A five-year plan (2021-2026) to improve mental health, suicide prevention and alcohol and other drug treatment services in Western Queensland
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

DRAFT FOR PUBLIC CONSULTATION
A five-year plan (2021-2026) to improve
mental health, suicide prevention
and alcohol and other drug treatment
services in Western Queensland
Sponsored by:
Western Queensland
Primary Health Network,
Central West HHS,
North West HHS and
South West HHS
WESTERN QUEENSLAND
An Australian Government Initiative
Forward
For inclusion in version 2 February 2021
2
Contents
Forward 2 Part B: Delivering change 27
List of acronyms 4 1. Building a connected and person-centred care sector 28
Executive summary 5 2. Proactive prevention and early intervention 31
Gayaa Dhuwi (Proud Spirit) declaration 6 3. Promote and protect mental health and wellbeing
across the lifespan 34
How mental health impacts us 7
4. Supporting Aboriginal and Torres Strait Islander
Our plan 8
social, emotional and cultural wellbeing 37
State and national policy context 9
5. Strengthen and integrate alcohol and other drug
Challenges and opportunities 10 treatment and harm reduction within a stepped
care framework 40
Developing this plan 13
6. Making suicide prevention everyone’s business 45
Summary of findings 15
7. Coordinating treatment and support for people who
Our population 18 experience severe and complex mental health 47
Part A: Transforming mental health care 22 8. Building workforce capability and grassroots
training opportunities 50
Place-based, co-designed planning approach 23
9. Responding to climatic extremes and these impacts
The Western Queensland Health Care Home Model of Care 24 within rural and remote communities 53
Stepped Care Framework for mental health services 25
Part C: Measuring change 56
Making safety and quality central to mental health
service delivery 26 Reporting and measuring progress 56
Addressing stigma and discrimination 26 Implementing the Plan 56
Performance monitoring indicators 57
Bibliography 58
3
List of acronyms
ABS Australian Bureau of Statistics MHNIP Mental Health Nurse Incentive Program
ACCHO Aboriginal Community Controlled Health Organisation MHSPAOD Mental Health Suicide Prevention, Alcohol and Other Drugs
ACCHS Aboriginal Community Controlled Health Service MICRRH Mount Isa Centre for Rural and Remote Health
AEDC Australian Early Development Census NDSS National Diabetes Services Scheme
AIHW Australian Institute of Health and Welfare NGO Non-Government Organisation
AHPRA Australian Health Practitioner Regulation Agency NHPA National Health Performance Authority
AOD Alcohol and Other Drugs NMHSS Nukal Murra Health Support Service
ASR Age Standardised Rate NMHSPF National Mental Health Service Planning Framework
ATAPS Access to Allied Psychological Services NWHHS North West Hospital and Health Service
BAP Better Access Program NWRH New Ways Real Health
CACH Cunnamulla Aboriginal Corporation for Health PBS Pharmaceutical Benefits Scheme
CWHHS Central West Hospital and Health Service PHIDU Public Health Information Development Unit
COPD Chronic Obstructive Pulmonary Disease PHN Primary Health Network
CWAATSICH Charleville and Western Areas Aboriginal and Torres PP Private Practice
Strait Islander Community Health RACF Residential Aged Care Facility
CWHHS Central West Hospital and Health Service RFDS Royal Flying Doctor Service
ED Emergency Department SA2 Statistical Area Level 2
EPC Enhanced Primary Care SD Statistical Division
FTE Full Time Equivalent SEIFA Socio-Economic Indexes for Areas
GP General Practitioner SMO Senior Medical Officer
HNA Health Needs Assessment SWHHS South West Hospital and Health Service
HHS Hospital and Health Service WQPHN Western Queensland Primary Health Network
IRSD Index of Relative Social-Economic Disadvantage WQHSIC Western Queensland Health Service Integration Committee
LGA Local Government Area WQ HCH Western Queensland Health Care Home
LGBTIQ+ Lesbian, gay, bisexual, transgender, intersex, QLD Queensland
people and/or queer people
MBS Medicare Benefits Scheme
4
Executive summary
TBC
WESTERN QUEENSLAND
An Australian Government Initiative
5
Gayaa Dhuwi (Proud On 27 August 2015, the National Aboriginal and Torres Strait Islander Leadership in Mental Health
launched the Gayaa Dhuwi (Proud Spirit) declaration.
Spirit) declaration This declaration sets out five themes that are central to the development and implementation of the Fifth
National Mental Health and Suicide Prevention Plan and the Western Queensland Social, Emotional and
Cultural Wellbeing Plan.
We are committed to working 1. Aboriginal and Torres Strait Islander concepts of social and emotional wellbeing, mental health and
healing should be recognised across all parts of the Australian mental health system, and in some
with Aboriginal and Torres circumstances support specialised areas of practice.
Strait Islanders leaders to
2. Aboriginal and Torres Strait Islander concepts of social and emotional wellbeing, mental health and
ensure Australia’s mental healing combined with clinical perspectives will make the greatest contribution to the achievement of
health system achieves the the highest attainable standard of mental health and suicide prevention outcomes for Aboriginal and
Torres Strait Islander peoples.
highest attainable standard
of mental health and suicide 3. Aboriginal and Torres Strait Islander values-based social and emotional wellbeing and mental health
outcome measures in combination with clinical outcome measures should guide the assessment of
prevention outcomes for mental health and suicide prevention services and programs for Aboriginal and Torres Strait
Aboriginal and Torres Strait Islander peoples.
Islander peoples 4. Aboriginal and Torres Strait Islander presence and leadership is required across all parts of the
Australian mental health system for it to adapt to, and be accountable to, Aboriginal and Torres Strait
Islander peoples for the achievement of the highest attainable standard of mental health and suicide
prevention outcomes.
5. Aboriginal and Torres Strait Islander leaders should be supported and valued to be visible and
influential across all parts of the Australian mental health system.
6
How mental
1 in 4
Neary half of all Australians (25%) of young adults
health impacts us will experience mental health aged between 16 and 24
issues in their lifetime will experience mental
Over the course of our lifetime, health issues2
every one of us will be touched by
mental health, suicide and alcohol
and other drug (AOD) issues. Mental health can be One in five (20%)
Australians will experience
Getting the right type of support at
the right time is essential to improve
affected by genetics,
lifestyle and environment
20% a common mental disorder
the mental health and wellbeing of over a 12 month period2
our communities.
We all play a role in recognising the Social problems include
triggers and warning signs of mental People living in low socio-economic
poverty, unemployment,
health issues in order to access areas are 1.4 times more likely
support for ourselves along with homelessness, isolation
to have mental health issues2
supporting friends, neighbours and and stigma
families to seek help.
All of have a responsibility to
promote protective factors for good In Western Queensland In Western Queensland
mental health and wellbeing, and to people present to emergency risky alcohol consumption is
support the most vulnerable in our departments with mental 1.4 times more common than in
communities, including children
and young people whose future health issues 1.6 times more other parts of Queensland3
health and wellbeing relies on the than the rest of Queensland1
people around them, and access
to services.
2x
Suicide and self-inflicted
injury rates are twice as high
in Western Queensland than
the rest of Australia2
7
Our plan
The Plan
This comprehensive five year Mental
Health Suicide Prevention and Regional approach for collaborative action on mental health
Alcohol and Other Drug (MHSPAOD) and related services.
Plan (herein known as the ‘Plan’) is a
refresh of the first Plan (2017-2020).
Consumers, carers, people with a lived experience
Our Plan has been developed
using a co-design process with our
partners and other key parties who
have committed to working together WQPHN Consortium representatives
to achieve better health and social WQPHN
outcomes in Western Queensland Nukal Murra Alliance
North West HHS Health care providers
through integration in planning,
service delivery and evaluation. Central West HHS Clinicians
South West HHS Consumers
Importantly, it incorporates the ideas
and feedback from consumers, carers
and people with a lived experience.
Key stakeholders
The Plan sets out shared objectives, Local government Peak bodies
an agreed set of actions and key General Practice Networks
responsibilities to address priority Health care providers
Aboriginal and Islander WQPHN Clinical and
areas. It includes a regional approach Community Controlled Health
for collaborative action to improve Services (AICCHSs) Consumer Councils
integrated mental health and
related services.
Western Queensland Community
8
State and national policy context
Our Plan builds upon the Fifth National Mental Strategy and National Natural Disaster Mental
Health Plan 2017-2022 (Fifth Plan), existing state and Health Framework.
commonwealth MHSPAOD services along with the
national health and mental health reforms.4 The Plan was developed following engagement
with target groups such as consumers with severe
It incorporates reform and system transformation psychosocial disability and alcohol and other drugs
recommended by the PHN Advisory Panel on (AOD) services, to strengthen their interface with
Mental Health and also considers a range of state and the National Disability Insurance Scheme (NDIS)
national mental health and suicide prevention policy as mental health reforms are implemented across
reviews including: communities.
y Productivity Commission, Mental Health
Finally, it has been shaped within the context of
Inquiry Report5
Queensland Government’s Connecting Care to
y The National Drug Strategy 2017-20266 Recovery 2016-2021 Plan9 for state funded mental
health, alcohol and other drug services, and within the
y The Queensland Mental Health Commission’s
vision of My health, Queensland’s future: Advancing
(QMHC) Shifting Minds7 and Every Life
health 2026.10
Strategic Plan.8
Our goals and vision align to create a system that
This is a dynamic Plan that will be regularly reviewed
works better for individuals, families and communities
and updated to ensure inclusiveness of contemporary
by strengthening collaboration and promoting
material such as the Productivity Commission, the
effective integration, thus enabling better connected
National Mental Health Commission releases, the
care and recovery oriented services.
National Children’s Mental Health and Wellbeing
9
Challenges and opportunities
Challenges of delivering mental health
care in Western Queensland
Positive social, emotional and cultural wellbeing is
important for all people and communities in Western
Queensland. Yet the impact of mental ill health,
problematic AOD use and suicide across the region
presents many challenges.
A significant number of people in Western Queensland
continue to experience social dislocation, economic
hardship and isolation which contributes to poor
mental health and risky AOD use, with the impacts
going far beyond the health sector.
There is significant health disparity and gaps in
access to services and economic participation for the
most vulnerable and at-risk populations for Western
Queensland compared to city or urban regions.5; 11
10Vulnerable communities
While there are pockets of social and economic advantage, large areas of
Western Queensland experience extreme disadvantage compounded by
social determinants which result in high levels of mental health issues or
distress, suicide and problematic relationship with AOD use.
The health workforce
The Western Queensland health workforce is predominately generalist in
nature. This presents a challenge in providing integrated, specialised and
holistic care.
Transient populations with high need
In Western Queensland, there are significant numbers of fly-in/fly-out
workers (FIFO), seasonal workers and tourists (particularly grey nomads)
leading to skyrocketing demands for health services during the
peak seasons.
Geographical challenges
Western Queensland’s vast landscape means people travel long distances
to access services. Many experience factors that contribute to increased
mental health risk including:12
y Geographical isolation
y Telecommunication constraints
y Poor access to public transport
y Extreme weather conditions such as flood and drought
y A small population spread across widely dispersed communities.
11Opportunities for improving mental health The region’s AICCHO sector has been strengthened Partnerships
through the Nukal Murra Alliance improved social
care in Western Queensland and emotional wellbeing which provides significant Continue building on local, regional and state
cultural leadership capacity and change needed to collaborations and partnerships to support
Western Queensland’s MHSPAOD system has address entrenched mental health-related stigma, improvements and momentum to achieving
undergone significant transformation including.13 shame and discrimination for First Nations people in better mental health and wellbeing outcomes for
the region.14 Western Queenslanders.
y Emphasis on recovery-oriented practice and
widespread adoption of harm minimisation
Other opportunities for reform Western Queensland Foundation Plan
y Increased focus on creating pathways for
consumers, carers and people with a lived Place-based approaches The Western Queensland Foundation Plan has
experience to participate, influence and lead positioned the sector well to consolidate and build on
co-design of a better mental health system for Continue adoption of place-based approaches the important ground work in the MHSPAOD space
Western Queensland. to harness the strengths and enable communities and lead reform across our region. Learnings and
to lead and support their own wellbeing including recommendations from the Foundation Plan have
There has also been a shift away from siloed, wrapping care around the people who need it most. helped shape this Plan.
organisational centric care to a focus on a better
integrated and coordinated primary mental health
system of care.
12Developing this plan
Review of the Foundation MHSPAOD Plan
2017–2020
WQPHN contracted the Substance Use and Mental
Health Unit at the Centre for Health Services Research
at The University of Queensland to conduct an
independent evaluation of the foundation MHSPAOD
Plan 2017-2020.12 Areas of evaluation included
implementation, effectiveness, achievements,
strengths and areas for improvement.
The evaluation consisted of semi-structured interviews
with key informants involved in a variety of roles related
to the planning or delivery of mental health services
across Western Queensland. The findings of this
evaluation have informed the direction and objectives
of this Plan.
13Summary of findings
Areas of strength Areas of potential improvement Recommendations
Overall, the majority of key informants were highly While the majority of key informants praised the 1. The development of a complementary
complementary of the Plan’s implementation (in implementation and content of the Plan, key communication strategy
particular its focus on place-based implementation informants also highlighted areas of potential
2. The development of a complementary
and stakeholder input), and emphasis on improvement for the 2021-2026 Plan in the
implementation plan
collaboration, co-design, team care, cross referrals, following areas:
and consumer input. 3. Formation of a new Consortium for the
y Greater distinction of: 2021-2026 Plan
In particular, most key informants recognised the ▸ Implementation milestones 4. Inclusion of an executive summary at the
WQPHN’s significant efforts in co-designing and ▸ Service use characteristics beginning of the document
implementing an innovative Plan that represents
substantial progress in improving the mental health ▸ Visibility of cross referrals 5. Further explanation of the Stepped Care model
and wellbeing of Western Queensland’s residents. 6. Review of the Plan by the Consumer
▸ Improved mental health outcomes among
priority populations Advisory Council
Most key informants perceived that the Plan had a
strong focus on promoting consumers’ and service ▸ Involvement of Aboriginal and Torres Strait 7. Distribution of written and multimedia material
providers’ awareness of Western Queensland’s Islander people in the Plan’s design and promoting the Plan
MHSPAOD Services across the continuum of care, implementation 8. Host in-person and online workshops/training
and a promotion of General Practice settings as key introducing new Plan
y Utility and effectiveness of Stepped
providers of mental health care.
Care model 9. Review and implementation of Patient Reported
The majority of key informants believed the Plan y Involvement and activities of the Consumer Experience Measures (PREMs) and Patient
had a clear focus on addressing existing disparities Advisory Council Reported Outcome Measures (PROMs) systems
in mental health support targeted at Aboriginal and 10. As part of communication strategy, regular
y How to measure relevant outcomes
Torres Strait Islander and other priority populations. progress updates
In particular, several key informants commended the y Occasional lack of integration, communication
Nukal Murra Alliance for allowing the perspectives and collaboration between various agencies 11. Continued hosting of mental health round tables
of Aboriginal and Torres Strait Islander-led health and services 12. Ongoing seminars to disseminate
services in creating and implementing the Plan. data-driven updates.
y Lack of understanding of some aspects of the
Stepped Care model
Finally, the majority strongly endorsed the Plan’s
focus on integration of the Stepped Care model, in y Lack of opportunities for consumer feedback.
particular the model’s promotion of cross-referral
between services.
14Western Queensland Stewardship
Consortium
The Western Queensland Health Service Integration Committee
(WQHSIC) has provided overarching stewardship for this Plan’s The Western Queensland
development and will provide ongoing support for its approval Consortium brings together
and implementation under the Maranoa Accord. stakeholders and consumer
representatives who have
Plan sponsors considered contemporary
evidence, Commonwealth and
y WQPHN Queensland policies and our
y North West HHS unique local context in order
to consider joint approaches
y Central West HHS that leverage from integrated
y South West HHS. care, stepped care and joint
commissioning.
Plan partners
Our Plan is a road map
y Nukal Murra Alliance grounded in evidence and
consumer expectations. The
y Clinical and Consumer Councils Consortium and working
y Health care providers groups are the touch points for
implementation and co-design.
y Clinicians
y General Practice networks
y Aboriginal and Islander Community Controlled
Health Services (AICCHSs)
y NGOs
y Local government
y Peak bodies
y People with lived experience and carers.
15Western Queensland Stewardship
Western Queensland Health Services Integration Committee
WQ MHSPAOD Consortium
Western Alliance
WQPHN Clinical &
Nukal Murra Alliance QAIHC AOD Mental Health
Consumer Council
(WAMH)
Queensland Health
Headspace RHealth Child & Youth Lived Experience
MHAOD Branch
Qld Mental Health North West HHS
Older Person's MH MHNiGP rep Roses in the Ocean
Commission MHAOD
Australian
Psychological GP (special
QNADA CheckUP Central West HHS
Society MHSPAOD
MHAOD
(Telehealth) interest)
Health Workforce University of Qld RFDS (Qld Section) NDIA South West HHS
Qld MHAOD
The Plan will not over-ride existing funding agreements, service agreements or broader jurisdictional planning
or business protocols. However, it will be used to guide commissioning and delivery of mental health, AOD and
suicide prevention services. Having clear roles and responsibilities linked to implementation at a regional level
will enable measurement and review of progress against the shared objectives and actions.
1634%
Community engagement
Our Plan:
of PARTICIPANTS
y Aims to improve mental health, reduce the
risk of suicide and address AOD issues in a
31 EVENTS
sustainable way
y Is underpinned by the principles of early
were carers and people with a
engagement, inclusivity, transparency, lived experience
shared power, equity of knowledge
and responsibility
11 2
y Builds on the strengths and abilities of local
communities and services
y Was developed through a 12-month
co-design process
y Empowers local communities through
co-creation and co-design.
LOCATIONS SURVEYS
3 CONSUMER
FACEBOOK CAMPAIGNS
17manton
manton
WQPHN COMMISSIONING
WQPHN COMMISSIONING
LOCALITIES
LOCALITIES
reek Lower Gulf
reek
y
Mornington
Island
Lower Gulf
Our population
ay
Mt Isa and Surrounds
Mt Isa and Surrounds
Western Corridor
Karumba
Western Corridor Geography and demography
Normanton
Winton Burketown Central West
Winton Muttaburra Central West
Doomadgee
Muttaburra WQPHN is the fourth largest PHN in Australia,
Gregory Far South West
Aramac
Aramac Far South West with a total land area of 956,438 km2 – equating to
Longreach Maranoa 55% of the total land area of Queensland.
Longreach Barcaldine Alpha Maranoa
Barcaldine Alpha
Jericho Balonne
Camooweal Isisford
Jericho Balonne Home
WQPHN to:
COMMISSIONING
15
Stonehenge Isisford Blackall HOSPITAL AND HEALTH LOCALITIES
Blackall HOSPITAL AND HEALTH
62,369 people
Stonehenge
Jundah Yaraka Tambo SERVICE BOUNDARIES
Jundah Mount Isa
Yaraka Cloncurry Julia Creek
Tambo SERVICE BOUNDARIES Lower Gulf
Windorah
Windorah McKinlay North West HHS Mt Isa and Surrounds
10,435 17.2% are
Augathella Injune North West HHS
Urandangi Dajarra Augathella Injune
Western Corridor
Quilpie
Charleville
Charleville
Mitchell Roma Indigenous Australians
Morven Mitchell
Winton Roma Central West
Quilpie Muttaburra Central West HHS
Morven Wallumbilla
34 Aboriginal language groups
Central West HHS
Boulia Wallumbilla
Surat Aramac Far South West
Surat
Longreach Maranoa
Barcaldine Alpha
Thargomindah Cunnamulla St George
34% under 25
Balonne
Thargomindah Cunnamulla St George Jericho
Bollon South West HHS
Bedourie Isisford
Bollon Dirranbandi South West HHS
Stonehenge Dirranbandi Blackall HOSPITAL AND HEALTH
Mungindi SERVICE BOUNDARIES
88% of the population live in
Jundah Yaraka Tambo
Mungindi
Windorah
remote
North Westand
HHS very remote areas
Augathella Injune
Birdsville
Quilpie
Charleville Mitchell Roma 61% of the regions population
Morven
Wallumbilla
are in the
Central two most disadvantaged
West HHS
Surat quintiles (SEIFA)
Thargomindah Cunnamulla St George
Bollon South West HHS
Dirranbandi
Mungindi
1837, 914
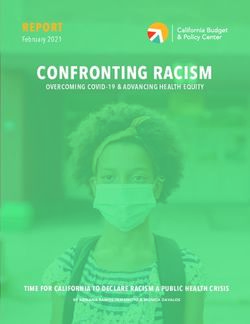
Prevalence rates
14351
The National Mental Health Service Planning
Framework (NMHSPF) is a tool developed by
the University of Queensland to assist with the 5494
prediction of the prevalence of mental health
conditions and demand for mental health services.
2774
1836
It utilises national averages which are applied to the
population of a region (in this case the estimated
resident population in June 2018 as determined
by the Queensland Government Statistician’s At risk Mild Moderate Severe Well
Office, Queensland Treasury).16 These averages population
do not yet account for rurality and remoteness, 37, 914
Aboriginal and Torres Strait Islanders or people with
low socio-economic status – all of which are higher
in Western Queensland and are known factors
that contribute towards increased mental health 23% At risk
prevalence. As such the figures from the NMHSPF
14351 to assist in planning and
are a conservative estimate
coordination of services.
9% Mild
The figure to the right provides the estimated 4% Moderate
5494
mental health prevalence across severity levels
(severe, moderate, mild, at risk and well population) 3% Severe
in Western Queensland with the graph showing 2774the
estimated number of people in each category and
1836 61% Well population
the pie graph showing the percentage of
the population.
At risk Mild Moderate Severe Well
population
Estimated prevalence of mental health in the Western Queensland population
19Treatment targets
When adjusting for treatment targets based on
severity level relative to the estimated number
of people at each level, approximately 1 in 5
people are in need of mental health treatment.
This estimate of demand against the WQPHN
population of 62,369 suggests
that approximately:
y 3,129 (5.0% of the WQPHN population)
will require early intervention and relapse
prevention. They represent people who do
not yet meet the criteria for a mental disorder
and those that previously experienced
a mental disorder, but no longer have a
diagnosable disorder.
y 2,747 (4.4% of the total WQPHN population)
will need a variety of services to treat mild
mental illness/disorders
y 2,220 (3.6% of the WQPHN population)
will need services for moderate mental
illness/disorders
y 1,836 (2.9% of the WQPHN population) will
need services for severe mental illness.
20Overview of the Plan Part A: Transforming mental health care
y WQ HCH – supporting a patient centred approach to care
Our Plan incorporates three discreet and y Embedding stepped care framework for mental health services
complementary areas of work including:
y Adopting a place-based, co-designed planning approach
y Mental health y Making safety and quality central to mental health service delivery
y Suicide prevention y Addressing stigma and discrimination.
y Alcohol and other drugs (AOD) services.
It identifies significant opportunities for both Part B: Delivering change
service and system improvement based on y Proactive prevention and early intervention
extensive engagement and feedback from
y Providing care across the lifespan
people who live and work in the region. This
includes improvement to existing services y Supporting Aboriginal and Torres Strait Islander social, emotional
along with enhancements to commissioning and cultural wellbeing
approaches and services. y Strengthening and integrating AOD treatment and harm reduction
y Making suicide prevention everyone’s business
The Plan also identifies opportunities to expand
y Supporting people who experience severe and complex mental health
and tailor service delivery in conjunction with
ongoing co-design and health planning linked to y Building workforce capability and grassroots training opportunities
future service demand. y Responding to climatic extremes and rural decline.
It makes no commitment to funding for
additional future services, but instead commits Part C: Measuring change
to shared regional resource planning through
the Consortium to consider proposed new or y Measuring individual and service system outcomes
extended services. y Reporting and measuring progress
y Implementing the Plan.
21Make safety
Our vision: Western
and quality
central to health
service delivery
Queenslanders and
their communities Adopt
place-based,
experiencing good co-designed
planning
approaches
Embed a
stepped care
mental health and framework for
mental health
wellbeing. Part A:
services
Transforming
mental health care
Implement
Address the Western
stigma and Queensland Health
discrimination Care Home
(WQ HCH) model
of care
22As individuals we contribute to and are Place-based, co-designed
affected by both the social and physical planning approach
environments of our communities. Western Queensland communities face multiple
challenges and often ‘wicked’ problems that are
complex and difficult to solve. These problems often
relate to living conditions, societal influences, limited
In turn, this can have an impact on access to services, geographical isolation, and ‘siloed’
funding models.
people’s health and wellbeing. A sense To address these problems we require a coordinated
of belonging and feeling connected and cohesive approach that recognises and champions
the important role communities play in shaping services
to others with strong and supportive and embedding consumer, carer and lived experience
engagement into planning.
networks matters for people’s
wellbeing. As a community, this This Plan presents our blueprint for implementing
stepped care using place-based, co-design approaches.
protects against risk factors.17 It harnesses the leadership, resources and opportunities
of people and seeks contributions to strategies
and ideas to improve health, social, economic and
environmental outcomes.17
It embeds meaningful public and multi-stakeholder
participation into service delivery and offers
opportunities for Western Queensland organisations to
address challenges and work together.
Ultimately, this is about reducing inequalities by
improving the social, emotional and cultural wellbeing
of our people and places.
23The Western Queensland Health
Care Home Model of Care
Western Queensland Health WQ HCH provides the gateway
Care Home (WQ HCH) model to the wider health system through
provides proactive patient-centred, access to community-based
coordinated and flexible care with multi-disciplinary team-based
a team of professionals working care, early intervention services,
together to make sure the patient and hospital and specialist services
receives care, based on their needs. where these are required to:
At the heart of this model is a y Identify lifestyle and other
whole-of-system integration health risk factors early
approach that is focused on y Proactively manage people with
improving patient outcomes and chronic disease
experiences and places consumers
at the heart of the local primary y Help vulnerable people navigate
care system. the health care system
y Support people who
This model of care is conceptualised are geographically isolated
within three core domains that or who suffer economic
support general practitioners to disadvantage
deliver holistic assistance close
to people’s homes; and where y Support people with complex
individuals, families and carers are mental health care needs
active partners in a person’s y Remove the organisational
care journey: and professional barriers that
y Ready Access to Care impact care and prevent better
coordination across social,
y Proactive Preventative Care primary and acute care settings.
y Engaged Chronic and
Complex Care.
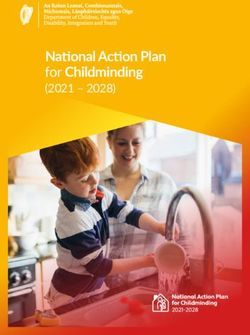
24Step 4: Services for severe and
3% complex mental health needs Case management
Severe
4% Step 3: High intensity
Moderate mental health services Risk management &
The stepped care approach
Step 2: Low intensity early intervention
9% is flexible - as a person’s
Mild mental health services needs change, the service
changes with them,
ensuring the service type is
23% Step 1: Identification, right for them.
At risk groups assessment, active
monitoring
Self management
61% Not receiving
treatment
Well Population
Stepped Care Framework for mental health services
The Stepped Care Framework describes a hierarchy A stepped care approach to mental health service y Define a comprehensive ‘menu’ of evidence
of interventions. These interventions range from planning generally involves the following five based services required to respond to the
lower intensity steps that support people before core elements:18 spectrum of need
illness manifests, to higher levels of care for those
y Use the least restrictive or intensive treatment y Match service types to the treatment targets for
who present with severe symptoms.
option appropriate to the individual’s needs each needs group and commissioning/delivering
services accordingly.
Under this framework people are assessed on their y Stratify the population into different ‘needs groups’,
needs and then allocated appropriate support. ranging from whole of population needs for mental
Regular monitoring ensures that people continue to health promotion and prevention, through to those
receive the right help as their needs change with severe, persistent and complex conditions
over time.
y Set appropriate interventions for each stratified
group (this is necessary because not all needs
The service intervention continuum allows people
require formal intervention)
to enter the mental health care system at any level to
make best use of workforce and technology.18
25Making safety and quality Addressing stigma and
central to mental health discrimination
service delivery Reducing stigma and discrimination is at the core
of all our efforts to improve mental health and
Our work across the mental health sector to advance wellbeing, and break down barriers to
safety and quality in the health sector aligns with the access support.
work of the Australian Commission on Safety and
Quality in Health Care (ACSQHC). Shame and discrimination can contribute to
unemployment, social exclusion and poverty
This Plan focuses on building a recovery-oriented and can trap people in a cycle of marginalisation
culture across all health services involved in that impacts on their physical, social and
the delivery of mental health, AOD and suicide emotional health.
prevention treatment and care.
Our outback culture, lifestyles and social
This will be achieved by: norms play a very important role in the way we
understand and talk about mental health, suicide
y Adopting the safety and quality commitments and AOD use, including how, where and when
of the Fifth Plan that include the National Safety help is sought.
and Quality Health Service (NSQHS) Standards
(second edition) and National Standards for Whether it’s those well recognised stoic
Mental Health Services (NSMHS) behaviours within our farming communities, or
y Monitoring and improvement of mental health the unique intergenerational experiences of our
services through measuring progress and Aboriginal and Torres Strait Islander communities,
reporting on indicators, such as timely access or even the ‘she’ll be right’ attitudes and
and effectiveness of care as measured by patient mindsets that have prevailed across generations;
experience and continuity of care as measured by addressing stigma and discrimination will require
follow-up after hospital admissions. disruption and this Plan needs to support
and enable Western Queenslanders through
understanding and adopting important protective
factors and normalising help seeking behaviours
linked to recovery and wellbeing.
26PART B: Delivering change
Our Plan identifies system redesign priorities
through a commitment to nine focus areas
for change.
1. Building a connected 2. Proactive prevention 3. Promote and protect
For each focus approach area, we provide: and person-centred and early intervention mental health and wellbeing
care sector across the lifespan
y Consultation insights
from this strategy’s supporting community
engagement program
y Shared objectives
y Priority actions designed
to improve the quality, integration
and coordination of MHSPAOD care.
4. Supporting Aboriginal 5. Strengthen and integrate 6. Making suicide prevention
and Torres Strait Islander Alcohol and Other Drug everyone’s business
social, emotional and treatment and harm reduction
cultural wellbeing within a stepped care framework
7. Coordinating treatment 8. Building workforce 9. Responding to climatic
and support for people capability and grassroots extremes and these
who experience severe and training opportunities impacts within rural and
complex mental health remote communities
27Focus area 1: Building a connected and person-centred care sector
‘We need to open doors to care by ‘We need 'community of
listening to people with a excellence’ models with planned
lived experience’ services and integration across all
providers within one community
Lived Experience Participant
or place’
‘Using information systems that NW Mental Health Roundtable
don’t talk is problematic and leads Mount Isa
to consumers falling through the
gaps, lost data and a breakdown in ‘We need to inter-link culture and
care continuity’ clinical responsiveness in order
to be able to deliver culturally
General Practitioner
safe services’
‘We need to recognise and be Aboriginal Health Practitioner
responsive to the different cultures
across Western Queensland ‘It’s no long a ‘taboo’ subject and
from Indigenous, Bush and stigma has decreased somewhat,
GP practices, primary care
Mining cultures’ but we still have a long way to go’
clinics and AICCHOs were
rated highest in supporting Consumer Forum Meeting Lived Experience Focus Group
consumer confidence and
recovery of care. ‘We need to expand cross agency ‘Stop the silo mentality with both
delivery of care using a partnership funding and service provision’
44% of survey model focused on systems,
participants referred to WQPHN Online Lived Senior Executive
operations, commitment, joint
a mental health service Experience Survey Results
deliverables and outcomes’
did not attend due to
stigma/fear. Anonymous
WQPHN Online Lived
Experience Survey
Results
28Focus area 1: Building a connected and person-centred care sector
Consultation insights
Having access to services centred around a person’s Breakthrough Opportunities y Potential role telehealth and digital eMental Health
needs that are as close to home as possible is tools play in addressing access issues relating to
essential, for people to be able to remain well and y Continue to build on strong community leadership distance and travel
connected to their family and community. This to harness expertise to drive reform and to co-
y Data sharing for planning, evaluating interventions
includes supporting individuals to take proactive design an integrated care agenda
and performance monitoring
steps, so they are not managing symptoms on
their own. y Strengthen the collective voice of people with a
y Development of place-based health intelligence
lived experience so the service access points and
reports that have identified need and potential
system can be shaped around these needs
Challenges in Western Queensland service improvement strategies for interagency
y Strengthen the WQ HCH model in delivering health planning.
y Not a ‘one size fits all’ approach coordinated and efficient primary care
y Low population density and tyranny of distance to y Facilitating local stepped care reform that engages
services and travel required to reach them local commissioned service providers, general
practice and wider WQ HCH neighbourhood
y Lack of participation and engagement of those
with lived experience y Move towards a shared resourcing model Continuing to build on the
incorporating shared fund pooling, infrastructure WQ HCH model in supporting
y Siloed funding models multidisciplinary team-
and workforce models
y Sustainability of private practice settings in rural based care that connects
y Electronic shared digital referral
and remote Western Queensland individuals with the broader
y Communication and interoperability challenges
y Build on high value care provided by AICCHOs health and social care system
and benefit of the block funding model is fundamental to driving a
across provider networks
y Reform the funding model with a shift to a mixed person-centred approach.
y Knowledge and awareness of visiting services
model of private billing fee-for-service and
y Higher health care costs. population-based block funding based on the
population served and the health needs of
the community
y Support diversity and capability expansions
through cultural leaders, trusted advocates and
mentors as part of the broader team.
29Focus area 1: Building a connected and person-centred care sector
Shared objectives Priority actions Lead agency
Shared objective 1 - Deliver 1. Strengthen leadership development and partnerships to embed comprehensive responses across
person-centred services through the continuum of care.
the WQ HCH and Stepped
Care Framework 2. Implement flexible models of care that support integration of primary and secondary care
incorporating the stepped care framework to better connect consumers to services.
3. Broaden digitally enabled models of care, care pathways, information-sharing protocols and
electronic health records in coordinating care.
Shared objective 2 - Increase 1. Utilise engagement processes outlined in QMHC Stretch2Engage Framework and Lived
engagement and participation Experience Framework that support inclusive engagement and incorporate peer workforce
of people who understand the tailored for the Western Queensland context.
lived experiences of MHSPAOD
in place-based co-designed
planning and governance
Shared objective 3 - Making 1. Develop an evaluation framework that incorporates safety and quality measures to support
safety and quality central to planning, monitoring, evaluation and reporting on progress.
mental health service delivery
2. Adopt place-based, needs-based planning to inform Commissioning Locality funding and
service enhancements.
3. Adoption of refeRHealth electronic referral to support coordination and team care.
Shared objective 4 - Address 1. Develop a WQ stigma reduction strategy/framework that incorporates priorities around
mental health stigma and engagement, training, communication, leadership and advocacy.
discrimination including
embedding principals of human 2. Develop a safe language interagency terminology guide for service providers, consumers, carers
rights protection and people with a lived experience.
30Focus area 2: Proactive prevention and early intervention
‘Under investment in prevention ‘Help people understand the
and early intervention, means that warning signs and to not be afraid
too many people live with poor to seek help in the early stages’
social and emotional wellbeing
WQPHN Online Survey - Lived
for too long’
Experience
WQPHN SW Mental Health
Roundtable, Charleville
‘We need to take a pragmatic
approach and invest in evidence
based interventions that we know Good mental health
will work’ builds resilience,
buffers against
CW Mental Health Roundtable, adversity, reduces the
Longreach
chances of physical
‘Cannot underestimate the critical illness, promotes
role of screening and health checks recovery and increases
in early detection and prevention’ life expectancy.21
Clinician
Early intervention
services were
identified as the
highest priority area for
service development.
Lived Experience and
Clinician/Stakeholder
31Focus area 2: Proactive prevention and early intervention
Consultation insights
Strengthening positive mental health and wellbeing, Breakthrough opportunities
and preventing mental health issues, problematic
relationship with AOD use and suicide risk contributes y Address workforce issues by upskilling
to better health, increased life expectancy, education local providers
and employment outcomes, increased productivity,
community participation, social capital and y Empower people to recognise early signs of
community cohesion. vulnerability, distress, so they access support at an
early stage
These benefits span generations and highlight how we y General practice and primary care providers
can help prevent the incidence, severity and impact provide ongoing surveillance and ready access to
of mental illness, suicide and harm reduction. When proactive preventative care
executed well, preventive actions are more effective,
less expensive and have a greater population impact y Greater advocacy and promotion by primary care
than managing and treating ill-health.19;20 providers of evidence-based early intervention low
intensity programs and services
Challenges in Western Queensland y Identifying risk factors early through universal and
targeted screening Widening ‘poverty gap’
y Poor understanding of low intensity early in rural and remote
intervention primary mental health services y Standardising screening tools to drive
prevention efforts settings highlights the
y Residents present late, are diagnosed late and at a need to strengthen
more advanced stage of illness, with corresponding y Building knowledge of what services are available prevention and early
physical comorbidities. to provide appropriate and timely advice and intervention efforts20
interventions
y Invest in prevention and early intervention, and
build the evidence base for promotion
y Use e-health as an enabler to deliver early
intervention services.
32Focus area 2: Proactive prevention and early intervention
Shared objectives Priority actions Lead agency
Shared objective 1 - Increase 1. Map existing resources to identify gaps or opportunities to support service delivery for agencies/
mental health, AOD and suicide councils who provide MHSPAOD information.
prevention literacy
Shared objective 2 - Increase 1. Expand screening and psychological service delivery through digital health and telehealth,
early intervention response targeted events, GP health checks, workforce capacity, and joint commissioning (and other
funding models).
2. Universal adoption of ‘best of breed’ strength-based eMental health programs including
‘Weathering Well’ and ‘Stay Strong’.
33Focus area 3: Promote and protect mental
health and wellbeing across the lifespan
‘We need to start with our mothers ‘There is a need to develop
and babies so we can improve better links between schools and
the life trajectory of our most agencies to strengthen capacity
vulnerable families’ for early identification of risk’
Anonymous Psychologist, Health
Roundtable
‘Regular health checks in the early
years are key to identifying mental ‘Active engagement of the client
health and developmental issues throughout planning of their care
early’ plan helps support health seeking
behaviour and patient activation’
Healthy Outback Kids
Nearly 1 in 5, 15-24 Coordinator WQPHN, Online Survey
year olds in WQPHN
region were admitted ‘It is critical we work with teenagers ‘Older persons mental health
to hospital for Mental and young people to enhance their services are really limited in most
coping abilities, so they are able areas, or simply do not exist’
and Behavioural
to respond in positive ways to the
Disorders in risks, stresses and adversities of life’
General Practitioner
2019-2020.23
Police Officer
Over one third (36%) ‘We need to give youth and young
of Prep aged children people agency of choice’
15% of people living in in WQPHN region School Counsellor, Mental
WQPHN region in the are developmentally Health Roundtable
active GP population vulnerable in one or
were diagnosed with more domains of the
depression, anxiety, AEDC (QLD 25%).22
bipolar disorder and/or
schizophrenia.3
34Focus area 3: Promote and protect mental health and wellbeing across the lifespan
Consultation insights
Physical, social, emotional, cultural and Breakthrough opportunities
environmental conditions impact people’s mental
health from infancy to old age. y Integrated school-based assessment to connect
young people to care
Supporting families through the early years of a
y Practical support tools for students and families
child’s life provides strong foundations for life-long
physical, mental, social and cultural wellbeing. y Implement the WQ HCH model of care to help
identify risk factors and strengthen referral pathways
Challenges in Western Queensland and care coordination
y Older persons enrolment and health check to ensure
y Suitably skilled local health workforce to support
wellbeing and is part of individual needs, including
the uptake and engagement of health services
access to psychosocial support
by children and their families
y Integrate place-based primary health care approaches
y Coordination between visiting and local health
founded on strong and effective partnerships
and social care services in remote communities Photo courtesy of Gidgee Healing
y Messaging around healthy ageing topics such
y Collaboration between health and education
as dementia
sectors to support prevention and early
intervention y Connectivity between the health sector and schools
to identify at risk children (and young people) and
y Enhanced co-design of services with youth and
demystifying mental health
young people
y Stigma reduction strategy
y Interdependencies of social determinants on
equitable access to services, resources and y A Young Persons Positive Mental Health Strategy that
clinical care engages young people in its design and delivery
y Engagement and support for older peoples y Expanded access to Headspace in the South West
mental health
y Grow local health workforce through increased
y Loneliness and social isolation is an issue participation in education
for older people and for people who are
y Increase access to services such as active transport
geographically isolated.
and telehealth-care.
35Focus area 3: Promote and protect mental health and wellbeing across the lifespan
Shared objectives Priority actions Lead agency
Shared objective 1 - Promote 1. Review existing WQPHN Child and Family Framework and Early Years Plan and existing programs
the best start in life such as Healthy Outback Kids to ensure alignment and improved pathways to care.
2. Promote screening and early intervention to support good perinatal mental health.
Shared objective 2 - Embed 1. Support key agencies to deliver place-based young person’s reference groups’ that links into
proactive planning and support an overarching youth strategy. The group would help to inform workforce capacity building and
for young people support for vulnerable groups.
2. Embed proactive planning and support for children and young people involved in child protection
and/or youth justice system focusing on SEWB and pathways to participation and inclusion.
Shared objective 3 - Strengthen 1. Increase care coordination capacity to increase uptake of better access and more proactive
the WQ HCH model of care to management of people with mental health issues.
support planned and structured
care for the adult population 2. Configure primary mental health services to support stepped care approaches and meet the needs
of the region.
3. Develop a WQ HCH place based neighbourhood strategy to support integrated
person-centred care.
Shared objective 4 - Expand the 1. Improve mental health and quality of life for older people, including early detection and
reach and diversity of MHSPAOD intervention through measures such as risk screening, telehealth and increased training.
prevention services specifically
for older Western Queenslanders 2. Expand and develop psychosocial support to increase social connection and reduce impacts from
(65+ years and 55+ years for social isolation and loneliness.
Aboriginal and Torres Strait
Islander populations)
36Focus area 4: Supporting Aboriginal and Torres Strait
Islander social, emotional and cultural wellbeing
‘Words are powerful, we need to ‘Need to create opportunities
use our stories to carry hope and for non-clinical support to be
possibility.’ recognised as equally important
in care approaches’
Aboriginal Health Worker
WQPHN Roma Mental Health
‘We must consider and harness our Roundtable
unique cultural strengths to deliver
effective solutions for our people’ ‘Creating a culturally competent
and safe workforce with training
Stephanie King, Health Advocate
in trauma-informed care must be
a priority moving forward’
‘Shame for our People still exists
and continues to be a barrier to Mount Isa Mental Health Forum
help seeking behaviour’
SEWB Worker
‘We need to address the 65% of all Mental
interdependence of the Health ED
socioeconomic and cultural factors presentations for
that contribute to risk factors for 15-24 year olds were
poor mental health outcomes for for Indigenous young
Indigenous people’
people.1
WQPHN Clinical Advisory
Council member
37Focus area 4: Supporting Aboriginal and Torres Strait Islander social,
emotional and cultural wellbeing
Consultation insights
Building a Plan that identifies the strengths and Breakthrough opportunities y Recognise and value the role and function of
builds protective factors within Aboriginal and Health Workers and other similar type roles so
Torres Strait Islander populations is a fundamental y Nukal Murra Social and Emotional wellbeing the workforce is well positioned to work at the
driver to preventing the onset and exacerbation Framework to expand capacity of top of its scope of practice. This also includes
of mental health, problematic substance use and AICCHO services creating opportunities for clinical and non-
other issues. Through the Nukal Murra Social and clinical support to be recognised as equally
Emotional Wellbeing (SEWB) Framework14 we have y Culturally safe services and holistic family care important in care approaches.
built the foundations for implementing strengths- emphasises wellness, harmony and balance rather
based primary health care approaches within our than illness treatment and symptom reduction.
Aboriginal and Torres Strait Islander communities y Wrap care around families to reduce risk factors
in Western Queensland. It has been designed in and enhance protective factors for social, cultural
close collaboration with Aboriginal Community and emotional wellbeing. Indigenous people in
Controlled Health Organisations (ACCHOs) and WQPHN have nearly
Alliance partners and draws on the intelligence and y Expand leadership and governance structures to double the number
knowledge of these institutions, but importantly ensure a strong presence of Aboriginal and Torres of mental and
also harnesses the cultural resilience within our Strait Islander peoples. behavioural episodes
Aboriginal and Torres Strait Islander peoples. y Co-design all aspects of regional planning of hospital admitted
and service delivery with people who have care compared to
Challenges in Western Queensland lived experience. non-Indigenous.23
Approximately
y Impacts of intergenerational trauma, institutional y Integrate clinical and culturally informed services 60% of the MH
racism and poor experiences of care which are supported by staff who understand the ED presentations
interconnections of a holistic approach. are for people
y Poverty and economic barriers that impact access
to care such as transport, telecommunications, y Understand the service gaps in psychosocial from Indigenous
affordability and remoteness therapies encompassing digital and strengths backgrounds.1
based social and emotional wellbeing services such
y Low health literacy that impacts capacity of a as the Stay Strong App.
person to understand and apply information to
make effective decisions y Promote Aboriginal and Torres Strait Islander
mental health as a career pathway to build local
y Integrating culturally safe and responsive capacity and to address workforce shortages.
MHSPAOD care into mainstream services.
38Focus area 4: Supporting Aboriginal and Torres Strait Islander social,
emotional and cultural wellbeing
Shared objectives Priority actions Lead agency
Shared objective 1 - Continue 1. Support ‘Stay Strong’ eMental Health Tool and promote routine screening wellbeing support,
to foster Indigenous self- recovery and complementary therapy.
determination and leadership
through the Nukal Murra Alliance 2. Empower self-determination through culturally centred processes of decision making
(incorporating lived experience) that deliver solutions that respond to local context (in alignment
with the Guyaa Dhuwi declaration).
3. Increase profile and role of Indigenous cultural mentors or consultants to ensure they have cultural
authority to guide culturally responsive service delivery.
Shared objective 2 - Improve 1. Promote a culturally competent workforce with training in trauma-informed care and in
culturally safe and responsive identification of risk to deliver services to Aboriginal and Torres Strait lslander people.
MHSPAOD services
2. Adopt healing-informed approaches by service providers in their communication, policies
and practices.
Shared objective 3 - Expand 1. Support and build the Aboriginal and Torres Strait Islander health workforce, including Aboriginal
and integrate new care roles and Torres Strait Islander Health Workers, Health Practitioners and community researchers as
into Aboriginal and Torres Strait important cultural brokers.
Islander Health Workforce
2. Broaden non-clinical care connector and wellbeing roles into multidisciplinary team
care arrangements.
39You can also read