Identification of Prognostic Risk Model Based on DNA Methylation-Driven Genes in Esophageal Adenocarcinoma
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hindawi BioMed Research International Volume 2021, Article ID 6628391, 20 pages https://doi.org/10.1155/2021/6628391 Research Article Identification of Prognostic Risk Model Based on DNA Methylation-Driven Genes in Esophageal Adenocarcinoma Yuhua Chen,1 Jinjie Wang,2,3 Hao Zhou,2,3 Zhanghao Huang,2,3 Li Qian ,4 and Wei Shi 5 1 Nantong Health College of Jiangsu Province, Nantong, 226010 Jiangsu, China 2 Nantong Key Laboratory of Translational Medicine in Cardiothoracic Diseases and Research Institution of Translational Medicine in Cardiothoracic Diseases, Affiliated Hospital of Nantong University, Nantong, 226001 Jiangsu, China 3 Department of Thoracic Surgery, Affiliated Hospital of Nantong University, Nantong, 226001 Jiangsu, China 4 Department of Oncology, Affiliated Hospital of Nantong University, Nantong 226001, China 5 Department of Science and Technology, Affiliated Hospital of Nantong University, Nantong 226001, China Correspondence should be addressed to Li Qian; ntqianli@163.com and Wei Shi; fyweis@ntu.edu.cn Received 7 December 2020; Revised 15 April 2021; Accepted 8 May 2021; Published 11 June 2021 Academic Editor: Suyan Tian Copyright © 2021 Yuhua Chen et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. DNA methylation is an important part of epigenetic modification, and its abnormality is closely related to esophageal adenocarcinoma (EAC). This study was aimed at using bioinformatics analysis to identify methylation-driven genes (MDGs) in EAC patients and establish a risk model as a biological indicator of EAC prognosis. Method. Downloaded EAC DNA methylation, transcriptome, and related clinical data from TCGA database. MethylMix was used to identify MDGs. R package clusterProfiler and the ConsensusPathDB online database were used to analyze the rich functions and pathways of these MDGs. The prognostic risk model was established by univariate Cox regression, Lasso regression, and multivariate Cox regression analysis. Finally each MDG in the model were carried out through the survival R package. Results. A total of 273 MDGs were identified, which were enriched in transcriptional regulation and embryonic organ morphogenesis. Cox regression analysis established a risk model consisting of GPBAR1, OLFM4, FOXI2, and CASP10. In addition, further survival analysis revealed that OLFM4 and its two related sites were significantly related to the EAC patients’ survival. Conclusion. In summary, this study used bioinformatics methods to identify EAC MDGs and established a reliable risk prognosis model. It provided potential biomarkers for the early treatment and prognosis evaluation of EAC. 1. Introduction States from 2009 to 2015 is only 20%, most of which are EAC patients [5]. Almost all EAC develop from Barrett’s Esophageal cancer (EC) is a common malignant tumor of the esophagus (BE), which is the most important facilitator for digestive system. Its global morbidity and total mortality EAC. However, progress from BE to EAC is very slow, and ranked seventh and sixth, respectively, in 2018 [1]. There are patients with BE usually have no obvious symptoms, which two main histological subtypes of EC, esophageal adenocarci- make early diagnosis and treatment impossible [6]. Current noma (EAC) and esophageal squamous cell carcinoma treatment methods for EAC include a combination of surgery, (ESCC). Among them, ESCC is the principal subtype, chemotherapy, and radiation therapy. However, EAC usually accounting for 80% of all EC [2]. ESCC is one of the most has metastasized at the time of diagnosis, so the patient’s prog- aggressive squamous cell carcinomas, which is very wide- nosis is poor [7]. Therefore, early diagnosis and intervention spread in Southeast Asia and Africa. Since the diagnosis is gen- are of great significance to reduce the morbidity and mortality erally at an advanced stage, the mortality rate is high [3, 4]. of EAC. However, in the western world, the incidence of EAC is Epigenetic modification plays an important role in the increasing at an alarming rate, and the overall 5-year relative occurrence and development of tumors and may cause survival rate of esophageal cancer diagnosed in the United changes in the expression of tumor-related genes in the early
2 BioMed Research International stage [8]. Among them, DNA methylation is an important came from the Illumina HiSeq RNASeq platform and the aspect of epigenetics research, and its relationship between Illumina Infinium Human Methylation 450k platform, tumors has been a hot research topic in recent years [9–11]. respectively. Meanwhile, when studying the clinical prognosis, Generally, tumor-suppressor genes are usually hypermethy- samples with incomplete clinical information (including 16 lated and their transcription levels are reduced, while hypo- EAC tissues) had been excluded (Table S1). methylation of tumor-promoting genes increases their At the same time, we downloaded the EAC and esopha- expression, thereby jointly promoting the maintenance and geal normal squamous tissue methylation expression data development of tumors [12]. Since DNA methylation usually set GSE81334 from GEO (https://www.ncbi.nlm.nih.gov/ occurs in the early stages of cancer, and in future studies, we geo/). We selected 56 cases of esophageal normal squamous are expected to detect EAC early by detecting changes in tissue and 23 cases of EAC in this data set for the next study. DNA methylation in the blood, so we can detect the occur- The GSE81334 data set was built on the results of the Illu- rence of cancer earlier by monitoring changes in the gene mina HumanMethylation450 BeadChip. DNA methylation status [13]. With the superiority of the big data field, online publicly 2.2. Identification of MDGs. First, the LIMMA package in R available databases such as The Cancer Genome Atlas software was used to normalize the downloaded data [17]. (TCGA) contain gene expression levels, methylation charac- With the help of the MethylMix R software package, we obtain teristics, and related clinical prognosis information of various the DNA methylation value of all CpG sites related to each tumors and normal samples [14]. This allows us to find gene, and the total β value of each gene was calculated by aver- potential aberrant DNA methylation genes through online aging all the methylation value. Then, the MDGs were identi- databases. In order to find methylation-driven genes (MDGs) fied with the screening criteria of (∣logFC ∣ >0:2, P < 0:05, in EAC patients, we used the MethylMix R software package, ∣Cor ∣ >0:3). At the same time, Pheatmap R software package which is an algorithm based on the β mixed model that can was used to draw the differential distribution map of the compare the DNA methylation status of tumors and normal expression and methylation of these genes. Finally, we estab- samples and perform correlation analysis through tran- lished a β-mixed model with these MDGs. All data came scriptome data to identify the MDGs of the disease. More directly from the TCGA database and did not require the precisely, the MethylMix package first identifies each CpG approval of the local ethics committee. site and associates it with the closest gene. Secondly, the 2.3. Enrichment Analysis and Functional Annotations of the methylation status of genes is determined by univariate MDGs. Gene Ontology (GO) and Kyoto Encyclopedia of mixed β model. The variable included in the mixed model Genes and Genomes (KEGG) pathways of these MDGs were is the DNA value, which refers to the β value. For a gene, each performed using the R package cluster profiler based on the β mixed value represents a class of patients, and their β http://org.Hs.eg.db database [18]. The GO and KEGG analy- methylation status is determined as a distribution of specific sis results were visualized using the enrichplot and the DNA values. The methylation status of cancer is compared GOplot package [19]. In addition, the signal pathway analysis with the methylation status of normal tissues to screen out of MDGs was carried out by ConsensusPathDB, which genes with different degrees of methylation. Finally, if the contains 32 different public databases and describes multiple methylation level of a gene in the linear regression equation functional aspects of genes, proteins, complexes, and metab- can be significantly correlated with the gene mRNA expres- olites [20]. We set the P value < 0.05 as the default setting. sion, then this is the MDG we need [15, 16]. In this study, we used bioinformatics methods to extract 2.4. Construction of a Prediction Risk Model Based on the RNA data, DNA methylation data, and clinical data of EAC MDGs. In order to screen out the MDGs related to the prog- patients from TCGA. Then, MethylMix R software package nosis of EAC patients, we used Survival R software package to was utilized to obtain MDGs. In addition, a practical and perform univariate Cox regression analysis, Lasso regression reliable prognostic risk model was established and verified. analysis, and multivariate Cox regression analysis to This model can effectively identify patients with poor prog- construct a prognostic risk model [21]. The regression coeffi- nosis and guide individualized treatment. Finally, based on cient was then multiplied by the corresponding mRNA level the gene methylation level and the methylation level of to obtain the prognostic risk score. The screening criteria gene-related sites, survival analysis was conducted to further were all P < 0:05. study the potential key targets in the model. 2.5. Assessment of the Accuracy of the Risk Model. According 2. Materials and Methods to the formula, the risk score of each EAC patient in TCGA was obtained, and then, the median was taken to divide the 2.1. Data Source. RNA-sequencing data (including 9 normal EAC patients into two groups (high-risk and low-risk). The esophageal tissues and 78 EAC tissues), DNA methylation data Kaplan-Meier survival analysis in the survival R package (including 12 normal esophageal tissues and 87 EAC tissues), was used to compare the overall survival (OS) rate of the and the original clinical data of EAC patients (including 87 two groups [22]. Then, we used the survivalROC package EAC tissues) were downloaded from the official website of to draw a 3-year dependent receiver operating characteristic the TCGA database (https://portal.gdc.cancer.gov) (Table S3). (ROC) curve to evaluate the accuracy of the model [23]. Among them, 78 EAC tissues have both RNA-seq and DNA The AUC value is between 1.0 and 0.5. When the AUC is methylation data. The transcriptome and methylation data closer to 1, the diagnostic effect is better. In addition, the
BioMed Research International 3 Type 10 5 0 −5 Type Normal Tumor (a) Figure 1: Continued.
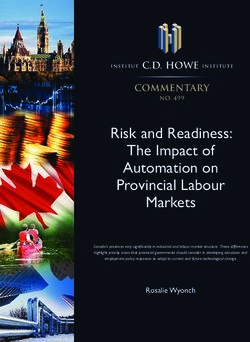
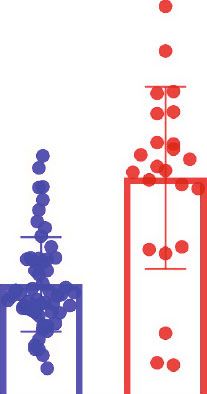
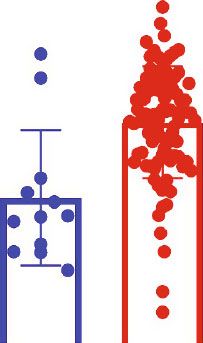
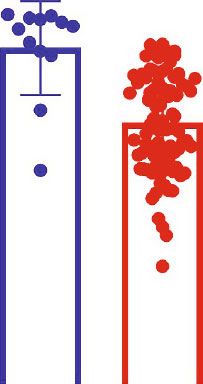
4 BioMed Research International Type 0.8 0.6 0.4 0.2 Type Normal Tumor (b) Figure 1: Heat map of MDGs between esophageal adenocarcinoma (EAC) and esophageal normal tissues. The blue rectangular bar at the top of the figure represents esophageal normal tissues, and the red rectangular bar represents EAC tissues. (a) Heat map of mRNA expression of MDGs: red: upregulated genes; blue: downregulated genes. (b) Heat map of DNA methylation β value: red: hypermethylated genes; green: hypomethylated genes.
BioMed Research International 5 Cor = −0.802 (P value = 1.064e‑18) Mixture model of ZNF518B 8 5 4 6 ZNF518B expression Density 3 4 2 2 1 0 0 0.00 0.25 0.50 0.75 1.00 0.2 0.3 0.4 0.5 0.6 0.7 DNA methylation ZNF518B methylation Mixture component 1 2 (a) (b) Cor = −0.763 (P value = 4.789e‑16) Mixture model of ZNF502 5 4 4 ZNF502 expression 3 3 Density 2 2 1 1 0 0 0.00 0.25 0.50 0.75 1.00 0.3 0.4 0.5 0.6 0.7 DNA methylation ZNF502 methylation Mixture component 1 2 (c) (d) Figure 2: Typical examples of MDGs. (a, c) Correlation between methylation level and gene expression: the abscissa is the β value of the DNA methylation, and the ordinate represents the mRNA expression of the gene. Cor is the correlation coefficient. (b, d) Distribution of methylation level of MDGs: red curve: the methylation level of EAC tissue; green curve: the methylation level of normal tissue; 1: normal tissue; 2: tumor tissue. clinical characteristics (age, gender, stage, T, M, and N) and 2.7. Survival Analysis of MDGs and Related Sites in the Risk risk score were combined to perform univariate Cox analysis, Model. In order to evaluate the independent prognostic and multivariate analysis was then performed to further evaluation of each MDG in the risk model, we conducted sur- determine whether the risk score was an independent risk vival analysis on the methylation level of each MDG and per- factor. At the same time, a stratified analysis was carried formed Kaplan-Meier curve analysis through the survival R out according to the clinical pathological characteristics of package. In addition, we used the Perl software package to the patient’s gender, tumor grade, and stage. extract methylation-related sites from the methylation data of EAC patients downloaded by TCGA. We combined meth- 2.6. Validation of the Methylation Risk Model through the ylation sites with corresponding transcriptome data to assess GEO Data Set. The GSE81334 data set was used to verify the effect of methylation sites on their expression. ∣Cor ∣ > the difference in methylation levels of the four MDGs in 0:45 was considered to be highly correlated [24]. We the model between normal esophageal squamous tissue and performed a prognostic survival analysis for each highly cor- EAC. Meanwhile, each sample was scored by the model related methylation site and drew a Kaplan-Meier curve formula to verify the wide applicability of the model in tumor through the survival R package. P < 0:05 was considered and normal samples. statistically significant.
6 BioMed Research International P value Embryonic organ development Embryonic organ morphogenesis Regionalization Sulfur compound biosynthetic process Ear morphogenesis BP Cell fate specification Feeding behavior Linoleic acid metabolic process 0.02 Alpha−linolenic acid metabolic process Serine family amino acid catabolic process Integral component of synaptic membrane Presynaptic membrane Intrinsic component of synaptic membrane Integral component of presynaptic membrane Intrinsic component of presynaptic membrane CC Rough endoplasmic reticulum 0.04 Neuron projection terminus Intercellular bridge Lateral element Calyx of Held Neuropeptide receptor activity RNA polymerase II activating transcription factor binding Neurotransmitter binding 0.06 Ferrous iron binding Galanin receptor activity MF Amine binding Serotonin binding Fatty acid synthase activity Protein serine/threonine phosphatase inhibitor activity Glutathione binding 0.02 0.04 0.06 Gene ratio Count 5 10 15 (a) GO: 71 0048 0 090 562 GO:0 GO ID Description 471 :00 0042 GO:0048562 Embryonic organ morphogenesis 436 5 GO:0043651 Linoleic acid metabolic process 1 GO: GO:0048568 Embryonic organ development GO: GO:0003002 Regionalization 72 0048 GO:0036109 Alpha−linolenic acid metabolic process 442 0 568 GO:0044272 Sulfur compound biosynthetic process O:0 G GO:0042471 Ear morphogenesis GO 109 030 :00 GO:0009071 Serine family amino acid catabolic process 0036 02 GO: z-score Decreasing Increasing LogFC Upregulated (b) Figure 3: Continued.
BioMed Research International 7 ZNF614 ZNF67 ZNF43 ZNF ZNF ZN ZN logFC ZN 82 F47 583 ZN 5 568 F5 0 F7 5 ZN 879 F5 69 ZN S1 1 90 F8 FA 3 F ZN F52 D 0 Z F7 8 ZN N ZN F25 ZN F350 7 ZN F682 ZNF F793 ZNF 334 ZNF8 492 GSTM 13 ZNF354 2 C ZNF418 ZNF429 SLC6A11 ZNF347 ZFP82 ZNF677 GNB4 GLDC 3 GSTM 65 ZNF6 701 ZNF 254 ZNF F578 ZN NAI1 6 G F25 8 ZN F20 ZN F3 1 ZN F33 F 0 ZN 0 N BH 708 Z GP T M X7 ZN 4 AD 2 CY H 3 2 5 F8 ZNF721 ID L2 VL AMT SRSF8 BST2 ELOV ELO GO terms Herpes simplex virus 1 infection Glutathione metabolism GABAergic synapse Fatty acid elongation Biosynthesis of unsaturated fatty acids Glycine, serine and threonine metabolism Fatty acid metabolism (c) Figure 3: Functional annotation and enrichment analysis of MDGs in EAC. (a) GO analysis is divided into three functional groups: biological process (BP), cell component (CC), and molecular function (MF). The scatter plot shows the top 10 important GO items. (b) GO analysis of significant enrichment items of MDGs in different functional groups. (c) The distribution of MDGs in different KEGG enrichment groups. Dimathylglycine dehydrogenase deficiency Non-ketotic hyperglycinemia Biosynthesis of unsaturated fatty acids - Homo sapiens (human) Gene expression (transcription) RNA polymerase II transcription 3-phosphoglycerate dehydrogenase deficiency Dihydropyrimidine dehydrogenase deficiency (DHPD) Alpha-linolenic (omega3) acid linoleic (omega6) acid metabolism Dimathylglycine dehydrogenase deficiency Glutathione metabolism - Homo sapiens (human) Linoleic acid (LA) metabolism Hyperglycinemia, non-ketatic Amine ligand–binding receptors Transcriptional regulation of pluripotent stem cells Sarcosinemia Glycine and serine metabolism Alpha-linolenic acid (ALA) metabolism Generic transcription pathway Monoamine GPCRs Node label color Node size (# genes) Node color (P value) Edge width (% shared geneas) Edge color (genes from input) The node label color 8 genes Hide legend denotes the type of P < 10−11 1% 41 the gene sets: 104 genes Neighborhood-based set Manually curated pathway P < 10−5 50% 20 Gene ontology category Protein complex 1373 genes P = 1.0 100% 0 Figure 4: Pathway enrichment analysis of MDGs in EAC by ConsensusPathDB. Node size: number of genes; node color: P value; edge width: percentage of shared genes; edge color: genes from input.
8 BioMed Research International 15 15 15 14 12 12 11 10 10 10 9 9 8 6 0 15 13 11 10 8 13 8 10.0 3 9 Partial likelihood deviance 6 9.5 4 Coefficients 6 2 9.0 8 5 7 2 11 0 15 10 8.5 −2 41 16 8.0 −4 14 12 −6 −5 −4 −3 −2 −6 −5 −4 −3 −2 Log ( ) (a) (b) 1.00 ++++++ 1.0 ++ ++ ++ + + Survival probability 0.75 + ++ 0.8 ++ ++ + + + ++ + + True positive rate 0.50 + ++ + 0.6 ++ ++ 0.25 + P = 2.698e−04 0.4 0.00 0 1 2 3 4 5 6 0.2 Time (years) Risk 0.0 + High risk + Low risk 0.0 0.2 0.4 0.6 0.8 1.0 False positive rate Risk score (AUC = 0.868) T (AUC = 0.587) Age (AUC = 0.545) M (AUC = 0.568) Gender (AUC = 0.495) N (AUC = 0.715) Stage (AUC = 0.771) (c) (d) Figure 5: Prognostic risk model based on EAC MDGs. (a) The choice of the adjustment parameter λ by Lasso-penalized Cox regression analysis. (b) Each curve represents a MDG. Tenfold cross-validation was utilized to calculate optimal lambda, which leads to minimum mean cross-validation error. The vertical axis represents the mean-square error, while the horizontal axis represents the value of log (λ). (c) EAC patients were divided into two groups according to the risk model score, and Kaplan-Meier survival curves were compared by log-rank test. P < 0:001. (d) ROC curve of the 3-year overall survival rate of the risk model. 3. Results Table 1: Multivariate Cox regression analysis of 4 MDGs associated with overall survival in EAC patients. 3.1. Identification of MDGs in EAC Patients from TCGA. Download the methylation data of 87 specimens (78 cancer ID Coef HR HR 95L HR 95H P value specimens and 9 normal specimens) and 99 specimens (87 GPBAR1 7.29573 1473.992 9.667861 224729.3 0.004447 cancer specimens and 12 normal specimens) from TCGA. OLFM4 -4.06339 0.017191 0.000272 1.086215 0.054748 First, we performed normalization and difference analysis on the downloaded data through the LIMMA software pack- FOXI2 6.166957 476.7333 8.376708 27131.74 0.002783 age. Then, we assessed the correlation between the methyla- CASP10 13.10559 491681.2 523.6679 4.62E+08 0.000175 tion level and the expression level of each gene based on Abbreviation: HR: hazard ratio. the MethylMix software package. With the standard of ∣ logFC ∣ >0:2, P < 0:05, and ∣Cor ∣ >0:3, we screened 273 MDGs related to EAC, including 250 hypermethylated genes
BioMed Research International 9 10 8 Risk score 6 4 2 0 0 20 40 60 80 Patients (increasing risk socre) High risk Low risk (a) Survival time (years) 6 5 4 3 2 1 0 0 20 40 60 80 Patients (increasing risk socre) Dead Alive (b) Type 0.8 CASP10 0.7 GPBAR1 0.6 0.5 OLFM4 0.4 0.3 FOXI2 0.2 Type High Low (c) Figure 6: The prognostic value of the risk model based on 4 MDGs in EAC. (a) The risk score of each EAC patient in TCGA increases from left to right. (b) The survival time and survival status of each EAC patient in TCGA. (c) The expression levels of MDGs in the risk model in the low-risk group and the high-risk group. and 23 hypomethylated genes (Table S2). The heat maps of in cell development, DNA binding regulation, and transcrip- mRNA expression and DNA methylation β values of these tion regulation. GO analysis showed that in terms of BP, these MDGs are shown in Figures 1(a) and 1(b). genes were enriched in “embryonic organ development, At the same time, the MethylMix R software package was embryonic organ morphogenesis, pattern specification pro- used to draw a distribution map of the methylation degree of cess.” In MF, genes were mainly involved in “DNA-binding MDGs. The two genes with the highest correlation between transcription activator activity, RNA polymerase II-specific, these genes were selected as shown in Figure 2. The distribu- DNA-binding transcription repressor activity, RNA polymer- tion of the degree of methylation indicated that in the normal ase II-specific and RNA polymerase II activating transcription lung tissue group, ZNF518B and ZNF502 presented a hypo- factor binding.” In terms of CC, “integral component of methylated state, while in the EAC cancer group, ZNF518B presynaptic membrane” was their main function (Figures 3(a) and ZNF502 presented a hypermethylated state. In addition, and 3(b)). Figures 2(a) and 2(c) show the correlation between the meth- KEGG showed that these MDGs were mainly enriched in ylation levels of ZNF518B and ZNF502 and their gene expres- “Herpes simplex virus 1 infection.” Through the analysis of sions, respectively. the ConsensusPathDB approach, the methylation-driven genes were mainly enriched in the gene expression, RNA 3.2. Functional Annotation and Enrichment Analysis of MDGs polymerase II transcription, and generic transcription path- in EAC. In order to further explore the molecular mechanism way (Figure 4). of these MDGs during the progress of EAC, we used the R clusterProfiler software package and the ConsensusPathDB 3.3. Establishment of a Risk Model Based on EAC MDGs. Uni- online database for function and pathway enrichment analy- variate Cox regression analysis was performed on the sis. Functional analysis showed that they were mainly involved obtained MDGs, and 16 MDGs related to EAC’s survival
10 BioMed Research International P value Hazard ratio Age 0.194 0.983 (0.957−1.009) Gender 0.346 0.598 (0.205−1.743) Stage 0.001 2.035 (1.322−3.135) T 0.283 1.304 (0.803−2.117) M 0.052 2.459 (0.992−6.095) N 0.117 1.471 (0.907−2.385) Risk score 0.001 1.057 (1.022−1.092) 0 1 2 3 4 5 6 Hazard ratio (a) P value Hazard ratio Age 0.201 0.980 (0.950−1.011) Gender 0.020 0.221 (0.062−0.791) Stage 0.003 5.244 (1.763−15.599) T 0.149 0.617 (0.320−1.189) M 0.097 0.194 (0.028−1.346) N 0.287 0.673 (0.324−1.396) Risk score 0.001 1.060 (1.023−1.098) 0 5 10 15 Hazard ratio (b) Figure 7: Cox analysis on the impact of risk score and clinical characteristics on the survival of EAC patients. (a) Forest plot of univariate Cox regression independent prognostic analysis of EAC patients. (b) Forest plot of independent prognostic analysis of multivariate Cox regression for EAC patients. Hazard ratio > 1 represents risk factors for survival and hazard ratio < 1 represents protective factors for survival. T: tumor, N: node, M: metastasis. were screened out, and the model was further optimized Meanwhile, we established a similar prognostic model through Lasso regression analysis and multivariate Cox based on mRNA expression levels. As shown in Supplemen- regression analysis (Figures 5(a) and 5(b)). Finally, four tary Figure 1, although the prognosis model based on mRNA prognostic-related MDGs (GPBAR1, OLFM4, FOXI2, and expression can also distinguish the prognosis of the high- and CASP10) were supposed to establish a prognostic risk model low-risk groups, its AUC value was 0.727, which was lower (Table 1). Risk score = ð7:2957 × GPBAR1Þ + ð−4:0634 × than the previous model, indicating that its prediction OLFM4Þ + ð6:1670 × FOXI2Þ + ð13:1056 × CASP10Þ. Next, accuracy was lower than that of the methylation risk model. the EAC patients in TCGA were scored according to the At the same time, Figures 6(a) and 6(b), respectively, scoring formula, the median was selected as the cutoff value, showed the risk score, survival time, and survival status of and EAC patients were then divided into high-risk groups each EAC patient. It can be seen from Figure 6 that as the (39 cases) and low-risk groups (39 cases). Kaplan-Meier risk score increased, the survival time of EAC patients survival analysis results show that patients in the high-risk decreased and the proportion of deaths gradually increased. group had poor survival rates (P < 0:01) (Figure 5(c)). Figure 6(c) showed the methylation levels of the 4 MDGs in the low-risk group and the high-risk group. 3.4. The Accuracy and Reliability of the Risk Model. From At the same time, in order to further verify the indepen- Figure 5(d), the AUC value of the model’s 3-year overall dent prognostic value of this model, we extracted EAC survival rate was 0.868. Compared with other clinical traits, patients with complete clinical information. Combining each it can better reflect the prognosis of EAC patients. patient’s age, gender, stage, and pathological T, M, N, and
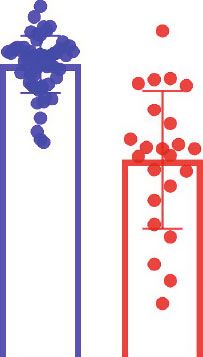
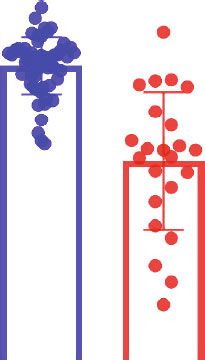
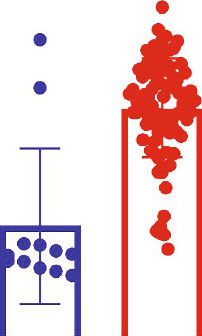
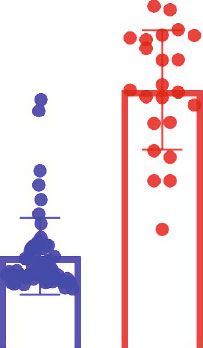
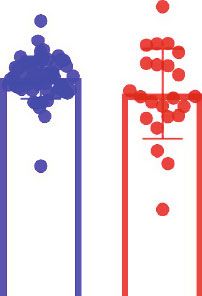
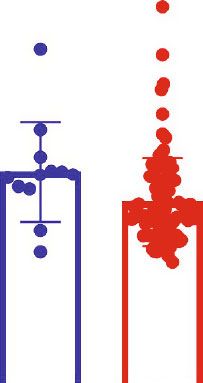
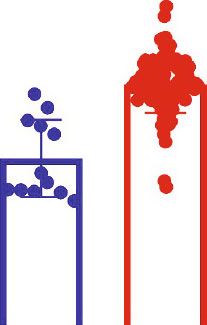
BioMed Research International FOX12 methylation level in TCGA GPBAR1 methylation level in TCGA Methylation risk level in TCGA 0 5 10 15 0.4 0.5 0.6 0.7 0.8 0.9 0.0 0.2 0.4 0.6 0.8 1.0 Normal (n = 12) Normal (n = 12) Normal (n = 12) (c) (a) (e) ⁎⁎ ⁎⁎ ⁎⁎ Tumor (n = 87) Tumor (n = 87) Tumor (n = 87) GPBAR1 methylation level in GSE81334 CASP10 methylation level in TCGA OLFM4 methylation level in TCGA 0.4 0.6 0.8 1.0 0.0 0.2 0.4 0.6 0.8 0.0 0.1 0.2 0.3 0.4 Figure 8: Continued. Normal (n = 56) Normal (n = 12) Normal (n = 12) (f) (b) (d) ⁎ ⁎⁎ ⁎⁎ Tumor (n = 23) Tumor (n = 87) Tumor (n = 87) 11
12 BioMed Research International OLFM4 methylation level in GSE81334 FOX12 methylation level in GSE81334 ⁎⁎ ⁎⁎ 0.9 1.0 0.8 0.8 0.7 0.6 0.6 0.4 0.5 0.2 0.4 0.0 Normal (n = 56) Tumor (n = 23) Normal (n = 56) Tumor (n = 23) (g) (h) ⁎⁎ CASP10 methylation level in GSE81334 ⁎⁎ 0.9 Methylation risk level in GSE81334 17 0.8 16 0.7 15 0.6 14 0.5 13 0.4 12 Normal (n = 56) Tumor (n = 23) Normal (n = 56) Tumor (n = 23) (i) (j) Figure 8: Validate the risk model with the GEO data set. (a–d) DNA methylation status of GPBAR1, OLFM4, FOXI2, and CASP10 in normal and EAC cancer tissues in the TCGA database. (e) The risk values of normal and EAC cancer tissues in the TCGA database. (f–i) DNA methylation status of GPBAR1, OLFM4, FOXI2, and CASP10 in normal and EAC cancer tissues in the GSE81334 data set. (j) GSE81334 data set normal and EAC cancer tissue risk values. Two-tailed P value by unpaired t test, ∗∗ P < 0:0001, ∗ P < 0:05. risk scores, univariate and multivariate Cox regression anal- 3.6. Survival Analysis of MDGs in the Risk Model. To further yses were performed (Figures 7(a) and 7(b)). Both univariate explore the independent prognostic value of each MDG in and multivariate Cox regression analyses showed that the the risk model, we combined the methylation level of each pathological stage and the prognostic risk score can be used MDG with the survival information of EAC patients in as independent prognostic factors. TCGA and drew the survival curve. It can be observed in Figures 9(a)–9(d) that only the methylation level of OLFM4 had an impact on the survival prognosis. The patient group 3.5. Verification of the Risk Model by the GEO Data Set. In with a high OLFM4 methylation level had a better survival order to verify the DNA methylation level of MDGs in the prognosis than the patient group with a low OLFM4 methyl- risk model and the reliability of the risk model, we chose ation level. There was a statistical difference between the two the data set GSE81334 in GEO. As shown in Figures 8(f)– groups (P < 0:05). At the same time, there was no significant 8(i), in the EAC tumor group, FOXI2 was in a hypermethy- differences in the survival prognosis of EAC patients grouped lated state, while in the normal group, OLFM4 and CASP10 based on the GPBAR1, FOXI2, and CASP10 methylation were in a hypermethylated state. These results maintained levels. This indicated that OLFM may have an independent the consistency of the results of the TCGA cohort study prognostic correlation for EAC patients. (Figures 8(a)–8(d)). Interestingly, after scoring the EAC samples and normal esophagus samples in GSE81334, the EAC risk value was significantly higher than that of the 3.7. Correlation Analysis between Methylation Sites and normal esophagus group (Figure 8(j)), which was consistent Corresponding Gene Expression Levels. To make a thorough with the results of the TCGA cohort. inquiry of the specific role of methylation sites for each
BioMed Research International 13 Survival curve (P = 0.348) Survival curve (P = 0.017) 1.0 1.0 0.8 0.8 Survival rate Survival rate 0.6 0.6 0.4 0.4 0.2 0.2 0.0 0.0 0 2 4 6 8 10 0 2 4 6 8 10 Time (year) Time (year) GPBAR1 hypermethylation OLFM4 hypermethylation GPBAR1 hypomethylation OLFM4 hypomethylation (a) (b) Survival curve (P = 0.657) Survival curve (P = 0.367) 1.0 1.0 0.8 0.8 Survival rate Survival rate 0.6 0.6 0.4 0.4 0.2 0.2 0.0 0.0 0 2 4 6 8 10 0 2 4 6 8 10 Time (year) Time (year) FOX12 hypermethylation CASP10 hypermethylation FOX12 hypomethylation CASP10 hypomethylation (c) (d) Figure 9: Kaplan-Meier survival curve of MDGs in the risk model. (a) According to the GPBAR1 methylation level, the EAC patients in the TCGA were divided into high and low groups and their survival curves were drawn. (b) According to the OLFM4 methylation level, the EAC patients in the TCGA were divided into high and low groups and their survival curves were drawn. (c) According to the FOXI2 methylation level, the EAC patients in the TCGA were divided into high and low groups and their survival curves were drawn. (d) According to the CASP10 methylation level, the EAC patients in the TCGA were divided into high and low groups and their survival curves were drawn. MDG in the risk model, we used Perl software to obtain the CASP10 (∣Cor ∣ >0:45) (Figures 10(f)–10(i)). This means that methylation site information about GPBAR1, OLFM4, it is possible that these highly correlated sites have a compre- FOXI2, and CASP10. We found that the GPBAR1 gene had hensive effect on the corresponding genes’ function. 8 sites, of which only cg22678065 had a high correlation with After that, we performed survival analysis on the highly GPBAR1 (Figure 10(a)). The OLFM4 gene had 8 sites, of correlated sites of genes. Using P < 0:05 as an important which cg24932628 and cg12582008 were highly related to indicator of prognosis, we found that there were only two OLFM4 (Figures 10(b) and 10(c)). The FOXI2 gene had 21 prognostic-related sites in these genes: cg24932628 and sites, of which cg26115633 and cg13929328 were highly cg12582008. The high methylation level of these two sites had related to FOXI2 (Figures 10(d) and 10(e)). The CASP10 a better prognosis (Figure 11). This means that cg24932628 gene had 10 sites, of which cg12105450, cg04781494, and cg12582008 may have independent prognostic effects on cg24401737, and cg24599065 were highly correlated with EAC patients.
14 BioMed Research International Cor = −0.522 (P value = 3.051e‑07) Cor = −0.551 (P value = 4.501e‑08) 4 12 10 3 GPBAR1 expression OLFM4 expression 8 2 6 4 1 2 0 0 0.5 0.6 0.7 0.8 0.9 1.0 0.2 0.3 0.4 0.5 0.6 0.7 0.8 cg22678065 methylation cg24932628 methylation (a) (b) Cor = −0.472 (P value = 5.241e‑06) Cor = −0.51 (P value = 6.282e‑07) 12 1.5 10 OLFM4 expression FOX12 expression 8 1.0 6 4 0.5 2 0 0.0 0.2 0.4 0.6 0.8 0.0 0.2 0.4 0.6 0.8 cg12582008 methylation cg26115633 methylation (c) (d) Cor = −0.481 (P value = 3.152e‑06) Cor = −0.608 (P value = 6.5931e‑10) 1.5 4 CASP10 expression FOX12 expression 1.0 3 2 0.5 1 0.0 0.2 0.4 0.6 0.8 0.1 0.2 0.3 0.4 0.5 0.6 0.7 cg13929328 methylation cg12105450 methylation (e) (f) Figure 10: Continued.
BioMed Research International 15 Cor = −0.607 (P value = 7.504e‑10) Cor = −0.535 (P value = 1.316e‑07) 4 4 CASP10 expression CASP10 expression 3 3 2 2 1 1 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.2 0.4 0.6 0.8 cg04781494 methylation cg24401737 methylation (g) (h) Cor = −0.502 (P value = 9.838e‑07) 4 CASP10 expression 3 2 1 0.1 0.2 0.3 0.4 0.5 0.6 cg24599065 methylation (i) Figure 10: Gene methylation sites and gene expression level in risk model. (a) The correlation between methylation sites and gene GPBAR1 expression. (b, c) The correlation between methylation sites and gene OLFM4 expression. (d, e) The correlation between methylation sites and gene FOXI2 expression. (f–i) The correlation between methylation sites and gene CASP10 expression. 4. Discussion driven genes to predict the prognosis of EAC [29]. Therefore, it is of great significance to establish a risk model for early Esophageal cancer (EC) is a common malignant tumor in the diagnosis and survival of EAC. digestive system, and its morbidity and mortality rank With the rapid development of bioinformatics and the among the top ten in China [25]. Esophageal squamous cell sharing of online databases, we can use big data to study carcinoma (ESCC) and esophageal adenocarcinoma (EAC) the molecular characteristics and genetic information about are the main histological subtypes of EC. Drinking and EC and provide an effective basis for seeking potential smoking are the two main risk factors for ESCC [26], and biomarkers. Epigenetics refers to changes in gene expression the pathogenesis of EAC is mainly related to the abnormal that can be inherited without relying on changes in DNA proliferation of esophageal epithelial cells caused by gastro- sequence [8]. DNA methylation is one of the epigenetic mod- esophageal reflux disease (GERD) [27]. Despite surgical ifications; it controls cell proliferation, differentiation, and treatment, radiotherapy, chemotherapy, and the use of apoptosis in eukaryotes and directly or indirectly controls targeted drugs, the prognosis of EC is still very poor [28]. tumorigenesis [30]. In particular, hypermethylation or hypo- Recent studies have demonstrated that lung cancer and lung methylation in the promoter region of a gene will affect the nodules can be distinguished early by detecting changes in expression of the corresponding mRNA, thereby affecting DNA methylation in the blood. This also provides support different stages of tumor development. Recent studies have for us to establish a risk model based on methylation- shown that DNA methylation has been widely used in the
16 BioMed Research International Survival curve (P = 0.184) Survival curve (P = 0.006) 1.0 1.0 0.8 0.8 Survival rate Survival rate 0.6 0.6 0.4 0.4 0.2 0.2 0.0 0.0 0 2 4 6 8 10 0 2 4 6 8 10 Time (year) Time (year) cg2267865 hypermethylation cg24932628 hypermethylation cg2267865 hypomethylation cg24932628 hypomethylation (a) (b) Survival curve (P = 0.001) Survival curve (P = 0.947) 1.0 1.0 0.8 0.8 Survival rate Survival rate 0.6 0.6 0.4 0.4 0.2 0.2 0.0 0.0 0 2 4 6 8 10 0 2 4 6 8 10 Time (year) Time (year) cg12582008 hypermethylation cg26115633 hypermethylation cg12582008 hypomethylation cg26115633 hypomethylation (c) (d) Figure 11: Continued.
BioMed Research International 17 Survival curve (P = 0.934) Survival curve (P = 0.909) 1.0 1.0 0.8 0.8 Survival rate Survival rate 0.6 0.6 0.4 0.4 0.2 0.2 0.0 0.0 0 2 4 6 8 10 0 2 4 6 8 10 Time (year) Time (year) cg13929328 hypermethylation cg12105450 hypermethylation cg13929328 hypomethylation cg12105450 hypomethylation (e) (f) Survival curve (P = 0.206) Survival curve (P = 0.393) 1.0 1.0 0.8 0.8 Survival rate Survival rate 0.6 0.6 0.4 0.4 0.2 0.2 0.0 0.0 0 2 4 6 8 10 0 2 4 6 8 10 Time (year) Time (year) cg04781494 hypermethylation cg24401737 hypermethylation cg04781494 hypomethylation cg24401737 hypomethylation (g) (h) Figure 11: Continued.
18 BioMed Research International Survival curve (P = 0.585) 1.0 0.8 Survival rate 0.6 0.4 0.2 0.0 0 2 4 6 8 10 Time (year) cg24599065 hypermethylation cg24599065 hypomethylation (i) Figure 11: Kaplan-Meier survival curve of relevant methylation sites. (a) GPBAR1-related methylation site survival curve. (b, c) OLFM4- related methylation site survival curve. (d, e) FOXI2-related methylation site survival curve. (f–i) CASP10-related methylation site survival curve. diagnosis and prognosis of different cancer types [31]. Previ- OLFM4, FOXI2, and CASP10 can be used as an independent ous studies have shown that abnormal methylation patterns prognostic factor for EAC. of genes (APC, CdH1, CDKN2A, and ESR1) are not only GPBAR1 (G protein-coupled bile acid receptor 1) is a limited to adenocarcinoma tissues but also found in precan- member of the G protein-coupled receptor (GPCR) superfam- cerous BE tissues. This indicates that DNA hypermethylation ily. GPBAR1 is implicated in the suppression of macrophage is an early epigenetic change in the multistep progression of functions and regulation of energy homeostasis by bile acids EAC [32]. In addition, the methylation frequency of multiple [35]. A previous report stated that GPBAR1 is highly expressed genes (APC, ID4, MGMT, RUNX3, SFRP1, TIMP3, and in human gastric adenocarcinoma and is positively correlated TMEFF2) found in metaplastic BE is similar to EAC. It shows with the expression of the epithelial-mesenchymal transition that gene methylation occurs in the early stage of Barrett’s (EMT) marker N-cadherin. It suggests that GPBAR1 may be metaplasia [33]. Therefore, DNA methylation may become involved in gastric adenocarcinoma [36]. OLFM4 (olfactome- one of the methods for early diagnosis of EAC. Recently, a din 4) is a secreted glycoprotein, usually called the antiapopto- study on EC established an epigenetic signature to evaluate tic molecule GW112 [37]. Olfm4 is frequently upregulated in a the prognosis of EC [34]. However, the prognostic model variety of human tumors, and the latest research shows that for EAC alone is still lacking. Therefore, it is still of great the low expression of OLFM4 is independently associated with significance to discuss the epigenetic changes of EAC and the lymph node metastasis of EAC, so it may prove to be a new the molecular mechanism of its progress separately. biomarker [38]. FOXI2 plays a role during development, In our current study, we screened out 273 MDGs between especially in the early stages of craniofacial development EAC patients and normal samples from TCGA. In order to [39]. Its methylation status may be associated with an examine the functional enrichment of these MDGs, we per- increased risk of oral cancer and colorectal cancer [40, 41]. formed GO and KEGG analysis. They had abundant molecu- CASP10 belongs to the caspase class of promoters, which is lar functions (Mf) with DNA binding transcription activator a homolog of caspase-8 and plays an important role in cell activity. In cellular components (CC), these genes showed apoptosis. CASP10 can inhibit the occurrence of tumors by abundant expression in the components of the presynaptic inhibiting ATP-citrate lyase-mediated and epigenetic repro- membrane. In addition, the biological process (BP) showed gramming [42]. that they were mainly manifested in the process of embryonic For the MDGs in the risk model, we further studied the organ morphogenesis. These functions not only showed the effect of their individual gene methylation levels on the prog- functions enriched by these MDGs but also showed how nosis of EAC patients. The results showed that only OLFM4 abnormal DNA methylation affects genes. had an effect on the prognosis of EAC survival, because DNA To further establish a prognostic risk mode, we used uni- methylation mainly occurs on CpG islands of genomic DNA. variate Cox, Lasso regression, and multiple Cox regression Therefore, we also did a survival analysis on the relevant sites analyses to screen out MDGs related to survival. The results of each methylation driver gene. We found that only two showed that a risk model consisting of the four genes GPBAR1, related sites of OLFM4 in these genes, cg24932628 and
BioMed Research International 19 cg12582008, have an impact on the prognosis. This result [5] R. L. Siegel, K. D. Miller, and A. Jemal, “Cancer statistics, also confirmed that OLFM4 may affect the occurrence, devel- 2020,” CA: a Cancer Journal for Clinicians, vol. 70, no. 1, opment and patient prognosis of cancer through the abnor- pp. 7–30, 2020. mal methylation of these two sites. [6] R. C. Fitzgerald, M. di Pietro, K. Ragunath et al., “British Soci- Compared with previous studies, we separately screened ety of Gastroenterology guidelines on the diagnosis and man- the risk model of EAC MDGs on the prognosis of EAC agement of Barrett's oesophagus,” Gut, vol. 63, no. 1, pp. 7–42, patients. The accuracy and reliability of the model are 2014. verified, and the results show that the model has a certain [7] H. Kuwano, Y. Nishimura, T. Oyama et al., “Guidelines for predictability for the prognosis of EAC patients. diagnosis and treatment of carcinoma of the esophagus April 2012 edited by the Japan Esophageal Society,” Esophagus, vol. 12, no. 1, pp. 1–30, 2015. Data Availability [8] M. Rodriguez-Paredes and M. Esteller, “Cancer epigenetics https://portal.gdc.cancer.gov,https://www.ncbi.nlm.nih.gov/geo/. reaches mainstream oncology,” Nature Medicine, vol. 17, no. 3, pp. 330–339, 2011. [9] A. Bird, “DNA methylation patterns and epigenetic memory,” Conflicts of Interest Genes & Development, vol. 16, no. 1, pp. 6–21, 2002. The authors declare that they have no known competing [10] J. Liu, H. Zhao, Y. Huang et al., “Genome-wide cell-free DNA financial interests or personal relationships that could have methylation analyses improve accuracy of non-invasive diag- appeared to influence the work reported in this paper. nostic imaging for early-stage breast cancer,” Molecular Can- cer, vol. 20, no. 1, p. 36, 2021. [11] H. Y. Huang, J. Li, Y. Tang et al., “MethHC 2.0: information Authors’ Contributions repository of DNA methylation and gene expression in human cancer,” Nucleic Acids Research, vol. 49, no. D1, pp. D1268– Yuhua Chen and Jinjie Wang contributed equally to this D1275, 2021. work. [12] H. Akhavan-Niaki and A. A. Samadani, “DNA methylation and cancer development: molecular mechanism,” Cell Bio- Supplementary Materials chemistry and Biophysics, vol. 67, no. 2, pp. 501–513, 2013. Supplementary Figure 1: prognostic risk model based on [13] K. Ennour-Idrissi, D. Dragic, E. Issa et al., “DNA methylation and breast cancer risk: an epigenome-wide study of normal mRNA expression levels. (A) The expression levels of genes breast tissue and blood,” Cancers, vol. 12, no. 11, p. 3088, 2020. in the risk model in the low-risk group and the high-risk group. (B) EAC patients were divided into two groups [14] G. F. Gao, J. S. Parker, S. M. Reynolds et al., “Before and after: comparison of legacy and harmonized TCGA genomic data according to the risk model score, and Kaplan-Meier survival commons' data,” Cell Systems, vol. 9, no. 1, pp. 24–34.e10, curves were compared by log-rank test. P < 0:001. (C) ROC 2019. curve of the 3-year overall survival rate of the risk model. [15] O. Gevaert, R. Tibshirani, and S. K. Plevritis, “Pancancer anal- Table S1: clinical information of EAC patients in TCGA ysis of DNA methylation-driven genes using MethylMix,” database. Table S2: methylation-driven genes (MDGs) in Genome Biology, vol. 16, no. 1, p. 17, 2015. EAC. 250 hypermethylated genes and 23 hypomethylated [16] O. Gevaert, “MethylMix: an R package for identifying DNA genes are shown in Table S2. The table shows the average methylation-driven genes,” Bioinformatics, vol. 31, no. 11, expression of each MDG in normal and tumor tissues and pp. 1839–1841, 2015. the statistical relationship between the two groups. Table [17] M. E. Ritchie, B. Phipson, D. Wu et al., “limma powers differ- S3: the barcodes of each TCGA file. S4: the R codes of the ential expression analyses for RNA-sequencing and microar- main step. (Supplementary Materials) ray studies,” Nucleic Acids Research, vol. 43, no. 7, p. e47, 2015. [18] G. Yu, L. G. Wang, Y. Han, and Q. Y. He, “clusterProfiler: an R References package for comparing biological themes among gene clus- ters,” OMICS, vol. 16, no. 5, pp. 284–287, 2012. [1] F. Bray, J. Ferlay, I. Soerjomataram, R. L. Siegel, L. A. Torre, and A. Jemal, “Global cancer statistics 2018: GLOBOCAN esti- [19] W. Walter, F. Sanchez-Cabo, and M. Ricote, “GOplot: an R mates of incidence and mortality worldwide for 36 cancers in package for visually combining expression data with func- 185 countries,” CA: a Cancer Journal for Clinicians, vol. 68, tional analysis,” Bioinformatics, vol. 31, no. 17, pp. 2912– no. 6, pp. 394–424, 2018. 2914, 2015. [2] S. Ohashi, S.’. Miyamoto, O. Kikuchi, T. Goto, Y. Amanuma, [20] A. Kamburov, K. Pentchev, H. Galicka, C. Wierling, and M. Muto, “Recent advances from basic and clinical studies H. Lehrach, and R. Herwig, “ConsensusPathDB: toward a of esophageal squamous cell carcinoma,” Gastroenterology, more complete picture of cell biology,” Nucleic Acids Research, vol. 149, no. 7, pp. 1700–1715, 2015. vol. 39, suppl_1, pp. D712–D717, 2011. [3] C. C. Abnet, M. Arnold, and W. Q. Wei, “Epidemiology of [21] I. S. Lossos, D. K. Czerwinski, A. A. Alizadeh et al., “Prediction esophageal squamous cell carcinoma,” Gastroenterology, of survival in diffuse large-B-cell lymphoma based on the vol. 154, no. 2, pp. 360–373, 2018. expression of six genes,” The New England Journal of Medi- [4] D. C. Codipilly, Y. Qin, S. M. Dawsey et al., “Screening for cine, vol. 350, no. 18, pp. 1828–1837, 2004. esophageal squamous cell carcinoma: recent advances,” Gas- [22] Z. Sun and H. M. Xu, “Identifying the minimum number of trointestinal Endoscopy, vol. 88, no. 3, pp. 413–426, 2018. lymph nodes required to ensure adequate pN staging:
20 BioMed Research International Kaplan-Meier survival analysis versus Cox regression model,” [38] L. Suzuki, F. J. C. ten Kate, A. W. Gotink et al., “Olfactomedin Annals of Surgery, vol. 252, no. 2, pp. 410-411, 2010. 4 (OLFM4) expression is associated with nodal metastases in [23] C. Combescure, T. V. Perneger, D. C. Weber, J. P. Daures, and esophageal adenocarcinoma,” PLoS One, vol. 14, no. 7, article Y. Foucher, “Prognostic ROC curves: a method for represent- e0219494, 2019. ing the overall discriminative capacity of binary markers with [39] T. Ohyama and A. K. Groves, “Expression of mouse Foxi class right-censored time-to-event endpoints,” Epidemiology, genes in early craniofacial development,” Developmental vol. 25, no. 1, pp. 103–109, 2014. Dynamics, vol. 231, no. 3, pp. 640–646, 2004. [24] T. Hachiya, R. Furukawa, Y. Shiwa et al., “Genome-wide iden- [40] J. P. Foy, C. R. Pickering, V. A. Papadimitrakopoulou et al., tification of inter-individually variable DNA methylation sites “New DNA methylation markers and global DNA hypome- improves the efficacy of epigenetic association studies,” NPJ thylation are associated with oral cancer development,” Cancer Genomic Medicine, vol. 2, no. 1, p. 11, 2017. Prevention Research (Philadelphia, Pa.), vol. 8, no. 11, [25] S. Yang, S. Lin, N. Li et al., “Burden, trends, and risk factors of pp. 1027–1035, 2015. esophageal cancer in China from 1990 to 2017: an up-to-date [41] S. M. Mitchell, J. P. Ross, H. R. Drew et al., “A panel of genes overview and comparison with those in Japan and South methylated with high frequency in colorectal cancer,” BMC Korea,” Journal of Hematology & Oncology, vol. 13, no. 1, Cancer, vol. 14, no. 1, p. 54, 2014. p. 146, 2020. [42] R. Kumari, R. S. Deshmukh, and S. Das, “Caspase-10 inhibits [26] T. L. Vaughan, S. Davis, A. Kristal, and D. B. Thomas, “Obe- ATP-citrate lyase-mediated metabolic and epigenetic repro- sity, alcohol, and tobacco as risk factors for cancers of the gramming to suppress tumorigenesis,” Nature Communica- esophagus and gastric cardia: adenocarcinoma versus squa- tions, vol. 10, no. 1, p. 4255, 2019. mous cell carcinoma,” Cancer Epidemiology, Biomarkers & Prevention, vol. 4, pp. 85–92, 1995. [27] Y. M. Yang, P. Hong, W. W. Xu, Q. Y. He, and B. Li, “Advances in targeted therapy for esophageal cancer,” Signal Transduction and Targeted Therapy, vol. 5, no. 1, p. 229, 2020. [28] Q. L. Xu, H. Li, Y. J. Zhu, and G. Xu, “The treatments and post- operative complications of esophageal cancer: a review,” Jour- nal of Cardiothoracic Surgery, vol. 15, no. 1, p. 163, 2020. [29] L. M. Schotten, K. Darwiche, M. Seweryn et al., “DNA methyl- ation of PTGER4 in peripheral blood plasma helps to distin- guish between lung cancer, benign pulmonary nodules and chronic obstructive pulmonary disease patients,” European Journal of Cancer, vol. 147, pp. 142–150, 2021. [30] P. M. Das and R. Singal, “DNA methylation and cancer,” Jour- nal of Clinical Oncology, vol. 22, no. 22, pp. 4632–4642, 2004. [31] A. Koch, S. C. Joosten, Z. Feng et al., “Analysis of DNA meth- ylation in cancer: location revisited,” Nature Reviews. Clinical Oncology, vol. 15, no. 7, pp. 459–466, 2018. [32] C. A. Eads, R. V. Lord, S. K. Kurumboor et al., “Fields of aber- rant CpG island hypermethylation in Barrett's esophagus and associated adenocarcinoma,” Cancer Research, vol. 60, no. 18, pp. 5021–5026, 2000. [33] E. Smith, N. J. de Young, S. J. Pavey et al., “Similarity of aber- rant DNA methylation in Barrett's esophagus and esophageal adenocarcinoma,” Molecular Cancer, vol. 7, no. 1, p. 75, 2008. [34] Y. Q. Jin and D. L. Miao, “Multiomic analysis of methylation and transcriptome reveals a novel signature in esophageal can- cer,” Dose-Response, vol. 18, no. 3, article 1559325820942075, 2020. [35] Y. Kawamata, R. Fujii, M. Hosoya et al., “A G protein-coupled receptor responsive to bile acids,” The Journal of Biological Chemistry, vol. 278, no. 11, pp. 9435–9440, 2003. [36] A. Carino, L. Graziosi, C. D’Amore et al., “The bile acid recep- tor GPBAR1 (TGR5) is expressed in human gastric cancers and promotes epithelial-mesenchymal transition in gastric cancer cell lines,” Oncotarget, vol. 7, no. 38, pp. 61021– 61035, 2016. [37] N. H. Kulkarni, C. A. Karavanich, W. R. Atchley, and R. R. Anholt, “Characterization and differential expression of a human gene family of olfactomedin-related proteins,” Geneti- cal Research, vol. 76, no. 1, pp. 41–50, 2000.
You can also read