between urban and cancer screening examinations provides further indica-
rural areas found for the utilisation of gynaecology services. tions of more recent developments. The current wave of
The study by Stentzel et al. [31] confirms this finding, show- the German Health Update (GEDA 2014/2015-EHIS) study
Around one third of women ing that even when gynaecologists are hard to reach, this of the Robert Koch Institute reported that 53.1% of women
does not impact the use of services. According to DEGS1 aged 20 years and older had a screening examination for
aged 50 years and older
data, women in rural regions report having made less con- cervical cancer (pap smear) during the last twelve months.
had an appointment with a tact with gynaecology practices within the last year than The proportion was highest for 30- to 34-year-old women
GP only and not with a women in large cities. These results call for further anal (67.9%). Of 60- to 64-year-olds, fewer than half (49.0%)
gynaecologist. ysis of differences in the utilisation of gynaecology services had this examination, in the age group 70 years and older
also with regard to the actually available services. less than a third (29.7%) [9]. Analyses of data from the
From GNHIES98 to DEGS1, the use of GP services by German Mammography Screening Programme show that
women has increased considerably across all age groups 49% of women who were invited to the Mammography
[2]. When observed as a whole, utilisation of GP services Screening Programme did take part in 2017. From 2008
has increased by 10% between the two surveys, from to 2013, participation rates by invited women increased,
70.9% to 79.4%. An increase in utilisation has also been but have been decreasing since 2014. An increase in par-
registered for gynaecology services. This increase is ticipation rates was only observed for women who had
mainly owing to older age groups: for the 60- to 69-year- already previously taken part in screening and had been
old age group, use of gynaecology services has increased invited again [34]. Mammography screening does not take
by 18%, from 44% in GNHIES98 to 62% in DEGS1, in the place in gynaecology practices. However, this could be an
70- to 79-year-old age group there has even been a 24% opportunity to seek consultation in a gynaecology prac-
increase from 21% to 45%, respectively [2]. Health insur- tice. Further reasons for consultation and treatment that
ance claims data can help estimate whether the utilisa- play a role for women aged 50 years and older beyond
tion of services has continued to increase since. Every cancer early detection are discussed in a second Focus
year, the BARMER health insurance provides a report article in this issue of the Journal of Health Monitoring.
Journal of Health Monitoring 2020 5(2) 20You can also read