HIV-Associated Apathy/Depression and Neurocognitive Impairments Reflect Persistent Dopamine Deficits
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

cells
Review
HIV-Associated Apathy/Depression and Neurocognitive
Impairments Reflect Persistent Dopamine Deficits
Kristen A. McLaurin † , Michael Harris † , Victor Madormo † , Steven B. Harrod, Charles F. Mactutus
and Rosemarie M. Booze *
Department of Psychology, University of South Carolina, Columbia, SC 29208, USA;
mclaurik@email.sc.edu (K.A.M.); mwh2@email.sc.edu (M.H.); vmadormo@email.sc.edu (V.M.);
harrods@mailbox.sc.edu (S.B.H.); mactutus@mailbox.sc.edu (C.F.M.)
* Correspondence: booze@mailbox.sc.edu
† These authors contributed equally.
Abstract: Individuals living with human immunodeficiency virus type 1 (HIV-1) are often plagued
by debilitating neurocognitive impairments and affective alterations;the pathophysiology underlying
these deficits likely includes dopaminergic system dysfunction. The present review utilized four
interrelated aims to critically examine the evidence for dopaminergic alterations following HIV-1
viral protein exposure. First, basal dopamine (DA) values are dependent upon both brain region
andexperimental approach (i.e., high-performance liquid chromatography, microdialysis or fast-scan
cyclic voltammetry). Second, neurochemical measurements overwhelmingly support decreased
DA concentrations following chronic HIV-1 viral protein exposure. Neurocognitive impairments,
including alterations in pre-attentive processes and attention, as well as apathetic behaviors, provide
an additional line of evidence for dopaminergic deficits in HIV-1. Third, to date, there is no compelling
evidence that combination antiretroviral therapy (cART), the primary treatment regimen for HIV-1
Citation: McLaurin, K.A.; Harris, M.;
Madormo, V.; Harrod, S.B.; Mactutus,
seropositive individuals, has any direct pharmacological action on the dopaminergic system. Fourth,
C.F.; Booze, R.M. HIV-Associated the infection of microglia by HIV-1 viral proteins may mechanistically underlie the dopamine deficit
Apathy/Depression and observed following chronic HIV-1 viral protein exposure. An inclusive and critical evaluation of the
Neurocognitive Impairments Reflect literature, therefore, supports the fundamental conclusion that long-term HIV-1 viral protein exposure
Persistent Dopamine Deficits. Cells leads to a decreased dopaminergic state, which continues to persist despite the advent of cART. Thus,
2021, 10, 2158. https://doi.org/ effective treatment of HIV-1-associated apathy/depression and neurocognitive impairments must
10.3390/cells10082158 focus on strategies for rectifying decreases in dopamine function.
Academic Editor: Eliseo Eugenin Keywords: dopamine; HIV-1; combination antiretroviral therapy; pre-pulse inhibition; attention;
apathy; microglia; dendritic spines
Received: 6 July 2021
Accepted: 18 August 2021
Published: 21 August 2021
1. Introduction
Publisher’s Note: MDPI stays neutral
with regard to jurisdictional claims in
Since the beginning of the acquired immunodeficiency syndrome (AIDS) epidemic,
published maps and institutional affil- neurocognitive impairments (NCI) and affective alterations have been associated with the
iations. disease [1,2]. Early in the AIDS epidemic, underlying focal processes and opportunistic
infections accounted for approximately 30% of the neurological complications in individu-
als with AIDS; a progressive dementia, however, was more commonly reported [3]. The
identification of human immunodeficiency virus type 1 (HIV-1) as the retroviral etiology
Copyright: © 2021 by the authors.
of AIDS [4,5] led to the hypothesis that NCI and affective alterations may result from
Licensee MDPI, Basel, Switzerland.
the direct effect of the virus on the brain. Indeed, HIV-1 penetrates the central nervous
This article is an open access article
system (CNS) early in the course of infection [6], evidenced by the presence of HIV-1 in
distributed under the terms and postmortem brain tissue [7–9], findings which led to the characterization of this progressive
conditions of the Creative Commons dementia, which became known as AIDS dementia complex (ADC, also recognized as
Attribution (CC BY) license (https:// HIV-associated dementia (HAD)).
creativecommons.org/licenses/by/ ADC, which afflicted approximately 66% of autopsy-verified AIDS patients early in
4.0/). the epidemic, was a neurological syndrome primarily occurring during the later phases of
Cells 2021, 10, 2158. https://doi.org/10.3390/cells10082158 https://www.mdpi.com/journal/cells
Cells 2021, 10, 2158 2 of 30
systemic AIDS [3]. Early clinical characteristics of ADC included NCI (e.g., forgetfulness,
loss of concentration), affective alterations (e.g., apathy) and motor system deficits [3,10,11].
Across time, most patients with ADC exhibited a steady decline in neurocognitive function,
leading to severe dementia, ataxia and motor weakness [10].
Pathologically, distinct abnormalities in the white matter and subcortical structures,
including the basal ganglia, were observed in the brains of individuals with ADC [12],
observations which led researchers to hypothesize dopaminergic system dysfunction as
a potential mechanism underlying the disease [13]. Cerebrospinal fluid (CSF) levels of
dopamine (DA [14,15]) and homovanillic acid (HVA [15–17]), the primary DA metabolite,
were significantly reduced in HIV-1/AIDS patients relative to seronegative controls. In
HIV-1-infected brains, significant reductions in tyrosine hydroxylase (TH), the rate-limiting
enzyme of DA synthesis, were also observed [18]. Most critically, the relationship between
CSF HVA levels and neuropsychological function in HIV-1-infected patients provided
compelling evidence for the role of dopaminergic system dysfunction in the pathogenesis
of ADC [17].
With the discovery and introduction of antiretroviral therapies, however, AIDS/HIV-1
became a chronic, manageable disease, albeit NCI and affective alterations persist. The
development of zidovudine (azidothymidine [19]), the first generation of antiretroviral
therapy, provided early evidence that effective inhibition of HIV-1 may have some effects
on cognitive function in AIDS patients [20–22]. Zidovudine monotherapy did not, however,
mitigate affective alterations [20]. The subsequent utilization of multiple antiretroviral
compounds to treat HIV-1 (i.e., combination antiretroviral therapy (cART)) led to a dra-
matic decrease in the severity of NCI and affective alterations associated with HIV-1 [23].
Specifically, in the post-cART era, ADC is rare, afflicting only 2–8% of cART-treated HIV-1
seropositive individuals [23]. However, milder forms of NCI and affective alterations
persist, afflicting between 30% and 70% of HIV-1 seropositive individuals [24–27].
Although the pathophysiology of HAND and affective alterations in the post-cART era
is likely multidimensional, dopaminergic system dysfunction persists [28–30]. Using four
interrelated aims, the present review will examine evidence for alterations in dopaminergic
levels in HIV-1 in the post-cART era. Given that approximately 73% of HIV-1 seropositive
individuals are currently accessing antiretroviral treatment [31], the present review focuses
on studies using biological systems (i.e., HIV-1 seropositive individuals, primates, rats,
mice) with viral suppression. First, we will report basal/tonic values of DA in the CNS,
including a discussion of the experimental approaches (e.g., high-performance liquid
chromatography (HPLC), microdialysis, fast-scan cyclic voltammetry (FSCV)) used to
measure DA. Second, the present review will examine the prominent evidence, including
both anatomical and clinical symptomology, for the persistent decreased dopamine in
HIV-1 seropositive individuals. Third, the potential effects of cART on the dopaminergic
system will be assessed. Finally, we will address the mechanistic implications for dopamine
decreases in HAND.
2. Basal Dopamine Concentrations in the Central Nervous System
The physiological significance of DA [32], and its presence in the brain [33–35], was
first established in the 1950s. Subsequent methodological advances, including the develop-
ment of microdialysis, HPLC and FSCV, afforded a critical opportunity to detect changes
in basal (or tonic) DA [36]. However, DAs precise influence on cognition and behavior
remains unclear, in large part due to inconsistencies in measured DA levels. Thus, one
of the primary goals was to illustrate the inconsistencies in values via examination of the
standard error of the mean and relative standard error.
DA concentration was estimated using the reported means, which were converted
into ng/g of tissue (Table 1). Reported estimates are collapsed across species and biological
sex under the assumption that the variability between brain regions and methodological
approach are greater than the variability between species and sex [37]. Each manuscript,
therefore, provided a single observation for each brain region that was reported. All
Cells 2021, 10, 2158 3 of 30
estimates, as well as information regarding species and biological sex, are reported in
Supplementary Table S1.
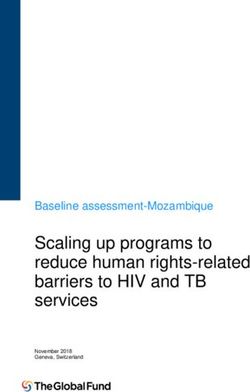
Critical evaluation of the literature revealed that basal DA values are dependent upon
not only brain region, but also methodological technique (between-subjects ANOVA with
log estimated DA concentration in ng/g of tissue as the dependent variable: brain region
by method interaction, F(5,104) = 7.05, p ≤ 0.001, ηp 2 = 0.253; Table 1; Figure 1). For
example, utilization of HPLC to measure DA in the nucleus accumbens (NAc) results in an
average estimated DA concentration over 40,000 times greater than the average estimated
DA concentration measured using microdialysis. This outcome might be anticipated due to
tissue homogenization prior to HPLC measurement; HPLC, therefore, measures total tissue
DA content, whereas microdialysis measures extracellular DA levels [38]. Additionally,
substantial variability in reported basal DA values within a single methodological approach
was observed. For example, the relative standard error for the NAc was 33.9%, 17.1% and
27.8% for HPLC, microdialysis and FSCV respectively, values which are even higher in
other brain regions (e.g., amygdala: 84.1% (HPLC) and 50% (microdialysis)). Given the
substantial variability within and between methodological techniques, a brief discussion
of some of the critical experimental considerations underlying these discrepancies is war-
ranted. In addition, the potential utility of the latest technology (i.e., G protein-coupled
receptor (GPCR) biosensors) for monitoring DA release is briefly reviewed.
Table 1. Estimated basal dopamine (DA) values. Abbreviations: High Performance Liquid Chromatogrphy (HPLC); Fast
Scan Cyclic Voltammetry (FSCV).
Estimated DA
Concentration in ng/g Relative Standard
Brain Region Methodology References
of Tissue Error
(X ± SEM)
HPLC 3683.85 ± 3097 84.1% [39–43]
Amygdala
Microdialysis 0.06 ± 0.03 50% [44–47]
HPLC 16,365.9 ± 12,341.04 75.4% [28,39,41,48–54]
Caudate
Microdialysis 0.88 ± 0.66 75% [44,55,56]
HPLC 200.73 ± 84.41 42.1% [28,39,42,52,54,57–62]
Frontal Cortex
Microdialysis 0.23 ± 0.10 43.5% [44,63–65]
HPLC 35,772.90 ± 12,020.28 33.6% [41–43,51,52,57,59,60,62,66–68]
Nucleus Accumbens Microdialysis 0.76 ± 0.13 17.1% [44,45,47,55,63–65,67–99]
FSCV 6.95 ± 1.93 27.8% [100–104]
HPLC 67,460.52 ± 29,013.28 43% [59,61,62,66,67,105–111]
Striatum
Microdialysis 1.42 ± 0.40 28.2% [64,73,74,76,79,82,85,112–114]
HPLC 9200 [66]
Ventral Tegmental Area
Microdialysis 0.25 ± 0.07 28% [75,83]
2.1. High-Performance Liquid Chromatography (HPLC)
Broadly, chromatography is a well-established separative and analytical technique
introduced by James and Martin [115]; the emergence of HPLC, however, is attributed to
Huber and Hulsman [116]. To conduct HPLC, a pressurized liquid solvent (i.e., mobile
phase) containing the sample is passed through a column filled with a solid adsorbent
material, and each compound elutes at a unique rate, resulting in the separation of compo-
nents as they flow through the column [117]. The isolated compounds are subsequently
identified and quantified using a detector (e.g., UV/Vis spectrometry). HPLC can be
further subdivided into multiple types dependent upon the type of column (e.g., liquid–
liquid, ion-exchange, size exclusion) and “mobile phase” (e.g., non-polar, polar), factors
which influence sensitivity, resolution and the method of brain tissue extraction. Critically,
Cells 2021, 10, 2158 4 of 30
Cells 2021, 10, x FOR PEER REVIEW 4 of 29 pH value,
differences in extraction methodology (e.g., time of initial extraction, aqueous
extraction solvents) result in drastic differences in percent recovery, an indirect measure of
basal DA concentration [118].
Figure 1. Graphical illustration of the profound differences in estimated dopamine (DA) concen-
tration (ng/g of tissue; X ± SEM) dependent upon methodology (i.e., (A) high-performance liquid
chromatography, (B) microdialysis, (C) fast-scan cyclic voltammetry) and brain region. Each dot
represents the estimated DA concentration from a study.Cells 2021, 10, 2158 5 of 30
Given HPLC’s wide use, sources of random and systematic error in HPLC have
been studied extensively [119]. The brief discussion in the present review will focus on
sources of error reported to affect the electrochemical detection of DA. First, the mobile
phase column composition (e.g., ion pairing agent type, organic modifier, pH) has a
pronounced effect on the capacity factor (k’), retention time, peak height units of DA and
peak symmetry [120–124]. Second, the flow gradient rate, similarly, has a prominent effect
on the resolution of the eluting compounds, k’ and background current [125]. Finally,
chromatographic instrumentation, including the column temperature, alters the retention
time of DA, whereby an increase in column temperature is associated with a decrease in
retention time [123]. Additionally, column age may influence the resolution between DA
and its metabolite (i.e., 3,4-Dihydroxyphenylacetic acid), whereby decreased resolution has
been observed after approximately 500 injections of the biological material directly onto
the column top [121].
2.2. Microdialysis
The utilization of microdialysis to quantify neurotransmitters in the brain was first
reported in the 1970s and 1980s [126–128], research which contributed significantly to
the widespread implementation of microdialysis methods. Microdialysis relies on the
principle of diffusion, whereby molecules move from an area of high concentration to
an area of low concentration. Methodologically, a microdialysis probe composed of a
semipermeable dialysis membrane is surgically implanted into the brain, and a perfusion
medium is infused slowly and continuously [129]. During perfusion, molecules in the
extracellular space diffuse through the semipermeable membrane, are transported into
outflow tubing and are collected for analyte quantification (e.g., HPLC [129]; Figure 2A).
Although microdialysis detects neurotransmitters at low- to sub-nanomolar levels (for
DA, see [113]), the technique has relatively low spatiotemporal resolution and is unable to
evaluate real-time changes in the neurochemical environment.
Despite being considered the “gold standard” for obtaining basal neurotransmitter
levels, methodological limitations may impede precise and/or consistent measurements.
The diameter of a typical microdialysis probe is approximately 300 µm, a size which is
substantially larger than neurons and glial cells (5–100 µm), as well as blood capillaries
(8–10 µm) and vessels (~1 mm) in the brain [130]. Implantation of microdialysis probes,
therefore, damages brain tissue, as evidenced by signs of ischemia [131,132] and a com-
promised blood–brain barrier [131,133]. Additionally, tissue damage resulting from the
microdialysis probe disrupts synapses and neurons [134]. Critically, dopaminergic activity
is disrupted by the implantation of microdialysis probes, as evidenced by both decreased
DA release over post-probe implantation time [135] and alterations in the amplitude of
evoked responses [136,137]. Recently developed novel approaches, including pharmaco-
logical agents [138,139] and a microfabricated probe [140], have the potential to mitigate
some of the concerns regarding tissue disruption.
Consistent measurement of basal DA levels is further dependent upon multiple
methodological details. Although HPLC is often used as a method to quantify the output
from microdialysis, the methodological details discussed within the present section are
conducted prior to the quantification of analytes. First, inappropriate concentrations of
specific ions (e.g., Ca2+ , NA+ , K+ ) in the perfusate medium disrupt the homeostatic balance
of the extracellular environment, altering the basal DA concentration. For example, in-
creases in basal DA concentration are observed when the perfusate medium contains higher
(e.g., 3.4 mM) levels of Ca2+ [63,141] or K+ [128]. In sharp contrast, utilization of a perfusion
solution with too little Ca2+ [128,142] or too little K+ [142] results in decreased extracellular
DA levels. It is vital, therefore, that the composition of perfusion solutions mimic the brain
extracellular fluid; additional parameters, including pH and temperature, are also critical
considerations [143]. Second, substantial increases in the concentrations of extracellular
DA occur immediately following death [144–146]. Basal DA levels subsequently decrease
as the postmortem interval increases [144–146]; albeit, basal DA concentration remainsCells 2021, 10, 2158 6 of 30
elevated, relative to pre-death levels, for at least an hour postmortem [144,145]. Third, in
neutral and basic aqueous solutions, DA degrades rapidly [147], including in many com-
mon (e.g., aCSF, brain dialysate) perfusion solutions [148]. Several approaches, including
temporal proximity (i.e., minimization of the time between sample collection and analy-
sis [149]), addition of stabilizing agents to either the collection bins [65] or microdialysis
media [150] and a microdialysis/LCMS system [148], have been implemented to mitigate
21, 10, x FOR PEER REVIEW 6 of 29
the DA instability problem. Despite the validity of these approaches, inter-laboratory
differences may preclude determining an estimate of the “true” basal DA concentration.
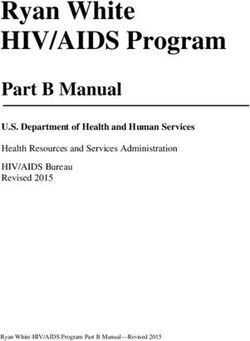
Figure 2. Technical illustration of three of the prominent methods utilized to detect dopamine (DA) levels in the CNS.
Figure 2. Technicalliquid
Given that high-performance illustration of three of the
chromatography prominent
(HPLC) is more methods utilized
classically usedtofor
detect dopamine
analyte (DA) on brain
quantification
levels in the CNS. Given that high-performance liquid chromatography (HPLC) is more classically
tissue homogenates or following microdialysis, the method is not illustrated. (A) During microdialysis, a probe composed
used for analyte quantification on brain tissue homogenates or following microdialysis, the method
of a semipermeable dialysis membrane is surgically implanted into the brain, and a perfusion medium (white arrows) is
is not illustrated. (A) During microdialysis, a probe composed of a semipermeable dialysis mem-
infused slowly
braneandiscontinuously. During perfusion,
surgically implanted molecules
into the brain, andina the extracellular
perfusion medium space diffuse
(white through
arrows) is the semipermeable
infused
membrane,slowly
and areandtransported
continuously.into outflow tubing andmolecules
During perfusion, collected in forthe
analyte quantification
extracellular (e.g., HPLC).
space diffuse through(B) theIn fast-scan
cyclic voltammetry, a small membrane,
semipermeable carbon-fiberand microelectrode is surgically
are transported into outflowimplanted
tubing into
and the brain. for
collected Theanalyte
voltagequan-
potential at the
carbon-fibertification
microelectrode is rapidly
(e.g., HPLC). increased
(B) In fast-scan and decreased,
cyclic resulting
voltammetry, in thecarbon-fiber
a small oxidation and reduction of is
microelectrode DA. During
surgically
the oxidation implanted
and reduction into thethe
processes, brain. The voltage
transfer potential
of electrons at the carbon-fiber
is measured in current at microelectrode
the surface ofisthe rap-
carbon-fiber
idly increased
microelectrode, and decreased,
and the amount of currentresulting in the oxidation
can be subsequently and reduction
converted into theof DA. During of
concentration theDA.
oxidation
Additionally, the
and reduction processes, the transfer of electrons is measured in current at the surface
voltammogram is used for analyte identification, whereby DA exhibits one oxidation and one reduction peak. (C) More of the carbon-
fiber microelectrode, and the amount of current can be subsequently converted into the concentra-
recently, G-protein coupled receptor (GPCR) biosensors for DA have been developed, affording an opportunity to track the
tion of DA. Additionally, the voltammogram is used for analyte identification, whereby DA exhibits
release dynamics of DA. DA biosensors have a circularly permuted fluorescent protein (e.g., Green: cpGFP, Red: cpmApple)
one oxidation and one reduction peak. (C) More recently, G-protein coupled receptor (GPCR) bio-
inserted into the third
sensors forintracellular
DA have been loop of the DAaffording
developed, receptor.anWhen DA binds
opportunity toto the the
track endogenous ligand, the
release dynamics GPCR exhibits
of DA.
a conformational change, resulting in an increased fluorescent intensity. Our laboratory
DA biosensors have a circularly permuted fluorescent protein (e.g., Green: cpGFP, Red: cpmApple) has recently transfected cells
with GRAB-DA2m, a DAthe
inserted into receptor 2 subtype biosensor,
third intracellular loop of thein vitro. Upon stimulation
DA receptor. When DA with binds100 nm endogenous
to the DA, an increase in the
fluorescenceligand,
intensity
theof cpGFP
GPCR is observed.
exhibits a conformational change, resulting in an increased fluorescent intensity.
Our laboratory has recently transfected cells with GRAB-DA2m, a DA receptor 2 subtype biosensor,
2.3. Fast-Scan
in vitro. Upon stimulation withCyclic
100 nm Voltammetry (FSCV)
DA, an increase in the fluorescence intensity of cpGFP is
observed. FSCV, an electroanalytical technique developed in the early 1980s [151,152], affords
a method to detect rapid neurotransmitter dynamics in the brain [153]. From a theoreti-
Despite being considered FSCV
cal perspective, the “gold standard”
relies for obtaining
upon chemical sensingbasal neurotransmitterat carbon-fiber
of neurotransmitters
levels, methodological limitations
microelectrodes. may impede
Specifically, theprecise
voltageand/or consistent
potential measurements.
at the carbon-fiber microelectrode is
The diameter of a typical
rapidly microdialysis
increased probe isresulting
and decreased, approximately 300 μm, and
in the oxidation a size which isof electroactive
reduction
substantially larger than neurons
substances and glial cells
[154]. Examination (5–100
of the μm),
cyclic as well as blood
voltammogram, whichcapillaries
presents data as time
(8–10 μm) and(x-axis)
vesselsby (~1voltage
mm) in(y-axis),
the brain [130].
allows forImplantation of microdialysis
compound identification probes,
[155,156]. The strengths of
therefore, damages
FSCVbrain tissue,
include as evidenced
its high by signs of acuity,
spatial (micrometer) ischemia
high[131,132]
temporaland a com-
(sub-second) resolution
promised blood–brain barrier [131,133]. Additionally, tissue damage resulting from the
microdialysis probe disrupts synapses and neurons [134]. Critically, dopaminergic activ-
ity is disrupted by the implantation of microdialysis probes, as evidenced by both de-
creased DA release over post-probe implantation time [135] and alterations in the ampli-
tude of evoked responses [136,137]. Recently developed novel approaches, includingCells 2021, 10, 2158 7 of 30
and high chemical (nanomolar range) sensitivity. However, FSCV is limited by the need
for digital background subtraction [157], which restricts measurements to relative neuro-
transmitter changes, a factor which precludes the measurement of basal concentrations of
electroactive species [154]. Therefore, FSCV has typically been utilized to measure phasic,
rather than tonic, DA release. Recent novel modifications have afforded an opportunity
to investigate tonic DA concentrations using FSCV [103,104,158,159]. While an in-depth
discussion of these modifications is beyond the scope of this review, it is an emerging
area of research that has the potential to transform our ability to accurately measure basal
DA levels.
2.4. G Protein-Coupled Receptor (GPCR) Biosensors
GPCR biosensors for DA (or DA biosensors), the most recent method developed for
monitoring DA dynamics, were first reported in 2018 [160,161], and contemporary versions
have expanded upon these initial reports [162,163]. Theoretically, fluorescent DA biosensors
rely upon the interaction between DA and D1 - and D2 -like GPCRs. DA biosensors were
developed by inserting a genetically encoded, circularly permuted fluorescent protein
(e.g., Green: cpGFP, Red: cpmApple) into the third intracellular loop of the naturally
occurring human DA receptor. When DA is released, it binds to the endogenous ligand,
causing a rapid conformational change in the GPCR, a conformational change that induces a
profound increase in fluorescence intensity (i.e., 90–900%, for a review, see [164]; Figure 2C).
DA biosensors exhibit high selectivity, molecular specificity, affinity (sub-micromolar) and
resolution (sub-second [160–163,165]), making them ideally suited for tracking DA release.
However, DA biosensors may be limited by low basal fluorescence levels, which precludes
the detection of basal DA levels. A more comprehensive discussion of GPCR biosensors
for DA is provided by Labouesse et al. [164].
2.5. General Experimental Considerations
Ideally, an estimate of basal DA values would be highly replicable when measurements
are obtained in the same brain region, using the same methodological technique and
in nearly genetically identical animals. However, basal DA concentrations are altered
by natural biological variation within and between subjects. Independent of species,
there is natural biological variation in basal DA concentrations resulting from within and
between subject’s factors. For example, basal extracellular DA levels change across the
functional lifespan, with significantly decreased DA observed in aged, relative to young,
animals [166]. Furthermore, basal DA levels in the NAc [167,168], striatum [149,169]
and medial prefrontal cortex (mPFC [170]) fluctuate in a circadian rhythm. Additionally,
hormones have a profound impact on basal DA levels, as evidenced by changes across the
estrous cycle [171,172] and resulting from gonadectomy [173].
To date, the substantial variability between studies, even within a single methodologi-
cal approach, has obfuscated our ability to experimentally determine the “true” basal DA
concentration. When appropriate experimental controls are implemented, the impact of
a treatment (e.g., HIV-1, substance use) on basal DA concentration can be reliably deter-
mined; comparing between studies, however, remains challenging. Stringent and detailed
reporting of methodological procedures may aid in determining which studies can be most
accurately compared. From a practical perspective, however, the information compiled
in Table 1 (expanded in Supplementary Table S1) provides a summary of the techniques
currently in use.
In sum, HPLC of tissue homogenates may reveal total DA tissue content, while
microdialysis enables sampling of the extracellular basal DA levels, but lacks temporal
resolution (minutes) and spatial resolution. FSCV is currently used for relative changes in
DA signals, and not for assessing basal DA levels. Although GPCR biosensors for DA may
not clarify basal DA levels in the brain, their ability to rapidly detect DA function has the
potential to transform our understanding of neural circuits. Critically, each neurochemicalCells 2021, 10, 2158 8 of 30
method for assessing DA levels has benefits and limitations that must be weighed when
designing an experiment.
Cells 2021, 10, x FOR PEER REVIEW
3. Chronic HIV-1 Results in Decreased Dopamine
Inconsistencies in the estimated basal DA values does not preclude the utilization or
importance of these methodological techniques for evaluating 1 infectiongroupindifferences. As demon-little clin
humans, suggesting
strated in Table 2, HPLC, microdialysis and FSCV havedopamine. been fundamental in elucidating
how HIV-1 viral protein exposure alters basal DA concentration Another relative
notable to seronegative
inference that can be
individuals or controls. Results (Table 2) overwhelmingly support decreased
cART on DA function DA inconcentra-
HIV-1 seropositiv
tions following chronic HIV-1 viral protein exposure inzidovudine either HIV-1(azidothymidine),
seropositive humans was first im
or biological systems utilized to model HIV-1. Critically, the strong support for decreased
0, x FOR PEER REVIEW Despite the overwhelming support for a hypodopaminergic both the pre- 9state
ofand29 inpost-cART
HIV-1 (i.e.,era.
lowA more co
levels of DA), there are a few outliers. Three studies [174–176] have reported
of cART in dopaminergic10system transitory
Cells 2021, 10, x FOR PEER REVIEW 29 dysfuncti
increases in DA concentration in the CSF, caudate putamenUndoubtedly, and prefrontal cortexof(PFC),
long-term HIV-1 viral p
0, x FOR PEER REVIEW 9 of 29
respectively. The subjects (i.e., humans, mice) evaluated in these studies share a key
independent
1 infection in humans, suggesting little clinical relevance for assessing acute increasesofintreatment with cART. It is p
commonality: early or acute HIV-1. Specifically, the clinical in DAsampleimmediately included individuals
following HIV-1 infectio
dopamine.
0, x FOR PEER REVIEW in clinical stage 1 [174], which is characterized by
Caudateasymptomatic
Nu- infection
9 of 29 and persistent
Another notable inference that can be drawn from Table 2 regards the influence of 1 seropositive individuals [179,180], howe
1 infection in humans, suggesting
generalized little clinical relevance
lymphadenopathy for assessing
[177]. Preclinical acute increases
measurements
cleus were in conducted either
cART on DA function in HIV-1 seropositive individuals. While monotherapy, the currentincludingclinical syndrome.
dopamine. one [176] or three [175] days after the completion of Tat
Globus protein induction by a doxycycline
Palli-
zidovudine (azidothymidine), was first implemented in 1985 [19], cART began in 1996.
Another notable regimen.
Kumar inference Critically,
et al., 2011 that canthese be drawn increases
from in DA 2either
Table regards
dusfailed
the to
Table persist
influence
2. Influence for longer viral
of intervals
Critically,
1 infectionthe strong support
in humans, for decreased
suggesting little dopaminergic
clinical relevance HIVfunction
for assessing spansacuteacross studies
Human
increases in of HIV-1HPLC protein exposu
cART on DA function after[29]
inTat protein
HIV-1 induction
seropositive (i.e.,
individuals.10 Days:
While [178], 40 Days:
monotherapy, trols. [175])
including
Asterisks or(*)were brain
indicate region- that me
manuscripts
both the
dopamine. pre- and post-cART era. A more comprehensive discussion for
Putamen the potential role
specific [176].was
zidovudine (azidothymidine), Moreover, there is no evidence
first implemented for a cART
in 1985 [19], hyperdopaminergic
began in 1996. state during chronic
of cART in dopaminergic
Another notable systemthat
inference dysfunction is presented in Section 5. the influence of
Critically, the strong HIV-1 infection
support in can
for decreased
be drawn
humans, dopaminergic
from Table
suggesting little
function
2 regards
clinical relevance
Substantia
spans across
Symbols: forDAassessing
studies in
concentration acuteisincreases
decreased ( )o
cARTUndoubtedly,
on DA function long-term
in in HIV-1
dopamine.
HIV-1 viral protein
seropositive exposureWhile
individuals. leads to persistent
monotherapy,
Nigra (
DA
)
deficits,
including
indicates no statistically significant diffe
both the pre- and post-cART era. A more comprehensive discussion for the potential role
independent(azidothymidine),
zidovudine of treatment with cART.
Another was first It isimplemented
possible that thatthere
in 1985is an initial
[19], cART transient
Tableincrease
began in 1996. the influence of
of cART in dopaminergic systemnotable
dysfunction inferenceis presented can be
in drawn
Section
Caudate 5.fromtrols.
Puta-
2 regards
in DA immediately
Critically, the strong following
support HIV-1
for infection,
decreased given
dopaminergic the increased
Acute function
Tat life expectancy
spans across for
studies HIV- in
Undoubtedly,cART on DA
long-term function
HIV-1 viral in HIV-1exposure
protein seropositiveleadsindividuals.
to persistent
men While monotherapy,
DA deficits, DA
including
Concentration
1 seropositive individuals
both the pre- and post-cART
zidovudine [179,180],
era. A however,
more
(azidothymidine), the
comprehensive acute phase
Protein
discussionfails to
for accurately
the Mouse
potential reflect
role HPLC
independent of treatment with cART. It is possible was first implemented
that there in 1985increase
is an initial transient [19], cART began in 1996.
References Relative to Con- Viru
thecART
of current clinicalCritically,
in dopaminergicsyndrome.
system
the dysfunction
strong support isfor
presented
decreased in Section
dopaminergic5.
NAc function spans across studies in
in DA immediately following
Kesby HIV-1
et al., 2016 infection, given the increased life
10 of 29 expectancy for HIV- trols
Undoubtedly,both long-term HIV-1
and viral
the [179,180],
[175] pre- proteinera.
post-cART exposure
A more leads to persistentdiscussion
comprehensive DA deficits, for the potential role
1Table
seropositive
2. Influenceindividuals
of HIV-1 viral protein however,
exposure onthe acute
dopamine phase
(DA) fails to Puta-
Caudate
concentration accurately
Larsson
relative etreflect
toal.,con-
1991
independent of treatment
of cART with
in cART.
dopaminergicIt is possible
system that there
dysfunction is an initial
is transient
presented in increase
Section 5. HIV
the current
trols. clinical syndrome. men [16]
in DAAsterisks (*) indicate
immediately manuscripts
following HIV-1 that
Undoubtedly,
measured
infection,
long-term given DAthe
HIV-1
metabolites
Tat increased
Protein
viral
(e.g.,
protein
homovanillic
lifeexposure
expectancy leads
acid).
for
Mouse toHIV-persistent HPLC
DA deficits,
NAc Berger et al., 1994
1Table
seropositive
2. Influenceindividuals
of independent
HIV-1 is [179,180],
viral Caudate however,
Nu-
of treatment
protein onthe
with acuteItphase
cART. is fails that
possible to accurately
there anreflect
is [14]toinitial transient increase HIV
Symbols: DA concentration decreased (exposure dopamine
) or increased ( )(DA) concentration
relative to controls.relative
The equal con-
sign
the current
trols. Asterisksclinical syndrome.
in DA immediatelycleus following HIV-1 infection, given the increased life expectancy for HIV-1
( ) indicates(*)noindicate manuscripts
statistically significantthatdifferences
measured in DADA metabolites (e.g., between
concentration
Caudate homovanillic
Puta- HIV et
Sardar acid).
andal.,con-
1996
seropositive Globus Palli-
individuals [179,180], however, the acute HIV
trols. men phase fails [15] to accurately reflect the
Kumar et al., 2011 Table 2. Influence of HIV-1
current viral protein
dus exposure on dopamine (DA) concentration relative to con-
Symbols: DA concentration HIV isclinical
decreased syndrome.
( ) orHuman
increased (
Acute
)HPLC
relative to controls. The equal sign
Tat Hippocampus
[29] trols.
( Asterisks
) indicates(*)noindicate etmanuscripts
DA Concentration
statistically
Kesby thatdifferences
significant
al., 2016 measured in DADA metabolites (e.g., between
concentration homovanillic
Di Rocco,
HIV andacid).
2000 [17]
con- HIV
Putamen Protein Mouse HPLC
trols. References Relative
Table 2. Influence of HIV-1 viral [178] to Con- Virus Brain Region
protein exposure on dopamine (DA) concentration relative Species Method
to controls. Asterisks (*) indicate
Symbols: DA concentration is decreased ( ) or increased ( PFC
) relative to controls. The equal sign
trols Substantia
(Larsson ) indicates DA Concentration
no statistically significant
et al., 1991 Nigra differences in DA concentration between HIV and con-
manuscripts that measured DA
trols.References metabolites
Relative to Con-(e.g., Virus
homovanillic
HIV acid).
Brain CSF Symbols:
Region HumanDA
OFC
Species concentration
et al.,is2001
HPLC*
Method
Czub decreased ( ) or
[16] SIV
Caudate
trols Puta- [181]
Berger et al., 1994Acute
Horn Tat
et al., 2017
DA Concentration
increased Larsson et al., 1991
( ) relative
[14] to controls.
Protein The equalmen
[186] sign ( HIV ) Mouse
indicates noCSFHIV Human
statistically
HPLC significant HPLC
CSF differences
Humanin DA concentration
HPLC
References Relative to Con- HIV
Virus BrainCSF Human
Region Species HPLC*
Method
betweenSardar
HIV and [16]controls.
Kesby et al., 2016 et al., 1996
Javadi-Paydar trolset al.,
NAc Caudate
HIV-1Nu- Pro- Ex vivo slice volt-
Berger [15]
et al., 1994 HIV HumanNAc HPLCRat
[175] Larsson et al., 1991 2017 [187] HIV cleus
teins
CSF Human Koutsilieri,
HPLC 2002 ammetry
[14] DA ConcentrationCaudate Puta-HIV CSF Pro- Human HPLC* HIV
[16] Denton et al., 2019 HIV-1 [182]
References
Di Rocco,
Sardar et 2000 [17] Relative to men
al., 1996 HIV Virus Caudate CSF Nu-BrainHuman
Region
NAc Species
HPLC*
Rat Method
FSCV
[30]
et al., 1994Tat Protein
Berger [15] Controls HIVMouse HPLC Human Jenuwein
teins HPLC et al., 2004
NAc HIV cleus
CSF Human HPLC SIV
[14] Saloner et al., 2020 [183]
HIV CSF Human HPLC
Larsson etDi Rocco,
al., 1991 2000
[16]
Sardar et al., 1996 [17] [188] HIV HIV CSF
Hippocampus
Caudate Nu- Human
CSF Scheller
HPLC*et al., 2005
Human HPLC *
Caudate Puta-HIV Human HPLC SIV
Czub et al., 2001
[15] cleus [184]
men SIV PFC
[181] Strauss et al., 2020 Acute Tat Primate HPLC
Berger et Di
al.,Rocco,
1994 [14]2000 [17]Acute[176]Tat HippocampusHIVHIV Hippocampus CSF Human Mouse
HPLC* HPLC
Kesby et al., 2016 Protein CSF
PFC Human HPLC
Czub et al., 2001 Protein Mouse HPLC Striatum
[178] PFC SIV Putamen Primate HPLC
[181] Denton et al., 2021 HIV-1 Pro- Kumar et al., 2009
Koutsilieri,
Sardar et al., 1996 [15] 2002 HIV Hippocampus
PFC Caudate NucleusNAc Human
Rat HPLC
FSCV HIV
[189] HIV Striatum
teins Primate HPLC[28]
Czub [182]
et al., 2001 OFC
SIV Putamen Primate HPLC
Jenuwein et al., 2004
[181]
Koutsilieri, SIV NAc Primate HPLC
Horn et al., 2017 [183] 2002 4. HIV-1
HIV ClinicalCSF Symptoms HIVHumanReflect aPFC
Hypodopaminergic
Striatum HPLC Primate State
HPLC
[186] [182]
Scheller et al., 2005 In 2007, the nosology for neurological Putamen complications in HIV-1 seropositive individu-
avadi-Paydar et al., Jenuwein et al., 2004
HIV-1 Pro- SIV Putamen
Ex vivo slicePrimate
volt- HPLC
Ferris et al., 2009
[184]
Koutsilieri, 2002als was updated NAc
to reflectSIV
the Rat
milder NAc
phenotype Primate
of NCI and HPLC alterations, collec-
affective Tat Pro
2017 [187] [183] teins HIV StriatumammetryPrimate [185]
HPLC
[182] tively Caudate Nu-
Denton et al., 2019 Scheller et al., 2005 HIV-1termed
Pro- HIV-1-associated neurocognitive disorders (HAND), Scheller et observed
al., 2010 in the post-cART
trols.
1Table on DA function
seropositive individualsin HIV-1 seropositive
[179,180], however, individuals. While fails
monotherapy, including
both
Symbols:
the
dopamine.
independent
zidovudine
pre- and
2. Influence of
DA concentrationofpost-cART
HIV-1 is
treatment
(azidothymidine), viral
with
era. A more
protein
cART.
decreased
was (exposure
It
first is onthe
comprehensive
possible
)implemented
or increased
acute discussion
dopamine
that
phase
(DA)
( there
in )1985is an
relative
to accurately
for
concentration
initial
the relative
potential
transient
to controls.
[19], cART
reflect
role
into91996.
con-
increase
The equal
began sign
0, x FOR PEER REVIEW of the current
cART
Another in clinical
dopaminergic
notable syndrome.system
inference dysfunction
that can be is
drawn presented
from in
Table Section
2 regards5. the influence of of
29
(trols.
in Asterisks
)
Critically,
1 infectionindicates
DA immediately the (*)noindicate
DA
strongfollowing
in humans,
manuscripts
Concentration
statistically
support HIV-1
for
suggesting
that
significant measured
differences
infection,
decreased
little clinical given DA
in
dopaminergic DAmetabolites
the increased
relevance function
for
(e.g.,
concentration life homovanillic
between HIV
expectancy
spans
assessing across
acute
acid).
and con-
for HIV-
studies
increases in
cART
trols. Undoubtedly,
on DA function
References long-term
in HIV-1
Relative HIV-1
to Con- viral
seropositive protein exposure
Virus individuals.
Brain leads to
WhileSpecies
Region persistent
monotherapy, DA deficits,
including
Method
1Table
both seropositive
the
dopamine. pre- and
2. Influence individuals
ofpost-cART
HIV-1 is [179,180],
viral era. A more
protein however, onthe
comprehensive acute phase
discussionfails to accurately
for the relative
potential reflect
role
independent
Symbols:
zidovudine of treatment
DA concentration
(azidothymidine), with cART.
decreased
trols was (exposure
It
first is possible dopamine
)implemented
or increasedthat in (DA)
( there
)1985is concentration
an
relative initial transient
to controls.
[19], cART began into91996.
con-
increase
The equal sign
0, x FOR PEER REVIEW of the current
cART in clinical
dopaminergic syndrome.system dysfunction is presented in Section 5. of of
29
trols. DAAnother
Cells 2021, 10, (Critically,
in Asterisks
Larsson
12158 ) immediately
indicates
infection et the
al.,
in
notable
strong
1991
humans,
DA inference
(*)noindicate manuscripts
Concentration
statistically
following
support
that that
significant
HIV-1
for
suggesting
can be drawn
measured
differences
infection,
decreased
little clinical given DA
in
dopaminergic
from
DA
the
relevance
Table 2(e.g.,
metabolites
concentration
increased
function
for
regards
life
assessing
the HIV
expectancy
spans
influence
homovanillic
between
across
acute
acid).
and
for
studies
increases con-
HIV-in 9 of 30
cART
trols. Undoubtedly,
on DA function
References long-term to HIV-1
in HIV-1
Relative viral HIV
seropositive
Con- protein
Virus exposure
individuals.
Brain CSF leadsSpecies
While
Region to
Humanpersistent Method
monotherapy, DA
HPLC*deficits,
including
1Table
both seropositive
the
dopamine. pre- and
2. [16]
Influence individuals
ofpost-cART
HIV-1 is [179,180],
viral era. A more
protein however, onthe
comprehensive acute phase
discussionfails to accurately
for the relative
potential reflect
role
independent
Symbols:
zidovudine of treatment
DA concentration
(azidothymidine), with cART.
decreased
trols was (exposure
It
first is possible dopamine
)implemented
or increasedthat in (DA)
( there
)1985is concentration
an
relative initial transient
to controls.
[19], cART began to1996.
con-
increase
The equal
in sign
0, x FOR PEER REVIEW of the current
Berger
cART etin clinical
al., 1994
dopaminergic syndrome.system dysfunction is presented in Section 5. 9 of of
29
trols. DAAnother
(Critically,
in
1Larsson
Asterisks
) immediately
indicates
infection et the
al.,
in
notable
strong
1991
humans,
DA inference
(*)noindicate manuscripts
Concentration
statistically
following
support
that that
significant
HIV-1
for
suggesting
can be drawn
measured
differences
infection,
decreased
little HIV
clinical given DA
in
dopaminergic
from
DA
the
relevanceCSF Table 2Human
metabolites
increased
function
for
regards
(e.g.,
concentration life the HIV
expectancy
spans
assessing
influence
homovanillic
between
across
acute
acid).
and
for
HPLC
studies
increases con-
HIV-in
cART [14]
Undoubtedly,
on DA function
References long-term to HIV-1
in HIV-1
Relative viral HIV
seropositive
Con- protein
Virus exposure
individuals.
Brain CSF leadsSpecies
While
Region to
Humanpersistent Method
monotherapy, DA
HPLC*deficits,
including
trols.
1Table
seropositive individuals [179,180], however,
both the
dopamine.
Sardar
independent
Symbols:
zidovudine
pre-
2. [16]
Influence
et
DA
and
1996 ofpost-cART
HIV-1 is
al.,concentration
of treatment
(azidothymidine), viral
with
era. A more
protein
cART.
decreased
trols was (exposure
It is
first
Tableonthe
comprehensive
possible
)implemented
acute
Cont.
2.dopamine
Caudate
or increasedthat in
phase
discussion
(DA)
Nu-
( there
)1985is an
relative
fails to accurately
for
concentration
initial
the relative
potential
transient
to controls.
[19], cART
reflect
role
to1996.
con-
increase
The equal
began in sign
the
of cART
trols. current
Berger et
Another
Asterisks clinical
al., 1994
in dopaminergic
notable syndrome.system
inference
(*)noindicate manuscriptsthat can
that HIV
dysfunction is presented
be drawn
measured DA from Table
metabolites Human
in Section
2Human
regards
(e.g., 5. the HIV HPLC
influence
homovanillic acid). of
(Critically,
in DA
Larsson) [15]
indicates
immediately
et the
al., strong
1991 DA Concentration
statistically
following
support significant
HIV-1
for decreaseddifferences
infection,
HIV given in
dopaminergic cleus
DA
the
CSFconcentration
increased
function life between
expectancy
spans across and
for
HPLC
studies con-
HIV-in
1 infection [14]
Undoubtedly, in humans, suggesting
DAlong-term
Concentration HIV-1little
viralclinical
protein relevance
exposure for
leadsassessing
to acute DA
persistent increases
deficits,
cART
trols. on
References DA function in
RelativeHIV-1
to Con- HIV
seropositive
Virus individuals.
Brain CSF While
Region Human
monotherapy,
Species HPLC*
including
Method
1
both
References seropositive
the
dopamine.
Di Rocco, pre-
[16] 2000 individuals
andofpost-cART
Relative [179,180],
toera. A morehowever, the
comprehensive
Virus acute phase
discussionfails to accurately
for the relative
Brainconcentration
Region potential reflect
Species role Method
Table
Sardar
independent
Symbols:
0, x FOR PEER REVIEW zidovudine
2. et
Influence
DA of[17] HIV-1
al.,concentration
1996treatment
(azidothymidine), viral
with
is protein
cART.
decreased
trols was first HIV
(exposure
It is on dopamine
possible
)implemented
HIV
or increased CSF
Caudate
that (DA)
in Nu-
( there
)1985is an
relativeHuman
initial
[19],
Human cART HPLC*
transient
to controls. The
began into91996.
con-
increase
equal
HPLC
sign
of of
29
the
of
trols. current
Berger
cART et
Another in
Asterisks
[15] clinical
al., 1994
dopaminergic
notable
(*) syndrome.
Controls
indicate
DA system
inference
manuscripts
Concentration dysfunction
that can
that be is
drawn
measured presented
DA from in
Table
metabolites
cleus Section
2 regards
(e.g., 5. the influence
homovanillic acid).
(Critically,
in DA) immediately
Larsson indicates
et the
al., no statistically
strong
1991 following
support significant
HIV-1
for decreaseddifferences
infection, given in DA
HIVdopaminergic the
CSFconcentration
increased
function life
Human between HIV
expectancy
spans across andHIV-
for
HPLC
studies con-
in
cART on[14]
Undoubtedly,
References DA function long-term to HIV-1
in HIV-1
Relative viral HIV
seropositive
Con- protein
Virus exposure
individuals.
Brain CSF leadsSpecies
While
Region to
Humanpersistent Method
monotherapy, DA
HPLC*deficits,
including
trols.
1 seropositive individuals [179,180], however,
Di Rocco, both
Di
Table the
Rocco,
2000
Sardar
independent
Symbols:
zidovudine 2.[17]
etpre-
[16]
DA 2000
Influence and
[17]ofpost-cART
HIV-1 is
al.,concentration
1996
of treatment
(azidothymidine), viral
with
trols
era. A more
protein
cART.
decreased
was ( It
first HIV
exposure
is) HIVonthe
comprehensive
possible
or
acute
dopamineCSF
Hippocampus
Caudate
increased
implemented that ( in
phase
discussion
(DA)
Nu-
there
) is an
relative
1985
fails
Human to accurately
for
concentration
CSF initial
to
[19],
the relative
potential
HPLC*
transient
controls.
cART The
began Humanreflect
role
to1996.
con-
increase
equal
in sign HPLC *
0, x FOR PEER REVIEW of the
trols. current
Berger
cART etin
Asterisks clinical
al., 1994
dopaminergic
(*) syndrome.
indicate system
manuscripts HIV
dysfunction
that measured is presented
DA in
metabolites Human
Section
(e.g., 5.
homovanillicHPLC 9 of 29
acid).
in Czub
(Critically,
DA ) et
[15]al.,
indicates
immediately
et the 2001 no DA Concentration
statistically
following
strong support significant
HIV-1 differences
infection,
for decreased HIV given in
dopaminergic cleus
DA
the
CSFconcentration
increased life
Human between HIV
expectancy and
for
HPLC con-
HIV-
1Larsson
infection in 1991
al., humans, suggesting little clinical
SIV relevance function
for assessingspansacute
across studies in
increases
trols.
[14]
Undoubtedly,
References
[181] long-term to HIV-1
Con- viral
Relative[179,180], HIVproteinBrain
Virus exposure
CSF leadsPrimate
Region Human
Species
HPLC
to persistent Method
DA
HPLC*deficits,
1Table
both seropositive
the
dopamine.
Di Rocco, pre-
[16]
2. et 2000
Influence individuals
and
[17] post-cART
of HIV-1 isviral era. A
protein however,
more HIV
exposure on the
comprehensive acute
dopamineCSF
Hippocampus
PFC phase
discussion
(DA) fails
Human to
for accurately
concentration
Hippocampus the potential
HPLC*
relative reflect
role
to con-
Sardar
independent
Symbols: DA al.,concentration
1996
of treatment with cART.
decreased
trols ( It is) possible
or Caudate
increasedthat ( Nu-
there
) is an
relative initial
to transient
controls. The increase
equal sign
0, x FOR PEER REVIEW of the
trols. current
Berger
cART et
Another in
Asterisks clinical
al., 1994
dopaminergic
notable
(*) syndrome.system
inference
indicate manuscriptsthat can
that HIV
dysfunction be is
drawn
measured presented
DA from in
Table
metabolites 2Human
Section
regards
(e.g., 5. the HPLC
influence
homovanillic
9 of of
acid).
29
(in Czub
DA ) et
[15]al.,
indicates
immediately 2001 no DA Concentration
statistically
following significant
HIV-1 differences
infection,
HIV given in cleus
DA
the
CSFconcentration
increased life
Human between HIV
expectancy and
for
HPLC con-
HIV-
1Larsson
infection et
[14] in
al., humans,
1991 suggesting little clinical
SIV relevance
Putamen for assessing
Primate acute increases
HPLC in
cART
trols. Undoubtedly,
on
References
[181] DA function long-term
Relative to HIV-1
in HIV-1 Con- viral
seropositive
HIVprotein
Virus exposure
individuals.
Brain CSF leadsSpecies
While
Region to persistent Method
monotherapy,
Human DA deficits,
including
HPLC*
Czub et al., 1Table
seropositive
dopamine.
Di Rocco,
2001 2. [16]
Koutsilieri,
[181]2000
Influence 2002individuals
[17]of HIV-1 [179,180],
viral protein however,
HIV
exposure on the acute
dopamineCSF
Hippocampus phase
(DA) fails to accurately
Human
concentration HPLC*
relative reflect
0, x FOR PEER REVIEW zidovudine
Sardar
independent
Symbols: et
DA al., 1996
of treatment
concentration
(azidothymidine), with
is cART.
decreased ( It
trols was first HIV is) orSIV
possible
increased
implemented
HIV thatPFC
Caudate
( Nu-
there
) is PFC
an
relative
in 1985 [19],
Striatum initial
to transient
controls.
cART began
Primate
Human
The into91996.
Primate
equal
HPLC
HPLC
con-
increase
sign
of of
29
HPLC
the current
Berger et
Another
[182] clinical
al., 1994
notable syndrome.
inference that can be drawn from Table 2 regards the influence
(trols.
in CzubAsterisks
)
Critically,
1Larsson
infectionet
[15]
etal.,
indicates
DA immediately the
in
al.,
(*)
2001 noindicate
strong
humans,
1991 DA manuscripts
Concentration
statistically
following
support for
suggesting
that
significant
HIV-1
decreased
little
measured
differences
infection,
HIV
clinical
SIV given DA
in
dopaminergic metabolites
cleus
DA
the increased
relevanceCSF function
for
(e.g.,
concentration life
Human
assessing
Primate
homovanillic
between HIV
expectancy
spans across
acute
acid).
and con-
for HIV-
HPLC
studies
increases
HPLC in
cART on[14] DA Putamen
al.,function in HIV-1 seropositive
HIV individuals. CSF WhileSpecies
monotherapy,
Human including
HPLC*
1Jenuwein
trols.
both References
the
dopamine.
Di
Table 2.
[181]
seropositive
[16]
Koutsilieri,
Rocco,
et
pre-
2000
Influence
2004 Relative
2002individuals
and
[17]ofpost-cART
HIV-1
to Con-
[179,180],
viral era. A more
protein
Virus
however,
SIV
HIV
exposure on
Brain
the
comprehensive acute
NAc
dopamine
Region
CSF
Hippocampus phase
discussion
(DA) fails for
Primate
Human
concentration
Method
to accurately
HPLCreflect
the relative
potential
HPLC* role
Sardar
Symbols:
zidovudine et
DA al., 1996
concentration
[183] (azidothymidine), is decreased (
trols was first HIV ) or increased
implemented
HIV
PFC
Caudate
( Nu-
) Putamen
relative
in 1985 [19],
Striatum to controls.
cART
Primate
Human
The
began into1996.
equal
HPLC
HPLC
con-
sign
the
of current
cART
Berger et
Another in
[182] clinical
dopaminergic
al., 1994
notable syndrome.system
inference dysfunction
that can be is
drawn presented
from in
Table Section
2 regards5. the influence of
(trols.CzubAsterisks
)
Critically,
1Scheller
infection
Larsson et
[15]al.,
indicates
et the
al.,
(*)noindicate
2001 DA
strong support
in 2005
humans,
1991
manuscripts
Concentration
statistically thatdifferences
significant
for decreased
suggesting little
measured
HIV DA
in
dopaminergic
clinical
SIV relevance
metabolites
cleus
DACSF function
for
(e.g.,
concentration
Human homovanillic
between
spansacute
assessing
Primate HIV
across HPLCacid).
and
increases
HPLC con-
studies in
cART on[14]
Undoubtedly,
DA long-term HIV-1 viral SIVprotein Putamen
exposure
Putamen leads to persistent
Primate DAHPLCdeficits,
Jenuwein
trols. References
[181]
[184]et al.,function in HIV-1
2004 Relative to Con-seropositive
Virus individuals.
HIV CSF
Brain Region WhileSpecies
monotherapy,
Human including
HPLC*
Method
both the
dopamine.
Di pre-
[16]
Koutsilieri,
Rocco, 2000 andofpost-cART
2002 era. A more SIVcomprehensive NAc discussionPrimatefor the relative
potential
HPLC role
Koutsilieri, Table2002
Sardar
independent
Symbols:
zidovudine 2.[183]
Influence
[182]
et
DA of[17] HIV-1 is
al.,concentration
1996treatment
(azidothymidine), viral
with
trols protein
cART.
decreased
was first HIV
(exposure
It is
HIV
HIV
orHIVon dopamine
possible
)implemented
increasedthat CSF
Hippocampus
PFC
Caudate (DA)
Nu-
( there
in
Striatum )1985is an
relativeHuman
concentration
Striatum
initial
[19], cART
Primate
Human
HPLC*
transient
to controls. The
began into1996.
Primate con-
increase
equal
HPLC
HPLC
sign HPLC
of cART
Berger etin dopaminergic
al., 1994 system dysfunction is Caudate
presented Nu-
in Section 5.
trols.
in DAAnother
Czub
(Critically,
Scheller
Larsson
[182]
Asterisks
et etal.,
[15]
) immediately
indicatesthe
al.,
notable
2001
strong
2005
1991 DA inference
(*)noindicate manuscripts
Concentration
statistically
following
support
that that
significant
HIV-1
for
can be drawn
measured
differences
infection,
decreased HIV
SIV given DA
in
dopaminergic
from
DA
the
CSF Table 2Human
metabolites
cleus
concentration
increased
function
regards
(e.g.,
life the HIV
between
expectancy
spans
influence
homovanillic
across acid).
and
for
HPLC
studies
of
con-
HIV-in
cART
Jenuwein
trols. on[14]
Undoubtedly,
References
[181] DA
et al., function
2004 long-term
in
RelativeHIV-1
to HIV-1 viral SIV
seropositive
Con- HIVprotein
Virus
Putamen
individuals.
Brain cleus
exposure
Putamen
CSF leadsPrimate
While
Region to
monotherapy,
Human
Species
HPLC
persistent Method
Primate DAHPLCdeficits,
including
HPLC*
1
both
Diseropositive
the [184]
pre-
[16]
Koutsilieri,
Rocco, 2000 2002individuals
and post-cART [179,180],
era. A however,
more SIV the
comprehensive acute
NAc phase
discussionfails
Primate to
for accurately
the potential
HPLC reflect
role
Jenuwein et al.,
Symbols: 2004
Sardar
independent
zidovudine [183][183]
etDA of[17]
al.,concentration
1996treatmentis
(azidothymidine), with cART.
decreased
trols was first HIV
( It is orSIV
possible
)implemented
HIV
HIV
Globus
increased CSF
Hippocampus
PFC
Caudate
that inPalli-
Nu-
( there
Striatum )1985is an
relativeHuman
NAc initial
[19], cART
Primate
Human
HPLC*
transient
to controls. The
began Primate
increase
equal
HPLC
HPLC
sign
in 1996. HPLC
the
of current
cART
Berger
Czub
Kumar etin
[182]
etet
[15]
clinical
dopaminergic
al.,
al.,
al., 1994
2001
2009 syndrome.
DA system
Concentration dysfunction is Caudate
presented
dus
cleus
Nu-
in Section 5.
(Critically,
in DA) immediately
Scheller
Larsson indicates
et the
al., no statistically
strong
2005
1991 following
support significant
HIV-1
for decreaseddifferences
infection,
HIV
SIV given in
dopaminergic DA
the
CSFconcentration
increased
function life
Human between
spans HIV
expectancy
across and
for
HPLC
studies con-
HIV-in
Jenuwein
trols.
[14]
Undoubtedly,
References
[181]
[28]et al., 2004 long-term to HIV-1
Con- viral
Relative[179,180],
HIV
SIV
HIVproteinBrain
Virus
Putamen
cleus
exposure
Putamen
CSF leadsPrimate
Region
Human
Primate
Human
Species
HPLC
to persistent Method
DAHPLC
HPLC*deficits,
1
both seropositive
the [184]
pre-
[16]
Koutsilieri, individuals
and post-cART era. A however,
more the
comprehensive
SIVSIV acute
NAc
Putamen phase
discussionfails
Primate to
for accurately
the potential
HPLC reflect
role
Di
Table
Scheller etindependent
al.,Rocco,
Sardar 2.[183]
2005 et al.,2002
2000
Influence
[184] of[17]
1996 of HIV-1 viral
treatment withprotein
trols cART.exposureHIV
It is
HIV
on dopamine
possible that CSF
Hippocampus
PFC
Globus
Caudate (DA)
Palli-
Nu-
there
Striatum
Human
concentration
Putamen
is an initial transient
Primate
HPLC*
relative to con-
Primate
increase
HPLC
HPLC
the
ofKumar current
cART
Berger
trols. etin
[182]
Asterisks clinical
dopaminergic
al., 1994
(*) syndrome.
indicate system
manuscripts that HIV
dysfunction
measured is Caudate
presented
DA Nu-
in
metabolites Human
Section
(e.g., 5.
homovanillicHPLCacid).
in Czub etet
[15]al.,
DA immediately
Scheller
Larsson al., 2001
2009 DA Concentration
1991 following HIV-1 infection,
et al., 2005 HIV given dus
cleus
the
CSFincreased life expectancy
Human for HIV-
HPLC
SIV Substantia
[14]
Undoubtedly, long-term to HIV-1
Con- viral
HIV
SIV
HIVproteinBrain Putamen
cleus
exposure
Putamen
CSF leadsPrimate
Human HPLC
to persistent Method
Primate
Human DAHPLC
HPLC*deficits,
1Jenuwein
Di
References
[181]
[28]
seropositive
[184]
[16]
Koutsilieri,
Rocco,
et al., 2004
2000 2002
Relative[179,180],
individuals Virus
however, the
SIV on dopamine acuteRegion
Nigra
NAc
Putamen phase Species
fails
Primate to accurately
HPLCreflect
Table
Sardar
independent
Symbols: 2.[183]
Influence
et
DA of[17]of HIV-1 is
al.,concentration
1996treatment viral
with protein
decreased
trols HIV
cART.(exposure
It is)
HIV
HIV
possible
or increasedthat CSF
Hippocampus
PFC
Globus
Caudate
( (DA)
Caudate
Palli-
Nu-
there
Striatum ) is an
relativeHuman
concentration
Nucleus
initial
to HPLC*
relative
transient
controls.
Primate
Human
The to con-
increase
equal
HPLC
HPLC
sign
0, x FOR PEER REVIEW trols. the current
Berger
Ferris
Czub
Kumar etet
et
[182]
Asterisks
et
[15]al., clinical
al.,
al.,
al., 1994
2009
(*)
2001
2009 syndrome.
indicate manuscripts that measured Caudate
DA Nu-
metabolites
dus
cleus (e.g., homovanillic 10 of 29
acid).
(in DA )
Scheller indicates
immediately
et
Larsson[14] 1991 al., no
2005 statistically
following significant
HIV-1 Tatdifferences
infection,
HIV
Protein given in DA
the
CSFconcentration
increased
Striatum
Substantia life
Human
Rat between HIV
expectancy and
for
HPLC
Microdialysis con-
HIV-
[185] SIV
HIV
SIV
HIV Putamen
cleus
Putamen
CSF Primate
Human
Primate
Human HPLC
HPLC
HPLC*
1Jenuwein
trols.
Di
Table Rocco,
2.
[181]
[28]
seropositive
[184]
[16]
Koutsilieri,
et al., 2004
2000
Influence 2002individuals
[17]of HIV-1 [179,180],
viral protein however,
SIV
HIV
exposure on the acute
Nigra
NAc
Putamen
dopamineCSF
Hippocampus
PFC
Globus
phase
(DA)
Globus fails
Primate
Human to accurately
concentration
Pallidus HPLC
HPLC*
relative reflect
to con-
Sardar[183]
Scheller
Symbols: et
et
DA al., 1996
al.,concentration
2010 is decreased ( HIV ) or increased ( Palli-
Caudate
Striatum Nu-
) relative to controls. The
Primate equal
HPLC sign
the current
Berger
Ferris
trols. et
et
[182]
Asterisks al.,clinical
al., 1994
2009
(*) syndrome.
indicate manuscripts that HIV
Early HIV
measured DA CSF
Caudate Nu-
metabolites Human
(e.g., homovanillicHPLCacid).
( Czub
Kumar ) etet
[15]
[174]al.,
al.,
indicates 2001
2009no DA Concentration
statistically significantTatdifferences
HIV
Protein in DAdus
cleus
CSFconcentration
Striatum Human
Rat between HIV and
HPLC
Microdialysis con-
Kumar et Scheller al., 2009[14]et
[28]al., 2005 SIV
HIV HIV Caudate
Substantia
Putamen
cleus Nu- Primate
Human Human
HPLC HPLC
Jenuwein
trols. [185]
References
[181]
[28]et al., 2004 Relative to Con- SIV
Virus Putamen
Brain Region Primate
Species HPLC
Method
Di
Table Rocco,[184]
Koutsilieri,
2.[183] 2000
Influence 2002
[17] SIV
HIV Nigra
NAc
cleus
Putamen
CSF Primate
Human HPLC
HPLC*
Sardar
Scheller
Symbols: et
et
DA al., 2010of HIV-1 is
1996
al.,concentration viral protein (exposure
decreased
trols on dopamine
Hippocampus
PFC
Globus
Caudate
) or increased
HIV Striatum )(DA)
( Palli-
Nu- concentration
Putamen
relative to controls.relative
The to con-
equal sign
Ferris
trols.Czub et
[182]
Asterisks
et al.,
al., 2009
(*)noindicate
2001 DA manuscripts
Concentration that HIV
Early HIV Caudate
measured Globus
DADA CSF Nu- Primate
Palli-
metabolites
dus
Human
(e.g., between
homovanillic
HPLC
HPLCacid).
Kumar
(Scheller ) et
[15]
[174] al.,
indicates
Larsson et al., 2005 2009
1991 statistically significant differences
Tat HIV
Protein in cleus
concentration
Striatum Rat HIV and
Microdialysis con-
[185] SIV Substantia
Putamen
cleus Primate
Human HPLC
Kumar
Jenuwein
trols. etetal.,
References
[181]
[28] al.,2011
2004 Relative to Con- SIV
HIV
Virus Putamen
Brain Region Primate
CSF
dus Human
Species HPLC
HPLC*
Method
Di Rocco,[184]
[16]
Koutsilieri, 2000 2002
[17] HIV
SIV
HIV Nigra
NAc
Putamen
CSF
Hippocampus SubstantiaHuman
Primate
Human HPLC
HPLC*
Scheller
Symbols: et
DA
[29]
[183] al.,concentration
2010 is decreased ( HIV
trols ) or increased PFC
Globus( Palli-
Striatum ) relative toNigra
controls. The equal sign
Berger
Ferris
Czub et
et
[182]
et al.,
al.,
al., 1994
2009
2001 DA Concentration Early HIV Caudate CSF Nu- Primate
Putamen Human HPLC
HPLC
Kumar
(Scheller ) et
[174]
Larsson[14] al.,
indicates 2009
et al., 2005 no
1991 statistically significant differences
HIV
Tat HIV
Protein in DAdus
CSFconcentration
Striatum Human
Rat between HIV and con-
HPLC
Microdialysis
[185] SIV Substantia
Putamen
cleus Primate
Human HPLC
Jenuwein
trols. References
[181]
[28]et al., 2004 Relative to Con- SIV
HIV
Virus Putamen
Brain CSF
Region Primate
Human
Species HPLC
HPLC*
Method
[184]
[16]
Koutsilieri, SIVProtein Substantia
Nigra
NAc
Putamen Primate HPLC
Ferris et al., 2009[183]
Sardar
Scheller [185]
et al.,2002
etal., 1996
2010 trols Tat
HIV
Hippocampus
Caudate
Striatum Nu- Striatum
PFCPalli-
Globus
Primate HPLC
Rat Microdialysis
Berger
Ferris et
et
[182] al.,
al., 1994
2009 Early HIV Nigra
CSF
Caudate Nu- Human HPLC
Czub
Kumar
Scheller etet
[15]
[174]
Larsson[14] al.,
al., 2001
2009
et al., 2005
1991 DA Concentration HIV
Tat HIV
Protein dus
cleus
CSF
Striatum Human
Rat HPLC
Microdialysis
[185] SIV Substantia
Putamen
cleus Primate
Human HPLC
Jenuwein
References
[181]
[28]et al., 2004 Relative to Con- SIV
HIV
Virus Putamen
Brain
Caudate CSF Puta- Primate
Region Human
Species HPLC
HPLC*
Method
[184]
[16]
Koutsilieri, Acute
SIV Tat Nigra
NAc
Putamen Primate HPLC
Scheller et Di al.,Rocco,
2010
Sardar
Scheller [174]
et
et
[183] al.,2002
2000
al., [17]
1996
2010 trols HIV
Early HIVCaudate
HIV
CSFPalli-
PFC
Globus
men
Striatum Nu- CSF Human HPLC*
Human HPLC
Berger et
Ferris [182]
et al.,
al., 1994
2009 Early
ProteinHIV Caudate CSF Nu- PrimateHuman
Mouse HPLC
HPLC
Kumar
Larsson[174]
Scheller et
[15] al., 2009
et al., 2005
1991 HIV
Tat HIV
Protein dus
cleus
CSF
Striatum Human
Rat HPLC
Microdialysis
[14]
[185] Substantia
Putamen
cleus Human HPLC
Jenuwein [28]etal.,
al.,2016
2004 SIV
HIV Putamen
CSF
NAc Primate
Human HPLC
HPLC*
Kesby
Di Rocco, et
[184]
[16]
Koutsilieri, 2000 2002
[17] SIV
HIV Nigra
NAc
Putamen
CSF
Hippocampus Caudate Primate
Human
Nucleus HPLC
HPLC*
Sardar et
Scheller[183] al., 1996
et al., 2010 Globus
Caudate Palli-
Nu-
[175] HIV
Early HIV Caudate Striatum
CSFPuta-
Caudate Primate
Human HPLC
HPLC
Berger
Ferris
Czub [182]
Kumar
Scheller etet
et
et
[174]
al.,
al.,
etal.,
[15] al., 1994
2009
al.,2001
2009
2005 HIV
Tat HIV
Protein dus Nu- Human
cleus
CSF
Striatum Rat HPLC
Microdialysis
[14]
[185] SIV Substantia
cleus Primate
Human HPLC
Jenuwein [181]
[28]et al., 2004 SIV Putamen
men Primate HPLC
Di Rocco,[184] Tat Protein
SIV Nigra
NAc
Putamen Mouse
GlobusPrimate HPLC
Sardar
Scheller et2000
et
[183] al., [17]
al.,1996
2010 HIV CSFPalli-
Hippocampus
PFC
Globus
Caudate
NAc Nu- Human
Pallidus HPLC*
Ferris et al., 2009 HIV
Early HIV CSF
Caudate Nu- Human HPLC
Kumar et Scheller Czub
Kumar
al., 2011 etet
[15]
[174]
etal.,
[29]al.,2001
al., 2009
2005 Tat HIV
Protein dus
cleus
Striatum Rat Microdialysis
SIV HIV Substantia
Putamen
cleus Primate
Human Human
HPLC HPLC
[185]
[181]
[28] SIV Putamen Primate HPLC
Di Rocco,[184]
Koutsilieri, 2000 2002
[17] HIV Caudate
Nigra
Putamen
CSF
Hippocampus Puta- Human
Putamen HPLC*
Scheller et al., 2010 PFC
Globus Palli-
HIV
Early HIV Caudate Striatum
CSF Nu- Primate
men Human HPLC
HPLC
Ferris
Kumar et
Czub [182]
et al.,
etal.,
[174] 2009
al.,2001
2009 dus
Tat HIV
Protein
SIV Striatum
Substantia
Putamen Rat
Primate
Human Microdialysis
HPLC
Jenuwein [185]
[181]et al., 2004 Acute Tat Hippocampus cleus
Kesby [28]
et al.,2002 2016
Koutsilieri, SIV NAc
Nigra
Putamen
Hippocampus Substantia
PFCPalli-
Globus Primate
Nigra HPLC
Scheller et al., 2010
[183] Protein
HIV Striatum Mouse
Primate HPLC
HPLC
Ferris
Czub [178]
et
[182]
et al.,
al., 2009
2001 Early HIV CSF
PFC Human HPLC
Kumar et
[174] al.,
Scheller et al., 2005 2009 Tat HIV
Protein dus
Striatum Rat Microdialysis
[185] SIV
SIV Substantia
Putamen
Putamen Primate
Human
Primate HPLC
HPLC
Jenuwein [181]
[28]
[184]et al., 2004
Koutsilieri, 2002 SIV NAc
Nigra
Putamen
PFC Primate HPLC
Scheller[183]et al., 2010 HIV OFC
Striatum
Ferris [182]
et al., 2009 Early HIV Caudate CSF Nu- PrimateHuman HPLC
HPLC
[174]
Scheller et al., 2005 Tat Protein Striatum
Substantia
Putamen Rat Microdialysis
Horn [185]
Jenuwein et etal.,al.,
2017
2004 SIV cleus
Putamen Primate HPLC
[184]
Koutsilieri, 2002 HIV
SIV CSF
NAc
Nigra Human
Primate HPLC
Scheller [186]
et
[183] al., 2010 Globus Palli-
HIV HIV Caudate Striatum Primate HPLC
Ferris [182]
Kumar
Scheller
et
et al., 2009
et al.,
[174]
Javadi-Paydar al., 2009
et al.,
2005
Early
HIV-1
Tat Pro-
Protein dus Nu- Human
CSF
Striatum Rat Ex vivo
HPLC
slice volt-
Microdialysis
[185] HIV
SIV cleus
NAc
Putamen Human
Rat
Primate HPLC
HPLC
Jenuwein2017 [28]
[184]et al.,
[187] 2004 teins ammetry
SIV NAcPalli- Primate
Putamen
Globus HPLC
Scheller[183]et al., 2010
Denton et al., 2019 HIV-1
Early HIVPro- Caudate CSF Nu- Human HPLC
Kumar[174]
Scheller et
et al.,
al., 2009
2005 dus
NAc Rat FSCV
[30] HIV
teins Substantia
cleus Human HPLC
[28] SIV Putamen Primate HPLC
Saloner[184] et al., 2020 Nigra
Putamen
Globus Palli-
HIV CSF Nu- Human
Caudate HPLC
Ferris
Kumar[188] et al., 2009
et al., 2009 dus
Tat HIV
Protein Striatum
Substantia Rat
Human Microdialysis
HPLCYou can also read