Healthcare Insights - Simon-Kucher
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Healthcare Insights
A publication for the clients of Simon-Kucher & Partners
2020 - Volume 12, Issue 1
Colourbox/-
INSIDE THIS ISSUE
◃
Comprehensive commercial alignment: the key to brand forecast accuracy
Actual sales miss the revenue forecast by an average of 50 percent – an alarming number.
What can pharmaceutical companies do to achieve their desired commercial performance
and improve forecast accuracy?
Account for ATU status in France when building your local and European
P&MA strategy
The Temporary Authorization for Use (ATU) program allows manufacturers to generate revenue even
before a drug is officially launched. However, the program is undergoing significant changes in France –
particularly in terms of eligibility criteria. How should companies effectively integrate ATU in a European
P&MA strategy?
Key account management: tackling the challenges of a dynamic
pharma market
The market environment for pharmaceutical companies is constantly changing, requiring a new approach
to key account management. What are the key measures to make use of revenue potential and drive
growth by improving KAM?
and more...
CONTENTS
P&R BRIEFS
USA 07
France 07
Spain 08
Switzerland 10
UK 11
Japan 12
China 12
Brazil 13
FEATURES
15
Comprehensive commercial alignment
Account for ATU status in France 22
Key account management 29
Introducing our new colleagues 34
About Simon-Kucher & Partners 36
SIMON-KUCHER & PARTNERS
EXECUTIVE EDITOR ARTICLE CONTRIBUTORS Rebecca Ford DISTRIBUTION
Nathan Swilling Diane Cosset Gabriela Honda Prerna Kakkar
Jonathan Haugen Patricia Lavina Oksana Prysiazhniuk
ASSOCIATE EDITORS Nick Keppeler Hugo Li Bettina Liesenfeld
Christopher Barr Clementine Legros Manuela Martin Rachel Pope
Emily Choate Lilia Meddeb Mia Marrazza Goekce Muege Cil
Madhurima Das Jens-Christian Oelker Josselin Meylan
Mia Marrazza Raf Onclin Ana Mozetic Bonn Office
Ryan Murphy Willy-Brandt-Allee 13
Tyler Perez Jens Mueller
Eric Wan 53113 Bonn, Germany
Jeremy Winkler Mathilde Pereira
Fangting Yu +49 22 8984 30
Lais Schoenacker
P&R BRIEFS CONTRIBUTORS Robert Spieker
GRAPHIC DESIGN Boston Office
Fan Chen Mariana Torgal
Genevieve Solomon One Boston Place
Inigo Cubillo Alice Tregrossi Suite 3301
Nicole Peterson
Madhurima Das Na Wei Boston, MA 02108
Judith Flecke Chris Wu +1 617 231 4500
Callum Foden Fangting Yu
Please send inquiries to:
LSCommunications@simon-kucher.com www.simon-kucher.com
Annual European Medical Technology Strategy Forum Advanced revenue models for profitable growth: Monetizing value in a new era Radisson Blu Zurich Airport, Switzerland, February 11, 2020 The MedTech industry has traditionally always experienced successful growth largely driven by a continuous launch of new innovations. Yet, constrained budgets on payer and provider sides has led to a decrease in willingness to pay and acceptance of good enough products. This growth gap, coupled with increased expectations from the investor community, has forced many MedTech companies to rethink their revenue models and find new avenues for profitable growth. Best-in-class companies have started to develop and extract value beyond the core product portfolio. Some have even taken the step of redefining themselves from product to solutions providers. Common among them is that they redesign their revenue model to de- liver unparalleled value to the customer by solving a clinical and/or economic need. These include, among others, enhancing value add services, monetizing integrated digital solutions, establishing win-win contracting models or forward integrating to care delivery. Join us for the Simon-Kucher & Partners European Medical Technology Strategy Forum in Zurich, where industry representatives and experts from Simon-Kucher & Partners will share insights, practical approaches and best practice examples on new revenue models through monetizing beyond the core. Attending the forum will provide you with valuable insights on: Current trends and challenges in the MedTech space Industry best practices on new revenue models Practical approaches on how to monetize beyond the core Successful implementation of new revenue models Industry Experts Michael Erdtmann Mike Genau Dr. Cosmin Bordea Michael Fetahi Laursen Judy Han Senior Director Sales SVP Managing Director VP, Head of BD Senior Regional Manager Consultant EMEA SPI Germany EMEA Global Sales Excellence Healthcare consulting Johnson & Johnson Medtronic Fresenius Medical Care WS Audiology Roche Diagnostics Simon-Kucher & Partners Joerg Kruetten Dr. Gerald Schnell Omar Ahmad Raf Onclin Jan Bordon Global Head of Health Senior Partner Managing Partner Partner Senior Director care and Life Sciences Simon-Kucher & Partners Simon-Kucher & Partners is a global consulting firm with more than 1,400 professionals in 39 offices worldwide focusing on TopLine Power®. Founded in 1985, the company has more than 30 years of experience providing strategy and marketing consulting and is regarded as the world’s leading pricing advisor. To find out more, go to www.simon-kucher.com www.simon-kucher.com

Your Market Access and
Pricing (MAP) function
plays a pivotal role in a
product’s success.
Is your organization set
up to seize opportunities
and face challenges?
Are you meeting all the
requirements to future-
proof the MAP
organization to ensure
success?
iStock/alex skp
Market Access Excellence
(MAXX) Scorecard:
A self-assessment for Simon-Kucher’s clients
Take Simon-Kucher MAXX survey to get immediate
results on how your MAP function compares to best
in class benchmarks with a performance score and
areas for improvement.
Survey link:
www.simon-kucher.com/en/market-access-excellence-scorecard/intro
For additional questions, please reach out to:
Stephan Schurz: stephan.schurz@simon-kucher.com
Fangting Yu: fangting.yu@simon-kucher.com
YOUR ROADMAP TO PROFITABLE GROWTH
June 23–24, 2020
Amsterdam, Beurs van Berlage
www.topline2020.com
#TopLine2020
Contact us:
TopLine2020@simon-kucher.com
+49 228 9843 335
Check out our video and get a glimpse of what’s to come!
Unique
keynotes
About TopLine 2020
In-depth TopLine 2020 deep-dives into the drivers of top-line growth, such as
case marketing, pricing, sales, digital strategies, and business models. Through
panel discussions, master classes, hands-on roundtable sessions, and
studies keynotes, this two-day conference will unveil growth opportunities for all
types of enterprises. Don’t worry, there will be plenty of time for networking
in our industry lounge or during the boat ride to the exclusive networking
dinner!
Be inspired
by keynote and panel discussions, multi-dimensional sessions,
exclusive one-on-one meetings, and master classes
Discover
new trends, methods, and insights that have never
before been released to the public
Experience
first-hand how the most brilliant minds in business have
grown their top lines
Why should I attend?
This two-day conference is designed for those who want to ensure
sustainable profits and satisfied customers in a digital world. If you’re in a
role that focuses on growth strategies, marketing, product development,
pricing, or sales, you can’t miss TopLine 2020!
Interactive
sessions
Exclusive
industry
lounge
P&R briefs: Recent developments in global
pricing & market access
USA targets the top 125 drugs by spend it is unlikely to impact
newly launched products. Knowing that a significant price
CMS drug price negotiation:
reduction may be in the future once the sales build up to
Is it truly a negotiation? a certain threshold, would manufacturers launch at even
The House Democratic leadership is pushing forward higher prices in anticipation of the effect of this bill on the
with a proposed plan to reduce drug prices: the Lower future prices of their products? How will this impact their
Drug Costs Now Act of 2019,a released on September international pricing strategies? ▵
19th, 2019. This bill includes the establishment of several
programs and requirements, primarily aiming to limit the
prices of top-spending drugs. One of the key programs France
proposed by this bill is the Center for Medicare and Med-
icaid Services (CMS) negotiation of maximum prices for Changes to nATU program
certain drugs, which is currently prohibited by law. Un- Over the years, the ATU program in France has become
der this program, the CMS must negotiate the maximum one of the key considerations for a manufacturer’s EU P&R
prices for insulin products and at least 25 single source, strategy. In an evolving P&R environment, where the path
brand name drugs that do not have generic competi- to market access can be long and complicated, ATU sta-
tion that are among the 125 drugs that accounts for the tus granted by the French National Agency for Medicines
greatest national spending or greatest spending under and Health Products Safety (ANSM) provides rapid access
Medicare Part D and Medicare Advantage. The US prices opportunities for drugs without a marketing authorization
would be tied to six international markets: Canada, Aus- or those undergoing P&R negotiations. Only drugs that
tralia, the UK, Japan, Germany, and France. The negoti- target serious or rare indications without available appro-
ated US price should not exceed 120% of the weighted priate treatment alternatives and presumed efficacy and
average price, i.e., average international market price (AIM safety data can benefit from the ATU program. Besides
price), across these six countries and should target at the obtaining a rapid market access, the ATU program also
lowest net average price in any one of the six countries. enables a manufacturer to set the drug price freely. This
The penalty for not reaching a price agreement with the generates substantial strategic appeal for manufacturers,
CMS within a defined period of time would be additional considering the international price referencing implica-
tax that starts at 65% of sales in the US for the drug in ne- tions across EU and the potential for early revenue.
gotiation and rises by 10% for every three non-compliant
months until the excise tax reaches 95% of its US sales. Typically, two types of ATU can be granted: nominative
ATU (nATU) or cohort ATU (cATU). While nATU is pa-
If enacted, this bill would essentially force the drug man-
tient-specific and granted at the request of individual phy-
ufacturers into price agreement with the CMS, with a like-
sicians, cATU is designated for a group of patients at the
ly much lower price tag for the US, possibly lower than
request of the drug manufacturer. The requirements and
the AIM price, unless that price is lower than 95% of the
eligibility criteria differ slightly between the two, with cATU
current US price. Further analyses need to be conducted
being somewhat more restrictive.
to understand the true impact of this bill. For example,
the negotiation-eligible drugs only include single source With the growing strategic importance of ATU status, both
drugs. However, this may exclude some brand name the number of drugs granted ATU and their prices have
medicines that have generic competition but the prices risen, leading to a significant budget impact with costs ex-
are not impacted in a significant way. As the proposed bill ceeding >€1B per year for the French healthcare system.
In an effort to offset the burden and continue this program
a
https://www.congress.gov/bill/116th-congress/house-bill/3
Simon-Kucher & Partners Healthcare Insights | Recent Developments in Global Pricing & Market Access 7
sustainably, the French authorities have been slowly intro-
ducing initiatives to reform the program. In its most recent Spain
iteration, French Social Security Law (LFSS) for 2020 im-
The Spanish Ministry of Health has
plemented two new changes for the nATU program:
published an action plan to promote
1. Additional monitoring mechanisms / conditions: the use of generics and biosimilars
Stricter eligibility criteria have been rolled out for The key priorities and work streams of the Spanish Minis-
nATU, mirroring requirements for cATU status. For ex- try of Health are uncertain, due to current political instabil-
ample, nATU will now require drug safety and efficacy ity in Spain. With four general elections and four different
to be “strongly presumed” (instead of “presumed to Ministries of Health in the last years, the Spanish Health-
be favorable”) and the clinical trial to be “ongoing” in care System has needed to adapt to the changing political
France (instead of “ongoing or submitted”). Addition- environment.
ally, the number of nATUs authorized per product will
now be capped. However, having a sustainable Healthcare System remains
a key priority for the Ministry of Health. In this context, the
2. Repeal of “free pricing” for nATU: The Ministry of Ministry has proposed an Action Plan to promote the use
Health will now determine the compensation rates of generic and biosimilar drugs. This is expected to lead
for nATU drugs rather than the manufacturer, but this to an increase in competition among manufacturers and
price is not expected to be published. Manufacturers eventually reduce pharmaceutical expenditure.
should still be able to freely set the price charged to
hospitals, but will have to pay back the difference ver- The key measures proposed in the Plan are the following:
sus the compensation amount set by the MoH (free
Actions related to P&R setting of generic and biosimilar
pricing will still apply for drugs with cATU status).
drugs:
The nATU program serves more than 2.5 times the 1. Voluntary discounts within the Fixed Reference
patients in cATU program. The high prices set by the Price (FRP) System: Products within the same
recent nATU drugs propelled the above changes, reference group will no longer be required to have
which may now impact P&R negotiations in France. the same price. Upon creation of the group, all prod-
It remains to be seen if the French ATU program can ucts (originator and generics/biosimilars) will need
preserve its strategic appeal. to have the same price (reference price), but after-
wards, manufacturers can offer discounts. These
For an in-depth overview of recent ATU changes
voluntary discounts will not be considered for the
and its implications, please refer to page 22 of this
reference price recalculation the next year.
issue. ▵
2. Dynamic prices: Price of the drugs within an FRP
group will be re-negotiated based on volume of
original and biosimilar sales vs. the total sales of the
active substancea.
3. Reference groups by ATC-4: The Plan would
create reference price groups based on ATC-4
drug classification (i.e., chemical subgroup) instead
of ATC-5 (i.e., chemical substance). For example,
currently infliximab drugs, including the originator
(Remicade) and its biosimilars (Inflectra, Zessly,
Remsima, Flixabi, etc.) are grouped following ATC-5
classification L04AB02. The new system would have
a reference price group based on the broader ATC-4
Simon-Kucher & Partners Healthcare Insights | Recent Developments in Global Pricing & Market Access 8
classification L04AB, and include drugs for the same prescription by active substancee. Additionally, they
indication, such as infliximab drugs (Remicade and argue that this change could lead to drug substitu-
its biosimilars), etanercept drugs (Enbrel and its tions that may result in medication errors by patients
biosimilars), adalimumab drugs (Humira and its bio- who are used to a certain presentation.
similars), certolizumab drug (Cimzia) and golimumab • Pharmacies reject the clawback system as it disin-
drug (Simponi). centivizes them from negotiating discounts and their
4. Lower price for generics and biosimilars vs. sustainability could be at riskf.
originator: Generics and biosimilars’ prices would • Patients are afraid of experiencing safety and quality
be fixed to a lower price vs. originator drug. Addition- issues when prescribed generics and biosimilarsg.
ally, this price will be based on the originator’s real
acquisition price (instead of list price). So far, this Action Plan only constitutes a list of ideas. Ap-
proval and implementation details are still to be defined.
Actions related to the prescription of generic and biosim- In the meantime, the Ministry of Health has welcomed
ilar drugs: feedback from industry stakeholders.
5. Prescription by active substanceb: It will become
mandatory for physicians to prescribe by active There are many uncertainties regarding the Action Plan,
substance. due to Spanish political instability which makes it difficult
to approve new measures, as well as pushback from the
Actions related to dispensation of generic and biosimilar industry. Although it is uncertain whether or not the differ-
drugs: ent measures of this Plan will ever come into existence, it
6. Pharmacy substitution: It will become mandatory is clear that the Spanish’ Ministry of Health continues to con-
for pharmacists to dispense the less costly drug, sider potential solutions to mitigate expenditure and guaran-
allowing automatic substitution of the originator tee the future sustainability of the Healthcare System. ▵
by generic/biosimilar if needed. Together with the a
The price revision date will be set on the resolution of the drug inclu-
prescription by active substance, this aims to foster sion in the National Healthcare System.
competition among manufacturers and lower pricesc. b
Except for unsubstitutable drugs: (i) biologics; (ii) drugs which active
7. Clawback system: Pharmacy discounts negotiated substance is considered of narrow therapeutic margin, if they do not
have intravenous administration; (iii) drugs which active substance is
between the pharmacy and the manufacturer will
subject to special medical control or tracking; and (iv) respiratory sys-
need to be refunded by the pharmacies to the Na- tem drugs administered via intravenous injection or infusion.
tional Health System. c
Originator drug manufacturers realize that their drugs are no longer
profitable when generics or biosimilars enter the market, due to their
The Plan has not been well received by the majority of price reduction. Thus, these manufacturers would be incentivized to
pharmaceutical industry stakeholders, who criticize that focus on the launch new originator drugs that are profitable.
they have not been involved in the development of these d
Rodríguez, O. (2019). Farmaindustria pide incluir a los genéricos
initiatives. Many have publicly opposed the plan: en el convenio que limita el gasto farmacéutico. Retrieved 25 No-
vember 2019, from https://www.elespanol.com/economia/empre-
• Pharmaceutical manufacturers contend that the sas/20191106/farmaindustria-incluir-genericos-convenio-limita-gas-
Plan may damage drugs’ competitiveness without to-farmaceutico/442206708_0.html
generating savings to the system, as originator drugs e
Sobre el Plan de Fomento de Genéricos y Biosimilares (2019). Re-
already have the same price as generics/biosimilars trieved 25 November 2019, from https://www.interempresas.net/Far-
macia/Articulos/257456-Sobre-el-Plan-de-Fomento-de-Genericos-y-Bi-
due to the fixed reference price system. The Plan
osimilares.html; Rivera, M. (2019). Alegaciones al plan de biosimilares:
could risk the continuity of innovative companies as diferenciación, prescriptor y farmacia. Retrieved 25 November 2019,
their incentives would be temperedd. from https://www.redaccionmedica.com/secciones/sanidad-hoy/
alegaciones-al-plan-de-biosimilares-diferenciacion-prescriptor-y-farma-
• Physicians ask for the NHS to respect their respon- cia-1212
sibilities and decisions as prescribers, and oppose
Simon-Kucher & Partners Healthcare Insights | Recent Developments in Global Pricing & Market Access 9
f
Arganda, C. (2019). El CGCOF rechaza el ‘claw back’ de Sanidad: However, yet another pathway does exist for some spe-
“Cerrarían farmacias y aumentarían los desabastecimientos” Retrieved
cific patients through the invalidity insurance (managed
25 November 2019, from https://www.diariofarma.com/2019/11/21/
el-cgcof-rechaza-el-claw-back-cerrarian-farmacias-y-aumentarian-los-de- by the BSV/OFASb), which must legally pay for any drugs
sabastecimiento indicated for “congenital defects” for patients younger
g
Plan para el fomento de genéricos y biosimilares: “Aborda de forma than 20 years old, as defined by a list edited by the Fed-
parcial la realidad y obvia la revisión del gasto en su conjunto” (2019). eral Council (highest executive authority). The criteria for
Retrieved 25 November 2019, from https://elmedicointeractivo.com/
coverage are similar to the inclusion on the LS, even if
primeras-reacciones-al-plan-de-genericos-y-biosimilares-aborda-de-for-
ma-parcial-la-realidad-y-obvia-la-revision-del-gasto-en-su-conjunto/ less formalized and transparent. In some cases, this path-
way has proven to be successful, such as for Spinraza in
spinal muscular atrophy, but it is still not ideal. Indeed,
Switzerland patients older than 20 years old at treatment onset or suf-
fering from conditions that are not on the list of congenital
Current status and future developments in defects cannot get any funding through this pathway. This
innovative therapy funding in Switzerland has led to several cases that gained attention in the me-
dia, such as a successful crowdfunding for Spinraza by a
Innovative therapies with curative potential, such as cell
31-year-old patientc.
or gene therapies, are being brought to thousands of pa-
tients around the globe. These therapies usually target a This partial funding of innovative therapies is not an ideal
limited patient group that are affected by rare diseases, situation, as it keeps manufacturers from giving patients
and often require just one injection. However, they are access to the care they need. Several attempts have been
associated with a high price tag that is a challenge for made to solve the issue, such as the decision of santé-
healthcare systems (see table), who are often not ready suisse, an association of insurance companies, to fund
or structured to support such costs. This is especially the Novartis’ Kymriah outside of any framework with a lump
case in Switzerland, where healthcare costs are mostly sum of CHF 200,000d. There have also been some indi-
covered by private insurances on a regional level. These vidual parliamentary interventions to increase/suppress
insurances are subject to a national framework set by the 20-year-old limit (although all have been turned down
the BAG/OFSPa, which publishes a limited list of drugs or withdrawn). However, these are all too limited to restore
(List of Specialties – LS) that insurance companies have trust in the funding of these therapies, which is certainly
the obligation to reimburse. LS is built on the principles not encouraging manufacturers to invest the costs related
of cost-effectiveness, adequacy and efficacy. Given that to a Swissmedic approval (Swiss EMA/FDA equivalent).
these limited criteria could make it hard for some of the in- Nevertheless, this situation may be resolved soon, as
novative products to make the list, the Swiss government there are ongoing discussions in the Federal Commission
has built some flexibility into the system, through the arti- for Healthcare Services and Principles to make a funda-
cle 71b, c of the health insurance regulation. According to mental decision on how these therapies should be more
this article, insurance companies must still cover the costs systematically funded. Conclusions are expected in the
of a treatment that is not on the LS if two conditions are first semester of 2020. ▵
met: The treatment must bring an important therapeutic
benefit to the patient, and there is not an alternative, effica-
cious treatment included on the LS. Insurance companies
have challenged this rule, which has led to an uncertain
reimbursement situation.
Simon-Kucher & Partners Healthcare Insights | Recent Developments in Global Pricing & Market Access 10One time Congenital
Product Indication Price therapy Target Patient Age defect
Luxturna Retinal dystrophy €690,000 (Germany) Yes None, but the younger the better No
Strimvelis ADA-SCID €594,000 (Italy) Yes 1-6 years old No
(immunodeficiency)
Kymriah Leukemia, lymphoma €320,000 (France) Yessuch as budget capping, price-volume agreements, ric or orphan indication). As part of the update, MHLW is
risk-sharing, and outcomes-based agreements. considering granting premiums for indication expansions
• Unusual and unique circumstances when a launch other than orphan or pediatric use. For example, MHLW
is considered particularly challenging or commer- is looking to reward data demonstrated in the elderly pa-
cially unviable (i.e., when there is clear differentiation tient group (especially >75 years). Additionally, the update
in health gain between indications, significant loss may allow the summing up of price premiums, if a prod-
in revenue without commercial flexibility, and the uct qualifies for more than one at the same time, which is
impossibility of recovering from revenue loss in later currently not possible. All of these changes to the post-
years). By not clearly defining those elements, the launch premium system would be new incentives, reward-
discretionary terms on which NHSE decides on offer- ing additional research and development efforts.
ing a CAA are retained. However, MHLW outlines other proposed changes that
- Managed Access Agreements (MAAs): MAA should target new ways to realize cost savings. One example
be considered if there is a plausible potential for a involves changing the rules for the Comparator pricing
drug to satisfy the criteria for routine commission- method. Currently a new drug receives the same daily
ing but clinical and financial uncertainty remain. A price as the pricing comparator (plus a potential price pre-
time-limited data collection agreement is added to the mium). With the new pricing rule, a discount will be possi-
PAS or CAA and treatment is offered at a cost-effec- ble for the new drug if it does not qualify for the so-called
tive price for the duration of the MAA. “Price Maintenance Premium” (PMP), while the pricing
- Budget impact test: Even if a medicine is cost-effec- comparator does qualify. The PMP protects products
tive, costs greater than £20 million in any of the first from the regular NHI price cut and is granted to products
three years of launch will result in NHSE engaging in meeting certain criteria (e.g. orphan drug indication or
commercial negotiation to address affordability. qualifying for a price premium due to clinical usefulness).
The pricing rule change would result in a lower launch
Next steps
price for products not meeting these criteria for innovation
Overall, the draft framework emphasizes the increasing
or clinical necessity.
influence of NHSE and signals that complex commercial
schemes will likely be more frequent going forward. The The discussed changes suggest that MHLW is willing to
finalized framework is expected in early 2020 and feed- reward products that are innovative, while strictly restrict-
back can be provided until January 10th, 2020. ▵ ing the budget for products that are not. This policy is a
consequent step in responding to a healthcare budget
Japan that is too limited to distribute without differentiation, and
should continue for the foreseeable future. ▵
Potential rule changes in the 2020
NHI price revision
The next regular NHI price revision is approaching in
China
April 2020, and the Japanese Ministry of Health, Labour 2019 NRDL price negotiations concluded
and Welfare (MHLW) has recently published information with 70 drug inclusions
about potential changes coming in 2020.
The result of China’s 2019 national drug price negotia-
One proposed change is an update to the so-called “post- tion was announced by the National Healthcare Security
launch premium” system. This system allows manufactur- Administration (NHSA) on November 28, 2019. The 2019
ers to receive a price premium for an already-launched NRDL negotiation targeted single-source drugs which
product when new data are made available (either by were launched in China before December 31, 2018. Out
further demonstrating the clinical usefulness for the ex- of 119 drugs negotiated, 70 were successfully added to
isting indication or supporting an expansion to a pediat- the National Reimbursement Drug List (NRDL), including
52 medicines from MNCs and 18 Chinese medicines.
Simon-Kucher & Partners Healthcare Insights | Recent Developments in Global Pricing & Market Access 12Additionally, out of 31 drugs which were added to the
NRDL in 2017, 27 re-negotiated successfully, including Brazil
22 medicines from MNCs. The outcomes of the 2019
Outcomes-based agreements
NRDL negotiation will become effective on January 1,
2020, and be valid for two years until December 31, 2021. The newly-elected government in Brazil is expected to
bring changes to the health care system landscape, with
The average price cut was 61% for the 70 products which a higher focus on more affordable and fair public reim-
were negotiated for the first time, whereas it was on av- bursement. Denizar Vianna, the appointed head of SC-
erage 26% for the 27 products re-negotiated. For some TIE (Science, Technology and Strategic Input Secretariat),
therapy areas the price cut was particularly high: the av- is expected to lead these changes. He has made public
erage price cut of HCV drugs was more than 85%; prices statements regarding his focus on defining public priori-
of oncology and diabetes drugs were cut by approximate- ties, budget constraints, considerations of unmet needs
ly 65% on average. For the first time manufacturers can and the future technologies landscape, and is also a
choose not to disclose the negotiated prices publicly. Out strong advocate for the implementation of risk sharing
of 74 medicines from MNCs added to the NRDL, post agreements (RSA) in Brazil. The first RSA pilot was closed
NRDL prices of 46 drugs are confidential. in June 2019 for Spinraza in Spinal muscular atrophy
(SMA) types II and III.
The 2019 NRDL negotiation prioritized therapeutic areas
including oncology, rare diseases, chronic diseases and SMA is a rare genetically-inherited neuromuscular dis-
pediatrics as well as essential drugs. As a result, all 5 na- ease that causes progressive muscle weakness and loss
tional essential drugs were included in the NRDL. Look- of movement, and is the most common genetic cause of
ing at the split by therapeutic areas, 22 oncology drugs, 7 death in infants. There are 4 types of SMA, and type I is
rare disease drugs, 14 chronic disease drugs (including the most severe and common. Type I patients never de-
diabetes mellitus, hepatitis B, rheumatoid arthritis, etc.), velop the ability to sit unsupported, and typically do not
and 4 pediatric drugs successfully negotiated. From 5 survive after the first 2 years if no intervention is provid-
PD-(L)1s launched in China, only one local novel PD-1 in- ed. Spinraza is the first treatment approved beyond sup-
hibitor was included in the NRDL. With the inclusion of portive care, and got a fast-track approval 3 months after
7 orphan drugs, the NRDL increased coverage of rare submission by ANVISA (the Brazilian Health Regulatory
diseases such as pulmonary arterial hypertension (PAH), Agency). Access was granted in November 2017.
Niemann-Pick disease type C (NPC), and multiple sclero-
sis (MS). The first submission for public funding happened in Janu-
ary 2018 for SMA type I, however CONITEC (the Brazilian
According to the NHSA, a dynamic adjustment mech- HTA agency) gave a negative preliminary recommenda-
anism for NRDL will be put into place in the future that tion due to fragile clinical evidence, lack of demonstrated
allows review and inclusion on a yearly basis. Once it clinical improvement, inconsistent cost-effectiveness rela-
becomes effective, drugs that failed to be added to the tion, and evidence that it could compromise the financial
NRDL this year may have the chance to be included in the sustainability of SUS (The Unified Health System) finan-
NRDL the following year. ▵ cial sustainability. In January 2019, Biogen made a new
submission proposing a 62% discount vs. list price and
achieved a positive funding recommendation 3 months
later for SMA type I. The fast assessment by CONITEC
was a result of the high awareness and perceived unmet
needs for SMA. The public consultation for the first sub-
mission achieved a record of 37K contributions, followed
by 42K contributions for the second public consultation,
which received 95% in favor of incorporation.
Simon-Kucher & Partners Healthcare Insights | Recent Developments in Global Pricing & Market Access 13For SMA types II and III, due to uncertainties on efficacy and budget impact, the MoH decided to implement the first RSA pilot in the public setting, which is the biggest innovation in the public sector since the early days of tech-transfer. For Denizar, it is important that each contract is tailored case-by-case and with transparency. He also gave public statements about being open to discussing ideas and building future RSA models. The RSA reached with Biogen consists of a patient cap based on epidemi- ology, a negotiated price discount, and payment based on performance, which will be monitored by the MoH through Albert Einstein Hospital. The data will be used by CONITEC for a new assessment in three years. Since the beginning of November, patients with SMA types II and III have been able to request access to Spinraza and be directed to a reference center by the MoH. Although there are still several challenges for rolling out outcomes-based contracts, including infrastructure avail- ability for results monitoring, patient database develop- ment, and legal constraints (e.g., the MoH cannot receive paybacks in the case of treatment underperformance), this is a new access opportunity in Brazil that is especially relevant for orphan drugs. Offering the MoH support for developing the required capabilities and having high pub- lic awareness, perception of unmet needs, and indication severity can improve chances of success. Denizar high- lights the importance of the MoH and industry engaging in discussions to improve access that guarantees the sus- tainability of the public system. ▵ Simon-Kucher & Partners Healthcare Insights | Recent Developments in Global Pricing & Market Access 14
Comprehensive Commercial Alignment:
The Key to Brand Forecast Accuracy
By Nick Keppeler, Tyler Perez, and Jeremy Winkler
Actual sales miss the revenue forecast by an average
of 50 percent – an alarming number. What can
pharmaceutical companies do to achieve their
desired commercial performance and improve
forecast accuracy?
Colourbox/-
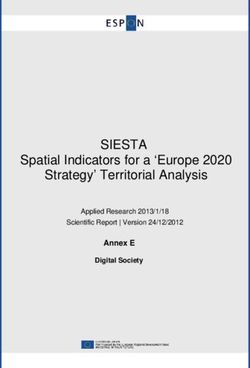
Simon-Kucher & Partners Healthcare Insights | Features 15The success of mid- to long-term planning in pharma re- Poor outcomes are due to a lack of alignment between
lies heavily on the commercial alignment and accurate patients, payers, prescribers, and the brand, causing
forecasting of future revenue from new product launches. forecasts to be unrealistic and critical brands falling short
However, this continues to be a difficult exercise to pre- in terms of value and sales potential. While we don’t be-
dict. From 2015 to 2018, 65% of new products across the lieve that major pharmaceutical companies neglect any
pharmaceutical industry failed to achieve their forecasted of these four key stakeholders in isolation, poor planning
revenues, with 14 of 23 new oncology products failing across activities for these customers can significantly de-
to reach their forecasted revenue by an average of 50% rail a new product launch (and by extension its forecast).
(Figure 1).a There continues to be debate around what For example, a brand team might capture prescriber per-
is considered to be an acceptable variation in actual vs. ception and preference share for a new brand without
forecasted peak sales two-years prior to launch. The gen- accurately capturing how payer access and authoriza-
eral consensus from industry experts considers a 6-15% tion requirements will impact provider decisions. There-
variation in forecast vs. actual peak sales to be accept- fore, planning across these diverse commercial activities
able, however market share assessments from primary re- needs to be carefully carried out and accounted for to
search more often than not overstate the real world share improve commercial performance and forecast accuracy.
that is actually captured.b To successfully achieve desired
commercial performance, companies must go beyond One way that Simon-Kucher focuses on getting commer-
just capturing health care provider preference share es- cial alignment correct is by analyzing an event that we
timates by taking a multi-faceted approach to develop refer to as the “Prescribing Epicenter”. The “Prescribing
alignment across several real world factors. Epicenter” captures four key drivers or cornerstones of
Oncology products launched 2015-2018
Underperformance >15%
Launch Year: 2015 2017 2018
1.2
Forecast
38%
1 Actual
97%
92%
Total lost
0.8
potential of
In Billion USD
launches:
0.6 $3.0 billion
64%
21%
0.4
26% 62%
72%
52%
0.2 45% 34%
39% 25%
0
1 2 3 4 5 6 7 8 9 10 11 12 13
Figure 1: Forecasted revenue vs.
Product actual sales (2015-2018 U.S. billions
of dollars)
a
Figure based on data taken from Globaldata.com
b
Simon-Kucher & Partners Chicago Forum Survey 2019
Simon-Kucher & Partners Healthcare Insights | Features 16brand strategy that serve as the pivotal juncture where pa-
tients can be helped by a new brand (Figure 2). These four
“From 2015 to 2018, 65%
drivers include: 1) brand differentiation and the customer
journey, 2) dynamic patient events that create opportuni-
of new products across the
ties to start or change therapy, 3) physicians’ willingness
to prescribe based on brand interest and experience,
pharmaceutical industry
and lastly 4) available access through payer and orga-
nized customer engagement. Balancing these elements
failed to achieve their
requires a complete assessment of the levers across all forecasted revenues, with
relevant stakeholders and segments. By comprehensive
commercial alignment and optimization across each of 14 of 23 new oncology
the four drivers of the Prescribing Epicenter, companies
can maximize the potential value for a new brand while products failing to reach
ensuring commercial performance matches forecasts.
their forecasted revenue by
an average of 50%.”
Simon-Kucher’s Drivers of Prescribing Epicenter Performance
(select elements)
• Dynamic opportunities to
• Create calls to action start/change therapy
• Differentiate from alternatives • Engage customers to identify
ion & act in these situations
• Support customers through tiat Pa
tie
en n
initiation & use journey er • Align product strengths to
tE
iff
these events
dD
ve
nt
Bran
Prescribing
Epicenter
er
Ava
• Right level of payer, hospital,
rib
• Reach through preferred
ila
sc
system engagement
bl
re
e
channel(s) at right time
P Ac
ing ces
Will
• Allows use in a target patient
s
• Build interest & belief in brand
event
• Establish confidence &
• Perform relative to alternative
experience
options
Figure 2: Drivers of Prescribing
Epicenter Performance
The Prescribing Epicenter for each product is unique
and may require different activities to ensure balance is
achieved across the four cornerstones. Each cornerstone
requires different key considerations to help determine
which activities are needed to ensure a comprehensive
commercial alignment. The first Prescribing Epicenter
cornerstone is the brand differentiation of a new product.
A product’s brand must articulate the differentiating fac-
tors between alternatives, highlight key value messages
Simon-Kucher & Partners Healthcare Insights | Features 17and engage stakeholders at the right time to achieve suc- the population. This might create a scenario where mes-
cess. Patients and prescribers might display an interest in saging on the importance of accurate diagnosis and early
a product, but if the brand is not agreeable with payers, treatment to help bring the disease under control should
then restricted access can limit commercial performance be prioritized for physicians in City B. Shifting focus
at launch. across different commercial activities to account for these
differences across geographies can make the difference
The cornerstone around dynamic patient events is the between achieving high levels of prescribing from both
next key driver that can easily fall out of alignment within providers versus only achieving high levels of prescribing
the prescribing epicenter. Events such as the diagnosis of from one. The winning result is prescriber strategies and
a new disease or when a prior therapy has been identified education that reinforce the brand in the context of that
as not meeting the patient’s needs are the natural start, prescriber’s local Prescribing Epicenter.
stop, or inflection points in the patient journey. When a
relevant event occurs, it is critical that the product is both The last cornerstone is focused on available access for a
clinically appropriate and available to the customer. For new product. While this is an area that all pharma com-
example, if the brand is not top of mind for physicians panies prioritize, payer activities need to be carried out
at the time of an event, readily accessible from payers mutually in conjunction with the other three cornerstones.
or amenable to patient needs, this could derail product Often times there is misalignment within the manufactur-
adoption. To deal with these challenges it is important to ers’ teams at this step – for example when a brand team
assess how elements such as digital engagement, direct positions the product as a first line option while the vast
to consumer marketing or patient support programs can majority of payers expect to have access requirements of
help overcome these gaps. In order for adoption to fit into two or more competitor therapies. Companies should be
the natural progression of care, products must be mar- cognizant that gaining access alone will not guarantee
keted effectively across patient segments so that they are the best commercial performance of a new product. If the
in the decision set at the right time of the patient journey. product gains access but doesn’t account for the other
three cornerstones, patients and prescribers could fail to
Next, when considering the “willing prescriber” corner- see the need for the new product even if payers do.
stone, it is helpful to think both of the prescriber as an
individual but also the environment in which they oper- Creating harmony across all four cornerstones of the Pre-
ate. For example, most commercial organizations track scribing Epicenter allows for a new brand to be launched
the communication preferences of their physician tar- at its maximum potential. Identifying short-comings ahead
gets. However, what is less common is looking at how of time helps commercial activities and forecasts to be
the environment in which they operate affects the way the adapted for potential suboptimal factors and reasonably
physician is engaged with the manufacturer. Take as an account for future commercial performance. These exer-
example two specialists who both prefer digital communi- cises require investment across multiple groups within a
cations, but one practices in City A and the other in City B. given company to prevent future miscalculations that can
Now, consider that City A has access challenges for your damage the commercial performance of a new product.
product and only 20% of lives have unrestricted access to
your product. In this geography, it would be more impact-
ful to prioritize communications related to the strength of
access support programs and approaches to help pa-
tients initiate treatment onto a product quickly while they
are working through the authorization process. For the al-
ternative physician in City B (assuming very good access)
those same messages may be of lower priority. What
might be unique about City B is the low level of patient
events in the area relative to the size and demographics of
Simon-Kucher & Partners Healthcare Insights | Features 18Case 1: What do you mean I won’t hit my
forecast? Missing the mark
It is well understood that physician-stated preference example, four key market-based adjustments were used
share from market research needs to be adjusted to to help achieve a more accurate real world share expecta-
create more realistic expectations for real world market tion including: (1) Payer access, (2) sales force reach, (3)
share. While there are a variety of approaches to do this, physician uptake and (4) awareness and impact of com-
there are still a number of manufacturers who only con- petition. These factors were then applied for one brand
duct physician research and then apply an off-the-shelf across four possible patient events. The key findings were
haircut of 50% to their preference shares to help adjust that the “haircut” factor a) ranged from 50-75% and b)
forecast estimates. This approach is a common mistake varied across patient events for the same product. By an
and can be a big contributor to why so many forecasts order of magnitude, applying a typical 50% adjustment
significantly miss the mark. Simon-Kucher applies a differ- factor rather than Simon-Kucher’s comprehensive com-
ent approach – by developing custom estimates of actual mercial alignment approach would have led to an over-
market factors across the Prescribing Epicenter for each estimate of >$1 billion per year in peak revenue forecast.
brand and competitive situation. In the following blinded
Peak preference shares by patient event
pre- vs. post-market factors Impact of
market factors
40%
1 “Naïve” patients 25%
10%
44%
Switching to or adding
2 Class A product 34%
15%
39%
Changing within
3 Class A products 49%
19%
6%
Switching within
4 Class B products 33%
2%
Pre-market factors
% of patients in each event Post-market factors Figure 3: Percent peak preference
share by pre- / post-market factors
Simon-Kucher & Partners Healthcare Insights | Features 19Case 2: Predicting regional pockets of whole. Second, it helps advance from strategic planning
opportunity to comprehensive commercial alignment readiness, in
order to make a launch as successful as possible. This
As a brand gets closer to launch, forecasting and stra-
approach serves as a quantitative bridge to launch readi-
tegic planning needs to be taken a step further to look
ness and critical success factor planning.
at how the business will perform in a local sales region.
Simon-Kucher uses a quantitative regional assessment
In the graphic below, this detail illustrates tremendous
known as the Top Line Power Commercial Engine to
variation across the USA in terms of launch environment
elucidate the effects of comprehensive commercial align-
including: a) drivers of competitors’ commercial perfor-
ment on prescribing. In this example, advanced analytics
mance, b) areas of opportunity with low treatment rates
(Tableau for data management and visualization, Python
today, c) geographies where the competitor seems to
for prediction models) is used to assess competitor per-
focus less on its sales and marketing efforts and d) rel-
formance in the market environment to draw competitive
evant actions around payer strategy, physician targeting
insights for the product of interest. Data from US census
and disease awareness. For example, one takeaway was
data, CDC prevalence, MMIT formulary status, # of spe-
that competitors were facing access hurdles in Alabama
cialists & TRx data (IMS), CMS open payment data and
– most likely caused by access of the product at Prime
Google was used to evaluate the variation in prescribing
/ BCBS Alabama. We estimated that 40% of the com-
as it relates to factors such as sales / marketing spend to
petitor volume was untapped due to this access position
prescriber, % of covered lives facing no step edits, num-
(Figure 4). Another key insight from this type of analyt-
ber of specialists in an area, and Google searches for
ical approach debunks the use of traditional physician
the competitor product. Given the power behind this ap-
targeting based on prescriber deciles to identify markets.
proach, there is the flexibility to use a range of data inputs
The result could be rather than targeting competitor en-
including a client’s sales force effectiveness data, target
trenched areas that will put the manufacturer head to
call lists, and advertising spend to name a few.
head with its competitor, focus on opportunities in low dis-
ease treatment areas or low marketing spend areas with
This Top Line Power Commercial Engine approach
high untapped potential. New tools are making it easier
serves two important functions. First, it helps better refine
to evaluate this type of added complexity and return more
forecasts closer to launch as sales estimates are rolled up
targeted and actionable opportunities for manufacturers.
from a detailed geographic territory view to an aggregate
Categorization of launch environments based
on Competitor Y performance vs. expectations
800-lb gorilla areas
60 ZIP3s; 49% of TRx
High use vs. expected cases
Average areas
247 ZIP3s; 35% of Competitor Y TRx
Use in line with expectations
Under marketed areas
93 ZIP3s with low marketing / sales focus
17% of cases vs. 9% TRx
Payer limited areas
58 ZIP3s with access policies
that affect TRx potential
11% of cases vs. 6% TRx
Low penetration areas
98 ZIP3s with minimal Competitor Y use This type of visualization
15% of cases vs. 2% TRx illustrate key prescribing drivers
(access vs. other factors) Figure 4: Categorization of launch
Geography excluded environments based on competitor
Y performance vs. expectations
Simon-Kucher & Partners Healthcare Insights | Features 20Future challenges and opportunities
Redefining a multifaceted approach for strategic initia-
tives and tactics is vital for successful commercial perfor-
mance as well as creating a path forward. With a huge
percentage of new products failing to reach their fore-
casted numbers, expanding the considerations in com-
mercial activities for a product launch can improve accu-
racy and help to identify blind spots in launch readiness
planning. Strategies around the four cornerstones of the
Prescribing Epicenter all contribute to the potential suc-
cess of a launch and accuracy of forecasting commercial
performance. Systematically evaluating the Prescribing
Epicenter for a product helps to identify short-comings of
a product’s go-to-market strategy and improve the ability
“By comprehensive
to more accurately forecast and prepare mid- to long-term
planning. We strongly believe that comprehensive com-
commercial alignment
mercial alignment is a critical factor to both significantly and optimization across
improving forecasting accuracy and creating a solid foun-
dation for long-term brand performance. each of the four drivers of
the Prescribing Epicenter,
companies can maximize
the potential value for a
new brand while ensuring
commercial performance
matches forecasts.”
For correspondence related to this article, please contact
Nick Keppeler at nicholas.keppeler@simon-kucher.com
Simon-Kucher & Partners Healthcare Insights | Features 21ATU in France: the case for early
consideration in local and European
P&MA strategy
By Diane Cosset, Clementine Legros, Jonathan Haugen, Lilia Meddeb
Examining the recent changes in France’s
early access program and its implications for
manufacturers’ European P&MA strategy.
Colourbox/-
Colourbox/-
Simon-Kucher & Partners Healthcare Insights | Features 22Time to access in France, with an average duration of 209 What is the ATU program?
daysa after marketing authorization in 2018, continues to
exceed the European directive of 180 days. However, the ATU status is granted by the French National Agency for
ATU (Temporary Use Authorization) early access program Medicines and HealthaProducts Safety (ANSM) to pro-
enables reimbursed access to drugs prior to marketing mote fast access to innovation, before marketing autho-
authorization. Since its implementation in 1994, the ATU rization and conventional pricing and market access pro-
program has garnered symbolic importance, and today cess completion. In order for a drug to be granted ATU
serves as an emblem of France’s pioneering position in status, three key criteria must be met:
this field. Although this program represents an oppor-
1. The drug must be intended for a serious or rare
tunity for patients and pharmaceutical companies alike,
indication
manufacturers must carefully consider the impact on their
2. There must be no other appropriate therapies
future negotiated prices in France and in other European
available for this indication in France
countries when setting prices for ATU drugs. This is even
3. The drug must have presumed efficacy and safety
truer considering this program has been on French health
in light of the available scientific data, and the treat-
authorities’ radar for the past few years and has been sub-
ment cannot be delayed for patients
ject to increasingly strict pricing rules, in particular with the
recent repeal of the free pricing policy for nominative ATU. Within this program, two types of ATU can be granted.
A nominative ATU (nATU) is for one specific identified
patient at the request of his or her physician. A cohort
ATU (cATU) is designated for a group of patients at the
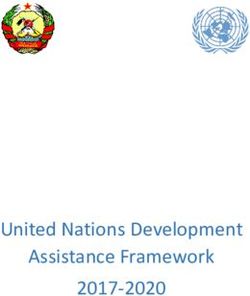
Figure 1: Comprehensive overview of cohort ATUs granted in 2018
per therapeutic area request of the drug manufacturer (with requirements
and eligibility criteria differing slightly between the two).
ALL: acute lymphoblastic leukemia; AML: acute myeloid leukemia;
aPTT: acquired thrombotic thrombocytopenic purpura; nmCRPC:
Non-metastatic castration resistant prostate cancer: DLBCL: Diffuse ATUs allow early access for thousands of patients each
Large B cell Lymphoma; NSCLC: non-small cell lung cancer; PMBCL:
Primary mediastinal B-cell lymphoma; VWD: von Willebrand disease
year; roughly 22,000 patients benefited from the ATU pro-
gram in 2018 alone includ-
Oncology (7 cATU) ing over 230 different drugs
• Erleada (apalutamide) – nmCRPC
• Alunbrig (brigatinib) – ALK+ NSCLC (nATUs: 217 drugs and
• Imfinzi (durvalumab) – 2L NSCLC 15,987 patients; cATUs: 20
• Kymriah (tisagenlecleucel ) – 3L+ R/R DLBCL / ALL
• Lorviqua (lorlatinib) – 3L ALK+ NSCLC drugs and 5,642 patients)b
• Vyxeos (daunorubicine, cytarabine) – 1L AML
Oncology • Yescarta (axicabtagene ciloleucel) which underscores just how
3L+ R/R DLBCL and PMBCL
Hematology extensive the program is.
Hematology (5 cATU)
• Atgam (Lymphocyte immune globulin
26%
bone marrow suppression
• Cablivi (caplacizumab) – aPTT
The ATU program was initial-
• Hemlibra (emicizumab) – hemophilia A ly designed to guarantee ear-
• Poteligeo (mogamulizumab) – mycosis fungoides
37% • Vonvendi (vonicog alfa ) – VWD ly access mainly to new HIV
11% Rare disease,
genetic, congenita
Rare disease, genetic, congenital (2 cATU) therapies, but now mostly
• Crysvita (burosumab) –hypophosphatemic rickets
• Ursofalk (ursodeoxycholic acid) – cystic fibrosis covers oncology and hema-
11% Neurology (2 cATU) tology products as well (see
5% Neurology
5% 5% • Onpattro (patisiran) – polyneuropathy
Figure 1).
• Tegsedi (inotersen) – polyneuropathy
Ophtalmology Ophtalmology (1 cATU)
Endocrinology • Luxturna (voretigene neparvovec)
Cardiology Leber's congenital amaurosis
Cardiology (1 cATU)
• Takhzyro (lanadelumab) –hereditary angioedema
Endocrinology (1 cATU)
• Metreleptin (metreleptin) –lipodystrophy a
2018 CEPS report
b
2018 ANSM annual report
Simon-Kucher & Partners Healthcare Insights | Features 23ATU status to post-ATU status: For some ATU drugs, such as Yescarta, the P&R process
what are the implications? can be rather quick, and may be completed within a year
of their MA. However, the average post-ATU status duration
Once a product has its marketing authorization (MA), it
is approximately 630 daysc (see Figure 2) , which is signifi-
loses its ATU status. The manufacturer must then submit
cantly longer than the average time of 209 daysd between
a request for reimbursement for the licensed indication
marketing authorization and P&R completion in 2018, de-
within one month in order to benefit from post-ATU sta-
spite the priority review given to these drugs by the TC.
tus, which enables funding during the P&R process and
ensures continuous access for patients.
By their very nature, ATU drugs address diseases with
high unmet need for which there may not be any alterna-
During the post-ATU phase, the product goes through
tive treatment available, implying a lack of price bench-
Transparency Committee (TC) assessment and then
marks and comparators which often results in challeng-
through pricing negotiations based on the SMR and
ing and lengthy price negotiations with the Economic
ASMR ratings granted by the TC. The ATU phase may
Committee for Health Products (CEPS). Therefore, ben-
support favorable reimbursement by providing real-world
efiting from the ATU/post-ATU status is a key advantage
evidence (though this is not often taken into account in
for manufacturers, as it prevents major delays in products’
the TC’s evaluation due to insufficient data quality), and
commercialization and therefore loss of revenue. It also
also by generating experience and familiarity within the
contributes to explaining why the post-ATU phase is lon-
clinical and patient community.
ger than average. The fact that patients already have early
treatment access implies limited pressure for health author-
The length of the post-ATU phase heavily depends on
ities to complete the P&R process quickly and may be an-
the context of broader P&R negotiations (price level re-
other explanation for the longer P&R process of ATU drugs.
quested by the manufacturer, existence of price bench
marks, etc.).
Figure 2: Time between MA and
price publication (i.e., post-ATU
VYXEOS 240
status) – in days
YESCARTA 330
MEKTOVI 330 Comprehensive list of drugs with a
HEMLIBRA 330 post-ATU status start after 2014 and
Average
BRAFTOVI 330 time end before November 2019
since M
MEPSEVII 390 A is
630 da
OCREVUS 420 ys
TREMFYA 450
MYLOTARG 450
TECENTRIQ 510
DUPIXENT 540
ZEJULA 540
BAVENCIO 540
LUTATHERA 690
SPINRAZA 690
NALSCUE 720
DARZALEX 1110
WAKIX 1140
TAGRISSO 1260 c
Average time between market-
ZYDELIG 1710 ing authorization and post-ATU
expiration date of all ATU drugs with
From MA to start of post ATU Length of post-ATU a post-ATU effective date between
2014 and November 2019
d
2018 CEPS report
Simon-Kucher & Partners Healthcare Insights | Features 24You can also read