Health Service Plan 2018 2028 - Amazon AWS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Health Service Plan 2018 – 2028

Townsville Hospital and Health Service (Townsville HHS) Health Service Plan 2018 - 2028 Published by the State of Queensland (Townsville Hospital and Health Service), January 2018 This document is licensed under a Creative Commons Attribution 4.0 Australia license. To view a copy of this license, visit creativecommons.org/licenses/by/4.0/au © State of Queensland (Townsville Hospital and Health Service) [2018] You are free to copy, communicate and adapt the work, as long as you attribute the State of Queensland (Townsville Hospital and Health Service). For more information contact: Strategy and Planning Unit Office of the Chief Executive, Townsville Hospital and Health Service PO Box 670, Townsville, QLD 4810 Health planning data presented within this document has been obtained and verified by the Queensland Department of Health, while population data was sourced from the Australian Bureau of Statistics. All data presented was accurate at the time of publication.

Acknowledgment to Traditional Owners
The Townsville Hospital and Health Service respectfully acknowledges the
traditional custodians past, present and future of the land and sea which we
service and declare the Townsville Hospital and Health Service commitment to
reducing inequalities between Indigenous and non-Indigenous health outcomes
in line with the Australian Government’s Closing the Gap initiative.
This original artwork was produced for Queensland Health by Gilimbaa. Gilimbaa is an
Indigenous creative agency.
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 4

Contents 1. Foreword 6 2. Introduction and Overview 8 3. Townsville Hospital and Health Service 11 4. Managing demand for hospital services by changing models of care 21 5. Closing the gap in health outcomes for Aboriginal and Torres Strait Islander People 29 6. Making better use of Townsville HHS rural and remote services 35 7. Strengthening the tertiary referral role of Townsville Hospital 41 8. Working with the private hospital sector in Townsville 47 9. Priority planning actions for selected specialty services 51 10. Future requirements for capital infrastructure 57 Appendix A: Overnight bed projections Townsville HHS 60 Appendix B: Glossary of Terms 62

Message from the
Board Chair
As Chair of the Townsville Hospital and necessary strategies to meet the needs
Health Service, I am proud of the public of patients and consumers that include
health services we provide to our diverse Aboriginal and Torres Strait Islander
northern Queensland communities across peoples, children, the frail aged, and
the continuum of care. people living with mental illness and
chronic disease.
The Townsville HHS Health Service Plan
2018 - 2028 is the blueprint for how these Charting a 10-year course for any
services will be delivered over the next organisation is a monumental task. I
decade: articulating a vision for how we will thank the many staff who have taken
meet the needs of our growing and ageing the time to tell their stories and the
population. This is a vision we share with stakeholders and partners who have
the stakeholders which have contributed shared their ideas about how we can work
substantially to the development of this together to map a journey that will deliver
plan through an extensive consultation and better access, care and treatment for the
engagement process. communities we serve.
A health service is enriched by stakeholder I am very pleased to endorse this plan
engagement; ultimately it is this and am excited and optimistic about its
engagement that helps create, develop and potential to deliver better health care
nurture the services that deliver the right services for the individuals, families, and
care at the right time in the right place. communities of our region.
As a health service we are rich in diversity
- diversity of population, demography, Mr Tony Mooney AM, B ED BA HONS, FAICD
ethnicity and culture. This plan is reflective Chair
of the challenges we face and the Townsville Hospital and Health Service
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 6
Message from the
Health Service
Chief Executive
I am delighted to contribute this Foreword to improve this access for our patients
to the Townsville HHS Health Service Plan and communities.
2018 - 2028 and honoured to champion
it as a roadmap for building a stronger, I sincerely thank and acknowledge the
more sustainable and more resilient support of the Townsville Hospital and
health service into the future. Health Service Board in the development
of this plan. I would also like to thank the
Consultation with staff and other many staff - both clinical and non-clinical
stakeholders has been key to the - who have provided invaluable insight
creation of this plan. It reflects practical and ideas.
strategies and actions to meet the
important challenges of the future I feel confident in our future and the
including an ageing population, the steadfast determination of all our staff to
growing burden of chronic disease and work with stakeholders to create a health
continuing challenges with Indigenous care system that is robust, inclusive,
life expectancy and health status. innovative and compassionate.
The Townsville HHS Health Service Plan I am proud to dedicate this plan to the
2018 - 2028 also supports a future where patients and communities of Townsville
our health service works co-operatively and northern Queensland.
with the private health care sector and
neighbouring HHSs to deliver more
joined-up health care to people where Dr Peter Bristow FRACP, FCICM, FRACMA, GSM, GAICD
they live. Importantly, the plan identifies Health Service Chief Executive
barriers to equity of access and strategies Townsville Hospital and Health Service
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 7
2. Introduction and Overview
The purpose of the Townsville Hospital health outcomes for Aboriginal and
and Health Service (Townsville HHS) Torres Strait Islander peoples
Health Service Plan (the Plan) is to clearly xx Keep pace with (and ideally lead)
articulate a vision for how clinical services technological change
will be delivered in the future. The Plan
identifies priority actions which will be xx Build strong relationships between
used to drive changes needed to provide facilities within Townsville HHS,
safe and sustainable service models that with other HHSs and with private,
meet the needs of both the Townsville government and non-government service
HHS population and that of the broader providers across the care continuum.
population of northern Queensland.
In line with these principles, this Plan
The Plan represents the outcome of a articulates five key directions for the future
detailed and collaborative planning development of services. These are:
process undertaken over the course of 12 xx Managing demand for acute inpatient
months underpinned by a comprehensive services through changing models of care
stakeholder consultation process. There
xx Closing the gap in health outcomes for
has been significant input into the process
Aboriginal and Torres Strait Islander
by the health care professionals who
peoples
provide services to the community and by
those who use health services or have a xx Making better use of rural and remote
community interest in them. The Plan has services
also been informed by comprehensive xx Strengthening the role of The Townsville
data analysis and scenario modelling that Hospital (TTH) as the tertiary referral
envisages significant change to service type hospital for northern Queensland
and location, and the model of care for the
xx Working closely with the private hospital
delivery of services.
sector in Townsville
The Townsville HHS approach to planning
for public sector health services is a flexible The implementation of the Plan will occur
and staged process incorporating a number as phased process across a 10-year cycle
of levels. The Plan sits under the umbrella from 2017 to 2027. The Plan will be used
of the Townsville HHS Strategic Plan 2014 - to inform a number of other planning
2018 with a particular focus on the strategic processes including workforce, information
pillar of providing safe, effective, efficient and communication technology (ICT) and
and sustainable health services. operational plans. However, one of the other
key uses of the information will be to inform
The planning principles underpinning the the next phase of site master planning in a
development of this Plan are: number of locations.
xx Deliver services as close as possible
to home wherever possible, including Given the long time horizon needed for
in people’s own homes, in community capital planning, high level infrastructure
settings and local hospitals projections have been provided for a
20-year period to 2036 - 2037. These
xx Make meaningful improvements in projections focus on the projected demand
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 8
for overnight inpatient beds as they have major cost and planning implications for Townsville HHS. However, it must be noted that there will be additional requirements for ambulatory services, both hospital- based and those based in the community. Further detailed planning and development of models of service delivery will need to be undertaken in order to quantify the future demand for these ambulatory services. It is therefore critical to note that whilst implementation of the priority planning actions is ongoing, the infrastructure projections contained within the Plan will need to be reviewed annually. The following sections of the Plan describe the key planning information, considerations and priority planning actions for each of the five key directions. Detailed actions for selected specialty areas are also described. TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 - 2028 Page 9

About our HHS TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 10
3. Townsville Hospital and Health Service
The Townsville Hospital and Health Service Townsville HHS faces a variety of challenges in
provides quality public health services to providing health care to our communities and
an area of approximately 148,000 square for the greater northern Queensland region
kilometres or 8.5 per cent of the total area of as a whole. Many of the communities within
Queensland, and has a resident population our region are designated as remote or very
of 5.1 per cent of the total Queensland remote, and with this isolation brings specific
population. The Townsville HHS also challenges relating to equity of access to care.
provides tertiary services to 670,000 people
throughout northern Queensland from Mackay Townsville is tactically a well placed location
to the Torres Strait and out to the Northern for northern Queensland’s tertiary level
Territory border. health services due to our central location
within the northern half of the state, existing
The Townsville HHS is the region’s largest infrastructure and clinical service capability.
local employer, employing more than 6000 This sees us playing a pivotal role for the
staff. The Townsville Hospital, as northern region in the delivery of highly specialised
Australia’s principal tertiary healthcare and complex tertiary services for people and
facility, is a major teaching hospital for James communities across northern Queensland
Cook University, TAFE Queensland North and extending as far as the Torres Strait Islands
universities nationally. The Townsville HHS and Papua New Guinea.
is also a leader in clinical research across a
range of disciplines. For planning purposes, Townsville HHS is
made up of seven local planning regions
including Burdekin, Charters Towers,
3.1 Geography Hinchinbrook, Northern Highlands, Townsville
City, Townsville North and Townsville South.
Approximately three quarters (77 per cent) of
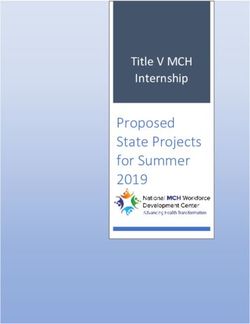
From a geographical perspective, the the population reside within Townsville.
Planning regions and facilities
Joyce Palmer
Ingham Health Service
Hospital
CSCF level 6
CSCF level 3
The Townsville
Hospital Ayr Hospital
CSCF level 2
Home Hill
Hospital Charters Towers
Hinchinbrook
Charters Towers
Hospital Northern Highlands
Burdekin
Townsville
Richmond
Hospital
Hughenden
Hospital
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 11Population density
Townsville
Charters Towers
Richmond
Hughenden
0 10+
People/km2
Remoteness Index
Hinchinbrook
Joyce Palmer
Ingham Health Service
Hospital
Townsville
The Townsville
Hospital Ayr Hospital
Charters Towers
Home Hill
Hospital
Burdekin
Northern Highlands Charters Towers
Hospital
Richmond
Hospital
Hughenden
Hospital
0 Remoteness Index 10
3.2 Population
According to the 2016 Census, the Townsville net effect of the reduced population growth of
HHS population currently stands at approximately recent years is that our current population is
258,000 residents. Our population growth in approximately 15,000 people less than what
recent years has slowed as a direct result of was predicted in 2011, which is a significant
economic and social factors which appear to consideration for planning purposes.
have impacted most significantly on our younger When analysing the population data the following
generations (primarily young families). The statistics were observed;
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 12xx The population had decreased between xx Approximately nine per cent of the
the 2011 Census and the 2016 Census in population are aged 70 years and over.
all regions of THHS except for Townsville This cohort is predicted to increase at
an annual growth rate of 4.1 per cent,
xx When analysed by 5 year age group, the
compared to total population growth of
largest differences were in the younger
1.5 per cent
age groups (persons aged 0 - 40 years). In
contrast, actual population growth in the xx Aboriginal and Torres Strait Islander
older age groups has been largely in line peoples account for approximately
with that previously projected eight per cent of the population
xx The current population projections xx The socio-economic status of THHS
predict an increase to 348,000 residents residents varies significantly between
by 2036 - 2037 Townsville and rural areas. Large areas
of THHS are classified as relatively
xx Approximately 20 per cent of the
disadvantaged, including some parts of
population is aged between 0 and 14
Townsville
years of age
Census population comparison
20,000
15,000 2016 projected population
2016 Census population
10,000
5,000
0
Population by age and region
0-14 15-44 45-69 70+
2016
2026
2036
2016
2026
2036
2016
2026
2036
2016
2026
2036
2016
2026
2036
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 13Population projections by region
300,000
250,000
200,000
150,000
25,000
20,000
15,000
10,000
5,000
0
2011 2016 2021 2026 2031 2036
Northern Highlands Charters Towers Burdekin Hinchinbrook Townsville
SEIFA Index
Hinchinbrook
Joyce Palmer
Ingham Health Service
Hospital
Townsville
The Townsville
Hospital Ayr Hospital
Charters Towers
Home Hill
Hospital
Burdekin
Northern Highlands Charters Towers
Hospital
Richmond
Hospital
Hughenden
Hospital
0 SEIFA Index 10
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 14TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 15
3.3 Services
Townsville HHS is responsible for the direct management of both hospital and community based facilities and
services within the HHS’s geographical boundaries. A wide range of quality public sector health services,
education and research are delivered including; medical, surgical, emergency, obstetrics, paediatrics, specialist
outpatient clinics, mental health, critical care, allied health and other clinical support services to the Townsville
HHS population and to the wider catchment of northern Queensland.
Location: The Townsville Hospital is located in the suburb of
Douglas in Townsville.
Size: 589 beds (inclusive of bed alternatives)
Capability: CSCF Level 6.
The Townsville
Hospital Services: The Townsville Hospital (TTH) is a tertiary referral hospital
and treats patients from across northern Queensland. It is also the
major teaching hospital for James Cook University's schools of
medicine, nursing and allied health and for TAFE Queensland North.
The Townsville Hospital provides a wide range of specialist services
including cardiac, obstetric, gynaecological, paediatric,
neurosurgical, orthopaedic, cancer, mental health, neonatal, allied
health, anaesthetic, intensive care, inpatient and outpatient
medical services and emergency services.
Location: Ayr Health Service is a rural health service located 87
kilometres south of Townsville.
Size: Ayr Health Service has 28 inpatient beds, an operating and
Ayr Health procedure room with first and second stage recovery, an
Emergency Department that has acute and day only beds, and
Service there is a helipad on site.
Capability: CSCF Level 3
Services: The Ayr Health Service provides a range of inpatient and
outpatient services including: acute care, birthing, endoscopy,
emergency, surgery, clinics, Aboriginal and Islander health, nursing
discharge liaison, community mental health, child health,
physiotherapy, medical imaging, speech therapy, occupational
therapy, social work and pharmacy.
Location: Home Hill Health Service is a rural health service located
100 kilometres south of Townsville, and 12 kilometres south of the
neighbouring town of Ayr.
Size: Home Hill Health Service has a 13 bed inpatient unit, one
Home Hill dedicated palliative care bed, outpatient clinics, a physiotherapy and
Health Service occupational therapy room, one minor procedural room and a
private medical practice. An eight chair renal unit that operates as
an outreach service from The Townsville Hospital is also located here.
Capability: CSCF Level 2.
Services: Services provided include generalist nursing care for
inpatients with a broad range of health care needs. The emergency
service is a 24-hour nurse led emergency triage, with patient’s
requiring medial assessment transferred to Ayr.
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 16Location: Charters Towers Health Service is a rural health service
located 135 kilometres west of Townsville.
Size: Charters Towers Health Service has a two-bed Emergency
Charters Towers Department space with 23 inpatient beds. When required the health
service can provide for imminent birthing and procedural capacity.
Health Service
Capability: CSCF Level 3
Services: A range of services are provided including emergency,
acute inpatient, low-risk procedural, all-risk caseload group
midwifery practice (ante- and post-natal), community health, child
and family and school based youth health services. Outreach
nursing clinics including diabetes, women’s health and renal
health services as well as visiting specialist medical clinics
(cardiac, paediatric, gastroenterology and surgical) are provided
from TTH .
Location: Hughenden Multi-Purpose Health Service (MPHS) is
246 kilometres west of Charters Towers, 517 kilometres from
Mount Isa and is 384 kilometres from Townsville.
Hughenden Size: Hughenden MPHS has nine acute beds and six high-care
Multi-Purpose aged care flexible beds.
Health Service Capability: CSCF Level 2.
Services: The MPHS provides an integrated acute and community
health service, including Aboriginal and Torres Strait Islander
community health. Emergency care is available 24hours per day.
Ambulatory clinics are conducted Monday – Friday. There is no
outpatient clinic, all patients requiring access to a Doctor are
referred to the private practice conducted by the Medical
Superintendent (the exception being after hours or accident and
emergency care). There is no birthing service or operating theatre,
however pre-natal and post-natal care is available from the MPHS
midwife in partnership with the General Practitioner and TTH.
Location: Richmond is the midpoint between Townsville and
Mount Isa (approximately 500 kilometres from both centres).
Size: Richmond Health Service has 10 acute available beds,
Richmond including four long stay nursing home type beds.
Health Service Capability: CSCF Level 2.
Services: Richmond Health Service provides a range of services
including emergency care 24/7 to CSCF level 2, Queensland
Ambulance services 24/7, general medical/surgical and paediatric
services and Aboriginal and Torres Strait Islander community
health. General x-ray services are limited but available via
licensed operators.
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 17Location: The Joyce Palmer Health Service (JPHS) is located within
the Aboriginal and Torres Strait Islander community of Palm Island,
70 kilometres north of Townsville - off the coast near Ingham.
Joyce Palmer Size: The JPHS consists of an emergency department and a 15 bed
Health Service general ward. Outpatient clinics are provided. A four chair renal
dialysis outreach unit from TTH is also located here.
Capability: CSCF Level 2
Services: During 2016, the JPHS provided health services to over
3,500 Palm Island people, including all non-critically ill patients
who may be neonates, children, adults and aged care. Services
include emergency services, general management of medical and
aged patients, minor surgical procedures, outpatient clinics, basic
radiography, pathology sample collection, antenatal and postnatal
care, pharmacy, child health, men’s and women’s business, mental
health, oral health, and wound clinic. A number of visiting
specialists conduct regular clinics with the facility.
Location: Ingham is located 110 kilometres north of Townsville.
Size: The Ingham facility has a 28 bed inpatient unit with a
dedicated birth suite and two palliative care beds, an emergency
Ingham Health unit with a two bay resuscitation area and two bed consult. There
is an operating suite with two procedural rooms, preadmission
Service and Post Anaesthetic Care Unit (PACU) areas, and medical
imaging. The facility also has a community services wing which
includes oral health services, allied health services with a
rehabilitation gym and Activities of Daily Living (ADL) kitchen,
mental health services, midwifery services and Aboriginal and
Torres Strait Islander services.
Capability: CSCF Level 3
Services: Inpatient care is provided to patients with a broad range
of health care needs ranging from cardiac monitoring, paediatrics,
aged care, rehabilitation, general medicine, oncology, birthing,
physiotherapy, occupational therapy, speech pathology, dietetics,
social work, Aboriginal and Torres Strait Islander health and
palliative care. The emergency area provides services 24
hours/day. The operating suites are used regularly for elective lists
by visiting general surgeons and gastroenterologists. Pharmacy
services provide both inpatient and outpatient services, and
medical imagining provides x-ray services Monday to Friday, with
on call capacity and weekly ultrasound clinics. There are also a
range of outreach specialist clinics provided on a regular basis,
including Aboriginal and Torres Strait Islander health services.
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 18In addition to the hospital-based services and facilities, the THHS also provides a large number of
community-based services from which a range of mental health, Aboriginal and Torres Strait Islander health,
community health, child health and aged care services are delivered:
Cambridge Street Health Campus
Cardwell Community Clinic
Community- Charters Towers Rehabilitation Unit
based services Eventide Residential Aged Care Facility
Garbutt Facility of Townsville Aboriginal and Islanders Health
Services (TAIHS)
Josephine Sailor Adolescent Inpatient Unit and Day Service
Kirwan Health Campus
Townsville Community Care Unit and Acquired Brain Injury Unit
Magnetic Island Community Clinic
North Ward Health Campus
Palmerston Street Health Campus
Parklands Residential Aged Care Facility
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 19Planning for
the Future
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 204. Managing demand for hospital services by
changing models of care
4.1 Planning Information
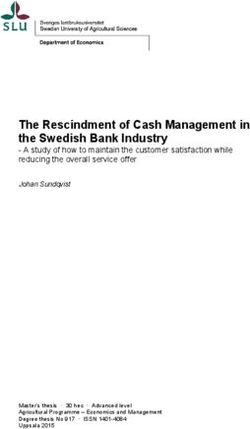
The Queensland Department of Health Acute is projected to grow by more than four per
Inpatient Modelling (AIM) methodology has an cent per annum over the next 20 years.
inbuilt assumption that decreases in overnight
length of stay across almost all clinical By 2036, people aged 70 and over, will
specialties will continue. For Townsville HHS make up more than 14 per cent of the total
facilities, overnight average length of stay is Townsville HHS population but will account
projected to decrease over the next 20 years for approximately 55 per cent of all overnight
from 5.5 to 4.7 days for adults and from 2.9 to beddays for Townsville HHS residents in
2.3 days for children. Townsville HHS hospitals.
Despite this, the AIM tool projects large The percentage of overnight separations for
increases in the volume of overnight beddays people aged 70 and over will increase across all
from Townsville HHS facilities for medical, specialty groups with cardiology/cardiothoracic
surgical/procedural and subacute services and surgical/procedural services expected
driven by population growth and ageing. to have the largest percentage of overnight
The Townsville HHS population aged 70 and over separations of older people.
Overnight ALOS by specialty: Townsville HHS facilities, adults
25.0
15.0
10.0
6.0
5.0 2014/15
2026/27
4.0
2036/37
3.0
2.0
1.0
0
Surgical/Proc Cardiology/ Medical Sub Acute Obs & Gynae Neurosciences
Cardiothoracic
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 21Overnight beddays by specialty: Townsville HHS facilities, adults
100,000
80,000
2014/15
60,000 2026/27
2036/37
40,000
20,000
0
Medical Subacute Surgical/Proc. Cardiology/ Neurosciences Obs & Gynae.
Cardiothoracic
100%
25%
33%
Use of Townsville HHS hospitals by 80%
40%
49%
40%
age group: Overnight separations 55%
and beddays 60%
Aged 70+ ON Beddays 40% 75%
67% 60%
60%
AgedTOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 23
4.2 Planning Considerations
There are many different models of care Changes To Models of Care “Outside the Walls”
known to reduce overall demand for hospital
services or reduce the length of time spent in Expansion of community based care - “Many
hospital that are both relevant and feasible to front doors”
implement (or expand) in Townsville HHS. Improving access to community-based
and home-based services via a model that
These models focus on ways to avoid or creates “many front doors” is a key strategy.
substitute for acute hospital inpatient stays There are many opportunities for community
by providing services differently “outside the health services to be the central entry point
walls” of a hospital or on improving patient for patients requiring treatment for a wide
flow “within the walls” of the hospital. range of health conditions, particularly
Changes to models of care particularly target for management of chronic illnesses and
services for the frail aged and people with rehabilitation services.
chronic disease and will have the largest
impact on TTH. A model that increases direct access to
community-based services will require
It is increasingly recognised that traditional significantly more capacity for both nursing
hospital based models of care may not and allied health services in community
provide optimal health outcomes particularly settings, streamlined referral pathways and
for older people and those with multiple heightened consumer awareness of the
chronic disease. Robust evidence exists to services available.
support providing acute care outside the
acute hospital setting. A 2012 meta-analysis At the same time, it is important to expand
found that hospital in the home (HITH) diversion programs from the Emergency
services resulted in reduced mortality, a Department (ED) for example by implementing
reduction in hospital readmission and greater initiatives such as a Geriatric Emergency
patient satisfaction as well as lower costs.1 Department Intervention (‘GEDI’) nurse
model and increasing the role of allied health
Data from the Australasian Rehabilitation within the ED. A close working relationship
Outcomes Centre Annual Report 2015 shows with hospital discharge planners and strong
that provision of rehabilitation in Australia support from private and non-government
grew in volume by 6.3 per cent in 2015 community health services and General
compared to the previous year with the Practitioners is also essential.
majority of that growth coming from the
“reconditioning impairment” group. Given
Expanding Hospital in the Home (HITH) /
that the highest priority for an older person is
Hospital in the Nursing Home (HINH)
to maintain independence and mobility, the
need for reconditioning services suggests that There is the potential to grow the adult
this is increasingly a challenge for busy acute HITH service and to establish a service for
hospitals in caring for the growing number of paediatrics in the future. The preferred model
frail aged people with complex clinical, care for HITH services would be a single point of
and support needs. The challenge is therefore entry for referral coordination and triage.
to implement models that deliver coordinated, There would be a focus on care within the
person-centred care preferably outside of an person’s own home wherever possible with
acute inpatient ward wherever possible. additional support from telehealth and remote
1
Caplan, G. A., Sulaiman, N. S., Mangin, D. A., Aimonino Ricauda, N., Wilson, A. D., & Barclay, L. (2012). A meta-analysis of “hospital
in the home”. Med J Aust, 197(9), 512-9.
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 24monitoring technology. An alternative would Palliative Care in the Community
be presentation to a community health campus The Grattan Institute Dying Well Report in 2014
if the patient’s place of residence is unsafe highlighted that surveys consistently show
or out of range. Service provision could be by between 60 and 70 per cent of Australians
Townsville HHS or by a contracted partner. would prefer to die at home with hospitals
and residential care being their least preferred
HITH separations currently account for just places to die2. Yet today only about 14 per
over 1 per cent of total separations from TTH. cent of people die at home, 54 per cent die in
Increasing this progressively to 3 per cent hospitals and 32 per cent in residential care
by 2021 - 2022 would have the potential to in Australia.2 Stakeholders advise that these
reduce the need for additional overnight beds statistics are similar for Townsville and there is
at TTH by at least 37 beds in 2036 - 2037. significant opportunity to better utilise home-
based services to reduce admissions to hospital.
Closing the Gap for Aboriginal and Torres
Strait Islander Health - Integration with The vision is for TTH to take a lead role for the
Primary Care planning and coordination of palliative care
The vision for Aboriginal and Torres Strait services. Strategies include providing support
Islander Health services is to support to the ED in order to reduce potentially
holistic / wrap-around primary care services preventable admissions and develop a care
in order to address chronic disease within plan for palliative patients. The role would
the population as early as possible. The also involve providing support for other non
overarching goal is to take a proactive Townsville HHS services to increase home-
approach to avoid hospitalisation, for chronic based care. Providing assistance to nursing
disease conditions to be managed as much homes to plan and deliver palliative care
as possible in the community primary care would be a priority.
space and to strengthen partnerships with
Aboriginal Medical Services within the region. Investment in home-based palliative care
The priorities for change are detailed further services would have a direct impact on
in the next section of this Plan. reducing the number of patients receiving
2
Broad, et al. (2013) as cited in Swerissen, H and Duckett, S., 2014, Dying Well. Grattan Institute
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 25such care in hospital. It is estimated that even Same-Day Geriatric Management Unit
reducing the percentage of hospital-based Expanding the same-day geriatric
palliative care separations in TTH by only 30 management unit to include the establishment
per cent could result in 11 beds less than the of a “day hospital” service for Geriatric
projected requirements needing to be built by Evaluation and Maintenance (GEM) patients
2036 - 2037. would reduce both the number of admissions
and length of stay for older patients. The
Improving Patient Flow “Within the Walls” new subacute care unit at TTH is a suitable
The Acute Medical Unit concept location for GEM day rehabilitation. The current
model for community-based rehabilitation is a
Shortening overnight length of stay for adult
brokered service to a community organisation
medical patients by expanding the scope
or services provided through the Transition Care
of the existing Acute Assessment Unit to
Program and has limited capacity. The model
an acute medical unit (AMU) model is a
would be dependent on effective links with
priority. AMUs are staffed by multidisciplinary
general practitioners for referring and sufficient
medical, nursing and allied heath teams. The
access to community-based nursing and allied
model of care is that once initial assessment
health to support discharge from the program.
is completed, a plan is developed which
may include a short period of time under
Creation of an Orthogeriatric Unit
observation/receiving treatment in the AMU,
admission into the wider hospital under the The large projected growth in the ageing
care of another specialty team if necessary, population will place significant demand
or home to continue care in the community. on orthopaedic services in the future. The
A close working relationship with hospital consequences of falls in these patients is
discharge planners and strong support from major as they will be increasingly frail and
private and non-government community likely to have multiple co-morbidities. An
health services and general practitioners is orthogeriatric model of care is preferred with
therefore essential. orthopaedic surgeons and geriatricians jointly
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 26providing comprehensive medical assessment accommodation in Townsville for diagnostic
and treatment supported by specialist nursing testing and pre-operative workup. One option
and allied health staff. to address this issue is to more extensively use
nurse navigator roles to coordinate services
Paediatric Short Stay Unit particularly for cancer and cardiothoracic
patients. However, capacity and coordination
The paediatric ED service is staffed by of the diagnostic services is also a contributing
generalist medical and nursing staff and does factor to increased length of stay.
not currently have a dedicated paediatric
short stay unit. Shortening length of stay for
children in an acute hospital environment Alternative settings for the care of non-acute
is highly desirable both for the child and patients awaiting nursing home placement
to reduce disruption for the family who are In TTH, there are significant numbers of non-
providing support. Implementation of a short acute patients, many of whom are waiting
stay unit model is known to further assist in transfer to residential care and no longer
reducing length of stay for children. need the level of acute care provided in a
hospital environment. Addressing this issue
Dedicated Mental Health/ Alcohol, Tobacco would be reliant on the availability of out-of-
and Other Drugs (ATODS) units for special hospital services, potentially entering into
needs groups. partnerships with local aged care providers,
or utilising other existing HHS facilities in new
xx Creation of a dedicated acute older ways. An option may be to seek to increase
persons unit within the additional bed the availability of the Australian Government-
allocation for adult acute mental health subsidised Transition Care Program for older
xx Allocation of dedicated drug and people who have been in hospital. Transition
alcohol detoxification beds within one care may be provided in their own home, in
of the medical units to address the a ‘live-in’ setting such as part of an existing
current issue of these patients being aged care home or a health facility such as the
distributed throughout the hospital separate wing of a hospital.
xx Expansion of the eating disorders Finding an alternative care setting for non-
services to increase community acute patients has the potential for up to 39
alternatives to care and to support additional beds that would not need to be
more children to transition to adult built by 2036 - 2037.
services once they are aged 18
xx Creation of a Family Unit for treatment Streamlining outpatient services
of mothers and babies and for children
aged 0 - 11 years. Changing models of care will also impact
on demand for outpatient services. The
management of chronic complex care will be
Coordination of access to Diagnostic (and increasingly reliant on non-admitted care and
other support) Services co-ordination between primary, community
The difficulty of coordinating access to acute and subacute services. Some current
diagnostic services for patients with complex clinics may not need to be delivered in future
conditions is often the cause of increased or be delivered in a non-hospital setting. For
length of stay by admitting otherwise “well” many services, the trend will increasingly be
patients for workup prior to surgery or to deliver multidisciplinary clinics in a more
other interventions. This is a particularly person-centred model. The use of digital
important issue for a hospital such as TTH technology will have a major impact on
where large numbers of patients come from models of service delivery.
outside the immediate area and also require
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 27It is therefore important to review models Within TTH, a range of changes to the way
of care and undertake pathway and process services are organised:
redesign to streamline outpatient processes
prior to modelling future demand for xx Expansion of the concept of the Acute
outpatient services. Medical Unit (AMU) model of care at
TTH
4.3 Priority Planning Actions xx Expansion of the Same Day Geriatric
Management Unit at TTH
Initiatives specifically aimed at reducing xx Creation of an Orthogeriatric Unit
length of stay and hospital admissions
xx Establishment of a dedicated acute
include:
older person’s mental health unit
xx Expansion of community based care
within the additional bed allocation for
including nursing and allied health
adult acute mental health
xx Implementation of hospital avoidance /
xx Allocation of dedicated drug and
hospital diversion programs from the ED
alcohol detoxification beds
xx Increasing HITH /HINH for adults
xx Creation of a Family Unit for mental
xx Introducing HITH for paediatric patients health treatment of mothers and babies
(commencing with services for children and for children aged 0 - 11 years
aged 12 years and over)
xx Establishment of a Paediatric Short
xx Further integration with primary care Stay Unit
services for Aboriginal and Torres Strait
xx Increasing day of surgery admission
Islander peoples
rates by addressing access to
xx Expanding palliative care services and diagnostic services
increase support for home-based care.
xx Identifying appropriate alternative
settings for the care of non-acute
maintenance-type patients who are
waiting nursing home placement.
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 285. Closing the gap in health outcomes for
Aboriginal and Torres Strait Islander peoples
5.1 Planning Information
Hospitalisation rates for the Townsville HHS of hospital separations from Townsville HHS
Indigenous population are high. The Closing facilities are for Indigenous people. For renal
the Gap Performance Report 2016 shows that dialysis, Indigenous patients account for 57
Townsville HHS had the highest Indigenous per cent of separations.
age standardised rate per 1,000 persons for
all cause hospital separations in Queensland Surgical/procedural services account for
for the period 2011 - 2012 to 2015 - 2016.3 the largest volumes of overnight beddays
for Indigenous persons in Townsville HHS
Excluding renal dialysis, around 15 per cent facilities.
Mortality (ASR/100,000 (deaths) 2009-2013) Separations (ASR/1,000 (seps/year) 2011/12-2015/16)
Gap: 22 Gap: 745
QLD: 964 Townsville QLD: 836 Townsville
HHS: 986 HHS: 1,581
Indigenous beddays by specialty: THHS facilities, all ages
40%
Renal Dialysis Separations
Indigenous
30% 43% Non-Indigenous
57%
20%
10%
0%
Surgical/Procedural Cardiology/Cardiothoracic Obstetrics/Gynaecology
Subactute Medical Neurosciences
3
Queensland Health. (2017). Closing the Gap performance report 2016. Retrieved from http://www.health.qld.gov.au
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 29Shortened life expectancy is highlighted by Use of hospital services by age group is different
only two per cent of Indigenous Townsville for Indigenous and non-Indigenous Townsville
HHS residents being over 70 years of age HHS residents. The 0 - 14 year age group
compared to nine per cent for the non- represented 16 per cent of inpatient separations
Indigenous population. In contrast, people for Indigenous persons compared to only eight
aged under 24 years of age make up over 55 per cent for the non-Indigenous persons. In
per cent of the Townsville HHS Indigenous contrast, only six per cent of total separations
population compared to only 35 per cent of for Indigenous persons were for people aged 70
the non-Indigenous population. and over compared to 27 per cent for the non-
Indigenous population.
Townsville HHS population pyramid, 2015: Indigenous and Non-Indigenous
Non-indigenous
85+
80-84 Indigenous
75-79
70-74
65-69
60-64
55-59
50-54
45-49
40-44
35-39
30-34
25-29
20-24
15-19
10-14
5-9
0-4
15% 10% 5% 0% 5% 10% 15%
% of population
Indigenous separations by facility: Indigenous separations by age group:
Townsville HHS facilities, all ages Townsville HHS facilities
Indigenous
100%
75%
16% 47% 32% 6%
50%
20%
15%
Non-Indigenous
10%
8% 30% 34% 27%
5%
0%
0-14 5-44 45-69 70+
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 305.2 Planning Considerations consultation is the need to travel to Townsville
for specialist medical services and hospital
admission which further compounds the social
Consultation with key stakeholders in and economic difficulties for the community.
Townsville HHS identified the vision for Many patients who must come to Townsville
Aboriginal and Torres Strait Islander Health regularly for treatments such as renal dialysis
is to support the provision of holistic, wrap- have to relocate but frequently do not have any
around primary care services in order to suitable accommodation in Townsville.
address chronic disease within the population
as early as possible. The overarching goal is It is well known that lifestyle-related diseases
to work in partnership with other providers are potentially preventable by addressing
to take a proactive approach to avoid underlying factors including intergenerational
hospitalisation, and for chronic disease trauma and the social and economic
conditions to be managed as much as possible determinants of health. This requires effective
in the community primary care space and cross-sectoral responses many of which lie
to strengthen partnerships with Aboriginal outside the direct scope of a health service.
Medical Services within the Region. Strong partnership approaches are therefore
required between Townsville HHS and:
The high rates of hospitalisation for the xx Townsville Aboriginal and Islanders
Aboriginal and Torres Strait Islander population Health Services (TAIHS) community
that are the result of chronic diseases such controlled primary healthcare
as diabetes, cardiovascular, mental health services (General Practice (GP) and
and chronic kidney disease are consistently multidisciplinary services) to increase
highlighted in every planning process. It is the level of service integration with
commonly known that the Aboriginal and TTH. The vision is for a “service hub”
Torres Strait Islander community are less where the two organisations work
likely to regularly use general practice or other together seamlessly from the same
primary healthcare services. For this reason, physical location. Better integration
they are often sicker when they make first also includes TAIHS health workers
contact with the acute hospital sector, thereby at TTH to support patient transition
increasing the likelihood of needing hospital back into the community, better use of
admission. Many also use hospital emergency technology and overcoming barriers to
departments rather than general practices for information sharing. Responsibility for
ease of access and financial reasons but this case management is an issue still to be
further reduces the likelihood of accessing resolved in terms of who takes the lead
co-ordinated person-centred chronic disease in managing the ongoing care of this
management programs. patient cohort.
The recorded high rates of hospitalisation xx Northern Queensland Primary Health
must also be considered in the context Network to coordinate services for rural
that identification of Aboriginal and Torres and remote areas. Fragmentation and
Strait Islander people in health datasets duplication of services is an ongoing
is unreliable and considered to be an problem particularly in areas with
underestimate. Staff are trained to always ask significant volumes of visiting and
if the patient identifies as Aboriginal or Torres outreach services. A key role of the
Strait Islander but in practice this does not local health worker is to link people
consistently occur. with services, ensure that they are
culturally appropriate and support
An issue consistently raised through access to programs such as health
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 31TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 32
checks. Strengthening the role of the hearing health, oral health, rheumatic heart
local Indigenous health worker by disease and developmental issues.
working closely with nursing and allied
health staff to develop and implement Chronic illness prevention and management:
consistent management pathways will Early detection and intervention particularly
be important. for diabetes, chronic kidney disease and
cardiovascular disease needs to be a priority.
xx Palm Island Aboriginal Shire Council
System-wide changes to the approach to care
to implement the Palm Island Health
are required so that risk factors are identified
Action Plan 2017-2027 and develop
early and chronic illness is then managed by a
comprehensive primary health care
multidisciplinary team. This needs to include an
for Palm Island residents. The major
emphasis on services for children and families
priority of the action plan is to build
to address pre-disposing factors that may be
a community-controlled new primary
present from before birth and in early childhood.
healthcare service for Palm Island
which will offer general practice and
Sexual Health: Increased rates of syphilis and
non-acute multidisciplinary primary
a growth in Sexually Transmitted Infections
health care services. The Joyce Palmer
(STI) is occurring across northern Queensland
Health Service will continue to provide
and is a critical issue for Aboriginal and Torres
emergency care, inpatient care, renal
Strait Islander communities. Implementation
dialysis, high needs aged care and
of the community based actions contained in
pharmacy services.
the North Queensland Sexual Health Strategy
2016 – 2021 will be important during the
Specific services identified as needing further
planning period.
development within Townsville HHS include:
Child and youth health services: The scope of Care of older people and people with
child health interventions needs to be expanded disabilities: Older people and people with
to include proactive engagement of families with disabilities who have high-care needs
older children. There also needs to be improved frequently have to be moved to Townsville
access to specialist services for children for and separated from family. This is particularly
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 33an issue on Palm Island as it is repeating the controlled primary healthcare services
cycle of forced removal and trauma which
xx Work in partnership with the Palm
brought their families to Palm Island in the
Island Aboriginal Shire Council to
first place. The proposal to reorient the Joyce
implement the Palm Island Health
Palmer Health Service to a multipurpose
Action Plan 2017 - 2027 and establish
facility would enable people with high-care
the new community controlled primary
needs to remain on Palm Island.
healthcare service
Birthing services: Birthing in community xx Work closely with Northern Queensland
is consistently raised by communities and Primary Heath Network to improve service
is particularly an issue for Palm Island. To coordination in rural and remote areas
reintroduce birthing on Palm Island would
xx Strengthen the Townsville HHS
require significant action by individuals,
Indigenous health worker role by
families and the health service to address
working in close collaboration
risk factors in pregnancy including smoking,
with nursing and allied health staff
substance misuse and gestational diabetes
particularly in the smaller rural and
and reduce the large number of high risk
remote facilities to implement care
pregnancies. Workforce and infrastructure
pathways
issues would also need to be addressed to
enable low-risk birthing to be re-established. xx Expand local access to specialist
outpatient clinics by increased
Across all services, cultural capability training outreach and telehealth
for all staff is a vital contributing factor to
xx Further develop culturally appropriate
improving service delivery.
targeted programs particularly for child
and youth health, sexual health and
5.3. Priority Planning Actions chronic disease management
xx Ensure all staff have participated in the
xx Develop a collocated service model cultural capability training program.
between TTH and TAIHS community
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 346. Making better use of Townsville HHS rural and
remote services
6.1 Planning Information
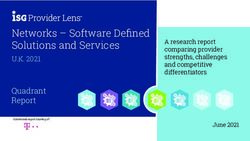
Rural and remote facilities in Townsville HHS Charters Towers, Ingham and Northern
are located at Ayr, Ingham, Charters Towers, Highlands residents are provided by their
Home Hill, Hughenden, Richmond and Palm local hospitals. Local provision of medical
Island (Joyce Palmer Health Service). Ayr, services for areas surrounding the rural hubs
Ingham and Charters Towers have rural hub ranges between 77 per cent and 79 per cent.
roles (CSCF level 3). Local provision of surgical services by the
three rural hub facilities is considerably lower
The percentage of people aged 70 and over between 41 per cent and 49 per cent.
residing in the rural areas of Townsville HHS is
projected to increase significantly. Seven of the top 10 specialties for which rural
Townsville HHS residents flow to TTH are for
Between 50 per cent and 60 per cent of surgical, procedural or obstetric services.
hospital separations for residents of Burdekin,
Planning regions and facilities
Joyce Palmer
Ingham Health Service
Hospital
The Townsville
Hospital Ayr Hospital
Home Hill
Hospital
Charters Towers
Hospital
Richmond
Hospital
Hughenden
Hospital
CSCF level 6 CSCF level 2 Hinchinbrook Burdekin
CSCF level 3 Charters Towers Northern Highlands Townsville
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 35Rural population proportions Top 10 SRGs to TTH
Burdekin Charters Towers
2016
Hinchinbrook Northern Highlands
2026
2036
2016
2026
2036
2016
2026
2036
2016
2026
2036
0-14 15-44 45-69 70+
Rural flows to TTH
41%
Joyce Palmer
Ingham
Health Service
Hospital
The Townsville
Hospital
Ayr Hospital
Home Hill
Hospital
38%
Charters Towers
49% Hospital
Richmond
Hospital 41%
Hughenden
Hospital
Local hospitals Burdekin Hinchinbrook Townsville
Flows to TTH Charters Towers Northern Highlands
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 366.2 Planning Considerations
Rural and remote facilities are located at From a service planning perspective, the ‘hub
Ayr, Ingham, Charters Towers, Home Hill, and spoke model’ aims to strike a balance
Hughenden, Richmond and Palm Island between addressing community desires and
(Joyce Palmer Health Service) and operate expectations for local, safe and sustainable
under a ‘hub and spoke’ model involving service delivery, and a need to maximise the
three hub hospitals: capacity of available infrastructure within
rural and remote facilities thereby reducing
xx Charters Towers Hospital, a 23 bed
the need for additional infrastructure at TTH.
facility with six bed alternatives
located 140 kilometres south-west of
There is capacity to increase service
TTH (approximately 90 minutes travel
capability and local self-sufficiency through
by road)
further development of a hub and spoke
xx Ingham Hospital, a 28 bed facility model based on rural hubs (i.e. CSCF Level
located 115 kilometres north of TTH (75 3 facilities) at Ayr, Ingham and Charters
minutes travel by road) Towers. Service areas to target include day
surgery, endoscopy, emergency, inpatient,
xx Ayr Hospital, a 28 bed facility located
low-risk maternity, rehabilitation and
90 kilometres south of TTH (60
palliative care.
minutes travel by road).
‘Hub’ sites are expected to provide core A contemporary model of care at a rural hub
services, comprising surgical and procedural, requires:
maternity, emergency and general medical,
at Level 3 Clinical Services Capability xx Restored focus on the core secondary
Framework (CSCF) v3.2. health services (day surgery,
endoscopy, emergency, inpatient,
Townsville HHS’s rural hospitals are pivotal low-risk maternity, rehabilitation and
to the delivery of health care to people in palliative care)
rural and remote communities, and provide xx A fully-functional rural hub that is
a range of general medicine, general surgery, digital-hospital ready, and provides
obstetrics, emergency, outpatient, primary a range of Level 3 services closer to
health and community services. home
Rural-based community stakeholders xx Improved collaboration with primary
consistently expressed a desire for the and community-based healthcare
following: providers, resulting in enhanced
coordination of care for patients with
xx Services to be provided for the chronic conditions and long-term
community, in the community needs
xx Efficient service delivery models xx Person-centred pathways that improve
xx Person-centred models of care accessibility to services, enable more
efficient staff and patient flows, are
xx Increased use of ICT and other health supported by clinically appropriate
technologies to support and improve and respectful treatment environments
local service provision and leverage the benefits of
xx To consider new models for supporting enhanced radiology and point of care
workforce attraction and retention. technologies.
TOWNSVILLE HOSPITAL & HEALTH SERVICE Health Service Plan 2018 – 2028 Page 37You can also read