Insulin resistance and obesity in childhood
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
European Journal of Endocrinology (2008) 159 S67–S74 ISSN 0804-4643
Insulin resistance and obesity in childhood
Francesco Chiarelli and Maria Loredana Marcovecchio
Department of Paediatrics, University of Chieti, Via dei Vestini 5, I-66100 Chieti, Italy
(Correspondence should be addressed to F Chiarelli; Email: chiarelli@unich.it)
Abstract
Childhood obesity is a significant health problem that has reached epidemic proportions around the
world and is associated with several metabolic and cardiovascular complications. Insulin resistance is a
common feature of childhood obesity and is considered to be an important link between adiposity and
the associated risk of type 2 diabetes and cardiovascular disease. Insulin resistance is also a key
component of the metabolic syndrome, and its prevalence in the paediatric population is increasing,
particularly among obese children and adolescents. Several factors are implicated in the pathogenesis
of obesity-related insulin resistance, such as increased free fatty acids and many hormones and
cytokines released by adipose tissue.
Valid and reliable methods are essential to assess the presence and the extent of insulin resistance, the
associated risk factors and the effect of pharmacological and lifestyle interventions. The two most
common tests to assess insulin resistance are the hyperinsulinemic euglycemic clamp and the
frequently sampled i.v. glucose tolerance test utilizing the minimal model. However, both these tests are
not easily accomplished, are time consuming, expensive and invasive. Simpler methods to assess
insulin resistance based on surrogate markers derived from an oral glucose tolerance test or from
fasting insulin and glucose levels have been validated in children and adolescents and widely used.
Given the strong association between obesity, insulin resistance and the development of metabolic
syndrome and cardiovascular disease, prevention and treatment of childhood obesity appear to be
essential to prevent the development of insulin resistance and the associated complications.
European Journal of Endocrinology 159 S67–S74
Childhood obesity: dimension of mellitus (T2DM). In particular, insulin resistance is the
the problem most common metabolic alteration related to obesity
(5), and it represents an important link between obesity
Childhood obesity is reaching epidemic proportions and and other metabolic as well as cardiovascular compli-
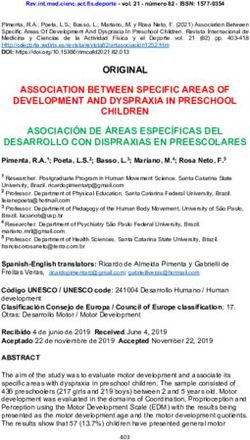
represents the most important chronic disease in this cations (5) (Fig. 1).
age group (1). In the USA 15.8% of children between 6 Data from the Bogalusa Heart Study clearly show that
and 11 years and 16.1% of adolescents have a body almost 20% of obese children have adverse levels of at
mass index (BMI) in the range of overweight (2). Similar least one cardiovascular risk factor (hypercholestero-
trends have also been observed in many European lemia, hyperinsulinemia, hypertriglyceridema, hyper-
countries, where, based on the latest International Task tension) and the presence of multiple risk factors is
Force criteria, overweight and obesity are present in strongly associated with early stages of atherosclerosis
31.8% of school-aged children (3). Furthermore, the (6). As cardiovascular disease is the first cause of
recent phenomenon of ‘nutritional transition’ with a morbidity and mortality in adulthood, the epidemic of
‘westernization’ of food, typical of many developing childhood obesity will cause a real burden for the future
countries, has caused a significant rise in obesity even of the society (1).
among populations that were unaware of this problem Obese children are also at risk of developing
until some years ago (4). psychological problems, orthopaedic and respiratory
Childhood obesity is associated with an increased risk disorders and also certain malignancies (7). Further-
for several metabolic complications, such as insulin more, childhood obesity frequently tracks into adult-
resistance, glucose intolerance and type 2 diabetes hood (8), thus representing a major contributor to the
adult obesity epidemic and to the increased cardiovas-
This paper was presented at the 5th Ferring International Paediatric cular morbidity and mortality in adult life. All these
Endocrinology Symposium, Baveno, Italy (2008). Ferring Pharma- data are alarming and underline how obesity is a real
ceuticals has supported the publication of these proceedings. threat for the health of children and adolescents.
q 2008 European Society of Endocrinology DOI: 10.1530/EJE-08-0245
Online version via www.eje-online.orgS68 F Chiarelli and M L Marcovecchio EUROPEAN JOURNAL OF ENDOCRINOLOGY (2008) 159
adolescents (14), and insulin resistance/hyperinsuline-
mia is believed to be an important link between obesity
and the associated metabolic abnormalities and cardio-
vascular risk (5). Approximately, 55% of the variance in
insulin sensitivity in children can be explained by total
adiposity, after adjusting for other confounders, such as
age, gender, ethnicity and pubertal stage (14). Obese
children have hyperinsulinemia and peripheral insulin
resistance with an w40% lower insulin-stimulated
glucose metabolism than non-obese children (15). In a
recent population-based study conducted in American
adolescents, insulin resistance was detected in w 50%
obese subjects (16) and adiposity was also confirmed to be
the most important factor affecting insulin sensitivity.
Adipose tissue seems to play a key role in the
pathogenesis of insulin resistance through several
released metabolites, hormones and adipocytokines that
can affect different steps in insulin action (17) (Fig. 1).
Adipocytes produce non-esterified fatty acids, which
inhibit carbohydrate metabolism via substrate compe-
tition and impaired intracellular insulin signalling
Figure 1 Obesity-mediated insulin resistance and associated (17–19). In children, as in adults, several ‘adipocyto-
complications. kines’ have been related to adiposity indexes as well as
to insulin resistance.
Obesity-related insulin resistance Adiponectin is one of the most common cytokines
produced by adipose tissue, with an important insulin-
Insulin resistance: definition and pathogenesis sensitizing effect associated with anti-atherogenetic
Insulin resistance is a state in which a given amount of properties (20, 21). Whereas obesity is generally
insulin produces a subnormal biological response (9, associated with an increased release of metabolites by
10). In particular, it is characterized by a decrease in the adipose tissue, levels of adiponectin are inversely related
ability of insulin to stimulate the use of glucose by to adiposity (17). Therefore, reduced levels of this
muscles and adipose tissue and to suppress hepatic adipocytokine has been implicated in the pathogenesis
glucose production and output (10). Furthermore, it of insulin resistance and metabolic syndrome (17).
accounts a resistance to insulin action on protein and Decreased levels of adiponectin have been detected
lipid metabolism and on vascular endothelial function across tertiles of insulin resistance in children and
adolescents (22), where it is a good predictor of insulin
and genes expression (11).
sensitivity, independently of adiposity (23).
Several defects in the insulin signalling cascade have
Adipose tissue also produces tumour necrosis
been implicated in the pathogenesis of insulin resistance,
factor-a, an inflammatory factor, which can alter
such as reduced synthesis or increased degradation of
insulin action at different levels in the intracellular
components of the system, an increased inhibitory serine
pathway (17). Interleukin-6 (IL-6) is another inflam-
phosphorylation of the insulin receptor or the insulin matory cytokine released by adipose tissue and its levels
receptor substrates, the interaction of components of the are increased in obesity (17). IL-6 stimulates the hepatic
system with inhibitory proteins or an alteration of the ratio production of C-reactive protein and this can explain the
of the different proteins of the signalling cascade (10–12). state of inflammation associated with obesity, and could
Insulin resistance is believed to have both genetic and mediate, at least partially, obesity-related insulin
environmental factors implicated in its aetiology (10, resistance (17). Data based mainly on animal studies
13). The genetic component seems to be polygenic in also suggest that increased levels of resistin, another
nature, and several genes have been suggested as molecule produced by adipose tissue, could impair
potential candidates (10). However, several other insulin sensitivity (17). There are also data showing a
factors can influence insulin sensitivity, such as obesity, close relationship between leptin levels and insulin
ethnicity, gender, perinatal factors, puberty, sedentary resistance in children (24). Recently, it has also been
lifestyle and diet (13). shown that serum levels of retinol-binding protein 4
(RBP4) correlate with insulin resistance in subjects with
The role of fatty acids and adipocytokines obesity as well as in those with impaired glucose
tolerance (IGT) or T2DM, therefore suggesting that it
Obesity represents the major risk factor for the could be useful in assessing insulin resistance and the
development of insulin resistance in children and associated risk for complications (25). A study
www.eje-online.orgEUROPEAN JOURNAL OF ENDOCRINOLOGY (2008) 159 Insulin resistance and obesity S69
conducted in normal weight and overweight children combination of these factors, also known as metabolic
has shown that serum RBP4 is independently related to syndrome (41). Furthermore, insulin resistance is
obesity as well as to components of the metabolic associated with systemic inflammation, endothelial
syndrome (26). dysfunction, early atherosclerosis and disordered fibri-
In obese children, diet composition might be an nolysis (42) (Fig. 1). It is alarming that these metabolic
additional factor promoting and/or worsening insulin and cardiovascular complications are already found in
resistance. Animal and human studies suggest that a obese children and adolescents (1). The presence of
high energy intake as well as a diet rich in fat and these alterations in prepubertal children (36, 40, 43) is
carbohydrates and low in fibre could increase the risk of then particularly worrying, as insulin resistance and
developing insulin resistance (27). related complications might be further exacerbated by
the influence of puberty, due to the physiological
decrease in insulin sensitivity associated with normal
The role of fat distribution pubertal development (44).
An altered partitioning of fat between s.c. and visceral or Obese children with a similar BMI can differ on the
ectopic sites has been associated with insulin resistance basis of the degree of insulin resistance in the risk for
(5). Visceral fat has a better correlation with insulin complications. In fact, those with a more impaired
sensitivity than s.c. or total body fat (28), in both obese insulin sensitivity show, for example, a greater risk for
adults and children. Based on the ‘portal theory’, this T2DM and cardiovascular disease (45).
could be related to a higher lipolytic activity of visceral It has also been clearly shown that insulin resistance
when compared with s.c. fat, and therefore to a greater in childhood can track in adult life (46). A recent study
amount of free fatty acids and glycerol carried directly to has shown that insulin resistance at the age of 13 years
the liver (10). Studies conducted in the paediatric predicts insulin resistance at age 19, independently of
population have shown that in girls the amount of BMI, and is also associated with cardiovascular risk in
visceral fat was directly correlated with basal- and adulthood (46).
glucose-stimulated insulin levels and inversely correlated - The fundamental role of insulin resistance in human
with insulin sensitivity and the rate of glucose uptake disease was already recognized in 1988 by Reaven (47)
(28). By contrast, no correlation was found between who emphasized its role in the development of a
abdominal s.c. fat and these metabolic indexes (28). grouping of metabolic abnormalities, which he defined
Ectopic deposition of fat in the liver or muscle can also as syndrome X. Later studies strengthened the concept
be responsible for insulin resistance in obese subjects, as of insulin resistance as a key component of the
the accumulation of fat in these sites impairs insulin metabolic syndrome, a cluster of IGT, dyslipidemia,
signalling, with a reduced glucose uptake in the muscle hypertension, hyperinsulinemia, associated with an
and a decreased insulin-mediated suppression of hepatic increased risk of T2DM and cardiovascular disease
glucose production (5). (41). The prevalence of the metabolic syndrome is not
Intramyocellular lipid (IMCL) accumulation has been particularly high in the overall paediatric population
shown as a factor related to decreased insulin sensitivity (w 4%) but it is as high as 30–50% among overweight
(29, 30). Obese insulin sensitive children and adoles- children and adolescents (22, 48). The presence of
cents present lower levels of visceral fat and IMCL when obesity, mainly visceral obesity and reduced insulin
compared with obese insulin resistant children (31). sensitivity are the main mechanisms implicated in the
Furthermore, higher IMCL has been reported in obese development of the syndrome. A direct correlation
children with IGT when compared with normal glucose between the degree of obesity and insulin resistance and
tolerance (32), suggesting a pathogenetic role of IMCL the prevalence of the metabolic syndrome has been
in the development of insulin resistance and IGT. reported already in obese youths (41).
Accumulation of fat in the liver has also been In obese children and adolescents, insulin resistance
associated with insulin resistance, independently of is the best predictor for the development of IGT (39) and
adiposity (33, 34). Recently, it has also been suggested T2DM (49). T2DM is a progressive disease with a
that deposits of fat around blood vessels can produce gradual increase in insulin resistance associated later
several cytokines and therefore contribute to the with a decline in insulin secretion with fasting
development of insulin resistance, through a so-called hyperglycemia. Over the last decade, there has been
‘vasocrine’ effect (35). an alarming increase of T2DM in youth, concomitant
with the rise of obesity in this age group (49) and in the
USA T2DM now accounts between 8 and 45% of all
Insulin resistance and associated cases of diabetes diagnosed among children and
complications adolescents (49).
Low insulin sensitivity is also a well-known con-
Insulin resistance in obesity is strictly related to the tributor of high blood pressure in children (36, 37, 50).
development of hypertension (36, 37), dyslipidemia Whereas in some studies, this has been attributed to the
(38), IGT (39), hepatic steatosis (40), as well as to the effect of obesity itself, in others insulin resistance has
www.eje-online.orgS70 F Chiarelli and M L Marcovecchio EUROPEAN JOURNAL OF ENDOCRINOLOGY (2008) 159
emerged as a predictor of blood pressure, independent of Assessing insulin resistance
BMI (36, 37, 50). An insulin-mediated effect on the
sympathetic nervous system and on renal sodium Valid and reliable methods are essential to assess the
reabsorption are the main mechanisms suggested as presence and the extent of insulin resistance, the
potential links between insulin resistance and increased associated risk factors and the effect of lifestyle and
blood pressure (51–53). pharmacological interventions. Different methods to
In obese children, insulin resistance is also associated assess insulin resistance are currently available and they
with an abnormal lipid profile, characterized by include fasting measurements of insulin and glucose, the
hypertriglyceridemia, hypercholesterolemia, low HDL- OGTT, the insulin tolerance test, the hyperinsulinemic
cholesterol, which increase the risk of developing early euglycemic clamp and the frequently sampled i.v. glucose
atherosclerosis (54). tolerance test (FSIVGTT) (62).
Increased levels of plasminogen activator inhibitor-1 The two most common tests to measure insulin
and fibrinogen have also been associated with insulin sensitivity are the hyperinsulinemic euglycemic clamp
resistance, and they might contribute to the enhanced and the FSIVGTT utilizing the minimal model (62). These
coagulability and the risk of cardiovascular diseases methods are accurate and, when labelled glucose tracers
related to obesity and insulin resistance (17). are used, they also allow differentiation between hepatic
In obese children, increased levels of inflammatory and muscular insulin resistance (62). Furthermore, the
markers, such as C-reactive protein and IL-6, have been use of stable isotopes also permits the assessment of
shown to progressively increase with insulin resistance protein and lipid metabolism together with insulin
(22), and some of them have been suggested as sensitivity (62). However, both these tests are difficult to
additional components of the metabolic syndrome (22). perform, time consuming, expensive and invasive (62).
In obese children, as in adults, evidence exists on an Simpler methods based on surrogate markers derived from
association between insulin resistance and hepatic fasting insulin and glucose or from an OGTT have been
suggested as potential alternatives. These surrogate
accumulation of fat (40). This has been related to a
measures include: fasting insulin, fasting glucose to
reduced effect of insulin action on adipose tissue, with a
fasting insulin ratio (FGIR), the homeostasis model
consequent lack of suppression of lipolysis and thus an
assessment of insulin resistance (HOMA-IR), the quan-
increased flux of free fatty acids to the liver (55). This
titative insulin sensitivity check index (QUICKI). These
effect, together with an increased hepatic lipogenesis
indices have been validated and proposed for the purpose
related to hyperinsulinemia, is responsible for the
of screening in large populations of adults (62). Validation
accumulation of triglycerides in the hepatocytes and
studies have also been performed in children and
the development of steatosis (55). Increased levels of adolescents with normal glucose tolerance, with good
liver enzymes, particularly alanine aminotransferase correlation coefficients, when compared with the results
(ALT), increase with worsening insulin sensitivity (56). derived from the clamp or FSIVGTT methods (63–65). In
Based on the association of steatosis and increased ALT children and adolescents, the simple use of fasting insulin,
with insulin resistance and IGT in obese adults and in presence of normoglycemia, could be an estimate of
children, steatosis has been suggested as the hepatic insulin resistance as good as HOMA-IR, QUICKI or FGIR
manifestation of the metabolic syndrome (56, 57). (66). However, the validity of these conclusions in children
Insulin resistance has also been associated with the with IGT or T2DM remains to be determined. Further-
development of polycystic ovary syndrome (PCOS), an more, it is also important to acknowledge that there are
ovulatory dysfunction associated with hyperandrogen- some limitations in the use of these surrogate indexes
ism not due to other causes (58). Obese girls with PCOS related to the variability in insulin measurements across
have an w 50% lower insulin sensitivity than obese- laboratories, with a consequent difficulty in comparing
matched controls together with a 40% lower first-phase results obtained in different centres (62). However, these
insulin secretion (59), and have a significantly fasting indexes could be of particular relevance for
increased risk of progression to T2DM, if they are left screening purposes in populations at high risk of diabetes,
without intervention. A screening of adolescents with such as obese children and adolescents.
PCOS demonstrated that 30% had IGT and 4% already Indexes derived from the OGTT have also been
had diabetes (60). developed (67). Some of them, such as the whole body
Insulin resistance has also been suggested as a insulin sensitivity index and the insulin sensitivity index
potential risk factor for the development of respiratory have been validated also in obese children and
problems, such as asthma, in severe obese children adolescents, and a strong correlation between these
and adolescents. In fact, obese children with asthma two indexes and the euglycemic clamp has been
have a higher degree of insulin resistance than obese reported (64). These indexes could have the advantage
children without this respiratory problem, and the over fasting indexes to detect earlier reductions in
state of inflammation associated with insulin resistance insulin sensitivity, mainly related to an impairment of
has been suggested as a possible mediator of this stimulated insulin to increase peripheral glucose uptake
relationship (61). (64). The OGTT can also offer the advantage of
www.eje-online.orgEUROPEAN JOURNAL OF ENDOCRINOLOGY (2008) 159 Insulin resistance and obesity S71
diagnosing IGT or overt diabetes, and to estimate first- Treatment of obesity and insulin
phase insulin responses to a glucose challenge, and thus resistance
to evaluate the relationship between insulin secretion
and insulin sensitivity (64). Therefore, the OGTT could A balanced diet and increased physical activity are
be used as a screening test to assess insulin resistance generally the cornerstone of the treatment of obesity
mainly in severely obese children or in those with other and insulin resistance in children and adolescents.
risk factors associated with obesity, such as a family Decreases in body weight have been associated with a
history of T2DM and cardiovascular diseases, who are at significant improvement in insulin sensitivity (74). A
particular risk not only for insulin resistance but also for recent study has shown that in obese children, an
impaired ß-cell function and IGT (39). Recently, insulin 8-week exercise training programme increased insulin
growth factor binding protein-1 (IGFBP-1) has been sensitivity and was associated with an improvement in
suggested as a new potential plasma marker to assess cardiorespiratory fitness but was independent of
insulin resistance (68). IGFBP-1 seems to have a good measurable changes in body composition (75).
correlation with FSIVGTT assessment of insulin sensi- In children and adolescents, there is not a wide
tivity, particularly in children younger than 10 years experience with weight loss medications or with insulin
(68). However, further studies are required to validate sensitizers. Metformin has been shown to improve insulin
the utility of this marker. sensitivity and BMI in non-diabetic obese adolescents with
fasting hyperinsulinemia and a family history of T2DM
(76). A similar efficacy of metformin on insulin sensitivity
and BMI has been found in two other small studies
Prevention of obesity and insulin conducted in obese normoglycemic adolescents (77, 78).
resistance Sibutramine seems to have a good efficacy in reducing
body weight in children and, in some studies, a positive
Prevention of obesity and insulin resistance includes effect on glucose and lipid metabolism has also been
strategies that need to be started early in life, already shown (79). However, this drug has been associated
during pregnancy and the perinatal period (69). It is with an increase in blood pressure and heart rate,
important to strongly recommend breast feeding and thereby posing limitations for its wide use in the
offer guidance for appropriated food choice, caloric paediatric population (79).
intake and exercise for children (69). The first step of Orlistat is a weight loss drug, which has been
prevention must aim towards maintaining normal BMI investigated in children and has been associated with
(69). A rapid weight gain must be avoided during the a significant weight loss, even though several side effects
first years of life as it causes an early adiposity rebound, have been associated with its use (80); mainly
which is a well-known risk factor for future persistence gastrointestinal disturbances, but also multiple vitamin
of obesity (70). When obesity is already developed, a deficiencies (80). No significant effects on glucose
programme of secondary prevention is required, in metabolism have been reported with this drug (80).
order to reverse or at least to avoid progression of In adults thiazolidinediones have also been shown to
obesity and reduce the risk of co-morbidities (69). have a good efficacy in improving insulin sensitivity (81);
Control of body weight is also particularly important however, their use in children has not been yet approved,
during adolescence, another important period for the based on the lack of relevant studies in this age group.
development of obesity (1). Puberty is a delicate period, Further controlled trials are required in order to have
associated with physiological insulin resistance and a better assessment of the safety and efficacy of drugs to
hyperinsulinemia. Therefore, the presence of obesity in contrast obesity and insulin resistance in children and
this phase, represents an additional stress for the body, adolescents, and to clarify which group of subjects really
with an increased risk for complications (1). needs pharmacological interventions.
Preventive strategies need to be further intensified in
presence of other risk factors, such as a family history of
obesity, T2DM or cardiovascular disease, or the presence Conclusions
of other risk factors for insulin resistance, such as
ethnicity (71). Insulin resistance represents a serious and common
A recent meta-analysis of studies investigating the complication of obesity during childhood and adoles-
effect of prevention of obesity in children and adoles- cence. A timely diagnosis and an appropriated preven-
cents has shown that these interventions are often of tion and treatment of obesity and insulin resistance are
limited success (72), thereby suggesting a need of major required in order to reduce the associated risk of
efforts in preventing childhood obesity. However, the metabolic and cardiovascular complications. Greater
same meta-analysis, as well as another systematic efforts are therefore required in order to avoid obesity
review, have shown that interventions to prevent and the associated insulin resistant status seriously
obesity are at least associated with improved dietary compromising the health of our children and the future
habits and physical activity (72, 73). of our societies.
www.eje-online.orgS72 F Chiarelli and M L Marcovecchio EUROPEAN JOURNAL OF ENDOCRINOLOGY (2008) 159
Disclosure 19 Randle PJ. Regulatory interactions between lipids and
carbohydrates: the glucose fatty acid cycle after 35 years.
This paper forms part of a European Journal of Endocrinology Diabetes/Metabolism Reviews 1998 14 263–283.
supplement, supported by Ferring Pharmaceuticals. The authors disclose: 20 Despres JP. Is visceral obesity the cause of the metabolic syndrome?
no potential conflicting relationship with Ferring. This article was subject Annals of Medicine 2006 38 52–63.
to rigorous peer review before acceptance and publication. 21 Gil-Campos M, Canete RR & Gil A. Adiponectin, the missing link in
insulin resistance and obesity. Clinical Nutrition 2004 23
963–974.
22 Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE, Yeckel CW,
Allen K, Lopes M, Savoye M, Morrison J, Sherwin RS & Caprio S.
References Obesity and the metabolic syndrome in children and adolescents.
New England Journal of Medicine 2004 350 2362–2374.
1 Dietz WH. Overweight in childhood and adolescence. New England 23 Lee S, Bacha F, Gungor N & Arslanian SA. Racial differences in
Journal of Medicine 2004 350 855–857. adiponectin in youth: relationship to visceral fat and insulin
2 Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR & sensitivity. Diabetes Care 2006 29 51–56.
Flegal KM. Prevalence of overweight and obesity among US 24 Chu NF, Wang DJ, Shieh SM & Rimm EB. Plasma leptin
children, adolescents, and adults, 1999–2002. Journal of the concentrations and obesity in relation to insulin resistance
American Medical Association 2004 291 2847–2850. syndrome components among school children in Taiwan – the
3 Wang Y & Lobstein T. Worldwide trends in childhood overweight Taipei Children Heart Study. International Journal of Obesity and
and obesity. International Journal of Pediatric Obesity 2006 1 11–25. Related Metabolic Disorders 2000 24 1265–1271.
4 Bhargava SK, Sachdev HS, Fall CH, Osmond C, Lakshmy R, 25 Graham TE, Yang Q, Bluher M, Hammarstedt A, Ciaraldi TP,
Barker DJ, Biswas SK, Ramji S, Prabhakaran D & Reddy KS. Henry RR, Wason CJ, Oberbach A, Jansson PA, Smith U &
Relation of serial changes in childhood body-mass index to Kahn BB. Retinol-binding protein 4 and insulin resistance in lean,
impaired glucose tolerance in young adulthood. New England obese, and diabetic subjects. New England Journal of Medicine 2006
Journal of Medicine 2004 350 865–875. 354 2552–2563.
5 Weiss R & Kaufman FR. Metabolic complications of childhood 26 Aeberli I, Biebinger R, Lehmann R, L’Allemand D, Spinas GA &
obesity: identifying and mitigating the risk. Diabetes Care 2008 31 Zimmermann MB. Serum retinol-binding protein 4 concentration
(Supplement 2) S310–S316. and its ratio to serum retinol are associated with obesity and
6 Berenson GS, Srinivasan SR, Bao W, Newman WP III, Tracy RE & metabolic syndrome components in children. Journal of Clinical
Wattigney WA. Association between multiple cardiovascular risk Endocrinology and Metabolism 2007 92 4359–4365.
27 Canete R, Gil-Campos M, Aguilera CM & Gil A. Development of
factors and atherosclerosis in children and young adults. The
insulin resistance and its relation to diet in the obese child.
Bogalusa Heart Study. New England Journal of Medicine 1998 338
European Journal of Nutrition 2007 46 181–187.
1650–1656.
28 Caprio S, Hyman LD, Limb C, McCarthy S, Lange R, Sherwin RS,
7 Ebbeling CB, Pawlak DB & Ludwig DS. Childhood obesity: public-
Shulman G & Tamborlane WV. Central adiposity and its metabolic
health crisis, common sense cure. Lancet 2002 360 473–482.
correlates in obese adolescent girls. American Journal of Physiology
8 Guo SS, Wu W, Chumlea WC & Roche AF. Predicting overweight
1995 269 E118–E126.
and obesity in adulthood from body mass index values in
29 Jacob S, Machann J, Rett K, Brechtel K, Volk A, Renn W, Maerker E,
childhood and adolescence. American Journal of Clinical Nutrition
Matthaei S, Schick F, Claussen CD & Haring HU. Association of
2002 76 653–658. increased intramyocellular lipid content with insulin resistance in
9 Kahn CR. Insulin resistance, insulin insensitivity, and insulin lean nondiabetic offspring of type 2 diabetic subjects. Diabetes
unresponsiveness: a necessary distinction. Metabolism 1978 27 1999 48 1113–1119.
1893–1902. 30 Thamer C, Machann J, Bachmann O, Haap M, Dahl D, Wietek B,
10 Matthaei S, Stumvoll M, Kellerer M & Haring HU. Pathophysiology Tschritter O, Niess A, Brechtel K, Fritsche A, Claussen C, Jacob S,
and pharmacological treatment of insulin resistance. Endocrine Schick F, Haring HU & Stumvoll M. Intramyocellular lipids:
Reviews 2000 21 585–618. anthropometric determinants and relationships with maximal
11 Bajaj M & Defronzo RA. Metabolic and molecular basis of insulin aerobic capacity and insulin sensitivity. Journal of Clinical
resistance. Journal of Nuclear Cardiology 2003 10 311–323. Endocrinology and Metabolism 2003 88 1785–1791.
12 Biddinger SB & Kahn CR. From mice to men: insights into the 31 Weiss R, Taksali SE, Dufour S, Yeckel CW, Papademetris X, Cline G,
insulin resistance syndromes. Annual Review of Physiology 2006 Tamborlane WV, Dziura J, Shulman GI & Caprio S. The ‘obese
68 123–158. insulin-sensitive’ adolescent: importance of adiponectin and lipid
13 Liu L, Hironaka K & Pihoker C. Type 2 diabetes in youth. Current partitioning. Journal of Clinical Endocrinology and Metabolism 2005
Problems in Pediatric and Adolescent Health Care 2004 34 90 3731–3737.
(Supplement 1) 254–272. 32 Weiss R, Dufour S, Taksali SE, Tamborlane WV, Petersen KF,
14 Caprio S. Insulin resistance in childhood obesity. Journal of Pediatric Bonadonna RC, Boselli L, Barbetta G, Allen K, Rife F, Savoye M,
Endocrinology and Metabolism 2002 15 487–492. Dziura J, Sherwin R, Shulman GI & Caprio S. Prediabetes in obese
15 Caprio S, Bronson M, Sherwin RS, Rife F & Tamborlane WV. youth: a syndrome of impaired glucose tolerance, severe insulin
Co-existence of severe insulin resistance and hyperinsulinaemia in resistance, and altered myocellular and abdominal fat partition-
pre-adolescent obese children. Diabetologia 1996 39 1489–1497. ing. Lancet 2003 362 951–957.
16 Lee JM, Okumura MJ, Davis MM, Herman WH & Gurney JG. 33 Tiikkainen M, Tamminen M, Hakkinen AM, Bergholm R,
Prevalence and determinants of insulin resistance among US Vehkavaara S, Halavaara J, Teramo K, Rissanen A & Yki-
adolescents: a population-based study. Diabetes Care 2006 29 Jarvinen H. Liver-fat accumulation and insulin resistance in
2427–2432. obese women with previous gestational diabetes. Obesity Research
17 Matsuzawa Y. White adipose tissue and cardiovascular disease. 2002 10 859–867.
Best Practice and Research. Clinical Endocrinology and Metabolism 34 Kelley DE, McKolanis TM, Hegazi RA, Kuller LH & Kalhan SC.
2005 19 637–647. Fatty liver in type 2 diabetes mellitus: relation to regional
18 Griffin ME, Marcucci MJ, Cline GW, Bell K, Barucci N, Lee D, adiposity, fatty acids, and insulin resistance. American Journal of
Goodyear LJ, Kraegen EW, White MF & Shulman GI. Free fatty Physiology. Endocrinology and Metabolism 2003 285 E906–E916.
acid-induced insulin resistance is associated with activation of 35 Yudkin JS, Eringa E & Stehouwer CD. ‘Vasocrine’ signalling from
protein kinase C theta and alterations in the insulin signaling perivascular fat: a mechanism linking insulin resistance to
cascade. Diabetes 1999 48 1270–1274. vascular disease. Lancet 2005 365 1817–1820.
www.eje-online.orgEUROPEAN JOURNAL OF ENDOCRINOLOGY (2008) 159 Insulin resistance and obesity S73
36 Marcovecchio ML, Patricelli L, Zito M, Capanna R, Ciampani M, and fatty liver in childhood obesity: associations with insulin
Chiarelli F & Mohn A. Ambulatory blood pressure monitoring in resistance, adiponectin, and visceral fat. Journal of Clinical
obese children: role of insulin resistance. Journal of Hypertension Endocrinology and Metabolism 2006 91 4287–4294.
2006 24 2431–2436. 57 Musso G, Gambino R, Bo S, Uberti B, Biroli G, Pagano G &
37 Cruz ML, Huang TT, Johnson MS, Gower BA & Goran MI. Insulin Cassader M. Should nonalcoholic fatty liver disease be included in
sensitivity and blood pressure in black and white children. the definition of metabolic syndrome? A cross-sectional compari-
Hypertension 2002 40 18–22. son with Adult Treatment Panel III criteria in nonobese
38 Howard BV & Howard WJ. Dyslipidemia in non-insulin-dependent nondiabetic subjects Diabetes Care 2008 31 562–568.
diabetes mellitus. Endocrine Reviews 1994 15 263–274. 58 Rosenfield RL. Clinical review: identifying children at risk for
39 Sinha R, Fisch G, Teague B, Tamborlane WV, Banyas B, Allen K, polycystic ovary syndrome. Journal of Clinical Endocrinology and
Savoye M, Rieger V, Taksali S, Barbetta G, Sherwin RS & Caprio S. Metabolism 2007 92 787–796.
Prevalence of impaired glucose tolerance among children and 59 Arslanian SA, Lewy VD & Danadian K. Glucose intolerance in
adolescents with marked obesity. New England Journal of Medicine obese adolescents with polycystic ovary syndrome: roles of insulin
2002 346 802–810. resistance and beta-cell dysfunction and risk of cardiovascular
40 D’Adamo E, Impicciatore M, Capanna R, Loredana disease. Journal of Clinical Endocrinology and Metabolism 2001 86
Marcovecchio M, Masuccio FG, Chiarelli F & Mohn AA. Liver 66–71.
steatosis in obese prepubertal children: a possible role of insulin
60 Palmert MR, Gordon CM, Kartashov AI, Legro RS, Emans SJ &
resistance. Obesity 2008 16 677–683.
Dunaif A. Screening for abnormal glucose tolerance in adolescents
41 Eckel RH, Grundy SM & Zimmet PZ. The metabolic syndrome.
with polycystic ovary syndrome. Journal of Clinical Endocrinology
Lancet 2005 365 1415–1428.
42 Dandona P, Aljada A & Mohanty P. The anti-inflammatory and and Metabolism 2002 87 1017–1023.
potential anti-atherogenic effect of insulin: a new paradigm. 61 Al-Shawwa BA, Al-Huniti NH, DeMattia L & Gershan W. Asthma
Diabetologia 2002 45 924–930. and insulin resistance in morbidly obese children and adolescents.
43 Giannini C, de Giorgis T, Scarinci A, Ciampani M, Journal of Asthma 2007 44 469–473.
Marcovecchio ML, Chiarelli F & Mohn A. Obese related effects of 62 Borai A, Livingstone C & Ferns GA. The biochemical assessment of
inflammatory markers and insulin resistance on increased carotid insulin resistance. Annals of Clinical Biochemistry 2007 44
intima media thickness in pre-pubertal children. Atherosclerosis 324–342.
2008 197 448–456. 63 Conwell LS, Trost SG, Brown WJ & Batch JA. Indexes of insulin
44 Caprio S, Plewe G, Diamond MP, Simonson DC, Boulware SD, resistance and secretion in obese children and adolescents: a
Sherwin RS & Tamborlane WV. Increased insulin secretion in validation study. Diabetes Care 2004 27 314–319.
puberty: a compensatory response to reductions in insulin 64 Yeckel CW, Weiss R, Dziura J, Taksali SE, Dufour S, Burgert TS,
sensitivity. Journal of Pediatrics 1989 114 963–967. Tamborlane WV & Caprio S. Validation of insulin sensitivity
45 Bacha F, Saad R, Gungor N & Arslanian SA. Are obesity-related indices from oral glucose tolerance test parameters in obese
metabolic risk factors modulated by the degree of insulin children and adolescents. Journal of Clinical Endocrinology and
resistance in adolescents? Diabetes Care 2006 29 1599–1604. Metabolism 2004 89 1096–1101.
46 Sinaiko AR, Steinberger J, Moran A, Hong CP, Prineas RJ & Jacobs DR 65 Gungor N, Saad R, Janosky J & Arslanian S. Validation of surrogate
Jr. Influence of insulin resistance and body mass index at age 13 on estimates of insulin sensitivity and insulin secretion in children
systolic blood pressure, triglycerides, and high-density lipoprotein and adolescents. Journal of Pediatrics 2004 144 47–55.
cholesterol at age 19. Hypertension 2006 48 730–736. 66 Schwartz B, Jacobs DR Jr, Moran A, Steinberger J, Hong CP &
47 Reaven GM. Banting lecture 1988. Role of insulin resistance in Sinaiko AR. Measurement of insulin sensitivity in children:
human disease. Diabetes 1988 37 1595–1607. comparison between the euglycemic hyperinsulinemic clamp
48 Cook S, Weitzman M, Auinger P, Nguyen M & Dietz WH. and surrogate measures. Diabetes Care 2008 31 783–788.
Prevalence of a metabolic syndrome phenotype in adolescents: 67 Matsuda M & DeFronzo RA. Insulin sensitivity indices obtained
findings from the third National Health and Nutrition Exami- from oral glucose tolerance testing: comparison with the
nation Survey, 1988–1994. Archives of Pediatrics & Adolescent euglycemic insulin clamp. Diabetes Care 1999 22 1462–1470.
Medicine 2003 157 821–827. 68 Motaghedi R, Gujral S, Sinha S, Sison C, Ten S & Maclaren NK.
49 Alberti G, Zimmet P, Shaw J, Bloomgarden Z, Kaufman F & Insulin-like growth factor binding protein-1 to screen for insulin
Silink M. Type 2 diabetes in the young: the evolving epidemic: the resistance in children. Diabetes Technology & Therapeutics 2007 9
International Diabetes Federation Consensus Workshop. Diabetes 43–51.
Care 2004 27 1798–1811. 69 Barlow SE. Expert committee recommendations regarding the
50 Lurbe E, Torro I, Aguilar F, Alvarez J, Alcon J, Pascual JM & prevention, assessment, and treatment of child and adolescent
Redon J. Added impact of obesity and insulin resistance in
overweight and obesity: summary report. Pediatrics 2007 120
nocturnal blood pressure elevation in children and adolescents.
S164–S192.
Hypertension 2008 51 635–641.
70 Whitaker RC, Pepe MS, Wright JA, Seidel KD & Dietz WH. Early
51 Rowe JW, Young JB, Minaker KL, Stevens AL, Pallotta J &
Landsberg L. Effect of insulin and glucose infusions on sympathetic adiposity rebound and the risk of adult obesity. Pediatrics 1998
nervous system activity in normal man. Diabetes 1981 30 101 E5.
219–225. 71 Davis MM, Gance-Cleveland B, Hassink S, Johnson R, Paradis G &
52 Landsberg L. Insulin resistance and hypertension. Clinical and Resnicow K. Recommendations for prevention of childhood
Experimental Hypertension 1999 21 885–894. obesity. Pediatrics 2007 120 (Supplement 4) S229–S253.
53 DeFronzo RA. The effect of insulin on renal sodium metabolism. A 72 Summerbell CD, Waters E, Edmunds LD, Kelly S, Brown T &
review with clinical implications. Diabetologia 1981 21 165–171. Campbell KJ. Interventions for preventing obesity in children.
54 Maclaren NK, Gujral S, Ten S & Motagheti R. Childhood obesity Cochrane Database of Systematic Reviews 2005 CD001871.
and insulin resistance. Cell Biochemistry and Biophysics 2007 48 73 Flodmark CE, Marcus C & Britton M. Interventions to prevent
73–78. obesity in children and adolescents: a systematic literature review.
55 Browning JD & Horton JD. Molecular mediators of hepatic steatosis International Journal of Obesity 2006 30 579–589.
and liver injury. Journal of Clinical Investigation 2004 114 74 Reinehr T, Kiess W, Kapellen T & Andler W. Insulin sensitivity
147–152. among obese children and adolescents, according to degree of
56 Burgert TS, Taksali SE, Dziura J, Goodman TR, Yeckel CW, weight loss. Pediatrics 2004 114 1569–1573.
Papademetris X, Constable RT, Weiss R, Tamborlane WV, 75 Bell LM, Watts K, Siafarikas A, Thompson A, Ratnam N,
Savoye M, Seyal AA & Caprio S. Alanine aminotransferase levels Bulsara M, Finn J, O’Driscoll G, Green DJ, Jones TW & Davis EA.
www.eje-online.orgS74 F Chiarelli and M L Marcovecchio EUROPEAN JOURNAL OF ENDOCRINOLOGY (2008) 159 Exercise alone reduces insulin resistance in obese children 79 Berkowitz RI, Wadden TA, Tershakovec AM & Cronquist JL. independently of changes in body composition. Journal of Clinical Behavior therapy and sibutramine for the treatment of adolescent Endocrinology and Metabolism 2007 92 4230–4235. obesity: a randomized controlled trial. Journal of the American 76 Freemark M & Bursey D. The effects of metformin on body mass Medical Association 2003 289 1805–1812. index and glucose tolerance in obese adolescents with fasting 80 Chanoine JP, Hampl S, Jensen C, Boldrin M & Hauptman J. Effect of hyperinsulinemia and a family history of type 2 diabetes. Pediatrics orlistat on weight and body composition in obese adolescents: a 2001 107 E55. randomized controlled trial. Journal of the American Medical 77 Srinivasan S, Ambler GR, Baur LA, Garnett SP, Tepsa M, Yap F, Association 2005 293 2873–2883. Ward GM & Cowell CT. Randomized, controlled trial of metformin 81 Yki-Jarvinen H. Thiazolidinediones. New England Journal of for obesity and insulin resistance in children and adolescents: Medicine 2004 351 1106–1118. improvement in body composition and fasting insulin. Journal of Clinical Endocrinology and Metabolism 2006 91 2074–2080. 78 Kay JP, Alemzadeh R, Langley G, D’Angelo L, Smith P & Holshouser S. Beneficial effects of metformin in normoglycemic Received 26 March 2008 morbidly obese adolescents. Metabolism 2001 50 1457–1461. Accepted 17 September 2008 www.eje-online.org
You can also read