Fluorescent quantitative PCR detection of Mycobacterium tuberculosis in tissue sections from granulomatous lesions retrieved using EDTA - RBC ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Downloaded from http://jcp.bmj.com/ on October 11, 2016 - Published by group.bmj.com
JCP Online First, published on September 29, 2016 as 10.1136/jclinpath-2016-203738
Original article
Fluorescent quantitative PCR detection
of Mycobacterium tuberculosis in tissue sections
from granulomatous lesions retrieved using EDTA
Xuzhou Wang, Feilai Xie, Qiaoling Zheng, Xingfeng Qi, Min Li, Xiaoling Zhou,
Zhiyong Zheng
▸ Additional material is ABSTRACT which the prevalence of TB with positive sputum
published online only. To view Aims This study aimed to use EDTA to retrieve paraffin- smears was 66/0.1 million and the prevalence of
please visit the journal online
(http://dx.doi.org/10.1136/ embedded tissue sections of inflammatory granulomatous bacteria-positive TB was 119/0.1 million. So, the
jclinpath-2016-203738). lesions and increase the detection rate of tuberculosis epidemic situation was still very serious.2
(TB)/non-tuberculous mycobacteria. Due to the influence The pathological diagnosis was thought to be the
Department of Pathology,
Dongfang Hospital, Fujian of chemical reagents during the fixation process, the standard for TB diagnosis, but atypical tuberculous
Medical University, Fuzhou, amplification of fluorescent quantitative PCR was blocked lesions appeared frequently in the daily workup,
China after DNA extraction, and the results were not ideal. which needed to be differentiated from other
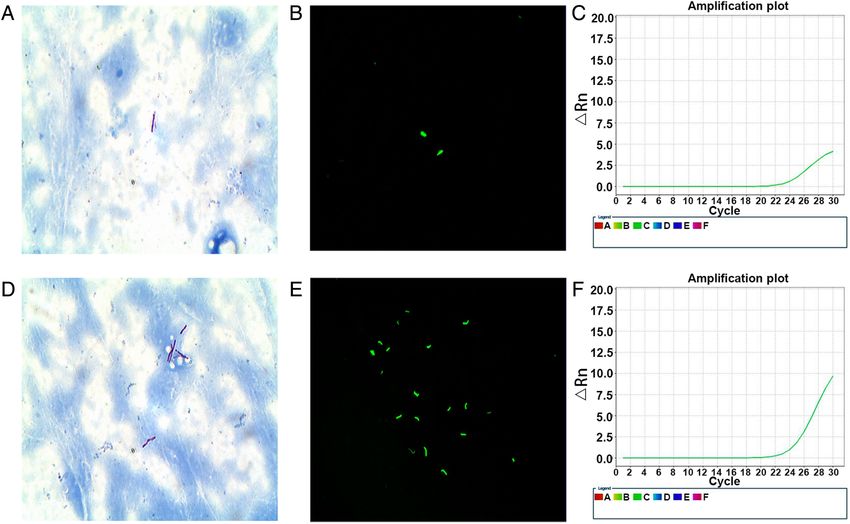
Methods Special staining technologies (acid-fast and lesions such as sarcoidosis, Crohn’s disease and
Correspondence to
Dr Zhiyong Zheng, Department Auramine O) and fluorescent quantitative PCR were used fungal granuloma. The use of acid-fast and
of Pathology, Dongfang to detect TB/non-tuberculous mycobacteria in 125 cases Auramine O staining or fluorescent quantitative
Hospital, Fujian Medical of inflammatory granulomatous lesions in paraffin- PCR to detect M. tuberculosis could provide
University, Fuzhou 350025 embedded tissue sections with and without EDTA powerful evidence in the pathological diagnosis of
China; 768203566@qq.com
retrieval. atypical tuberculous lesions.
Received 17 March 2016 Results In 125 cases of inflammatory granulomatous The use of acid-fast and Auramine O staining
Revised 3 September 2016 lesions, 75 cases (60%) were positive for mycobacteria showed the detection rate of tuberculous mycobac-
Accepted 11 September 2016 using fluorescent quantitative PCR without EDTA teria was lower. The detection rate of TB was 31%–
retrieval, of which 74 cases (59.2%) were detected with 50.1% and 40.5%–65.7% using Ziehl-Neelsen acid-
TB mycobacteria and 1 case (0.8%) with non- fast staining and Auramine O staining, respect-
tuberculous mycobacteria. The average cycle threshold ively.1–5 The detection rate of tuberculous mycobac-
value of positive specimens ranged from 29 to 32 teria using fluorescent quantitative PCR in frozen
(30.5). However, 88 cases (70.4%) were positive for tissue sections of TB lesions was up to 75.8%.6–8
mycobacteria using fluorescent quantitative PCR with However, the tuberculous mycobacteria detection
EDTA retrieval, of which 83 cases (66.4%) were rate was just 50%–60% when the same method was
detected with TB mycobacteria and 5 cases (4%) with used in the tissue sections of granulomatous lesions
non-tuberculous mycobacteria. The average Ct value of that were formalin fixed and paraffin embedded.3
positive specimens ranged from 27 to 30 (28.0). Sometimes tuberculous mycobacteria could not be
Statistical differences were found between the two detected in paraffin-embedded specimens of typical
groups ( p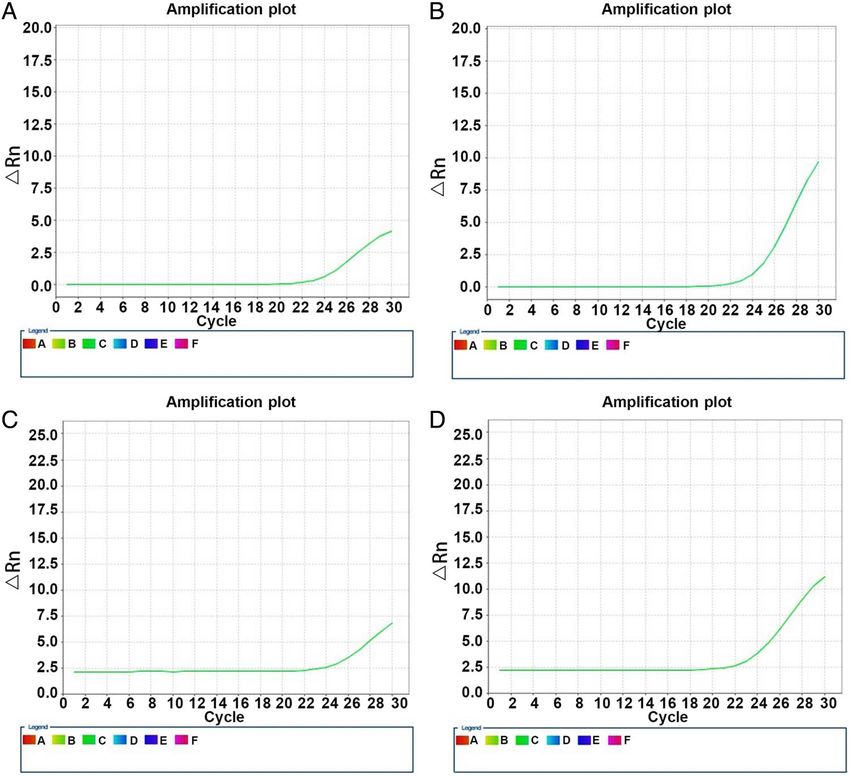
Downloaded from http://jcp.bmj.com/ on October 11, 2016 - Published by group.bmj.com
Original article
tissue sections.4 5 The antigen retrieval could open the tissue for 5 min at room temperature, the supernatant was discarded.
protein cross-linking caused by formalin fixation and signifi- The remnant was vortexed after adding 1 mL of anhydrous
cantly increase the detection rate of IHC.6 To verify that the ethanol. The supernatant was again discarded after centrifuging
EDTA heat-induced retrieval could improve the mycobacterial for 5 min at room temperature. The precipitate was dried at
detection rate using fluorescence quantitative PCR, M. tubercu- room temperature or 37°C. Then, 400 mL of buffer and 20 mL
losis was detected in this study using fluorescent quantitative of proteinase K were added to the precipitate. The mixture was
PCR in paraffin-embedded tissue sections of granuloma lesions incubated for 100 min at 56°C and 30 min at 90°C, cooled to
retrieved with EDTA, and compared with the results of routine ambient temperature and then transferred to the magnetic bead
fluorescence quantitative PCR. extraction apparatus for extracting DNA after filtering.
This study attempted to introduce antigen retrieval into the
process of fluorescent quantitative PCR and acid-fast and
Auramine O staining, and hoped to increase the detection rate Florescence quantitative PCR detection after EDTA heat-induced
of TB/non-tuberculous mycobacteria. The samples were put into retrieval
an Eppendorf (EP) tube, dewaxed and retrieved with EDTA; Ten 6 mm sections were put into an EP tube, and 1 mL of
then, DNA was extracted, and fluorescence quantitative PCR xylene was added for dewaxing. After mixing for 10 s and cen-
detection was carried out. Also, acid-fast staining and Auramine trifuging for 5 min at room temperature, the supernatant was
O staining were performed after heat-induced retrieval of the discarded. The remnant was vortexed after adding 1 mL of
samples with EDTA. The results showed that heat-induced anhydrous ethanol. The supernatant was again discarded after
retrieval with EDTA could greatly increase the detection rate of centrifuging for 5 min at room temperature. The precipitate was
TB/non-tuberculous mycobacteria. dried at room temperature or 37°C. Then, 1 mL of EDTA
retrieval liquid was added to the precipitate. The mixture was
METHODS put in a metal bath (95°C) for 10 min. The supernatant was dis-
Samples carded after centrifuging the mixture for 5 min at room tem-
A total of 125 specimens of tuberculous granuloma with H&E perature; 1 mL of distilled water was added for washing. The
staining were collected from February 2014 to May 2014 in the supernatant was again discarded after centrifuging for 5 min.
Department of Pathology of the Fuzhou General Hospital of Then, 400 mL of buffer and 20 mL of proteinase K were added
Nanjing Military Command. This study was approved by to the precipitate. The mixture was incubated for 100 min at
Fuzhou General Hospital ethics committee. It included 83 males 56°C and 30 min at 90°C, cooled to ambient temperature and
and 42 females with the mean age of 45.3 years (range 26–
65 years). The specimens were taken by lung puncture or bron-
chial fiberscope biopsy (58 cases), lymph node biopsy (52 Table 1 Comparison between mycobacterial detection results of
cases), lung resection (10 cases) and skin biopsy (5 cases). fluorescent quantitative PCR and acid-fast and Auramine O staining
Lymph node tissues of non-granulomatous lesions (30 cases) in 125 cases of inflammatory granuloma
were used as the negative control. Some patients were selected
Positive number for Positive number
for treatment and follow-up. acid-fast staining for Auramine O
Method (%)* staining (%)†
Methods
The slicing of all specimens was done in an airtight biological Fluorescent quantitative PCR 37/75 (49) 46/75 (61)
detection—positive
safety cabinet, and a separate microtome knife was used for
Fluorescent quantitative PCR 9/50 (18) 15/50 (30)
each specimen. All specimens were soaked in 95% ethanol solu- detection—negative
tion for 5 min and then dried. A total of 20 sections, 6 mm Fluorescent quantitative PCR 46/88 (52) 61/88 (69)
thick, were prepared from each, 10 of which were used for detection after EDTA retrieval—
routine fluorescence quantitative PCR and another 10 for fluor- positive
escence quantitative PCR with EDTA heat-induced retrieval to Fluorescent quantitative PCR 0/37 (0) 0/37 (0)
detect TB/non-tuberculous mycobacteria. Another two serial detection after EDTA retrieval—
sections were used for acid-fast staining and Auramine O stain- negative
ing, respectively, following the method described in previous *Comparison among groups, pDownloaded from http://jcp.bmj.com/ on October 11, 2016 - Published by group.bmj.com
Original article
then transferred to the magnetic bead extraction apparatus for two groups was assessed using χ2 test. A p valueDownloaded from http://jcp.bmj.com/ on October 11, 2016 - Published by group.bmj.com
Original article
acid-fast staining, fluorescence quantitative PCR was commonly
Table 3 Mycobacteria detection results of fluorescent quantitative
used to detect M. tuberculosis in tissues. The sensitivity and spe-
PCR detection before/after EDTA retrieval in 125 cases of
cificity of this method for detecting M. tuberculosis in sputum
inflammatory granuloma with different specimen types
or surgical fresh specimens were 73.3% and 99.4%,
Positive number of Positive number of respectively.10
fluorescent fluorescent quantitative However, the sensitivity and specificity of quantitative PCR
quantitative PCR PCR detection after
Specimen type detection (%)* EDTA retrieval (%)†
for detecting mycobacteria in tissue specimens (65% and
85.3%, respectively) were slightly lower than those in sputum
Lung puncture or bronchial 37/58 (64) 43/58 (74) or surgical specimens. Also, the detection rate of M. tuberculosis
fiberscope biopsy using fluorescent quantitative PCR in formalin-fixed,
Lymph node biopsy 35/52 (67) 38/52 (73) paraffin-embedded histological sections of granulomatous
Lung resection 2/10 (20) 5/10 (50) lesions generally ranged from 50% to 60%.3 In this study, the
Skin biopsy specimens 1/5 (20) 2/5 (40) sensitivity and specificity of fluorescent quantitative PCR in the
Lymph node tissues of 0/30 (0) 0/30 (0) tissues retrieved with EDTA were 72% and 98.5%, respectively,
non-granulomatous lesions
which were significantly higher than the values obtained when
*Comparison among groups, pDownloaded from http://jcp.bmj.com/ on October 11, 2016 - Published by group.bmj.com
Original article
eliminated the cross-linking between the tissue DNA and tuberculous mycobacterial detection rate using fluorescent quan-
the bacterial DNA, digested the tissue using proteinase K, titative PCR could be increased after EDTA heat-induced
extracted DNA in tissues and hoped to improve the detection retrieval. The mycobacterial detection rate increased by 10.4%,
rate. Because EDTA heat-induced retrieval is suitable for the and the amplification efficiency was significantly improved
process of fluorescent quantitative PCR, the specimens were put (figure 2). Moreover, the specificity was high. The method was
into an EP tube to dewax, followed by EDTA heat-induced simple to carry out. Hence, further large-scale studies are
retrieval, DNA extraction and fluorescence quantitative PCR required to validate the present findings before translating the
detection. research into clinical practice.
Fluorescent quantitative PCR showed that 75 of 125 (60%)
Handling editor Cheok Soon Lee
specimens were positive for mycobacteria; this detection rate
was slightly lower than the rate in sputum or surgical specimens. Contributors ZZ conceived the idea for the paper, XW wrote the manuscript, FX,
QZ, XQ, ML and XZ were involved in finding example cases for the publication and
Some difference was found when the results of routine path-
assisting the experimental operation. All authors read, edited and approved the final
ology special staining (46/125 (36.8%) for acid-fast staining and manuscript.
61/125 (48.8%) for Auramine O staining) were compared;
Competing interests None declared.
however, the detection rate was higher compared with the other
Patient consent Obtained.
two methods. Some cases were not detected by fluorescent
quantitative PCR, but the results of acid-fast or Auramine O Ethics approval This study was approved by Fuzhou General Hospital ethics
committee.
staining were positive, indicating that although the mycobacter-
ial detection rate using routine fluorescent quantitative PCR in Provenance and peer review Not commissioned; externally peer reviewed.
tissues was higher than the rate in the case of special staining
(acid-fast and Auramine O staining), still false-negative results REFERENCES
1 Banada PP, Sivasubramani SK, Blakemore R, et al. Containment of bioaerosol
were obtained. The mycobacterial detection rate using fluores-
infection risk by the Xpert MTB/RIF assay and its applicability to point-of-care
cent quantitative PCR after tissue retrieval with EDTA was settings. J Clin Microbiol 2010;48:3551–7.
70.4% (88/125), and the positive cases were also completely 2 Boehme CC, Nabeta P, Hillemann D, et al. Rapid molecular detection of
detected in acid-fast and Auramine O staining, which indicated tuberculosis and rifampin resistance. N Engl J Med 2010;363:1005–15.
that the protein cross-linking caused by formalin could be 3 Mishra PK, Gorantla VR, Bhargava A, et al. Molecular detection of Mycobacterium
tuberculosis in formalin-fixed, paraffin-embedded tissues and biopsies of
broken by the pretreatment with EDTA, which contributed to gastrointestinal specimens using real-time polymerase chain reaction system. Turk
tissue digestion and DNA extraction and avoided the false- J Gastroenterol 2010;21:129–34.
negative results of fluorescence quantitative PCR detection. 4 Ye F, Chen Y, He D, et al. [Detection of Mycobacterium tuberculosis complex in
Comparing the Ct value of PCR amplification with or without paraffin-embedded tissues by real-time fluorescent quantitative polymerase chain
reaction]. Zhonghua Bing Li Xue Za Zhi 2013;42:534–7.
EDTA retrieval indicated that the amplification efficiency was
5 Wang X, Xie F, Zheng Z. Application of fluorescent quantitative PCR detection of
improved by EDTA retrieval. A statistically significant difference mycobacterium tuberculosis / non-tuberculous mycobacteria in pathological
was found between the two groups ( pDownloaded from http://jcp.bmj.com/ on October 11, 2016 - Published by group.bmj.com
Fluorescent quantitative PCR detection of
Mycobacterium tuberculosis in tissue
sections from granulomatous lesions
retrieved using EDTA
Xuzhou Wang, Feilai Xie, Qiaoling Zheng, Xingfeng Qi, Min Li, Xiaoling
Zhou and Zhiyong Zheng
J Clin Pathol published online September 29, 2016
Updated information and services can be found at:
http://jcp.bmj.com/content/early/2016/09/29/jclinpath-2016-203738
These include:
Supplementary Supplementary material can be found at:
Material http://jcp.bmj.com/content/suppl/2016/09/29/jclinpath-2016-203738.D
C1.html
References This article cites 15 articles, 5 of which you can access for free at:
http://jcp.bmj.com/content/early/2016/09/29/jclinpath-2016-203738
#BIBL
Email alerting Receive free email alerts when new articles cite this article. Sign up in the
service box at the top right corner of the online article.
Topic Articles on similar topics can be found in the following collections
Collections Molecular biology (29)
Notes
To request permissions go to:
http://group.bmj.com/group/rights-licensing/permissions
To order reprints go to:
http://journals.bmj.com/cgi/reprintform
To subscribe to BMJ go to:
http://group.bmj.com/subscribe/You can also read

















































