Joint Commissioning Strategy for Dementia in Buckinghamshire 2015 2018 - Buckinghamshire County Council Aylesbury Vale Clinical Commissioning ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Joint Commissioning Strategy
for Dementia
in Buckinghamshire
2015 – 2018
Buckinghamshire County Council
Aylesbury Vale Clinical Commissioning Group
Chiltern Clinical Commissioning Group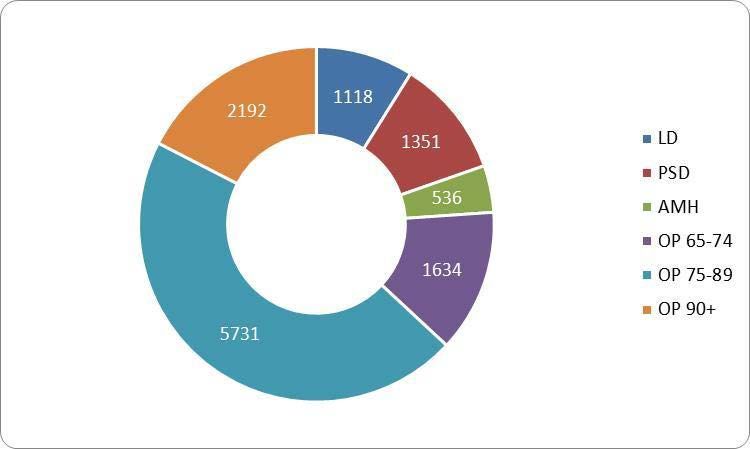
Contents Page
1 Introduction 3
What is a commissioning strategy? 4
Key information 4
2 Vision 6
3 National and local context 7
National drivers 7
Health and social care must ‘deliver’ 7
Parity of esteem 7
Good practice 8
Local drivers 8
4 Needs analysis 9
Expected local needs 9
Future care home demand 10
Clinical Commissioning Groups profiles 11
Chiltern Clinical Commissioning Group 11
Aylesbury Vale Clinical Commissioning Group 12
Number of people in receipt of support from social care 12
Number of people in receipt of support from Oxford Health NHS Foundation Trust 13
5 Supply analysis 14
Commissioned services 14
Care homes 14
Hospital Trusts provision 15
Memory Support Services 15
Dementia-Friendly Communities 16
Prevention Matters 16
Whole system resources 17
6 Gap analysis 19
7 Priorities 20
8 Monitoring and reviewing 22
9 Glossary 23
10 Appendix 1: Key information explained 26
11 Appendix 2: National policy and local arrangement 32
Page 2 of 34
1. Introduction
This commissioning strategy has been developed by Buckinghamshire County Council, Chiltern Clinical
Commissioning Group and Aylesbury Vale Clinical Commissioning Group. An engagement process has
been undertaken to inform its development and this has been achieved through:
• The Dementia Partnership Board
• The Service User and Carer Network
• Four focus group sessions
• Carers Bucks support groups
This strategy responds to the identified priorities within the Buckinghamshire’s Health and Wellbeing
Strategy and is in line with Living Well with Dementia, the national strategy for dementia.
There is a glossary on page 23 to explain what some of the words and terms mean. Words in this
document that are explained in the glossary are underlined.
The term dementia describes a group of symptoms that include loss of memory, mood changes, and
problems with communication and reasoning. Dementia is progressive, which means the symptoms will
gradually get worse over time. There are many different conditions that lead to dementia, the most
common of which are Alzheimer’s disease and vascular dementia.
Many people are now living longer and healthier lives and so Dementia costs the UK
the world population has a greater proportion of older people. economy £23.4 billion a year.
As of 2010, there were an estimated 35.6 million people with
Family carers of people with
dementia worldwide 1. It is estimated that about 800,000 people
are living with dementia in the UK and 6,588 people aged over
dementia save the UK public
65 living with dementia in Buckinghamshire 2. purse over £12 billion a year.
Dementia mainly affects older people over the age of 65, but it can affect people who are younger. In the
UK there are 17,000 younger people (aged under 65) living with dementia 3. There will be over a million
people of all ages with dementia by 2021.
The ‘Dementia 2010’ report 4 revealed that the cost of dementia in the UK is twice that of cancer, three
times as much as heart disease and four times as much as stroke 5. Dementia costs the UK economy £23.4
billion a year. Family carers of people with dementia save the UK public purse over £12 billion a year. By
2040, whilst the number of people affected is expected to double, it is claimed that the costs are likely to
1
http://www.alz.co.uk/research/statistics
2
POPPI (Institute of Public Care – POPPI database)
3
www.alzheimers.org.uk/statistics 2013
4
Luengo-Fernandez et al. 2010
5
http://www.dementia2010.org/reports/dementia2010Full.pdf
Page 3 of 34treble due to inflation in the health care costs and the number of people whose lives are impacted when
someone is diagnosed with dementia 6.
Everyone can reduce their overall risk by adopting a healthy lifestyle which combines a healthy diet with
physical, social and mental activity. Encouraging people to adopt a healthy lifestyle is also important as
delaying the onset of dementia by five years would reduce deaths directly attributable to dementia by
30,000 a year 7
What is a commissioning strategy?
A commissioning strategy is a document which sets out how support and services for individuals will be
developed. In order to decide what outcomes the council and its partners on the Dementia Partnership
Board and Health and Wellbeing Board need to work together to achieve and how the strategy will be
implemented, the following has been taken into account:
• The views of local people including carers
• Relevant legislation and national guidance
• An analysis of the needs of the local population and how these are likely to change in the future.
• An overview of the strengths and limitations of current support and services
• Resources currently available.
People in Buckinghamshire have been engaged to find out what the local issues are. The priorities that have
been identified can be seen on page 18.
This information, together with guidelines published by the Government, has informed the development of
this strategy to ensure that people with dementia living in Buckinghamshire and their carers are able to
have choice and control to live well with dementia and live as independently as possible.
Key national information
• Across the UK an average of only 44 per cent of people living with dementia have a formal
diagnosis 8.
• In the UK 61 per cent of people with dementia are female and 39 per cent are male 9.
• The proportion of people with dementia doubles for every five year age group and one third of
people over 95 have dementia 10.
• There are more than 17,000 younger people (aged under 65) with dementia in the UK 11.
6
Comas-Herrera A, Wittenberg R, Pickard L and Knapp m (2007). ‘Cognitive impairment in older people: future demand for long-
term care services and the associated costs’.
7
‘Forecasting the global burden of Alzheimer’s disease’ Brookemeyer et al. Alzheimer’s and Dementia 2007 Jul;3(3): 186-91
8
www.alzheimers.org.uk/statistics 2013
9
http://www.alzheimersresearchuk.org/dementiaFAQ/
10
www.alzheimers.org.uk/statistics 2013
11
http://www.alzheimers.org.uk/site/scripts/documents_info.php?documentID=164
Page 4 of 34• There are over 11,500 people with dementia from black and minority ethnic groups in the UK 12.
• It is estimated that in 2011 in England there were 1,191,000 people with a learning disability which
is 2.2 per cent of the population 13.
• One in three people with Down’s syndrome develop dementia in their 50’s 14.
• At any one time, a quarter of people staying in hospital beds are people with dementia aged over
65 15.
• Two thirds of people with a diagnosis of dementia live in the community while one third live in a
care home 16. 80 per cent of people living in care homes have a form of dementia or severe
memory problems 17.
• There are 670,000 carers of people with dementia in the UK 18. These unpaid carers save the UK
economy £12 billion every year 19.
• The expense to the UK economy of each person with dementia is £27,647 per year; more than the
UK median salary (£24,700). By contrast, people with cancer cost £5,999, stroke £34,770 and heart
disease £3,455 per year 20.
• Most of the cost of providing support for people with dementia in the UK (£12.4 billion per year) is
met by unpaid carers21.
• Government and charitable spending on dementia research is 12 times lower than on cancer
research. £590 million is spent on cancer research each year, with just £50 million being invested in
dementia research 22.
12
www.alzheimers.org.uk/statistics 2013
13
http://www.arcuk.org.uk/membersarea/wp-content/uploads/2012/05/IHAL-PWLD-England-2011.pdf
14
http://www.alzheimers.org.uk/site/scripts/documents_info.php?documentID=103 2013
15
Counting the Cost. Alzheimer’s Society. 2009.
16
www.alzheimers.org.uk/statistics 2013
17
www.alzheimers.org.uk/statistics 2013
18
www.alzheimers.org.uk/statistics 2013
19
www.alzheimers.org.uk/statistics 2013
20
‘Dementia 2010’ Alzheimer’s Research Trust
21
www.alzheimers.org.uk/statistics 2013
22
http://www.alzheimersresearchuk.org/dementia-statistics/
Page 5 of 342. Vision
Our vision for Buckinghamshire is that
“people will be supported to live active lives in caring
communities enabling people to live fulfilling lives
independently at home for as long as possible. When
care is required people will only have to tell their story
once. Information will be provided to enable people to
make the right choices regarding services for them”
Page 6 of 343. National and local context
National Drivers
The national drivers considered as part of the development of this strategy can broadly be seen as follows:
The National Dementia Strategy [2009]
• The National Carers Strategy [2010]
• Delivering on Dementia [2012 -2017] The Alzheimer’s Society
• Prime Ministers Challenge [2012]
• The Health and Social Care Act [2012]
• The Care Bill [2013]
• Personal Health Budgets
• NHS Outcomes Framework [2014 /15]
• NHS Five Year Forward View [2014]
Health and social care must deliver
When considering the above national policies some of the clearly defined requirements for health and
social care can broadly be seen as:
• Dementia services – raising awareness, encouraging earlier diagnosis and improving living conditions
for those with dementia.
• Preventative services – prevention and early intervention promoting healthy life style choices to
reduce the risk factors associated with dementia.
• Managing the market – stimulating and developing the market to ensure the right services are
available to meet local needs.
• Accountability – establishing local Health Watch and Health and Wellbeing boards.
• Partnership working – ensuring statutory partners, third sector organisations and local communities
work together
• Integration – health and social care will work together to deliver integrated services
• Parity of esteem – work together to ensure equal status is achieved for Mental Health and Physical
Health
• Quality assurance – clear arrangements in place to monitor services and to manage poor quality.
Parity of esteem 23
Mental health’s time has come. No longer is it good enough for mental health to be the poor relative of
physical health. No longer is it acceptable for there to be no parity of esteem. It is time to stop the
short term approach of simply treating the problem when it presents, and become more proactive
about prevention and early intervention. That means working with schools, colleges and universities,
23
NHS England (2014) www.england.nhs.uk/ourwork Parity of Esteem
Page 7 of 34employers, transport, police, health and social care, local authorities and community organisations to
raise the profile and priority of good mental health and early action if there are signs of difficulties in
any individual. It is time to stop accepting second best in mental health services and work with those
who have lived through the experience to design better services together.
It is time to shift care into the communities where people live by increasing
primary care mental health services and supporting specialist care - absolutely
essential for many who have episodic crises or enduring severe mental illness - in
moving to community environments with close links to primary care. We all need
specialists to be freer to respond when there is need. It is time to act and do what
the evidence shows.
Mental health and wellbeing are central to the work of GPs, and high quality primary care is critically
important for the health of local communities. Indeed we are, in many ways, at a moment of real
possibility in relation to mental health. Increasingly, a body of ideas is being shared that together
represent a coherent direction of travel. Care and support moving further out of hospital towards
home; moving from prescription to partnership in working with empowered citizens and people; seeing
the development of resilience and health promoting communities as key ingredients for real population
health; working towards holistic approaches that bridge the mind-body divide that we have artificially
created.
Good practice
The following good practice service models and research has informed the development of this strategy:
• Tamar Memory Assessment Service
• The Dementia Centre – Change – Pathways and Practices [07]
• NICE quality standards for dementia
• NICE support people to live well with dementia
• NICE the dementia pathway
• Service re-development: Integrated whole systems services for people with dementia. [The
dementia Partnership]
• Dementia and Neurological Conditions South West:” Pathways to Dementia Diagnosis:
Local drivers
The local drivers considered as part of the development of this strategy can broadly be seen as:
• The Joint Adult Mental Health Commissioning Strategy [2015-18]
• NHS Buckinghamshire Commissioners 5 Year Plan [2014-19]
• The Public Health strategy [2013]
• Buckinghamshire’s Joint Strategic Needs Assessment [2013]
• Buckinghamshire’s Multi-Agency safeguarding Vulnerable Adults Procedure
• Buckinghamshire’s Joint Health and Wellbeing Strategy [2013 -16]
• The District Councils Sustainable Communities Strategies
Page 8 of 344. Needs analysis
A needs analysis is a way of estimating what the needs of the population are so that appropriate support
can be planned. In this strategy Buckinghamshire County Council and Clinical Commissioning Groups have
identified the expected local need through the Joint Strategic Needs Assessment, Census and other data
sources. Local people and organisations were also asked for their feedback on needs and priorities for
people affected by dementia.
Table: People aged 65+ living in Buckinghamshire estimated to have dementia.
Year 2014 2015 2020
Number of people with dementia 6,588 6,826 8,123
Source: POPPI Database 24
Expected local needs
At the last census, 2011, the estimated population for Buckinghamshire was 505,283 Between 2001 and
2011 the population grew 5.5 per cent, less than the national growth rate (7.1 per cent) and the South East
growth rate (7.6 per cent).
Understanding growth rate is important because the most significant risk factor for developing dementia is
age. In Buckinghamshire, the largest population increase is predicted to be amongst those aged over 85+ an
84% increase between 2011 and 2025.
When the age profile and percentage of the population at 2011 and 2030 (using ‘planning4care’
projections) is applied to existing Buckinghamshire County Council adult social care service users we see
the following changes:
Table 1: Adult social care service users in 2012 by client group and older people age profile
Source: Swift AFW Client Recording System 2012 25
24
POPPI (Institute of Public Care – POPPI database) Crown copyright 2010
25
Buckinghamshire JSNA
Page 9 of 34Table 2: Adult social care service users projected in 2030 by client group and older people age profile
Source: Poppi 2012 and Swift AFW Client Recording System 26 (JSNA data)
Table 1 and Table 2, shows the total requirement for the provision of residential care, home care and day
care (assuming current service patterns) for all people in Buckinghamshire with social care needs at
moderate level and above who are in need of formal care (based on the typical levels of care for different
needs groups currently provided by the local authority at the time of data extraction in 2012 to inform the
JSNA). N.B. from 1 April 2015 the Care Act comes into effect and the definition for eligible needs will be
set nationally.
Table 3: Projected total population service requirements based on patterns of provision in
Buckinghamshire in 2012
Service 2011 2016 2031
Home care (hours per week) 47,500 55,000 82,200
Day Care (placements) 1,300 1,500 2,300
Residential Care 2,800 3,200 4,800
Source: Planning4care (2012) (JSNA data)
In line with the demographic projections, collectively these represent a projected increase of 73 per cent
more than the national projection of 54 per cent and the South East projection of 63 per cent between
2011 and 2031. 27
Life expectancy in Buckinghamshire is higher than the national average at 80.5 years for men and 84 years
for women. This is compared to 78.3 years for men and 82.3 years for women nationally.
Future care home demand
Access to nursing care is an issue within the county and especially in Chiltern and South Bucks. Including
known initiatives in the early stages of proposals, it is predicted that by 2033 an additional 2,000 beds will
be required across the county.
26
Buckinghamshire JSNA
27
Buckinghamshire JSNA
Page 10 of 34Table 4: The number of increased / decreased beds available in each geographical area by bed type by
2033
Residential Care Nursing Care
Aylesbury Vale DC 306 399
Chiltern DC -183 420
South Bucks DC -88 161
High Wycombe DC 249 686
Source: Buckinghamshire County Council’s ‘Specialist Housing for Vulnerable Adults’ Market Position
Statement March 2015
Although it is not possible to identify the exact number of specialist beds required, due to the projected
increases in the 65+ population it is reasonable to assume a large proportion of the beds indicated in Table
4 will need to be register for dementia.
It is also important to note that by 2033 Chiltern and South Bucks will have an oversupply of residential
beds. It will be important to work with providers to ensure continued stability in the market while
responding to market changes.
Clinical commissioning groups - profiles
Buckinghamshire is the eighth least deprived county in England and has some of the best health outcomes
as reported by Public Health Outcomes Framework published by Public Health England. As a result
Buckinghamshire has relatively low health care funding. Although a fifth of the population living in our most
deprived areas often have worse health outcomes than the national average.
We know that certain life style choices can increase the risk of dementia. Based on the Integrated
Household Survey, approximately 14% of adults are estimated to smoke in Buckinghamshire compared to
19.5 per cent in England [2012] Based on Active People’s Survey [2013] 24 per cent of adults in
Buckinghamshire are ‘inactive’ compared with 29 per cent in England.
Chiltern Clinical Commissioning Group
Chiltern CCG area has a total of 34 practices distributed across 4 localities. One GP practice was
successful in 2014 in a bid to NHS England to secure funds to become Dementia Friendly. It’s reasonable
to suggest that all practices need to work towards becoming Dementia Friendly
Chilterns profile can broadly be seen as:
• 18 per cent of the population are aged 65+
• 15.9 per cent of the population are from black and ethnic minority groups
• 10.7 per cent is the average deprivation score
• Diabetes detected prevalence rate is 4.4 per cent [Public Health England estimated prevalence is 7.3
per cent a possible gap of 5,000 people]
• 2.8 per cent of the population have coronary heart disease
• 1.3 per cent of the population have had a stroke
• 4.7 per cent of the population live with depression
Page 11 of 34Patient satisfaction with GP practices in Chiltern range from 73 per cent to 98 per cent. Please see
Appendix 1 for further details.
As of April 2015, the dementia prevalence calculator shows Chiltern Clinical Commissioning Group
diagnostic rate as 50.2 per cent NHS England dementia prevalence calculator indicates that roughly 2,400
people remain undiagnosed and the gap between the national targets of 67 per cent is approximately 1,000
Aylesbury Vale Clinical Commissioning Group
Aylesbury Vale CCG area has a total of 19 practices distributed across three localities. One GP practice
was successful in 2014 in a bid to NHS England to secure funds to become Dementia Friendly. It is
reasonable to suggest that all practices need to work towards becoming Dementia Friendly.
Aylesbury Vales profile can broadly be seen as:
• 17 per cent of the population are aged 65+
• 9.8 per cent of the population are from black and ethnic minority groups
• 9.8 per cent is the average deprivation score.
• Diabetes detected prevalence rate is 4.5 per cent [Public Health England estimated prevalence is 6.6
per cent a possible gap of 1,400 people]
• 3.1 per cent of the population have coronary heart disease
• 1.51 per cent of the population have had a stroke
• 5.37 per cent of the population live with depression
People’s satisfaction with GP practices in Aylesbury Vale range from 64% to 94%. Please see Appendix 1
for further details.
Aylesbury Vale Clinical Commissioning Group diagnostic rate is 58.02 per cent. The NHS England
dementia prevalence calculator roughly indicates 1,653 people remain undiagnosed and the gap between
the national target rates of 67 per cent is approximately 263.
Number of people in receipt of support from social care
In January 2015 a snap shot of clients and carers were recorded as being in receipt of care and support
with the category of dementia has been used to inform the development of this strategy. This can broadly
be seen as follows:
• 50 older people aged 65+ were being supported by the community mental health team for older
people (CMHT (OA)): 33 [66 per cent] were female and 17 [34 per cent] were male. 28
• Of the 50 older people aged 65+ being supported by CMHT (OA), 13 (26 per cent) have an unpaid
carer. 29
• Approximately two people are being supported by the community team for people with learning
disabilities (CTPLD) who have dementia 30
28
RIO Stats
29
RIO Stats
30
Buckinghamshire LD Dementia Register
Page 12 of 34• 7,405 people aged between 18 and 64 in Buckinghamshire were predicted to have a learning
disability 31 and a further 1,995 will be 65+. By 2020, there are predicated to be four people 65+
with downs syndrome living in Buckinghamshire. This is important because they present differently.
In addition, people with dementia as a secondary support need receive support through the Older People
and Complex Care Teams. This can broadly be seen as follows:
• 327 people were being supported by Adult Care Management Teams, of which 68 people had a
carer.
• 24 people were being supported through the re-ablement service of which seven had a carer.
Number of people in receipt of support from Oxford Health NHS Foundation Trust
The data below has been provided by Oxford Health as a snap shot in April 2015 of the number of people
currently accessing their services by level of need.
P18 - Cognitive Impairment (Low Need) (12 months) 215
P19 - Cognitive Impairment or Dementia (6 months)Complicated (Moderate Need) 372
P20 - Cognitive Impairment or Dementia (High Need) (6 months) 209
P21 - Cognitive Impairment or Dementia (High Physical or Engagement) (6 months) 121
Source: IM report MH – MC Diagnosis SSRS
This data demonstrates that 215 are being supported by the Older Adult Mental Health Teams [OAMHT]
with mild cognitive impairment /dementia, and the OAMHT is supporting /treating a further 702 people
with more complex dementia presentations.
Below is a count of the number of people who were referred and seen in Memory Clinics in 2014/15:
2014-04 2014-05 2014-06 2014-07 2014-08 2014-09 2014-10 2014-11 2014-12 2015-01 2015-02 2015-03 Grand Total
8 35 61 76 52 56 58 63 47 66 64 72 658
Source: IM report MH – MC Diagnosis SSRS
It is during these appointments that the assessment would be undertaken.
615 diagnoses are recorded on clinical information systems for people referred and seen in 2014/15 within
Memory Clinics.
413 diagnosis of dementia:
• 222 are coded to Dementia in Alzheimer's disease with late onset
• 191 are coded across a range of dementia diagnosis
Additionally the following diagnoses were made:
• 175 to mild cognitive disorder
• 27 received a diagnosis of a functional mental illness
31
Institute of Public Care (Poppi database) Dec 2014
Page 13 of 345. Supply analysis
Commissioned Services
Buckinghamshire has a variety of externally commissioned services which are provided county-wide:
• Advocacy, IMCA & IMHA Support Service – provided by third sector organisation
• Information and advice – provided by third sector organisations
• Direct Payment Support Service including personal assistants - provided by a third sector
organisation
• Brokerage service – external providers
• Carers support service – provided by third sector
• The community equipment service – provided by external provider
• Telecare equipment and monitoring – provided by external providers
• Sensory service – provided by third sector
• Memory support service and primary support service – provided by third sector organisations
• Community hot meals – provided by external provider
• Domiciliary care support – provided by external organisations
• Floating support – provided by external provider
• Day opportunities – provided by external organisations
• Respite Services – provided by external providers
• Home from hospital service – provided by the third sector
• Befriending service – provided by third sector organisations
• Extra care housing – provided by third sector organisations
• Residential and nursing sare – provided by external providers
All services are contract-managed through a contract framework. Services-users and carers report
reasonable levels of satisfaction.
All providers have signed up to There is evidence to suggest that the demand for some services
Buckinghamshire’s multi-agency is greater than availability e.g. residential and nursing care.
Service-user and carer feedback from the consultation indicates
policy and procedures for
gaps in cost-effective day care provision particularly for those
safeguarding vulnerable adults. diagnosed at an early age.
Care homes
Normally residential care facilities can meet the needs of people with dementia. Buckinghamshire County
Councils ‘Specialist Housing for Vulnerable Adults’ Market Position Statement March 2015, has been used
to inform the development of this section.
In Buckinghamshire, registered with the Care Quality Commission (CQC), are the following types of care
home provision capable of meeting the needs of people with dementia:
Page 14 of 34• 15 nursing homes
• 19 nursing homes registered for dementia
• 20 residential care homes
• 25 residential care homes registered for dementia
• 1 dual registered homes [residential and nursing]
• 1 dual registered home [residential and nursing] also registered for dementia
Hospital Trusts provision
The Buckinghamshire Clinical Commissioning Groups commission services from:
Buckinghamshire Healthcare Trust, who provide services from:
• High Wycombe Hospital
• Stoke Mandeville Hospital and Wexham Park Hospital
• Four community hospitals
Oxford Health NHS Foundation Trust, who provide mental health services from:
• The Whiteleaf Centre: community and inpatient services
• The Valley Centre: community services
• Amersham Hospital: community services
The above three facilities also provide memory clinics. During 2014 a total of four community-based
memory clinics across five GP practices were also established:
• Haddenham
• Denham
• Buckingham
• Stokenchurch
Feedback through questionnaires, completed by people and carers accessing the memory clinics, indicated
the number one priority was timely access to local services. This is also reflected as a priority in the ‘NHS
Five Year Forward View’ and commissioning mental health services in 2015 and beyond. 32
Memory support services
A memory Support Service is currently available county-wide except in Aylesbury Vale North locality were
a pilot primary care support service is accessed.
The primary care support service undertakes a screening process [CamCog software] with people. The
software operates a traffic light system ensuring people are appropriately referred to the memory clinics.
Patients report high levels of satisfaction with the process. Who undertakes an initial assessment and
32
The Five Year Forward View and Commissioning Mental Health Services in 2015 and Beyond [NHS England 2015]
Page 15 of 34assessments tools used, across the rest of Buckinghamshire is mixed as there is currently no agreed
defined process in place.
“NHS South of England, Pathways to Dementia Diagnosis: Reviews of services in the south-west” Nov 13
report concluded from their study “Fewer than 40% of people in the pathway audit were given a diagnosis
of dementia. Most areas use the 6CIT assessment found in GP’s IT systems and this is completed by people
with GP’s, receptionists, practice and community based nurses etc. ensuring appropriate use of resources.
Consideration needs to be given within Buckinghamshire to ensure best use of resources and to improve
patient experience.
Dementia-Friendly Communities
Dementia-friendly communities are a newly introduced By supporting communities to
initiative within Buckinghamshire. This was launched in January become more dementia-friendly
2015 with the first “Dementia Action Alliance” established in this will in turn enable people
Stokenchurch.
living with dementia to remain
The establishment of dementia-friendly communities is pivotal living well and active within their
to the success of de-stigmatising dementia. communities for longer.
Prevention Matters
Prevention Matters is a service that works with people on the cusp of eligibility for social care and with
those beginning to experience long term health and social difficulties.
Community Practice Workers (CPWs) work one-to-one with clients and link them to appropriate
community support services. Service users are regularly supported to access befriending & social groups,
activities and services to reduce the risk of social isolation.
Community Link Officers (CLOs) work with communities and organisations to increase the range of
services available to vulnerable people and enhance their quality and capacity. Dementia-friendly services
have been of particular focus and CLOs have worked to establish:
• Singing for the Brain groups
• Befriending services
• Carers dementia services
• Movers & Shakers groups
• Men in Shed groups
Prevention Matters also provide grants which have been awarded to a range of support services for people
with dementia. Other key services within Prevention Matters are the ‘Volunteer Hub’ and the ‘Time
Credits’.
Page 16 of 34Whole system resources
The chart found on page 18 shows the resources, services and tools currently available within
Buckinghamshire to support the following areas:
• Prevention
• Early diagnosis and support
• Living well in community’s
• Living well in hospital
• Living well in care homes
• End of life care
Page 17 of 34Prevention Early diagnosis & support Living Well - Living Well - Living Well – Care EoL
community hospital Home
CQC
Prevention Matters Practice Workers Discharge coordinator
Quality in care homes Older people's services
team – up skilling care bucks cc
Memory Advice Service (Age UK) workers
Nightingale service
Age UK, -information/advice & Dementia Link worker
Befriending Service Medicines optimisation
(H)
in care homes project: Advanced care planning
Dementia Primary Care Workers (Alzheimer's Society)
In house training 1 pharmacist
Alzheimer's Society Alzheimer's Society Community nurses
PIRLS – A&E psych in Falls pilot for care
-Talks, publicity, Memory - Dementia Cafes
reach workers, users, and
- Community Befriending families
Intergenerational Hospital Befriending
Schools teaching - Singing for the Brain
resource This is me My home life 30 older
General Practice; GP, Nurse, DN, dispending pharmacist people care home
'Home Instead' - NHS Health Checks MAGs Group communication
passport managers
Dementia training Carers Bucks
Dignity in care Smile for life
Carer's Bucks – CPN – community mental health champions
Training for Carers - Memory Clinics Oral health for older
Oxford Health older
CAB – Citizen's Advice Fire Safety Officer
adult in patient unit
Websites Healthwatch
Psychological Therapies Pathway
Service Users CBT for Carers CPN – Community
mental health
Dementia Action Alliance
Older People's Services (BCC)
Community Engagement Officer Dietician
A&E and Acute Hospital Assistive technology
Dementia Community Link Nurse (locality/BHT)
Community team –
Physio, OT, SLT
Memory Friendly Communities Project
Talking Point Housing Association/Trust
Radiology – MRI/CT scans
In Touch (carers) Police, ambulance, fire
SC clients/phone call
John Hampden Relatives
Support Group
Safeguarding Adults
Integrated Board
QiCHT upskilling Dom
Care Workers6. Gap analysis
Through data analysis, consultation with service-users, carers and professionals key themes have emerged.
These themes indicate a gap in service provision or the need for improvements to be made as follows:
• An improved and consistent approach to people’ experience within GP services regarding
diagnosis, information and sign posting.
• More meaningful, cost effective and local day opportunities for people with dementia, particularly
for those diagnosed at a young age.
• Improved and innovative ways of providing advice and information at key points in the pathway.
• Easy access to high quality, appropriate and effective training for health and social care
professionals, service-users, carers and business.
• De-stigmatising dementia by raising awareness in local communities.
• Improved dementia diagnostic rates.
• Improved access to generic community based facilities for people living with dementia and there
carers.
• Improved end of life planning.
People are living longer and Buckinghamshire has an ageing population. As we know age is a factor with
dementia and it is fair to say that we are going to see a steady increase in the demand for services for
people living with dementia and their carers over the coming years. We are aware of gaps in services and
our aim is to address these through future commissioning intentions.7. Priorities
The following priorities have been informed by people with dementia and their carers and the Department
of Health outcomes frameworks. Commissioners will take these into account when designing support and
services.
• Better dementia awareness
• Prevention and living well awareness
• Integrated services
• Information and advice
• Carers Support
• Personalised support and independent living
• Dementia-Friendly Communities
• Early diagnosis and intervention
• Care Homes
• Dementia-Friendly GP practices
• Specialist services – including crisis support
• Young people with dementia
The above priorities have been encapsulated into five strategic themes as follows:
• Improved diagnostic pathway and rate
• Dementia Awareness
• Personalised support and independent living
• Pre-crisis support
• Young people with dementia
The action plan below sets out the activity and timescales that will be undertaken to address the priorities
and strategic themes:
Page 20 of 34Strategic Themes Actions Lead responsibility Time Frame
1.1 Evaluate the MACH project Joint Commissioning Manager – Dementia 1.1 August 15
1.2 Develop agreed standards to ensure patient and carers Lead 1.2 Dec 15
1. Improved experience is the same throughout the pathway [Leads within partner organisations to be 1.3 March 16
diagnostic pathway 1.3 Increase the number of GP practices who are working identified for each work stream] 1.4 April 16
and rate towards becoming dementia friendly
1.4 Improve CCG’s diagnostic rates:
Chiltern – 52% by April 15 and 60% by Sep 15
Aylesbury Vale – 59% by April 15 and 67% by Sep 15
2.1 Develop a training program and resources for health, Joint Commissioning Manager – Dementia 2.1 Dec 15
social care, people with dementia, carers and businesses Lead 2.2 June 15
2. Dementia 2.2 Develop a communication strategy and materials [Leads within partner organisations to be 2.3 June 16
awareness 2.3 Implement dementia friendly communities identified for each work stream] 2.4 Review
2.4 All services to work towards becoming dementia friendly annually
2.5 Improved awareness with children and young people 2.5 April 16
3.1 Access to improved information in an appropriate and Joint Commissioning Manager – Dementia 3.1 April 16
timely manor Lead 3.2 Dec 15
3. Personalised 3.2 Agree a universal communication passport [Leads within partner organisations to be 3.3 April 17
support and 3.3 Facilitate market development to meet needs I.e. Housing, identified for each work stream] 3.4 April 16
independent living day opportunities etc.
3.4 Develop enhanced community based support services
4.1 Agree the pathway for people living with dementia who Joint Commissioning Manager – Dementia 4.1 April 16
are rapidly deteriorating Lead 4.2 June 16
4. Pre-crisis support 4.2 Ensure the pathway is effectively communicated [Leads within partner organisations to be
identified for each work stream]
5.1 Improve early diagnosis Joint Commissioning Manager – Dementia 5.1 June 16
5. Young people with 5.2 Enable people to continue to live well and independently Lead 5.2 June 16
dementia with communities [Leads within partner organisations to be
identified for each work stream]8. Monitoring and reviewing Commissioned services within the county are monitored in a number of different ways as follows: • The Care Quality Commission • Buckinghamshire County Council contract framework • The Commissioning Support Unit – outcomes indicator set. • Formal contract arrangements between the CCG’s and Oxford Health The implementation of this strategy will be monitored through appropriate governance arrangements which will include the Buckinghamshire Dementia Partnership Board and the Adult Joint Executive Team.
9. Glossary
Adjusted Clinical Groups The ACG System measures the morbidity burden of people
(ACG) populations based on disease patterns, age and gender. It
relies on information about diagnoses found in insurance
claims or other computerised medical records. This
provides clinical commissioning groups with a more accurate
representation of the morbidity burden of populations,
subgroups or individual people – as a constellation of
morbidities, not as individual diseases.
Alzheimer’s disease Alzheimer’s disease is the most common form of dementia.
Alzheimer’s disease was first described by a German
neurologist Dr Alois Alzheimer. Alzheimer’s disease is a
physical disease of the brain. During the course of the
disease plaques and tangles develop in the brain leading to
the death of brain cells. People with Alzheimer’s disease
have a shortage of some important chemicals which are
involved in transmitting messages within the brain.
Clinical Commissioning A Clinical Commissioning Group is a group of GP Practices
Group or CCG that are working in partnership to arrange health services
for local people.
The Clinical Commissioning Groups in Buckinghamshire are
called:
Aylesbury Vale Clinical Commissioning Group – supporting
the north of the county.
Chiltern Clinical Commissioning Group – supporting the
south of the county.
Clinician A person who works in the health service whose job it is to
give help and support to people, e.g. doctor, nurse, optician,
pharmacist.
Commission To authorise or have a contract with a person or
organisation to make something specific happen. This might
be to provide a particular service such as nursing care.
Commissioning Often commissioners pay the providers to run a particular
service.
Commissioners The people or organisations that commission other people
or organisations to do things. The joint commissioners
commission social care services on behalf of the local
authority and health services on behalf of the CCG’s.
Commissioning Please see commissioners
organisations
Commissioning Plan The plan that says exactly what commissioning organisations
are going to pay or authorise other people or organisations
to run. They should be quite detailed about the standards
that are expected and the times by which they want things
done.
Commissioning strategy Strategies are more ‘high level’ than plans, and say the kinds
Page 23 of 34of things that are going to be done to meet the needs and
wishes that have been identified. Commissioning plans
should be based on commissioning strategies.
Community Mental Community-based team of specialist healthcare and social
Health Team for Older care practitioners, supporting older people with mental
Adults (CMHT-OA) health conditions and people with dementia.
Department of Health The Department of Health is a part of Government that is
responsible for policy and some funding for health and social
care services, and for improving the country’s health and
wellbeing.
Dementia The term “dementia” describes a set of symptoms
associated with an ongoing decline of the brain and its
abilities. This includes problems with:
• Memory loss
• Thinking speed
• Mental agility
• Language
• Understanding
• Judgement
How fast dementia progresses will depend on the individual
person and what type of dementia they have. Each person is
unique and will experience dementia in their own way.
Down’s syndrome Down’s syndrome is a condition that people are born with.
People with down’s syndrome are likely to have:
• A learning disability
• Reduced muscle tone leading to floppiness
(hypotonia)
• Eyes that slant upwards and outwards
• Their palm may have one crease across it (palmar
crease)
• A below average weight and length at birth
GP General Practitioner: most people are registered with a GP.
Groups of GPs or those who work in the same surgery are
often referred to as a GP Practice.
Health and Wellbeing The Health and Wellbeing Board is a partnerships between
Board the local authority, the clinical commissioning groups and the
local Health Watch organisation for the area. Working in
partnership and under a specific duty to promote the health
of their population, in everything they do, Boards must seek
to:
• Improve health outcomes for local people
• Reduce health inequalities between different people
in the community.
Joint Health and A plan that sets out the priorities that commissioning
Wellbeing strategy or organisations need to think about when developing health
JHWS and social care services.
Joint Strategic Needs An assessment of the health needs of the local population,
Assessment or JSNA which then identifies where there are particular problems
that need attention.
Page 24 of 34Learning Disability A learning disability happens when a person’s brain
development is affected, either before they are born, during
their birth or in early childhood. A learning disability means
a person finds it harder to learn new things in any area of
life, not just at school, and everyday activities can be difficult.
Local Authority Refers to the county council, borough council, district
council, etc. For this strategy the council is
Buckinghamshire County Council.
Mild Cognitive Mild cognitive impairment causes cognitive changes that are
Impairment or MCI serious enough to be noticed by the individuals experiencing
them or to other people, but the changes are not severe
enough to interfere with daily life.
NHS National Health Service
Outcomes Something that happens as a result of action: it is important
to focus on the outcomes for people rather than the actions
which may not have the outcomes people want.
The Outcomes The Outcomes Framework, created by the Department of
Framework Health, sets out the areas (domains) that the council needs
to concentrate on within the action plan associated with
every strategy. The Outcomes Framework that relates to
adult social care also links into the Outcomes Framework
for both NHS and Public Health services. For details on how
these link together please see Appendix 1. Each of these
areas in turn has more detailed requirements. The detailed
requirements of the ‘Adult Social Care Outcomes
Framework’ (ASCOF) are listed below.
Partnership An arrangement when organisations or people work
together on things that they all have some responsibility for.
Primary Care Trusts or Large health organisations that were replaced by local
PCTs CCG’s
Priorities The most important or urgent things to work on. Things
might be a priority because of the number of people
affected, or because of what might happen if nothing is done.
Public Health The prevention and management of diseases, injuries etc.
through the promotion of healthy behaviours and
environments.
RiO Patient Record System used by Oxford Health Foundation
Trust (OHFT)
Social Care Support for people in relation to personal care, social
support and prevention of harm for people who are unable
to be independent in those areas.
Statutory Something that must happen because it is set out in law.
Vascular dementia A person can get vascular dementia when their brain does
not get the blood it needs to work properly. Over time,
parts of the brain get damaged and eventually die from a lack
of oxygen and nutrients.
Page 25 of 3410. Appendix 1
Key information explained
Diagnosis Gap
Across the UK an average of only 44 per cent of people living with dementia have a formal diagnosis 33.
Receiving a formal diagnosis of dementia can be upsetting. Diagnosis is vital because whilst there is
currently no cure, there is treatment available to improve symptoms. Getting an early diagnosis of
dementia enables people to:
• Gain access to information, resources and support
• Demystify and de-stigmatise the condition
• Maximise the quality of their lives
• Benefit from treatments
• Plan for the future
• Explain to family, friends and colleagues what has changed in their life and what their wishes for the
future are.
Getting an accurate diagnosis of dementia can take a very long time for younger people; often due to lack
of awareness that dementia can happen to younger people. Medical professionals often misdiagnose
younger people as being depressed, experiencing relationship difficulties, suffering from the effects of stress
or, for women it may be put down to the onset of the menopause.
Learning Disabilities
Down’s syndrome is the most common known cause of learning disability and people with Down’s
syndrome are at particular risk of developing dementia.
Dementia generally affects people with learning disabilities in similar ways to people without a learning
disability, but there are some important differences. People with a learning disability who develop dementia
may show different early symptoms, for example, changes in behaviour or personality are more often
reported as an early symptom of Alzheimer’s than memory loss.
In addition epilepsy that appears in someone with Down’s Syndrome later in life is almost always a sign of
dementia. People with Down’s Syndrome are therefore less likely to receive a correct or early diagnosis as
behaviour and difficulties are often attributed to the learning disability.
Also, some people with a learning disability may experience a more rapid deterioration in memory and
cognitive function. 1 in 3 people with Down’s syndrome develop dementia in their 50s 34. however, people
33
www.alzheimers.org.uk/statistics 2013
34
http://www.alzheimers.org.uk/site/scripts/documents_info.php?documentID=103 2013
Page 26 of 34with a learning disability are more likely to already live with some support which can be adapted and may
have developed alternative/additional ways of communicating which may be helpful when dementia
progresses.
There is no definitive record of the number of people with learning disabilities in England. However, it is
estimated that in 2011 in England, there were 1,191,000 people with a learning disability which is 2.2 per
cent of the population 35. Down’s syndrome is one of the most common genetic causes of learning
disability; 15-20 per cent of people with a learning disability have down’s syndrome 36.
Gender
In the UK, 61 per cent of people with dementia are female and 39 per cent are male. This is mostly
because women tend to live longer than men and dementia becomes more common as people get older 37
Age
Age is the most significant risk factor for developing dementia. The prevalence rates for dementia in the
UK are:
40-64 years: 1 in 1400
65-69 years: 1 in 100
70-79 years: 1 in 25
80+ years: 1 in 6
90+ years: 1 in 3 38
There are more than 17,000 younger people (aged under 65) with dementia in the UK. However, this
number is likely to be an under-estimate, and the true figure may be up to three times higher. Data on the
numbers of people with young-onset dementia are based on referrals to services, but not all those with
young-onset dementia seek help in the early stages of the disease 39.
Hospital
At any one time, a quarter of people staying in hospital beds are people with dementia aged over 65+
Minority Ethnic Communities
There are over 11,500 people diagnosed with dementia from black minority ethnic groups in the UK 40.
This is 1.4 per cent of the total number of people estimated to have dementia. Lower levels of awareness
about dementia and the existence of stigma within BME communities help explain with BME people are
currently under-represented in dementia diagnosis figures.
35
http://www.arcuk.org.uk/membersarea/wp-content/uploads/2012/05/IHAL-PWLD-England-2011.pdf
36
Pulsifier,M.B.(1996). The neuropsychology of mental retardation. Journal of the International Neuropsychological Society, 2,
159-176
37
http://www.alzheimersresearchuk.org/dementiaFAQ
38
www.alzheimers.org.uk/statistics 2013
39
http://www.alzheimers.org.uk/site/scripts/documents_info.php?documentID=164
40
Counting the Cost. Alzheimer’s Society. 2009.
Page 27 of 34Care Homes
Two thirds of people with a diagnosis of dementia live in the community while one third live in a care
home 41. 80 per cent of people living in care homes have a form of dementia or severe memory
problems 42.
Local Health Profiles
Health is influenced by a wide range of factors including the circumstances in which people are born, grow
up, live and work. The specific health needs of an area are also influenced by the population’s age and
ethnic mix, as different ethnic groups have different health needs.
The map below shows the geographical location of 53 GP practices within Buckinghamshire.
41
www.alzheimers.org.uk/statistics 2013
42
www.alzheimers.org.uk/statistics 2013
Page 28 of 34Chiltern Commissioning Group
Table : Chiltern Clinical Commissioning Group Locality’s Profile
High Southern Wooburn Amersham Chiltern
Wycombe Green & Chesham CCG
No of GP
9 8 8 9 34
practices
Size of
population as
a %age of the 27 24 27 22 100
total
[2014]
% of
population 13.7 19.6 19.6 20 18
65+
% of
population
from black &
31 14.6 6.9 9 15.9
minority
groups
[2011]
Deprivation
average score
[2010, Range
4.5 –13.6 15.8 9.9 8 8.2% 10.7
Highest =
greater
deprivation]
Source: Chiltern CCG locality profiles
Page 29 of 34Aylesbury Vale Clinical Commissioning Group
Table : Aylesbury Vale Clinical Commissioning Groups locality’s profile.
Central North South Aylesbury Vale
CCG
No of GP
9 7 5 20
practices
Size of
population as
a %age of the 51.8 24.5 23.6 100
total
[2014]
% of
population 19.6 18 21.6 17
65+
% of
population
from black &
20 5.2 3.6 9.8
minority
groups
[2011]
Deprivation
average score
[2010, Range
14 8 7 10
10–19Highest =
greater
deprivation]
Source: Aylesbury Vale CCG locality Profiles
The tables below looks at the percentage of the population recorded for each condition. [Regional and
national comparator values are not available]
Chiltern Clinical Commissioning Group
Page 30 of 34Table: Percentage of population in Chiltern and localities by health conditions
High Southern Wooburn Amersham Chiltern
Wycombe Green & Chesham CCG
Diabetes 5.3 4.4 3.8 4.2 4.4
Coronary
heart 2.7 3.1 2.8 2.8 2.8
disease
Heart
0.5 0.56 0.6 0.5 0.54
Failure
Stroke 1.3 1.82 1.7 1.6 1.63
Depression 5 5.1 4.3 0.5 4.7
Dementia 0.38 0.6 0.5 0.5 0.5
Aylesbury Vale Clinical Commissioning Group
Table : Percentage of population in Aylesbury Vale and localities by health conditions
Central North South Aylesbury Vale
Inner Outer CCG
Diabetes 5 4.2 4.2 4.5 4.5
Coronary
heart 2.4 3.4 3.1
3 3.4
disease
Heart
0.57 0.72 0.59
Failure 0.53 0.57
Stroke
1.3 1.7 1.14 1.79 1.51
Depression 5.7 5.2 5.52 4.8 5.37
Dementia 0.45 0.8 0.63 0.68 0.61
Page 31 of 3411. Appendix 2
National Policy
The National Dementia Strategy – Living Well with Dementia 2009
Living Well with Dementia sets the standard for improving the lives of people with dementia, for their
families and their carers, through raising awareness, encouraging earlier diagnosis and providing high quality
treatment and care.
https://www.gov.uk/government/publications/living-well-with-dementia-a-national-dementia-strategy
Alzheimer’s Society: Delivering on Dementia 2012–2017
The Alzheimer’s Society five year strategy is guided by seven things people with dementia have told the
Society they want to see in their lives:
http://www.alzheimers.org.uk/site/scripts/documents_info.php?documentID=1844&pageNumber=4
Prime Minister’s Challenge on Dementia: March 2012
This document builds on the achievements of the national dementia strategy – Living Well with Dementia.
http://dementiachallenge.dh.gov.uk/
The Health and Social care Act 2012
This legislation changed the way the health service [NHS] works to deliver person-centred healthcare.
Health and Wellbeing Boards have been created in each local authority area with the specific role to
improve health and wellbeing for all and reduce health inequalities between different people.
http://www.legislation.gov.uk/ukpga/2012/7/contents/enacted
The Care Bill (May 2013)
The Care Bill proposes to modernise over 60 years of care and support and brings together over a dozen
different pieces of legislation into a single, clear law built around people’s needs and what they want to
achieve in their lives.
https://www.gov.uk/government/publications/the-care-bill-factsheets
Personal Health Budgets
From October 2014 people have the right to have a personal health budget. This is similar to personal
budgets for social care.
http://www.personalhealthbudgets.england.nhs.uk/
Page 32 of 34QIPP (Quality, Innovation, Productivity and Prevention)
QIPP is a large scale programme of change in health services [NHS].
http://www.2020selection.co.uk/quipp-agenda-nhs-policy.asp
Think Local, Act personal: Next Steps for Transforming Adult Social Care
Think Local, Act Personal builds upon ‘Putting People First (2007)’ and sets out the principles for
‘Personalisation’.
http://www.thinklocalactpersonal.org.uk/
NHS Outcomes Framework [2014/15]
Provides an update on progress made against the implementation of outcome framework.
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/256456/NHS_outcomes.pdf
NHS Five Year Forward View [2014]
Forward View sets out how the health service needs to change, arguing for a more engaged relationship
with people, carers and citizens so that we can promote wellbeing and prevent ill-health.
http://www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf
Local Arrangements
Buckinghamshire Dementia Partnership Board
The Dementia Partnership Board is responsible for developing this strategy and overseeing the delivery of
the action plan to make sure support and services are delivered to people in need of support because of
dementia in line with the local strategy and action plan, as well as national legislation and guidance.
Buckinghamshire Clinical Commissioning Groups [CCG’s]
Buckinghamshire has two CCG’s, Chilterns Clinical Commissioning Group representing the south of
county and Aylesbury Vale Clinical Commissioning Group representing the north of the county.
The CCG’s are statutory organisations led by local GPs who are responsible for commissioning local health
services. They do this by commissioning or buying health and care services.
Buckinghamshire’s Health and Wellbeing Board
Page 33 of 34You can also read